
Abstract
Background
Laparoscopic surgery has spread quickly during the past twenty years, and has become one of the important treatments in the field of colorectal surgery. Recently, natural orifice transluminal endoscopic surgery (NOTES) has been studied as the next generation of minimally-invasive surgery, but the feasibility and safety of the NOTES method have not been evaluated. In such a situation, single-incision laparoscopic surgery has attracted interest from surgeons worldwide. However, single-incision laparoscopic colorectal surgery has not yet been standardized.
Methods
From February 2010, single-incision laparoscopic colectomy was performed for 7 patients presenting with early colon cancer. All procedures were performed by two experts with the License of Endoscopic Surgical Skill Qualification System (ESSQS) of Japan Society for Endoscopic Surgery (JSES) in the field of colorectal Surgery.
Results
We used the Gelport system (Applied Medical, Rancho Santa Margarita, CA, USA) as the access port and 3 trocars of different sizes (Ethicon, Inc., Cincinnati, OH, USA). Using this technique, we did not experience any difficulties or use any articulated instruments. All of the present 7 patients underwent the single-incision laparoscopic colectomy successfully and had no complications.
Conclusion:
Single-incision laparoscopic surgery using the Gelport was performed safely in the present cases. The use of the Gelport as an access port can address the technical difficulty associated with this new technique.
Keywords
INTRODUCTION
Laparoscopic surgery has spread quickly for use in cholecystectomy and in more complex surgeries such as gastrectomy, colectomy and rectal surgery over the past twenty years. Moreover, laparoscopic cholecystectomy has become the gold standard for the treatment of symptomatic gallbladder stone diseases, including acute cholecystitis (1, 2).
Recently, natural orifice transluminal endoscopic surgery (NOTES) has been advocated as the next generation of minimally invasive surgery, and can result in reduced scar formations. The NOTES method was reported for the first time by Kalloo et al., who introduced their work using transgastric pertitoneoscopy in the porcine model (3). Marescaux et al. also reported successful NOTES completion in a clinical case (4). Although several reports using NOTES were published, the feasibility and the safety of NOTES have not been evaluated.
In this situation, single-incision lapaparoscopic surgery has attracted interests from surgeons worldwide. Single-incision laparoscopic cholecystectomy has already been widely performed because of its simple procedure. However, single-incision laparoscopic colorectal surgery has not yet been standardized. There have been few reports of single-incision laparoscopic colectomy.
We have already begun using single-incision laparoscopic colectomy in patients with early colon cancer. In the present study, we described our procedures and evaluated the short-term results.
MATERIALS AND METHODS
From February 2010 to September 2010, single-incision laparoscopic colectomy was performed in 7 patients presenting with early colon cancer. All of the patients underwent colonoscopy to identify colon cancer and a CT scan for staging of the disease. All procedures were performed by two experts licensed according to the Endoscopic Surgical Skill Qualification System (ESSQS) of the Japan Society for Endoscopic Surgery (JSES) in the field of colorectal surgery. The details of these patients included the patient age, gender, body mass index (BMI), American Society of Anesthesiologists (ASA) score, the history of prior abdominal surgery, the disease type and tumor location. The operative parameters included operation method, blood loss, operative time, incision length, conversion to conventional laparoscopic surgery or open surgery, post operative pain measured by visual analog scale on post operative day 1 and 5 and complications. The pathological findings included the degree of differentiation, depth, lymph node metastasis, lymphatic vessel invasion, vascular invasion and the number of lymph nodes. This is a retrospective review of prospectively gathered data to show the feasibility of single-incision laparoscopic colectomy using the Gelport system. Post operative complications were followed up for 30 post operative days.
