
Abstract
Keywords
Advances in healthcare and the efficacy of modern medicine mean that most people in high-income countries now have a greater life expectancy, with the majority living into their 60s (World Health Organization [WHO], 2015). In the European Union (EU), for example, more than one-fifth (20.8%) of an estimated population of 447.2 million, are aged 65 years or older, a long-term trend, evident in all EU Member States (Eurostat, 2022). Moreover, it is estimated that the proportion of over 65s in the whole of Europe will have almost doubled from 14% of the population in 2010 to 25% by 2050 (WHO, 2022). This rapidly ageing population presents one of the major challenges for health and social care systems throughout Europe, a challenge exacerbated by increases in alcohol misuse among older adults (Hallgren et al., 2009; Raninen & Agahi, 2020).
The “Baby Boomer” cohort of older drinkers, people born between 1946 and 1964 (now aged between 58 and 76 years), who are drinking more than previous generations, are a major factor in the increase in problem drinking among older people (Wang & Andrade, 2013). For instance, the Tromsø study (Stelander et al., 2021), which looked at the drinking patterns of 20,939 older adults (aged 66–99 years), over a 22-year period (1994–2016), reported a significant increase in alcohol consumption among older adults, particularly among women aged over 60 years. Raninen and Agahi (2020) similarly reported an increase in alcohol consumption in the period 2004–2107, in a large sample (n = 225,134) of older Swedish adults (aged 60+ years) and, again, particularly among women. This trend is not restricted to Norway and Sweden. In England, for example, between 2006 and 2018, there was almost a fourfold increase in the number of over 65s in treatment for alcohol problems, compared to a 37% increase among those aged 25–29 years across the same period (Public Health England [PHE]; cited in Drink Wise, Age Well, 2019). It should be noted, however, that only 12% of the people in treatment for alcohol in England, for example, are aged 60 years or older (PHE, 2020a).
The recent COVID-19 pandemic, however, has adversely affected the availability of treatment for older problem drinkers, with many specialist alcohol treatments having to be delivered remotely. This has meant that uptake has been low, because many older adults have difficulty engaging with online technology (Seddon et al., 2021). The impact of the COVID-19 pandemic on the increase in late-onset problem drinking cannot be underestimated. For example, after the first lockdown in the UK in 2020, there were an estimated 171,000 people aged ≥50 years with “probable alcohol dependence” (Rao et al., 2021, p. 1). In England specifically, the highest prevalence for consuming above the UK recommended 14 units of alcohol a week was among adults aged 55–64 years (PHE, 2020b). However, viewed from a broader European perspective, the UK and Ireland appear to be outliers, as 21 other European countries experienced significant decreases in alcohol consumption during the pandemic, across all age demographics (Kilian et al., 2021). In addition, COVID-19 lockdown restrictions and the availability of treatment varied across Europe; for example, in Sweden, who probably experienced the least restrictions, there was no change in the number of people seeking treatment (Andersson & Håkansson, 2022). Nonetheless, a survey of 66,000 people aged ≥50 years undertaken before the pandemic across 18 European countries, in which almost half of the participants were aged ≥65 years, classified one in five adults who drank as hazardous drinkers (Bosque-Prous et al., 2017).
Furthermore, the Royal College of Psychiatrists’ (Royal College of Psychiatrists [RCPSYCH], 2018) reported that existing services in social care settings, the criminal justice system, older people's mental health services and acute hospital settings do not have the specialist knowledge that is needed to cope with the biopsychosocial complexities that elderly alcohol misusers present with. Consequentially, the RCPSYCH (2018) and others (e.g., Crome & Crome, 2018) advocate bespoke services, where staff are trained with the “appropriate knowledge, skills and attitudes” to identify, assess and treat older problem drinkers (RCPSYCH, 2018, p. 4). Moreover, according to Kelly et al. (2018), more research is needed in primary care prevention, where elderly alcohol misuse often goes unrecognised, and where factors such as ageism and stereotyping can result in signs of alcohol misuse (e.g., changes in mood) being mistaken for other symptoms, such as age-related depression (Rao et al., 2016).
