
Abstract
Aim
To investigate the informal caregiving experiences of adult offspring of patients recently hospitalized with alcohol-related liver disease (ALD).
Methods
A narrative analysis was conducted building on 13 semi-structured qualitative interviews with adult offspring of patients who were recently hospitalized with ALD at a department of medicine. Analytical frameworks were the rites of passage framework and its concept of liminality, combined with Taylor's social imaginaries and Järvinen and Bloch's complementary role requirements.
Results
Adult offspring of patients with ALD described longstanding mental health issues that had worsened in response to their parent's repeated hospitalizations. They described how internalized and institutionalized ideas about family shaped a strong sense of moral obligation to care for their parent, which was often intensified when hospital staff implicitly positioned them as caregivers. The offspring described a prolonged liminal phase marked by recurring crises that prevented them from regaining a stable and ordinary everyday life.
Conclusions
The study demonstrates the emotional and moral dilemmas of informal caregiving in adult offspring of a parent hospitalized with ALD. This is a psychosocially vulnerable group whose wellbeing may be further compromised when they are drawn into caregiving roles. Healthcare professionals should avoid reinforcing such roles and rather engage in open dialogue, acknowledge their position and needs.
Keywords
Introduction
I would check in with him once a day, write the same thing, just “Hi dad”, really, just to make sure he was alive you know? Then one day … he didn’t read my text from 11 am to 5 pm. My dad literally just lazes around during the day, if he's not watching TV, he's looking at his phone. So, I thought that was odd. That's why I drove over there, dropped off my wife and kids, and I thought to myself “I’m gonna find him on the floor”. And next thing I found my dad on the couch looking completely white, yellow eyes, lying in the darkness.
(Kevin, 34 years old)
This is Kevin describing the day of his father's third and latest hospitalization with alcohol-related liver disease (ALD) that year. This time around, his father was hospitalized for about 9 days. Kevin was the first adult offspring of a patient with ALD we interviewed, and Kevin's experience would be echoed in the next 12 interviews: the constant worrying and monitoring due to the recurrent acute situations inducing in them a sense of being caught between trying to save their parent and anticipating their death. Most of the informants would resonate with Kevin's notion that, if he did not keep an eye on his father, no one would, and, if his father did not respond to a text message, he could be lying on the floor, dying; a realistic thought, each of the informants had learned, making it no less intrusive. While the parent's hospitalization for ALD sometimes triggered relief in the adult offspring since their parent was now observed and treated by professionals daily, they were also faced with new caregiving tasks and emotional dilemmas.
Adult offspring of patients with ALD are a particularly vulnerable group of informal caregivers for several reasons. Previous studies have highlighted the unhealthy dynamics of families with parental substance use (Mardani et al., 2023; Muir et al., 2023), including the “parentification” of offspring of parents with alcohol use disorder (AUD) during childhood (Kelley et al., 2007; Lindeman et al., 2022) and the sympathy that an offspring sometimes automatically bestows on a parent independent of the mother's or father's parental capabilities (Järvinen & Bloch, 2017). A Danish register-based cohort study found the prevalence of non-intact family structure to be much higher in families with parental AUD; only 37.3% of offspring with parental AUD lived with both parents compared to 74.2% of offspring without parental AUD (Holst et al., 2020). Furthermore, there is a growing recognition of how AUD causes harm to affected others (Orford et al., 2010, 2013; Muir et al., 2023). A scoping review found that offspring of parents with AUD are more likely to experience violence and abuse than offspring of parents with other chronic diseases (Rossow et al., 2016) and other studies have shown that offspring of parents with AUD are vulnerable to adverse outcomes related to, for example, mental and somatic illness (Holst et al., 2022; Mardani et al., 2023), and a range of financial, social and cultural problems (Mardani et al., 2023). Thus, treatment aimed at offspring of parents with AUD is essential. Historically, treatment approaches have centered on the individual with AUD with limited consideration for relational, for example, family-orientated aspects. Research points to a lack of recognition of relational aspects of AUD and family-orientation in treatment institutions and advocates broader referrals to treatment options for the whole family rather than just the individual with an AUD (Selbekk & Sagvaag, 2016; Selbekk, 2019). Other studies advocate a separate focus on supporting affected others in their own right rather than as an integral part of the treatment of the person with AUD (Shorter et al., 2024). In a Danish context, the health authorities recommended in both 2015 and 2018 to implement the “Community Reinforcement and Family Training” model (CRAFT) (Danish Health Authority, 2018). The model suggests that treatment institutions – in Denmark located in community settings – offer interventions aimed at “concerned significant others” (CSOs) and that these interventions aim to support CSOs in motivating individuals with AUD to seek support (Hellum et al., 2019). CRAFT has a parallel focus on the well-being of CSOs, but it is ultimately an example of a model with a relational aim in which affected others are integrated in treatment with the primary goal of motivating the person with AUD to attend treatment. Note that, in Denmark, citizens with AUD are by law guaranteed the right to treatment but their offspring are not (Skarsholm, 2023; Skarsholm et al., 2024). Also noteworthy is the absence of clinical guidelines or established practices for identifying and supporting adult next-of-kin of hospitalized patients with ALD, which means that hospital staff generally do not initiate referrals of informal caregivers to available community support services. Consequently, adult offspring of patients with ALD are themselves responsible for seeking help and support within municipal and voluntary services.