SURGICAL TECHNIQUE
After obtaining informed consent, patients with right and transverse colon cancers were placed in the supine position. The Gelport (Applied Medical, Rancho Santa Margarita, CA, USA) was inserted through a 3-cm transumbilical incision and used as the access port. We usually used 3 trocars of different sizes (Ethicon, Inc., Cincinnati, OH, USA) to prevent clash between these trocars (Fig. 1A, B). The flexible video laparoscope (Olympus Medical System Corp, Tokyo, Japan) was used as in conventional laparoscopic colonic surgery. The energy source used was the Harmonic Ace (Ethicon, Inc., Cincinnati, OH, USA) and the other laparoscopic instruments were the same as used in conventional laparoscopic colonic surgery (Fig. 1C). The colon was mobilized using the medial-to-lateral approach. First of all, we usually look for the thin membrane which through we can see the duodenum and pancreas. We cut this membrane and dissect between mesocolon and duodenum to the lateral side. Lymph node dissection was intracorporeally performed
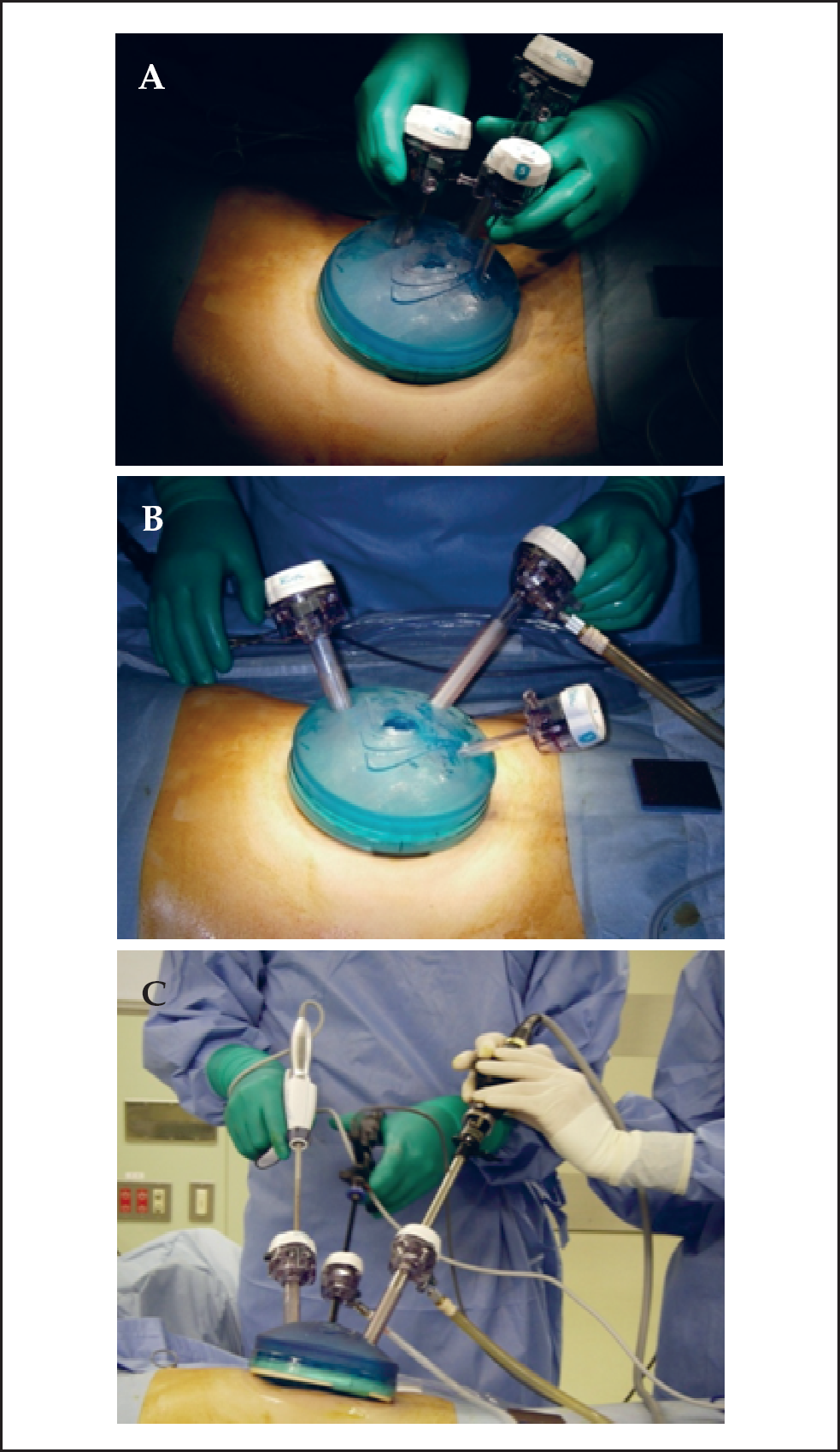
We usually use The Gelport (Applied Medical, Rancho Santa Margarita, CA, USA) as an access port. The advantage of the Gelport is that we can insert several trocars multiple times if necessary. Moreover, we can keep the trocars apart for as long as possible to maintain instrument triangulation and to prevent instrument clashing outside the abdomen.