Although a considerable body of literature has investigated alcohol use disorder (AUD) and problematic drinking in the elderly generally (e.g., Gell et al., 2015; Moos et al., 2009; Wadd & Papadopoulos, 2014), a crucially important difference within this population has often been overlooked. That is, older problem drinkers are composed of two distinct subgroups: early- and late-onset. Early-onset drinkers have, in all probability, drunk excessively and problematically throughout their adult lives (Schonfeld et al., 1987; Zimberg 1978). Two-thirds of older problem drinkers are early-onset, and because they experience problematic drinking earlier in life, they are more likely to have engaged with alcohol services at an earlier age than their late-onset counterparts. In contrast, far less has been reported concerning the remaining third; late-onset problem drinkers are individuals who drank alcohol moderately for most of their lives (in some case not at all), who start drinking problematically later in life (McGrath et al., 2005; Van Montfoort-De Rave et al., 2017). In addition, the stigma, associated with alcohol-related problems can be a barrier preventing late-onset drinkers from seeking treatment and engaging with alcohol services (Keyes et al., 2010; Lancaster et al., 2017; Wadd et al., 2011). That said, late-onset drinkers are reported to have better treatment outcomes, more social resources, fewer alcohol-related problems and less psychiatric co-morbidity than early-onset drinkers (Holley-Moore & Beach, 2016; Wadd et al., 2011). It is, therefore, important for alcohol practitioners to better understand the distinctions between these subgroups and “the implications for treatment” (Wadd et al., 2011, p. 26).
As people age, they are increasingly likely to experience major events and stressors, such as losing a partner, retirement, cognitive decline, social isolation, and pain. Many late-onset problem drinkers use alcohol as a coping mechanism for such stressful events (e.g., Dauber et al., 2018; Emiliussen et al., 2017a; Wadd & Papadopoulos, 2014), many of whom cite a “meaningless life” as the reason for their excessive drinking (Immonen et al., 2011, p. 1169). These elderly “reactors” (Christie et al., 2013, p. 25) seem to be experiencing a phenomenon that Frankl (2014) has conceptualised as an “existential vacuum” (p. 61), a psychological feeling of emptiness. Indeed, a body of evidence points to an association between a lack of meaning and purpose in life and AUD/alcohol dependence generally (e.g., Chen, 2006; Hart & Singh, 2009; Henrion, 2002; Kleftaras & Katsogianni, 2012; Straus et al., 2019; Waisberg & Porter, 1994). Although a lack of meaning and purpose in life may have a role to play in late-onset drinking, the primary purpose of the current review is to investigate what psychosocial characteristics late-onset problem drinkers have in common. By identifying the shared psychosocial characteristics of this cohort of older problem drinkers, the review aims to contribute to a better understanding and, importantly, a greater awareness of the risk factors associated with late-onset AUD/problem drinking.
Methods
Currently, there is not a universally agreed cutoff age for late-onset AUD/problem drinking. Typically, previous reviews have used a 20-year range, between the ages of 40 and 60 years (Liberto & Oslin, 1995; Sorocco and Ferrell, 2006; Widner and Zeichner, 1991), with the most recent reporting a cutoff age of >50 years (Emiliussen et al., 2017d). Therefore, for investigative purposes, the current review defined ≥50 years as an approximate cutoff age for late-onset AUD/problem drinking. Because of its focus on answering specific questions within a narrow health-related context, the systematic method is the most suitable for the current review. A comprehensive systematic review identifies key areas of the subject under investigation (Randolph, 2009), enabling the researcher to gather sufficient material to produce a wide-ranging narrative synthesis. The current review seeks to answer the following questions:
What psychosocial characteristics have been reported in relation to people who have received treatment for late-onset AUD/problematic drinking? To what degree has a lack of meaning and purpose in life been reported in relation to people who have received treatment for late-onset AUD/problematic drinking?
