
Abstract
Background:
Only limited data in the literature about single-incision laparoscopic rectal surgery, because the laparoscopic stapler does not allow low rectal transection without sufficient distal margins from the umbilicus port. We have developed single-incision plus one port laparoscopic anterior resection of the rectum (SILS+1-AR) as a reduced port surgery in which we can utilize the incision for drainage as an additional access route for laparoscopic procedures including the transection the lower rectum.
Methods:
A Lap protector (LP) mini was inserted through a 2.5 cm transumbilical incision, and an EZ-access was mounted to LP and three 5-mm ports were placed in EZ-access. A 12 mm port was inserted in right lower quadrant. Almost all the procedures were performed with usual laparoscopic instruments, and the operative procedures were much the same as in usual laparoscopic low anterior resection of the rectum using a flexible 5mm scope. The rectum was transected normally using only one endoscopic linear stapler inserted from the right lower quadrant port.
Results:
We underwent modified SILS+1-AR in 16 patients with advanced rectal cancer. In all cases, there was no need to extend the skin incision. We transected the lower rectum with one laparoscopic stapler in all six cases. Postoperative follow-up did not reveal any umbilical wound complications or recurrences.
Conclusions:
The safety and feasibility of SILS+1-AR for advanced rectal cancer was established in this study. However, further studies are needed to prove the advantages of this procedure to conventional laparoscopic law anterior resection.
Keywords
INTRODUCTION
Single-incision laparoscopic colectomy has been described through case reports and small case series (1–3). However, there is limited data in the literature about single incision laparoscopic rectal surgery (4), because the laparoscopic stapler does not allow low rectal transection without sufficient distal margins from the umbilicus port.
In low anterior resection of the rectum, many surgical institutes routinely use pelvic drains after anterior resection for an early detector of anastomotic leaks and reduction of the needs for reoperation. We have developed single-incision plus one port laparoscopic anterior resection of the rectum (SIL+1-AR) in which we can utilize the incision for drainage as an additional access route for laparoscopic procedures including the transection the lower rectum. In this study, we describe the methods and our initial results of SILS+1-AR for advanced rectal cancer.
PATIENTS AND METHODS
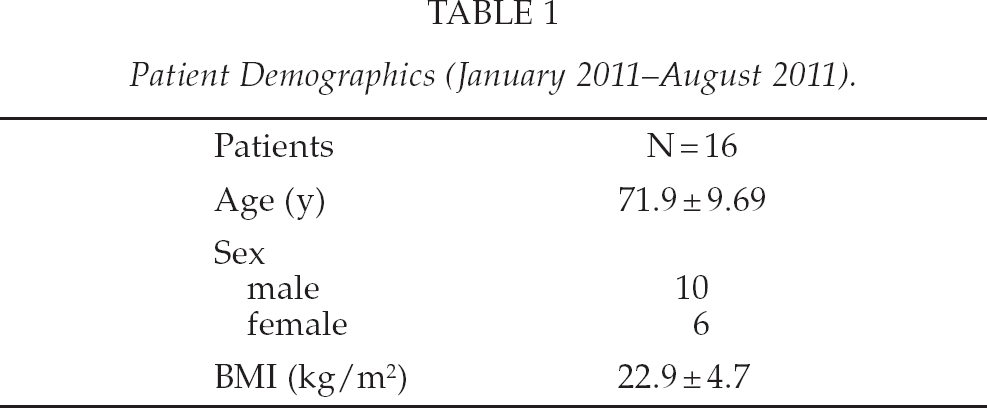
Our initial experience of performing a SIL+1-LAR with lymph node dissection in 16 patients is presented. 16 patients (6 women) with a mean age of 67.9 ± 10.6 years and a mean body mass index of 22.9 ± 4.7 kg/m2 adopted the SILS + 1 procedure for advanced rectal cancer between January and August 2011 (Table 1). In all cases, the patient's consent about single port laparoscopic surgery was obtained.
Patient Demographics (January 2011–August 2011).
SURGICAL TECHNIQUE
Under general anesthesia, the patients were placed in the modified lithotomy position. First, a Lap protector mini (LP; Hakkou Shoji, Japan) was inserted through a 2.5 cm transumbilical incision (Fig. 1a), the wound was protected. Next, an EZ-access (Hakkou Shoji, Japan) was mounted to LP (Fig. 1b) and three 5-mm ports were placed in EZ-access. A 12 mm port was inserted in right lower quadrant (Fig. 1c). Almost all the procedures were performed with usual laparoscopic instruments, and the operative procedures were much the same as in usual laparoscopic low anterior resection of the rectum using a flexible 5 mm scope. The peritoneum was incised at the level of the promontorium above the bifurcation of iliac artery and the sigmoid colon was mobilized using a medial to lateral approach with the left ureter and gonadal vessels preserved. The dissection was continued superiorly to the level of the root of the inferior mesenteric artery. All of the soft tissue anterior to the inferior mesenteric artery was completely removed and D3 lymph node dissection was achieved (Fig. 2a). Then the root of the superior rectal artery and inferior mesenteric vein were divided. The lateral attachments of the sigmoid colon were dissected until the previously dissected area, and full mobilization of the sigmoid colon was completed.