A Danish cohort study of offspring of patients with ALD based on data from nationwide health registers showed that offspring were particularly vulnerable at the time of their parent's ALD diagnosis, when they had a median age of 32 years. Their vulnerability was reflected by an increased incidence of hospital admission with poisoning and psychiatric disease and even an increased mortality (Jepsen et al., 2024). The study points to a specific time and setting with the potential for referring adult offspring of patients with ALD to support options: when they encounter healthcare professionals during a time of crisis (Jepsen et al., 2024). To our knowledge, no other studies have explored specific time points and settings to approach adult offspring of parents with AUD or the importance of timing and setting. This inspired our qualitative study in which we interviewed offspring of patients with ALD shortly after their parent's hospitalization with ALD.
As such, the present study aims to bridge a research gap by exploring the individual experiences and needs of adult offspring of patients with ALD leading up to and during their parent's hospitalization.
Methods
Semi-structured qualitative interviews were conducted with 13 adult offspring (≥18 years) of patients who were admitted to a medical department in a Danish hospital with ALD. Biological offspring, adopted offspring and stepchildren were included. The interviews were conducted by the first author over the telephone. They lasted between 40 min and 2 h. The interview guide encompassed themes such as the informant's personal background, family history, parent's history with alcohol and the ALD that caused their parent's hospital admission within the last 3 months preceding the interview. Informants were asked about their everyday lives, how they were coping with their parent's illness and hospitalizations, and whether they had ever been offered support, etc.
The interviews were audio-recorded, transcribed ad verbatim, and coded using the software program NVivo (https://lumivero.com/products/nvivo). Interviews were first coded using the thematic coding of Riessman (2017), which focuses on what is being said in participants’ narratives, including the content and recurring patterns of meaning across cases. Following Riessman (2017), this involved a close reading of each transcript, identifying and labeling meaning units, grouping these into broader categories, and gradually developing preliminary themes that captured shared experiences across interviews. This initial stage also served as a systematic and transparent tool for collaboration between the first and last investigators, who were responsible for the coding process. To ensure consistency and validity, both investigators coded the first couple of interviews separately, then met to compare and refine the thematic categories identified. This was important, because the first investigator, who conducted all interviews, was more immersed in the material than the last author, who contributed to the design of the interview guide, listened to selected audio files and read all the transcripts. After reaching consensus on the coding approach, the first investigator continued the thematic coding of the remaining interviews. Examples of thematic codes include “Own mental health problems” or “Feeling overwhelmed”.
In the second analytic phase we applied Riessman's dialogic/performative coding, which attends to how stories are told: the interactional, contextual and interpretive dimensions of narrative performance (Riessman, 2017). Whereas the thematic coding focused on identifying the explicit content of participants’ accounts, the dialogic phase examined how participants positioned themselves and others in their stories, the cultural and relational voices shaping their narratives, and how meanings were co-constructed in the interview setting. This phase was therefore more interpretive and theoretically oriented, emphasizing the interplay between individual experience and broader social imaginaries. Examples of dialogic codes include “Moral obligations to family” or “A well-kept secret”. Through is interpretive layer, we identified a theoretical framework highlighting the tension in participants’ narratives between institutionalized and internalized social imaginaries of family and their lived experiences as the offspring of a parent with ALD.
Informants
We recruited informants from February to June 2024. Informants were recruited via medical staff who obtained verbal consent from the patients to contact their adult offspring. The offspring were then asked if they would consider participating in a qualitative interview about their experiences with having a parent who had ALD. Since we needed verbal consent from the patient to contact their offspring, they had to be somewhat stable and capable of understanding the consent process. A subset of these patients experienced a sudden deterioration and died shortly before or after the interviews with their offspring. Due to the sometimes unpredictable progression of ALD, it was challenging to time the interviews. We provided space and expressed our condolences when notified of any adverse events.