Protocol and search strategy
Scoping search
A scoping search was performed on the title, abstract and subject/topic fields of five databases: BMC Systematic Reviews; The Cochrane Review Library; Library Plus; PsychInfo; and Web of Science. Library Plus is a University of Derby database that searches other databases, including the Allied and Complimentary Medicine Database (AMED), CINAHL Complete, Medline, PsychArticle, PsychINFO, and Psychology and Behavioural Sciences Collection. In addition, PROSPERO, a review registration database, was searched, to establish if similar reviews were in progress. The scoping review showed there were very few papers on the topic; the term late-onset was not in usage before 1980, and the papers that had reported on the phenomenon before 1980 (e.g., Droller 1964; Glatt et al., 1978; Rosin & Glatt, 1971, Zimberg, 1974), used language such as “heavy drinking in their later life” (Glatt et al., 1978, p. 64). Therefore, a broad timeframe was adopted for the main search to include studies spanning a 40-year timeframe between 1980 and 2020. Additionally, search terms needed to capture the approximate age range specific to the current review, so as well as “late-onset alcoholism” and “late-onset alcohol use disorder”, an appropriate number of synonyms for “elderly” were employed. Search terms for the scoping review were: late onset alcoholism OR late onset alcohol use disorder
AND
elderly OR aged OR older OR elder OR geriatric OR elderly people OR old people OR
older people OR senior
Inclusion and exclusion criteria
To help the current review remain focussed on its aims and reduce the risk of bias, pre-determined inclusion and exclusion criteria were used for the main search strategy (Table 1).
Study eligibility criteria.
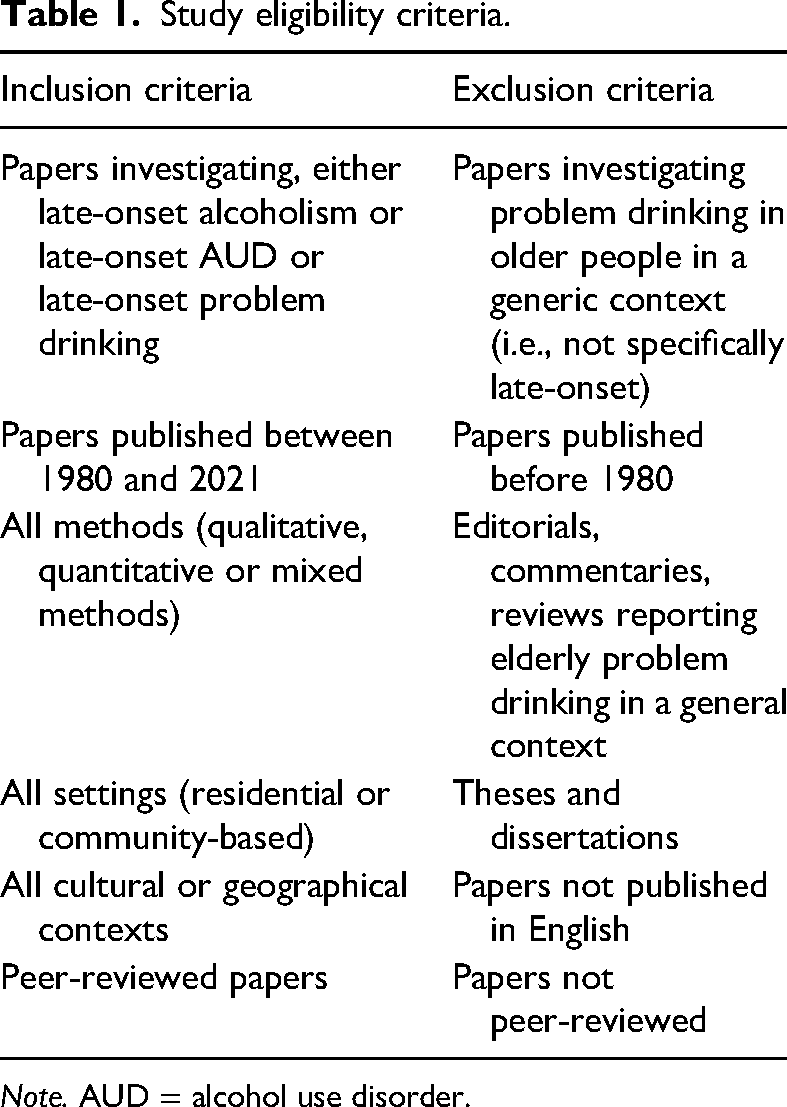
Note. AUD = alcohol use disorder.
Main search strategy
The scoping search highlighted a dearth of papers on the topic, encouraging a diverse search strategy, incorporating several methods. Using free-text search terms and the Boolean parameters AND, OR and quotation marks (“”), the primary searches were conducted on several databases: Library Plus; Google Scholar; Proquest; PubMed; Scopus; and Web of Science (Table 2).