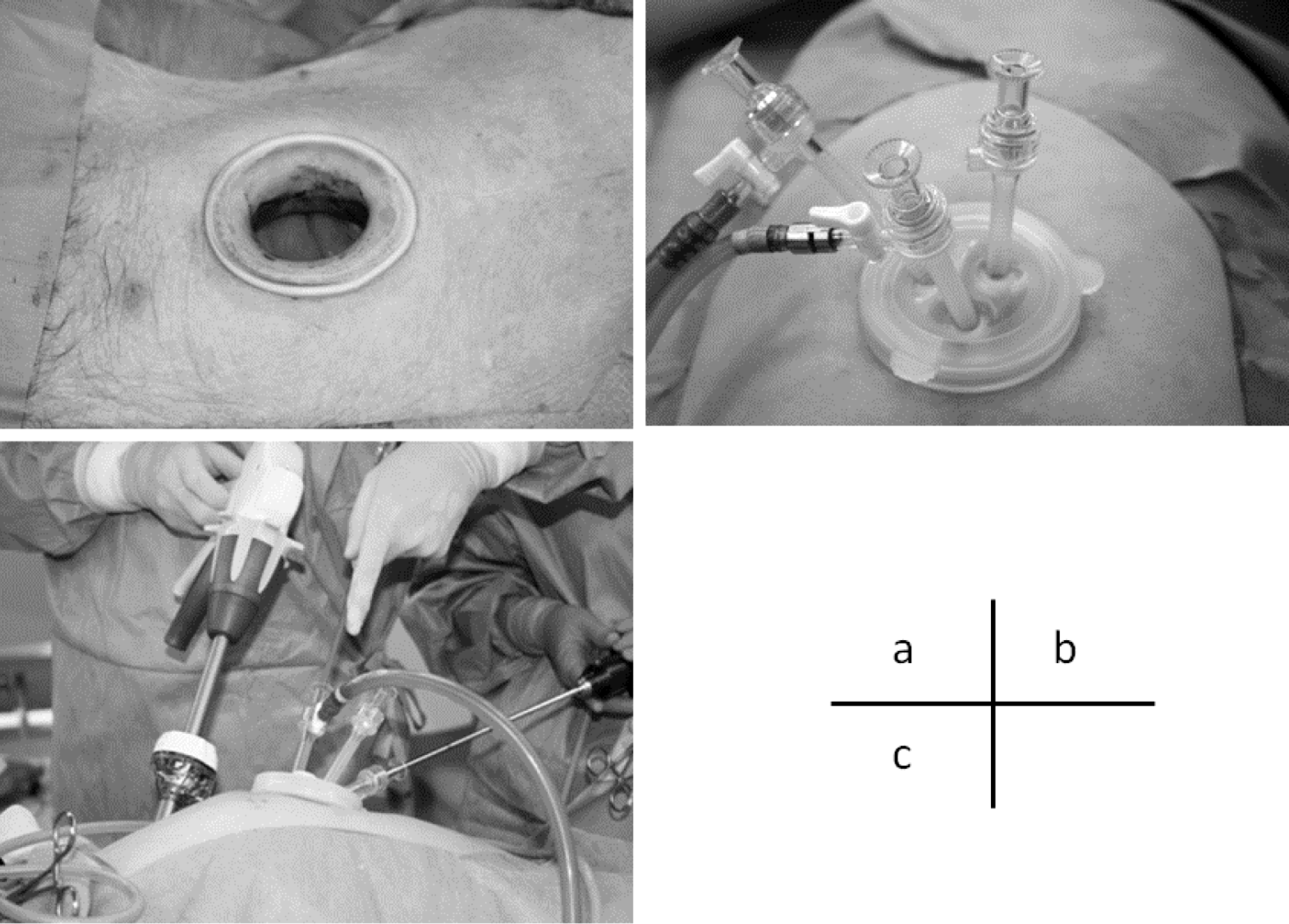
A Lap protector mini is inserted through a 2.5 cm transumbilical incision (a), and an EZ-access is mounted (b) and three 5-mm ports are placed in EZ-access. A 12 mm port is inserted in right lower quadrant of the abdomen(c).