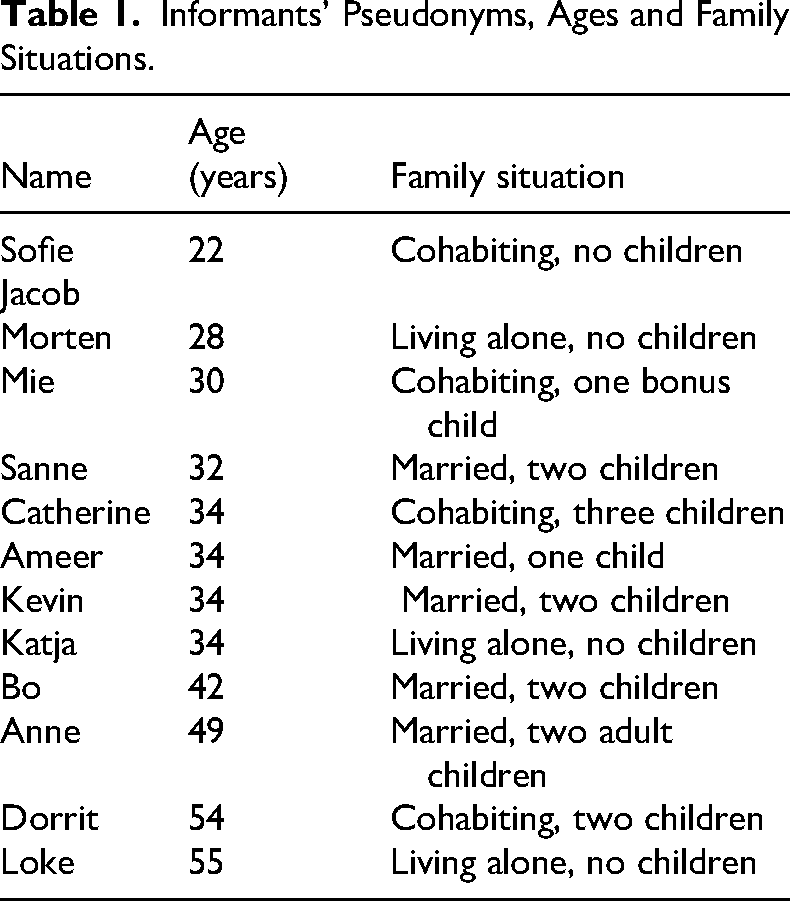
Out of 20 invited, 13 (65%) accepted the invitation and were interviewed. One informant (“Jacob”) never signed the consent form and data from this interview is not presented in the article. Six (30%) of the invited participants never responded and one (5%) rejected the invitation saying they were not interested. The informants were between the ages of 22 and 55 years (Table 1) with a median age of 34 years. We included informants whose parent had been hospitalized for ALD within the 3 months preceding the interview. While some had broken off contact with the parent at earlier points in life, they had some level of contact at the time of the hospitalization. At the time of the interviews, the parent with ALD was either still hospitalized, discharged, or had died. Most informants’ parents were divorced, some had only one living parent and some had two parents both struggling with AUD. Several informants had more family members who struggled with AUD. The majority had experienced previous hospitalizations of the parent, reflecting the common pattern among patients with AUD who often undergo repeated hospitalizations, ultimately succumbing to conditions such as ALD (Askgaard et al., 2020).
Informants’ Pseudonyms, Ages and Family Situations.
Ethical Considerations
The study was conducted in accordance with national and institutional ethical research guidelines, the principles of the Declaration of Helsinki and the EU General Data Protection Regulation (GDPR). In Denmark, qualitative interview studies that do not include biomedical procedures are exempt from approval by the national research ethics committee system. The study was approved by the Danish Data Protection Agency. Participation was voluntary, and all participants provided written informed consent. To protect anonymity, pseudonyms were used and identifying details were removed from transcripts. All data were stored securely on encrypted, access-restricted servers.
Given the vulnerable nature of the themes we interviewed our informants about and the timing of the interview, we continuously discussed ethical obligations at the micro level that needed careful consideration (Brinkmann, 2015). For some, it was their first time sharing their story in such detail while others had done so before in therapeutic settings. Conducting telephone interviews was helpful, making it easier for informants to participate during a uniquely stressful period. Some expressed that it helped them “open up” due to anonymity. However, the themes discussed were so vulnerable that the interviewer had to monitor signs pertaining to informants’ mental health and maintain an attentive, affirmative tone. There was a risk that the interviews could be misconstrued as therapy sessions. Such misunderstandings could compel informants to disclose more than preferred (Brinkmann, 2015). To mitigate this, the interviewer ensured they knew they could skip questions or elaborate as desired and clarified the distinction between an interview and a therapy session (Brinkmann, 2015). The interviewer formulated interpretations out loud, inviting corrections to ensure she interpreted their stories accurately. This is a type of “member-checking”, a processual approach to ensuring validity in qualitative research (Cho & Trent, 2006).
Theoretical Lens
As we explored the informants’ stories as told within the context of their parent's hospitalization, it was evident that their perceptions of the parent's current situation involving ALD was deeply intertwined with their experiences of family abuse, trauma and/or parental neglect. Rather than being temporary, the situation felt on-going and repetitive. We use the concepts of “liminality” and “reconnection” from the anthropological rites of passage framework to describe this (Turner, 1969; Barrett et al., 2016).
Furthermore, it became evident that they battled with emotional dilemmas fueled by expectations from parents and hospital staff as well as within themselves. We draw on Charles Taylor's theory of “social imaginaries” as well as Järvinen and Bloch's previous work with “complementary role requirements” to capture these different levels in their stories (Taylor, 1991, 2004; Järvinen & Bloch, 2017).