Search terms used for main search.
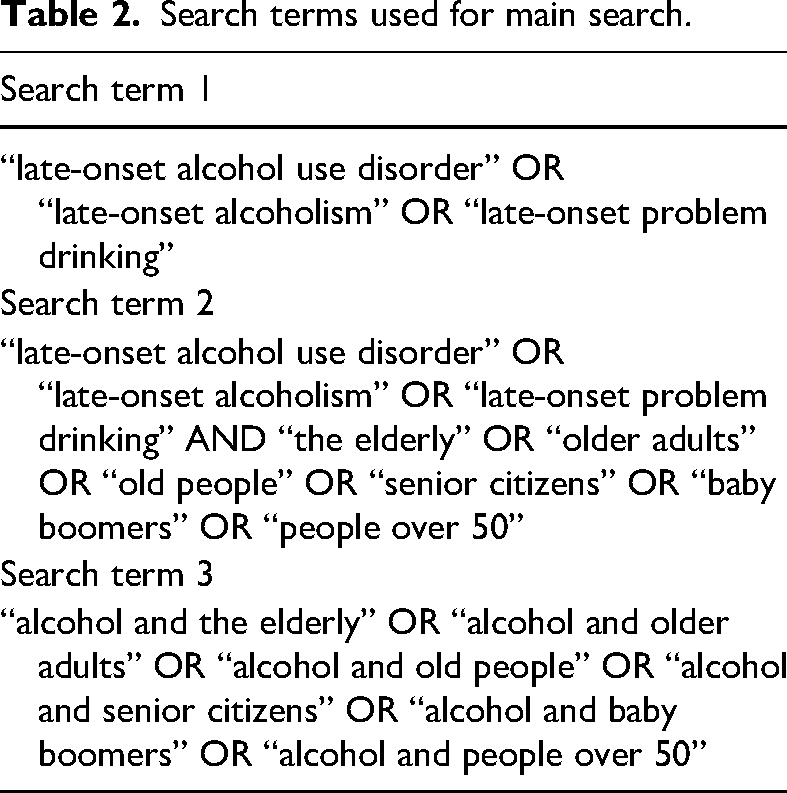
The three search term groups above were applied systematically to the following fields in each database: title; subject/topic; and abstract. The author field of each database was searched using the names of the key authors in the area as they became evident. Based on the inclusion and exclusion criteria, where database functionality allowed for it, the following limiters were applied: peer-reviewed journals; English language; and articles published between 1980 and 2020. The following totals shown for each database are the totals of the three search terms combined: Library Plus = 425; Google Scholar = 925; Proquest = 91; PubMed = 28; Scopus = 71; and Web of Science = 49.
Data screening
Primary screening
The screening strategy followed the Preferred Reporting Items for Systematic Reviews and Meta Analyses (PRISMA; Moher et al., 2009) framework (Figure 1). After removing duplicate studies, the primary search returned 1,595 papers. Based on a title scan, 1,514 articles were excluded at the initial screening stage. A total of 81 articles were retained based on title content (e.g., late-onset, late-life, alcohol use, alcohol consumption, older problem drinkers, older adults) and skim reading the papers’ abstracts. During initial screening, several seminal papers (22) were identified and obtained from other sources, increasing the total to 93. The reference sections of these 93 papers were scrutinised, and an iterative process of searching the reference sections of relevant papers (reference harvesting) was undertaken (Table 3), yielding a further 42 papers and increasing the number to 135 papers. After searching for “late-onset” throughout each paper, 70 more papers were excluded (Appendix 1a). The remaining 65 papers were further scrutinised, 39 of which were excluded at the final screening stage (Appendix 1b). Figure 1 describes the screening process.