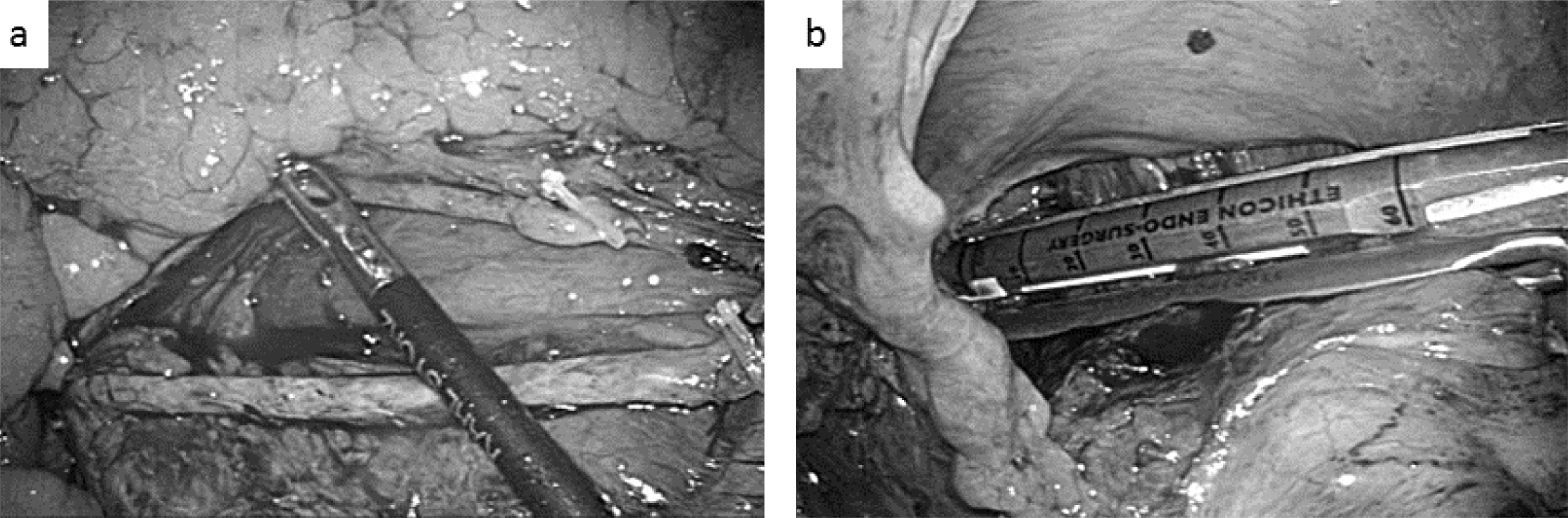
SIL+1-LAR with lymph node dissection around the inferior mesenteric artery and vein (a) and transection of the rectum with laparoscopic stapler inserted from the port of right lower quadrant of the abdomen (b).
Before starting the dissection of the mesorectum, the sigmoid colon was tightened with the fine cut gauze, and the assistant retracted this gauze to make the operative field with the grasper inserted from umbilicus port. The rectum was posteriorly mobilized at first in front of the hypogastric nerve. Thereafter anterior mobilization was performed at the plane immediately behind Denonvillier's fascia not to injure the neurovascular bundle. The lateral dissection of the rectum was performed afterwards, and the rectum enveloped within the fascia propria recti was completely removed. The rectum was transected normally using one endoscopic linear stapler (Ehelon flex 60; Ethicon Endo-Surgery Inc, Cincinnati, OH, USA) with gold cartridge inserted from the right lower quadrant port following after rectal lavage (Fig. 2b).
The proximal colon was extracted through the umbilical incision. Resection was achieved following extracorporealization, and the anastomosis was performed with double stapling technique using a transanally inserted circular stapler (CDH29; Ethicon Endo-Surgery Inc). Normally diverting stoma was not performed. A pelvic drainage tube was inserted from the right lower quadrant incision.
RESULTS
One patient (6.3%) required an additional port insertion because of the severe difficult dissection in the deep pelvic space. The other 15 patients (93.7%) underwent a curative anterior resection of the rectum without conversion to a multiport laparoscopic surgery or open surgery.