Juggling Between Moral Obligations and Self-Determination
Emotional dilemmas and a sense of moral obligation were ever present themes in our interviews. This led us to visit Charles Taylor's view of identity as dialogical: what others, especially our significant others, want to recognize in us, continually shape our identity and actions (Taylor, 1991). These expectations are always guided by what Taylor refers to as “social imaginaries”: collective understandings of the various domains in which shared meanings and practices are central to social life (e.g., family). Social imaginaries are not just theoretical but institutionalized and embedded in everyday practices (Taylor, 2004). We will show that a social imaginary of family is institutionalized and embedded in the caregiving practices of the Danish healthcare system as well. Adult offspring of patients with ALD constantly juggled living up to a social imaginary of “family” as opposed to protecting their own mental health, advance in their jobs or spend time with the families they had formed as adults. This left them with emotional dilemmas that can obviously present themselves in many people's family lives from time to time but seem to be particularly complex in families where the parent has AUD. To understand this dilemma, we are drawn to Margaretha Järvinen and Charlotte Bloch's use of Candace Clark's theory of sympathy-giving, focusing on the concept of “complementary role requirements” regarding adult offspring of parents with drinking problems (to use their terms) (Järvinen & Bloch, 2017). “Complementary role requirements” describes how socially standardized roles obligate family members to play their part if the other family member plays theirs: If the parent lives up to their role, the child is expected to sympathize with them. However, Järvinen & Bloch (2017) find that often when it comes to parents with drinking problems, the relationship is not complementary as the offspring emotionally overinvests although the parent underinvests.
Liminality and the Missing Reconnection
To reflect on the caregiving experience of having a seriously ill parent with ALD, we are inspired by the anthropological rites of passage framework and the concepts of “liminality” and “reconnection” (Turner, 1969; Barrett et al., 2016). We particularly build on the work of Barrett et al. (2016) as they incorporate Turner's concept of liminality in the field of family caregiving, arguing that entering a caregiving role constitutes a modern rite of passage. In this framework, liminality is a temporary phase in the transition process between regular life and a new life situation with a new social role and identity (e.g., that of an informal caregiver for relatives who have become severely ill). According to Barrett et al. (2016), caregivers often face an experience of: “… confusion, anxiety, and of searching for a way through bewildering new systems but also of learning to negotiate with these systems”.
Normally, the liminal phase is temporary and followed by a phase of reconnection with the broader community and with oneself. However, Barrett et al. (2016) point out that reconnection is not assured; the sense of moral obligation to help and support a family member does not always match the available provision of care and resources, sometimes leaving informal caregivers with a sense of powerlessness and a lack of choice. Specific to our informants, they were not suddenly entering the role as caregivers; rather, many of them had enacted aspects of this role from an early age reflecting the common pattern where children of parents with AUD are “parentified” (Kelley et al., 2007). Indeed, several studies have criticized the rites of passage framework for its linearity arguing that rites of passage can instead be fluid or cyclical and that they are always individual and context-dependent, culturally, socially and politically, etc. (Burack-Weiss, 2006; Mattingly, 2010; Hensley, 2019).
Results
The following section contains three sub analyses. First, we describe the psychosocial statuses of our informants as described by themselves. Second, we describe how informants juggle a sense of moral obligation to family against protecting their own mental health. Lastly, we describe how informants experience the parent's AUD, ALD and hospitalization, as seen through the “liminality” lens of the rites of passage framework.
The Psychosocial Statuses of Adult Offspring of ALD Patients
All our informants had some type of mental health problem and most of them had experienced neglectful upbringings to different degrees. An example is Katja (34 years old). At the time of the interview both of her parents had an AUD and the mother was hospitalized with ALD. Katja's parents subjected her to psychological as well as physical violence throughout her childhood. She now has severe mental health problems and a history of self-harm which, according to her, can be attributed to her childhood. Nonetheless, Katja explains to the interviewer that her father expects her to take care of practical tasks whenever one of them falls ill: The home carer had told my Dad that he had to take care of most of the mess at home to make room for a hospital bed for when my mom was discharged from hospital. And he had basically told the home carer: “Katja can do that”. And that's why she called me, to arrange for me to do it, because he wasn’t really able to. And that's what frustrates me […] It's overwhelming when I have such a bad relationship with my parents […] that they just say “Katja will do that, Katja does that”. It makes me so angry. […] I’m supposed to take care of everything. I had to talk to their landlord because they hadn’t paid their rent, I had to find their leasing agreement, send stuff to the municipality, speak on the phone… It was just everything, all at once. I couldn’t do that. I mean… I can’t (informant cries). (Katja, 34 years old)
Katja tells us that she used to self-harm and tried to commit suicide twice. She tells us that her parents’ behavior sometimes gives her the urge to self-harm again. Katja distanced herself from her parents earlier in life, but, at the time of the interview, she is tangled back in, partly due to being contacted by her father's home carer. Her story is just one example of many difficult childhood experiences described in our interviews. Like Katja's, Catherine's (34 years old) upbringing is characterized by physical and psychological violence: Interviewer: Was it physical violence or was it mostly threats, or…? Catherine: It's been both. Physical as well as psychological. Interviewer: And how is your relationship with your parents today then? Catherine: Well … I’ve been there for them both you know, and helped Dad with, you know with the alcoholism … I had to quit at one point where I shunned them, momentarily … And I say momentarily because he's admitted to hospital now, right? So, I’m back again, you know … But I had to have a break from it because it was too hard on me. I mean, I suffer from PTSD because of my childhood, so I’ve been through a long healing process … And I’m not done yet. But I’m there for him now because it's going downhill for him, so I wouldn’t want to sit back and regret things. (Catherine, 34 years old)