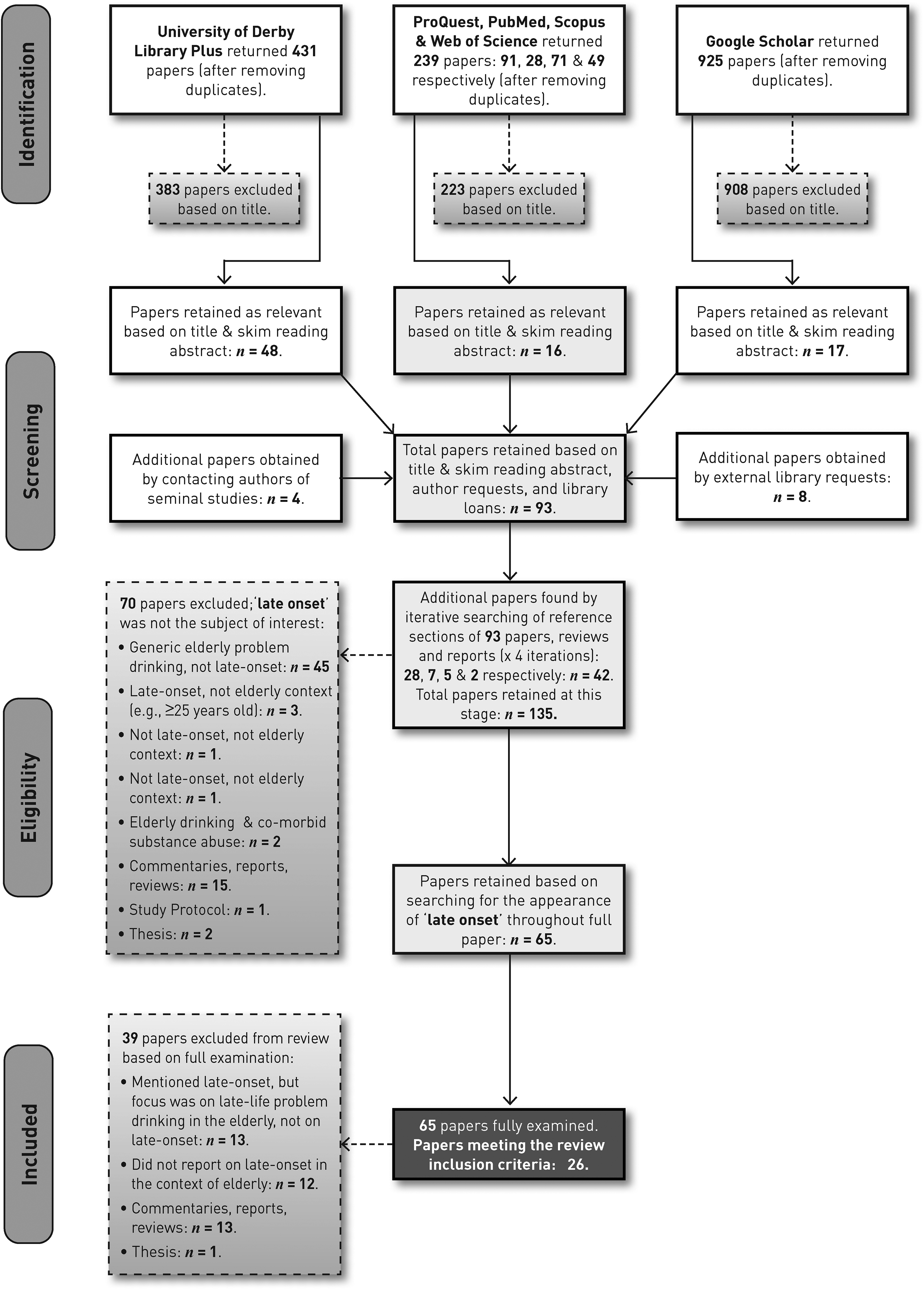
PRISMA flow diagram, adapted from Moher et al. (2009).
Reference harvesting: iterative stages.

Appraisal and data extraction
The final 26 papers that satisfied the inclusion criteria and were then checked against the Cohort Checklist of the Critical Appraisal Skills Programme (Critical Appraisal Skills Programme [CASP], 2020), 1 a tool that encourages researchers to take methodological biases into account. Finally, using a modified version of the JBI data extraction tool (Lockwood et al., 2020), each of the 26 studies was systematically appraised and scrutinised (Appendix 2), and tables summarising the main characteristics of the papers were compiled (Appendix 3), including the instruments/measures used by each study (Appendix 4). During the data extraction process, the homogenous and heterogeneous characteristics between studies were identified, informing the subsequent narrative synthesis.