RESULTS
Seven patients (3 male patients, 4 female patients) underwent single-incision laparoscopic colectomy using the Gelport system. The details of these patients are shown in Table 1. The median age was 68 years (range, 61–73). The median body mass index of the patients was 22.4 kg/m2 (range, 19.6–23.9). The sites of the tumors were the right colon (n = 6), and transverse colon (n = 1). Two patients had undergone a prior abdominal procedure. Both cases (Case 1 and 5) received appendectomy and we faced some adhesions during these operations. However, they were not problem to continue single-incision laparoscopic surgery.
Preoperative parameters of these six patients.
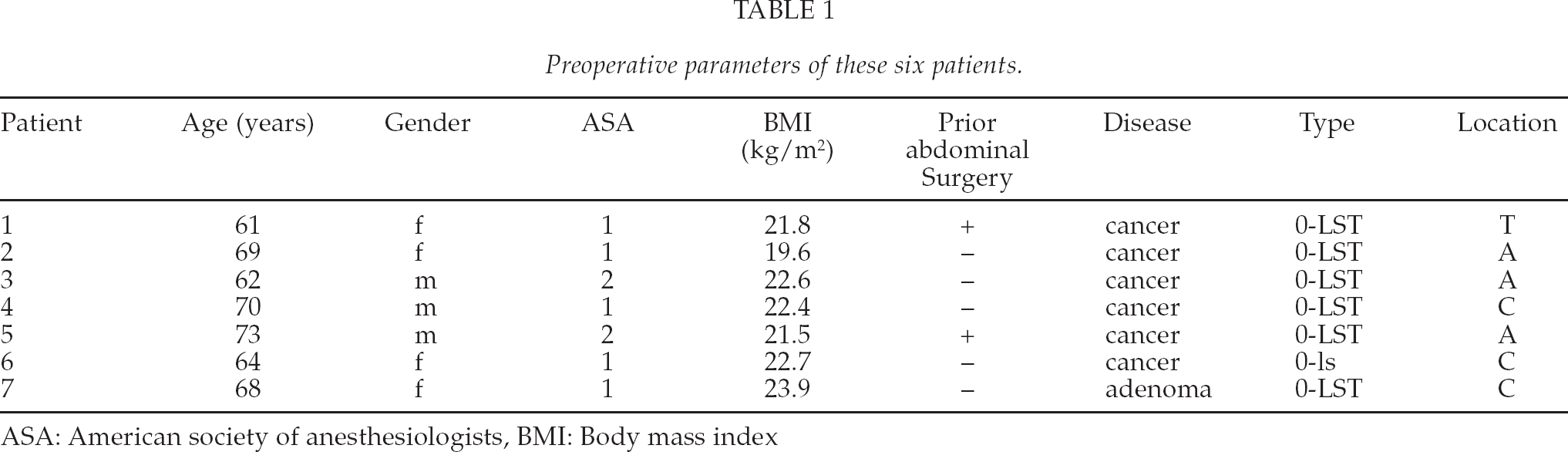
ASA: American society of anesthesiologists, BMI: Body mass index
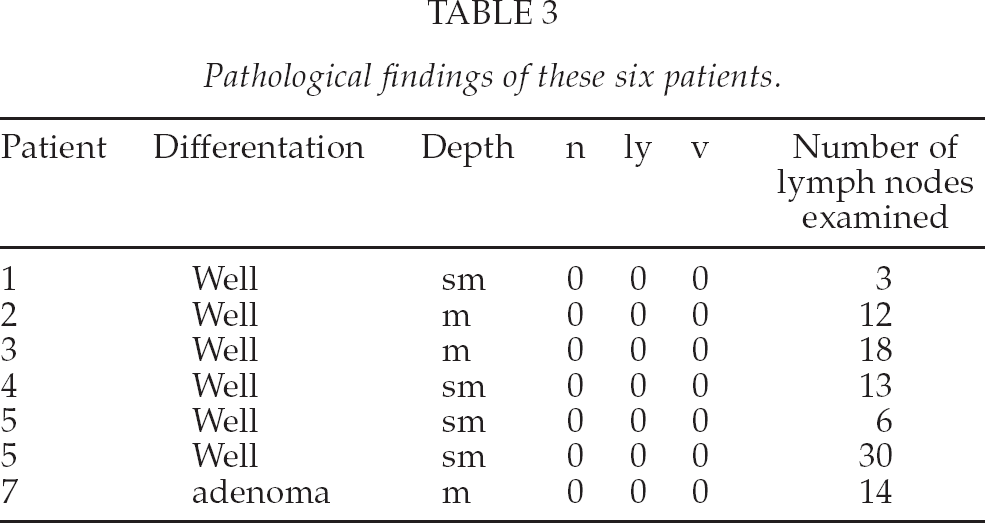
All of the 7 patients underwent the single-incision laparoscopic colectomy successfully and had no complication. There was no mortality or reintervention within 30 days. The median incisional length was 3.0 cm (range, 2–3). The median number of lymph nodes examined was 13 (range, 3–30). All of the resection margins were clear (Tables 2, 3).