Catherine explains how helping her father always triggers her post-traumatic stress disorder (PTSD). She jeopardizes her own mental health because she fears feeling guilty in case her father dies. Kevin shows a similar pattern. He is being assessed for attention-deficit/hyperactivity disorder (ADHD), suffers from death anxiety, and is put under immense pressure every time his father is hospitalized as he turns into his father's “secretary”, to use his own words. Just like Catherine and Katja, he sacrifices his own well-being to help his father: And, I mean, it's hard to go on these hospital visits all the time, especially when you suffer from death anxiety yourself […] My anxiety is through the roof. It feeds my anxiety to sit there with him. On the opposite side, I find it really hard to not sit there (laughs). […]. (Kevin, 34 years old)
Adult offspring of patients with ALD often feel unable to leave their parent's side even when they feel the individual need to do so. One of the reasons for this is a contextual factor that presents itself in all our informants’ stories: the veil of secrecy, shame, and stigma surrounding AUD and mental illness. Dorit (54 years old)'s story is a good example that AUD is an isolating condition for the person suffering from it as well as that person's family. In our interview with Dorit, she recounts witnessing two of her mother's suicide attempts, the first of which happened when Dorit was about 11–12 years old: “I was the big one”, she explains, because her sister, Anne, was 5 years younger when they both had to grapple with the situation. Despite the violent episodes during childhood that several informants told us about, only a small number of the informants had previously been offered support such as therapy or family counselling. Several of them still to this day abstained from sharing their stories or grief with anyone except, perhaps, the selected few. Sisters Dorit and Anne give us a glimpse into how this pattern started in their early childhood: Interviewer: No one reacted? Dorit: No. They didn’t. Interviewer: Do you think anyone knew? Dorit: Yes I do … But my mom is really, I mean, really strong. It might not sound like it, but she is. And really stubborn. So, I don’t think anyone would be granted that access. But no one did anything. (Dorit, 54 years old)
Several informants recount asking adults for help when they were young, notifying teachers or family friends of their parents’ drinking problems, and nothing happening as a result. The secrecy continues into adulthood causing new problems, as explained here by Anne: It's very shameful for my mom so my children don’t even know about her illness yet. Maybe they figured it out, I don’t know, but it's really shameful for her. And that's why … maybe that's also why she's used me and my sister so much because we actually do know about it. She wouldn’t want to use her friends or anyone else to … get a lift to a doctor's agreement for example. (Anne, 49 years old)
The shameful feelings involved with AUD hinders their ill mother from asking anyone but her children for help. Anne later explains how she herself feels hindered from speaking to her friends and family in case they know someone who knows her mother. When the interviewer asks Anne where she lives, she hesitates to answer. This type of hesitation occurs in several interviews, and it confirms to us that some of them are speaking about a well-kept family secret for the first time. In this way, the secrecy is passed on to the next generation where it generates new types of burden and loneliness, as it deprives the adult offspring of resources that might otherwise be available to them (e.g., receiving help from a friend).
Juggling Moral Obligation to Family with Self-Determination
A recurring theme throughout all interviews is a sense of moral obligation towards the parent. Notably, this sense of moral obligation persists even in the absence of a sympathetic complementary relationship. Building on the qualitative study of Järvinen & Bloch (2017), we notice that several of our informants demonstrate a case of role-dependent sense of moral obligation that is fueled by guilt rather than sympathy. Mie describes this dynamic: Interviewer: […] How is your relationship with your Mom and Dad today? Mie: Well, I mean, it's good … It's good. Well, there's been periods where I’ve needed a break. But I mean, it's all kind of based on a sense of duty and guilt from my side. I rarely enjoy visiting my Mom … It's more that I know she enjoys it, and I know she's lonely and doesn’t have anyone else than us children and then my Dad. But it's not nice, you know, your Mom drinking and being sick. She's either talking in a frenzy or there's a bad smell or you’re finding bottles all over the place. And she can’t do a single thing on her own. So … So … It can be nice to see her but really, it's only like every fifth visit where you leave thinking “well that was kind of nice” (Mie, 30 years old)
“It's good” she says, a common knee-jerk response among our informants followed by a description of a very tense and uncomfortable atmosphere. Like other informants, Mie is aware that she overinvests considering her mother's behavior, but she does not intend to stop. Her moral obligation to keep going is fueled by what she describes as “a sense of duty and guilt” rather than sympathy. Kevin elaborates on this dilemma as well. Throughout his interview, there is constant ambivalence in his reflections on his role in his father's life: My problem is that I have to navigate all this … I already have a stressful job and you know, two kids and a wife. And now my parents have divorced, so I can’t visit both at the same time. So, it's twice the time. So, it's not like there's a lot of space left to help my father. But no one else does it. And you can’t just let them lie there, wheezing […]. It's a difficult balance, right? […] Let's say he had 5 years to live, right? It would also be … totally nuts to destroy your whole life for someone who wasn’t motivated to learn or was too lazy to change … You’re thinking “oh he might get better” and stuff … But there's a constant balance between when to back out and when it's too late to back out … You know? (Kevin, 34 years old)
When Kevin says it might be “too late to back out” he is referring to the deterioration he is noticing in his own mental health. Kevin, as well as the other informants, frequently speak about “choice” in a contradictory manner. Some of them frequently rationalize that they should be better at practicing their own individual choice. Drinking is their parent's choice and whether they choose to assist their parent when they fall ill or withdraw from them is their own choice. However, they experience limited agency in the situation. Mie includes the interviewer in her reflections on this topic helping us understand the complexity of having a seriously ill mother: I mean what would you do if you saw a stranger on the sidewalk, one who looked like they were dying? I’m pretty sure you would help them, right? What if you saw the same stranger next week? And the next week again … And the week after … And again, the week after … Would you stop calling 911? No, you would never do that, so what if that stranger was your Mom? (Mie, 30 years old)
Note that Mie's mother is not on the sidewalk where other people can see her; she is in her house or apartment, behind closed doors, where she only lets her children in. Like Kevin senses that something is wrong if his father does not see his messages throughout the day as illustrated in the introductory quote, Mie has an overdeveloped sense of the timing of her mother's ups and downs, a sensitivity cultivated by the “parentification” she experienced throughout childhood. Mie conveys to the interviewer that despite hypothetically having the “choice” to withdraw most individuals would refrain from doing if they were the only person capable of saving another person, especially a parent.