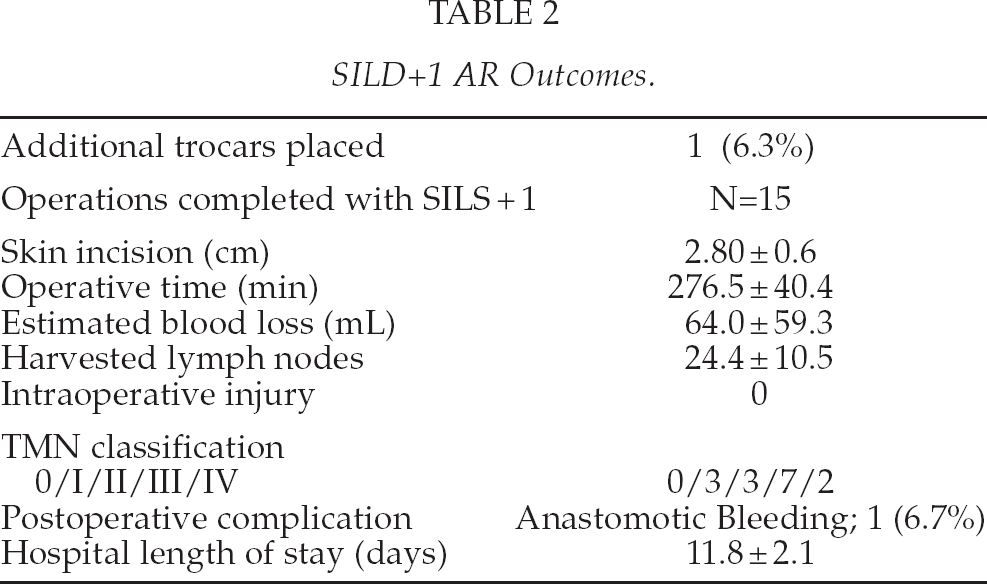
In the 15 cases, the mean incision length was 2.8 ± 0.6 cm. We transected the lower rectum with one laparoscopic stapler in 14 cases (93.3%). Average operative time was 276.5 ± 40.4 minutes. Average intra operative blood loss was 64.0 ± 59.3 g. The mesorectum of the specimens were macroscopically intact in all cases. Postoperatively anastomotic bleeding occurred in 1 patient; she was successfully treated with endoscopic approach and discharged 10 days after the operation. The mean number of lymph nodes extracted was 24.4 ± 10.5. All surgical margins were negative and the mean distal margin of the specimen was 3.91 ± 2.19 cm. The pathological stages included stage I (n = 3), stage II (n = 3), stage III (n = 7) and stage IV (n = 2). None of the patients developed neurogenic bladder, and none of male patients developed any sexual disturbances. Patients were discharged in average 11.8 ± 2.1 postoperative days, and postoperative follow-up (6–13 months) did not reveal any umbilical wound complications or recurrences (Table 2, Fig. 3).
SILD+1 AR Outcomes.

An umbilical scar and a small scar for the pelvic drainage.
DISSCUSION
Many surgeons have attempted to reduce the number and size of ports in laparoscopic surgery to decrease parietal trauma and improve cosmetic results, and single incision laparoscopic surgery has been developed, which completed laparoscopic procedures by trocars located at one umbilical incision (5, 6). The application of the single-incision laparoscopic surgery for colon and rectal surgery has emerged only recently in the published literature (1–4). The published studies have limited almost in the right (2, 3) and sigmoid (1) colon, and the data in the literature about single incision laparoscopic rectal surgery is extremely rare.
This is because the tip of the laparoscopic stapler is able to bent only 45 degrees in maximum which makes it very difficult to transect the lower rectum with sufficient distal margins from the umbilicus port. In the unique reported study of completed SILS sphincter-saving mesorectal excision in, Hamzaoglu et al. (4) transected the lower rectum with 4 to 6 laparoscopic staplers. Regarding a number of the staplers, Kim et al. (8) reported that a number of stapler firings is a significant risk factor for anastomotic leakage, and they concluded a reduction in the number of linear stapler firings is necessary to avoid anastomotic leakage after laparoscopic colorectal anastomosis with a double stapling technique.
Tsujinaka et al9, reported in their study in 196 patients who underwent elective anterior resection for rectal cancer that pelvic drainage may act as an early detector of anastomotic leaks and reduce the need for reoperation in selected patients undergoing rectal cancer surgery. We agree with this study and routinely use pelvic drains. In these patients, the small incision is required in the right or left lower quadrant of the abdomen for the drainage. To utilize this incision, we have developed SILS+1-AR in which we use this incision as an additional access route of the linear stapler at the transection of the lower rectum. This technique made it possible to transect the lower rectum with only one laparoscopic stapler and brought us excellent outcomes. Furthermore, this incision is also used as the trocar for the operator's right handed instrument which may decrease the confliction between the operative instruments and the camera caused by the limited space resulting from using only a single incision.
In conclusion, we have documented the safety and feasibility of SILS+1-AR for rectal cancer. This procedure is a promising alternative method as scarless abdominal surgery for the treatment of some patients with rectal disease. Further studies are needed to prove the advantages of SILS+1-AR to conventional laparoscopic law anterior resection.
Footnotes
ACKNOWLEDGMENT
Drs. Yasumitsu Hirano, Masakazu Hattori, Satsuki Shimizu, Yoshiki Sato, Kazuya Maeda, Kenji Douden and Yasuo Hashizume have no conflicts of interest or financial ties to disclose.