Intraoperative parameters of these six patients.
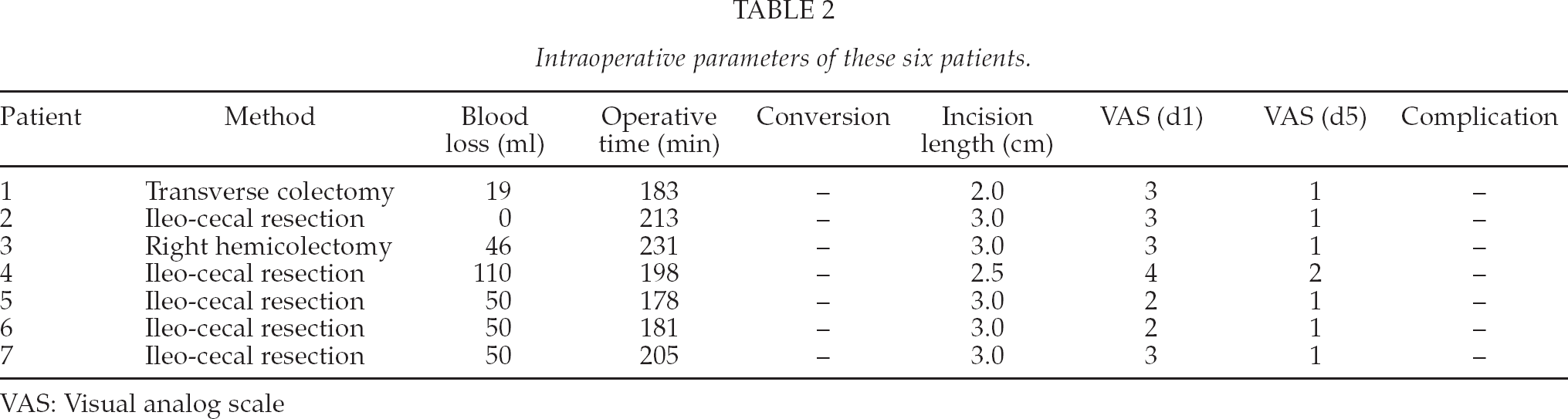
VAS: Visual analog scale
Pathological findings of these six patients.
DISCUSSION
Single-incision laparoscopic colectomy has not been established, because there are only a few reports of small patient series in the literature (5 –13). Katsuno G et al. analyzed retrospectively their 31 patients who were treated with transumbilical single-incision laparoscopic colectomy for colon cancer and showed the feasibility of their procedure (14).
The apparent advantages of single-incision laparoscopic colectomy are cosmetic. However, the main disadvantage is the difficulty in performing this procedure due to lack of instrument triangulation and the use of only two operating ports. Moreover, there are several problems with the technique; for example, the clash of instruments outside the abdomen, the pneumoperitoneum leaks and a requirement of the articulated instrument. To solve these problems, we primarily use the Gelport system.