The limited agency the informants describe might be partly due to the social imaginaries of family and the moral obligation that is embedded in this imaginary reinforced by them being the only ones with a sense of when and where their parent will fall ill next. Furthermore, every time the parent is hospitalized, it comes with a new encounter with healthcare professionals who have certain automatic expectations of what “informal caregiving” entails and what “family” means, referring to a collective social imaginary. Several of our informants describe how talking to healthcare professionals always comes with additional caregiving tasks. In this way, the parent's continuous hospitalizations seem to supercharge our informants’ sense of moral obligation to enact the role of “informal caregiver” for their parent.
Although most informants have a positive attitude towards the medical staff, they describe not trusting the setup around their parent. Sofie (22 years old), gives us insight into how the hospital setting plays into this dynamic. She describes at length how she feels insufficient in the hospital setting but unable to withdraw. Medical staff reinforces this feeling by including her at a level that she is uncomfortable with, perhaps due to the busyness of the department, or perhaps as a well-meaning gesture to make her feel less powerless as a daughter: I feel like, almost every time they (the doctors) do their rounds, they start with “how do you think he is” or “do you think he's progressing or is it going the wrong way” where, I mean, of course I notice that yesterday he wasn’t able to speak, and today is the same, so it's not exactly better … but honestly, I don’t feel like that's my role. […] I kind of expect them to read up on it. […] Instead, I very much feel like I’m the one who has to call for help when he's strangling himself with some tube or pulling something [e.g., a tube] out of his throat … You know, this time, I was asking “damn it, can you please just help me here?” … I thought, if I weren’t here, what would happen then?” (Sofie, 22 years old)
Sofie spends many hours at her father's bedside and witnesses the busyness of the medical department. The sense of responsibility Sofie describes is undoubtedly overwhelming, especially for a 22-year-old, but medical staff do not seem to realize the adverse effects of involving her at that level. As a result, Sofie and our other informants overcompensate and risk burning out. While the offspring give care when the parent falls ill and healthcare professionals treat their parent's acute illness to the best of their ability, the toll it takes on the adult offspring is overlooked.
An Everlasting Liminal Phase?
Barrett et al. (2016) assert that reconnection following the liminal phase is not assured. They also note that, specifically, adult offspring of patients are more susceptible to remaining in the liminal phase without transitioning to the reconnection phase due to the combination of their closeness to the patient and the lack of decision-making authority on the patient's behalf. Our findings concur with this perspective and based on our own study propose that offspring of patients with alcohol-related illness are particularly exposed to this risk due to the nature of AUD and the secrecy that surrounds it.
Several of our informants have experienced repeated hospitalizations of their parents over many years. Most of our informants verbally distance themselves from their parent's course of action but find it challenging to detangle themselves from the practical responsibilities that follow. Mie (30 years old) exemplifies this. Mie's mother was first hospitalized when she was about 13 years old. The interviewer asks her whether her mother's latest hospitalization has imposed any daily tasks on her and her siblings. Answering the question, she describes what has become a routine practice for her: Mie: During this round … well, we’ve been to her home, and of course – or I don’t know if it's a given – but there was shit on the floor. Because she can’t keep it in, she can’t get to the toilet in time because she has difficulty walking. And there's stale food on the kitchen counter that must be fixed and cleaned, there always is when I’m at her place. She can’t do it herself. Bills must be paid. Dog must be walked. Kind of everything … […] Interviewer: And are you automatically the ones to do that? Or have you ever gotten help from others, or professionals? Mie: It's always been us. This one time my dad said he would pay for house cleaning, but I think she was there like twice and then my mom couldn’t stand it. […] She likes that it's her children who come over and do it. […] She calls almost every day and if you don’t pick up, you’re bombarded with guilt because you receive a bunch of nasty messages from her. […] Interviewer: And you tell me that this alcohol problem isn’t getting better, you kind of know this by now. But how do you see your own role then, going forward? Are you going to keep cleaning, cooking, visiting? Mie: Well right now, well yes, because if no one else does it, you know. […] But it's not because it's rewarding for me to visit her, not personally. But I know that it is (rewarding) for her because she has no one else. Interviewer: Did you tell anyone, for instance, professionals about this burden of helping her daily? Mie: No, because I simply don’t know who to talk to or where to go to. So, I haven’t, actually […] And I think, I haven’t done a whole lot about it, because then I would start a lot of things and people would spend their time on it and then, when it's all about to go off, the bitch doesn’t want them to come … I mean … She doesn’t want it anyway … And I could just say “well I’m not gonna do it either, you can just live in a pigsty then”. And she’ll literally just do that. That's where she's damn tough, she’ll just say “Oh fine then, I’ll just do that then”. So crude. […] And I can’t really do that to her either, you know. She’ll be sitting there, it's smelling everywhere because she doesn’t shower, there's old food and it's nasty all over. And her dog doesn’t get walked because she's unable to do that. I mean, it's hard not to help. (Mie, 30 years old)
Mie recognizes that ultimately the task will fall back on her irrespective of her attempts to seek assistance, illustrating the lack of resources that Barrett et al. (2016) argue is a significant barrier to reconnection. Mie's routine of cleaning, cooking etc. for her mother started when she was a young teenager. While the term “routine” might typically connotate a reconnection phase rather than a liminal one, in this instance it does not signify a means of reconnecting; rather, this routine represents an endless burden because her mother “has no one else”.
Most of our informants hold little hope for any lasting improvement of the situation although they can never know for sure. Even when it seems to be going well, an eerie sense of unease persists. Morten explains how he is always expecting the next crisis; a recurrent theme in our interviews: When she says she doesn’t drink you know that she's … well, drinking anyway. But in those times where she's not hospitalized, at least you get some distance from it, because well … there's a daily life where she's home, and everything's, you know, going “well”, in inverted commas. And then the times where she's been hospitalized it's more top of mind and something you’re thinking about a lot. But I honestly find it creepy when it's going “well” because you know that it's … it's really not […] I don’t even know what's worse because … I also think it's worse to pretend that something isn’t what it really is, I’d rather stop beating around the bush. At least you’d know what to count on and what to do based on that. (Morten, 28 years old)
All informants have parents who are so ill that their next hospitalization could potentially be their last which means that the awaited next crisis could range from something profoundly sorrowful such as the loss of a parent to “just another round” as described by Mie (30 years old). This helps explain why informants occasionally express frustration with their parent's resilience to their illness, as demonstrated here by Kevin: I hope there's a difference between what I believe inside and what I hope will happen. Of course, I hope he will stop drinking. And I hope he gets a long life and dies of natural causes. That's my hope, and it's a naïve belief that I have, you know? And then there's what I think (laughs) … And I’m afraid I think he’ll die sooner from the effects of his alcohol problem. So that's what I think. I think he's in such a poor state that something will come about and kill him. Whether it's his liver or something else, something fucking up his diabetes, I don’t know. But right now, I just think it's going to go that way within the next five years. […] Sometimes it would just be easier if he were dead, you know? (Kevin, 34 years old)
Surely, Kevin does not wish his father dead, but these frustrated words are a result of him, like most informants, having said “goodbye” more than once, and a response to the toll his father's illness is taking on his own life. Kevin and our other informants momentarily grieve their parent during hospitalization and then get them back again. On each occasion, their parent oscillates between states of life and death, transitioning from home to hospital and perhaps back again, always drawing the informants back into the liminal phase.
Discussion
The present study focused on the informal caregiving experiences of adult offspring of patients with ALD, both leading up to and during the time of their parent's hospital admission with ALD. First, we described the psychosocial statuses of our informants as seen through their own eyes, revealing that all informants had mental health issues that were worsening due to their parent's previous and current AUD as well as parental mental health problems. Second, we described the impact of internalized and institutionalized social imaginaries of family on the adult offspring's sense of moral obligation to give care to their parent (Taylor, 2004). We showed that adult offspring's sense of moral obligation was oftentimes fueled by guilt and a habit of being “parentified” which was reinforced when healthcare professionals imposed caregiving responsibilities on them during their encounter at the hospital. Third, we showed that adult offspring of patients with ALD experienced what is known as a “liminal phase” following the rites of passage framework (Barrett et al., 2016). Their liminal phase was not short-term or singular, and the event of the hospitalization was not a unique event; rather, it was typically a repetitive event that had happened several times over the course of years, and, if the parent survived this “round”, their adult offspring were anxiously waiting to see what the next “round” would bring. We learned that several informants felt like they were constantly awaiting the next crisis over very long periods of time instead of reaching a sense of “reconnection” with a normal everyday life.