The first report of single-incision laparoscopic cholecystectomy used a multiple fascial puncture technique under a skin flap (15). The disadvantages of this technique are the weakness of the fascia, due to the creation of multiple defects and seroma formations. Therefore, the selection of the access port is an important consideration. There are several reports assessing the ideal access port location.
The Triport (Advanced Surgical Concepts, Wicklow, Ireland) is designed to be an access port for single-incision laparoscopic surgery. The Triport is introduced into the abdomen through the fascial defect by an introduction device. The outer component of the TriPort has three ports (two 5 mm ports and one 12 mm port) and contains an insufflations port, allowing regulated gas insufflation without the additional need for a Veress needle. Recently, several reports have described the use of a Triport for urologic procedures (16 –18)and cholecystectomies (19, 20). There are several advantages to this access port. One of these advantages is that multiple instruments can be inserted through this access port multiple times without a loss of the pneumoperitoneum. However, the disadvantage is that there is a limit to instrument mobility because these ports may be too close to each other.
The AirSeal (SurgiQuest, Orange, CT, USA) is an innovative trocar compared to the traditional trocar. This port does not use a mechanical barrier but a pressure barrier that exceeds the pneumoperitoneum. Currently, the AirSeal is available on a limited basis in the United States.
A: This is the thin membrane, which through we can see duodenum and pancreas. B: From this part, we start dissection. C: Medial approach was performed. D: Ileocecal vessels were clipped and cut.
The SILS port (Coviden, Inc., Norwalk, CT, USA) is made from an elastic polymer. This port is hourglass-shaped and can be deployed through a 2-cm fascial incision. The SILS contains four openings: one for insufflations and three trocars 5 to 12 mm in size.
We described our procedure of single-incision laparoscopic colectomy using the Gelport. Using this technique, we can insert several trocars multiple times if necessary. Moreover, we can keep the trocars apart for as long as possible to maintain instrument triangulation and to prevent instrument clashing outside the abdomen.
The most important issues of the single-incision laparoscopic surgery are the much smaller space outside the abdomen than in conventional laparoscopic surgery. To circumvent this issue, articulated instruments have been developed. The Roticulator (Coviden, Inc., Norwalk, CT, USA), the RealHand (Novare Surgical Systems, Inc. Cupertino, CA, USA) and the Cambridge Endo (Framingham, MA, USA) are already available. However, these articulated instruments require “the cross-handed technique,” which requires specialized training and visual-spatial skill.
The use of a flexible video laparoscope helps maintain the working space to some extent, and there is a limitation to working outside the abdomen. During this procedure using the Gelport and several sizes of trocars, we did not require any additional trocars or articulated instruments.
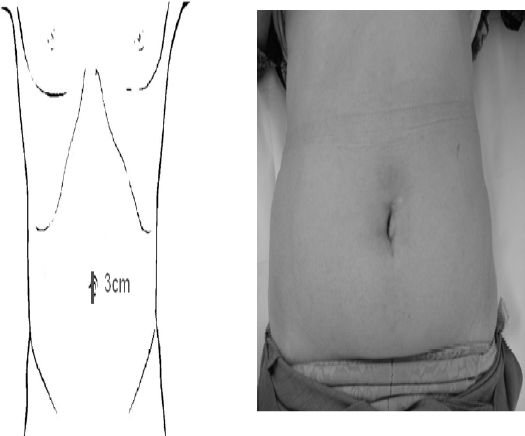
Generally, it is believed that single-incision laparoscopic surgery is not less invasive compared to conventional laparoscopic surgery. The disadvantage of single-incision laparoscopic surgery is the technical difficulty due to only two operating trocars, the lack of the instrument's triangulation, the clash of instruments outside the abdomen and the requirement of articulated instrument. The advantage of this technique, which operation was performed through the Gelport system, is that we don't require any articulated laparoscopic instruments and it is difficult to identify the surgical scar because of the small associated skin incision (Fig. 2). Therefore, we concluded that the Gelport has the potential to successfully address these considerations.
CONCLUSIONS
The use of the Gelport as an access port during single-incision laparoscopic colectomy helps to reduce the technical difficulties. The present seven patients underwent single-incision laparoscopic colectomy and had no conversion to conventional laparoscopic surgery or open surgery, and also experienced no complications. However, before extending the indication of this procedure, we must evaluate the oncological safety of using this system for the treatment of advanced cases and those with rectal cancer.