As such, this study contributes to the branch of literature that focuses on the burden of affected others as relatives of people with AUD, in their own right, rather than as a resource or mechanism in their family member's AUD treatment (Orford et al., 2010; Shorter et al., 2024). Our qualitative findings resonate with previous studies that show the psychosocial stressors of being the offspring of a parent with AUD (Kelley et al., 2007; Moore et al., 2011; Järvinen, 2015; Järvinen & Bloch, 2017; Hellum et al., 2019; Frederiksen et al., 2023; Muir et al., 2023; Shorter et al., 2024). This study further highlights a specifically difficult time in their adult lives; namely, when their parent with AUD is diagnosed with a severe alcohol-related case of liver disease. Our qualitative findings illustrate how the severity of ALD, as well as the family background and narrative, play into the offspring's informal caregiving experiences. As such, the study emphasizes that informal caregivers are a diverse group of people dealing with a range of conditions some of which are the root cause of family dynamics that harm offspring as seen in this case of parents with AUD. Based on this notion our study refrains from automatically viewing family, especially offspring, as a resource in the treatment of patients with ALD and instead assesses each adult offspring's individual experience with giving care to their parent, remaining open to the possibility that caregiving can be as harmful to them as it is meaningful to others. In the Danish healthcare context, current policies encourage involvement of relatives by presenting them as valuable partners who can contribute knowledge about the patient and help ensure coherence in treatment trajectories (Capital Region of Denmark, 2025; Bedre Psykiatri, 2025). No clinical guidelines concerning next of kin of patients with AUD exist, but national, general recommendations (Danish Health Authority, 2016) explicitly highlight relatives as potential resources in both communication and care coordination, while also acknowledging that they may be affected themselves and require independent support. Our findings complicate this policy framing: adult offspring of patients with ALD did not necessarily experience involvement as supportive; for many, it intensified long-standing emotional burdens rooted in parentification and repeated crises. When viewed alongside existing policy, the results underline that involvement of next of kin cannot be assumed to be beneficial. Instead, guidelines should clearly recognize that some relatives are vulnerable and may be harmed by additional caregiving expectations. Thus, this article supports the notion that offspring of parents with AUD are offered support irrespective of their parent's course of action (Orford et al., 2010; Shorter et al., 2024). Along with the national cohort study by Jepsen et al. (2024), the present study highlights an important time and setting for reaching out to this overlooked group of informal caregivers (Selbekk, 2019): the hospital department where their parents with AUD/ALD are hospitalized. Due to the median age of adult offspring being around 32 years during the time of the parent's ALD diagnosis (Jepsen et al., 2024), many of them will be in the process of forming their own families (Statistics Denmark, 2024), which makes it even more important to reach them at that point in time. We suggest the hospital setting as a possible point of broader referral for family members rather than just the person with AUD (in line with Selbekk & Sagvaag, 2016; Selbekk, 2019) and encourage cross-sectoral collaboration and knowledge-sharing between hospitals, municipal addiction treatment institutions, and NGOs offering therapy and support for the target group. Involving other departments (e.g., the emergency department) might help identifying offspring sooner, as we know patients with AUD often have several hospital contacts leading up to severe liver disease (Askgaard et al., 2020). Given the absence of clear guidelines and established practices, qualitative and interventional research is needed to understand how such collaborative efforts can be organized, how communication across sectors can be strengthened, and how hospital staff can be supported in assessing the individual needs of adult offspring of patients with AUD/ALD and referring them to appropriate community or voluntary support services. Such interventions should also include training for hospital and community healthcare professionals in AUD and its potential consequences for affected family members. We advocate for an individual focus on the offspring of the patient (e.g., in line with Shorter et al., 2024). Our argument is not in opposition to offering better support for their parents. Instead, we argue that the two focuses must not be confused: adult offspring of parents with AUD also need individual support.
One limitation of this study is that we only talked to offspring of patients with ALD who were still in contact with their parents. Because several of our informants disclosed to us that they had previously broken off contact with the parent once or several times, it is reasonable to assume that many other offspring of patients with ALD have broken off contact more permanently. This study cannot speak on their behalf because we only reached adult offspring who had some level of contact with the parent and with the medical department. Furthermore, we only interviewed a small number of people via one specific medical department which obviously limits geographical representativity.
Conclusions
This qualitative study shows that adult offspring of patients with ALD are particularly at risk of worsening their mental health when taking on caregiving responsibilities for their parent. In their encounter with the hospital setting, institutionalized and internalized collective imaginaries of what family means put them in a position as the parent's caregiver, which hindered them from taking care of their own mental health. Most of the offspring that we interviewed had never been offered support related to their parent's illness, in their own right. Consequently, they stayed in prolonged liminal phases with very little practical help and emotional support, in which they never knew when their parent would be hospitalized or die from their condition. This prohibited the offspring from (re)connecting with a normal everyday life.
Based on our findings, we propose the following recommendations for healthcare professionals who encounter and engage with patients with AUD/ALD:
Recommendations for Hospital Staff
Refrain from imposing caregiving responsibilities on adult offspring of patients with AUD/ALD of any age, unless they invite you to do so.
Enter dialogue with offspring of patients with AUD/ALD, ask open questions about their relationship rather than assuming that the parent-child relationship is complementary.
Reach out to adult offspring of patients with AUD/ALD and present them with local support options that target them in their own right. Hospital departments might consider doing so by acquiring and handing out flyers.
Cross-sectoral knowledge-sharing might be beneficial for hospital departments that engage with patients with AUD and, for example, local support services with a focus on therapy for offspring of parents with AUD. Hospital departments might consider inviting psychologists or social workers from these types of services to do talks and arrangements on-site, both with a focus on knowledge-sharing professionally and inviting informal caregivers to learn more about support services.
Footnotes
Ethical Approval
The project was accepted by the Danish Data Protection Agency and written consent was obtained from all informants.
Author Contributions
AKKL was responsible for the first draft of the article. All authors contributed to the writing and editing of the paper, and all authors read and approved the final version of the manuscript submitted for publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Novo Nordisk Fonden (grant number NNF22OC0079565).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.