Results
Context of included studies
Population and setting — Nine studies described samples of people who were receiving or had received treatment in a residential setting (study nos. 1, 2, 3, 15, 17, 19, 23, 24, 26). Nine studies included people receiving or who had received treatment in an outpatient or community setting (nos. 4, 5, 8, 10, 11, 12, 13, 14, 20, 25). Four studies included people with drinking problems who were or had been in contact with health services, though not in specialist addiction treatment programmes (nos. 6, 7, 21, 22). The population of one study (no. 9) was a mixture of people who had received treatment as either outpatients or inpatients. The population of two papers (nos. 16, 18) were a mixture of people who had received treatment in either an inpatient or outpatient setting, and people who had received no treatment.
Nationality, cultural context — Fifteen studies were carried out within the USA, four within Denmark, two within Germany, three within the Netherlands, and two within the UK.
Temporal context — A total of 14 studies were undertaken over a 9-year period between 1985 and 1994, and 10 were conducted between 2013 and 2019. Only two studies were carried out in the 19-year period between 1994 and 2013 (Schutte et al., 1998; Wetterling et al., 2003).
The defining characteristic of narrative syntheses is the use of text to summarise or “tell the story of” the findings from multiple studies (Popay et al., 2006, p. 5). Two factors support the use of a narrative synthesis: first, a lack of numerical data across the studies, preventing the collection of standardised effect sizes; and, second, if there is methodological heterogeneity across the reviewed papers. While most of the studies herein are cross-sectional, there are longitudinal and retrospective studies, and three are qualitative. In addition, outcome measures were inconsistent throughout, e.g., while some studies reported a follow-up outcome measurement, the majority did not. Taking these factors into account, a narrative synthesis is the most appropriate method of presenting the findings of the review.
Narrative synthesis
Investigative framework
The current review used an investigative framework comprising three defining characteristics: age of onset; gender differences; and psychosocial and mental health characteristics. In addition, the review investigated how meaning and purpose in life and treatment have been reported in the context of late-onset problem drinkers.
Towards a universal cutoff age for late-onset AUD/problem drinking
Many researchers in the current review (e.g., Christie et al., 2013; Schonfeld et al., 1987) agree that one-third of elderly problem drinkers are late-onset. Although the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association [APA], 2013) does not recognise late-onset as a subgroup within its AUD diagnostic criteria, it does state that “perhaps 10%” of all individuals diagnosed with AUD “have later onset” (p. 494). However, it can be difficult to detect late-onset AUD/problem drinking in older people. Stigmatisation associated with alcohol problems means that many older adults have great difficulty in accepting their drinking is problematic and, therefore, avoid seeking treatment (Hammarlund et al., 2018; Wadd et al., 2011). In addition, alcohol-related presentations are often mistaken for common age-related problems (e.g., falls, confusion, depression, etc.), or simply remain undetected by healthcare professionals (e.g., Cimarolli et al., 2018; DiBartolo & Jarosinski, 2017). Indeed, Finlayson et al. (1988, p. 767) suggested more than 30 years ago that “It is important for physicians to inquire about the occurrence of major life events such as retirement or loss of a spouse and to examine the patient's style of coping, including the use of alcohol”.
Therefore, it is important for clinicians and other health and social care professionals to understand (1) what the risk factors for late-onset drinking are, and (2) approximately when the onset of problematic drinking is likely to emerge. Although they are not the deciding factors for late-onset AUD/problem drinking, late-life events (e.g., bereavement, retirement, social isolation, etc.) are strongly associated with late-onset drinking, nonetheless. However, the inability to predict when such events are likely to occur can also make predicting a cutoff age for late-onset AUD/problem drinking more difficult, which may explain, in part, the considerable differences in how the cutoff age for late-onset AUD/problem drinking has been reported. By investigating this disparity, the current review moves a step closer to standardising an approximate age of onset, thereby informing health and social care professionals and others who are interested in the well-being of this vulnerable population. Tables 4 and 5 summarise how each study reported and categorises age of onset. It is worth noting that several studies in the current review conceptualised age of onset as a trichotomous variable (Adams & Waskel, 1991a, 1991b, 1993; Atkinson et al., 1990; Kist et al., 2014; Van den Berg et al., 2014; Van Montfoort-De Rave et al., 2017) rather than a straightforward dichotomous one, i.e., early- and late-onset.
How age of late-onset problem drinking/AUD has been determined and reported by the studies in the review.
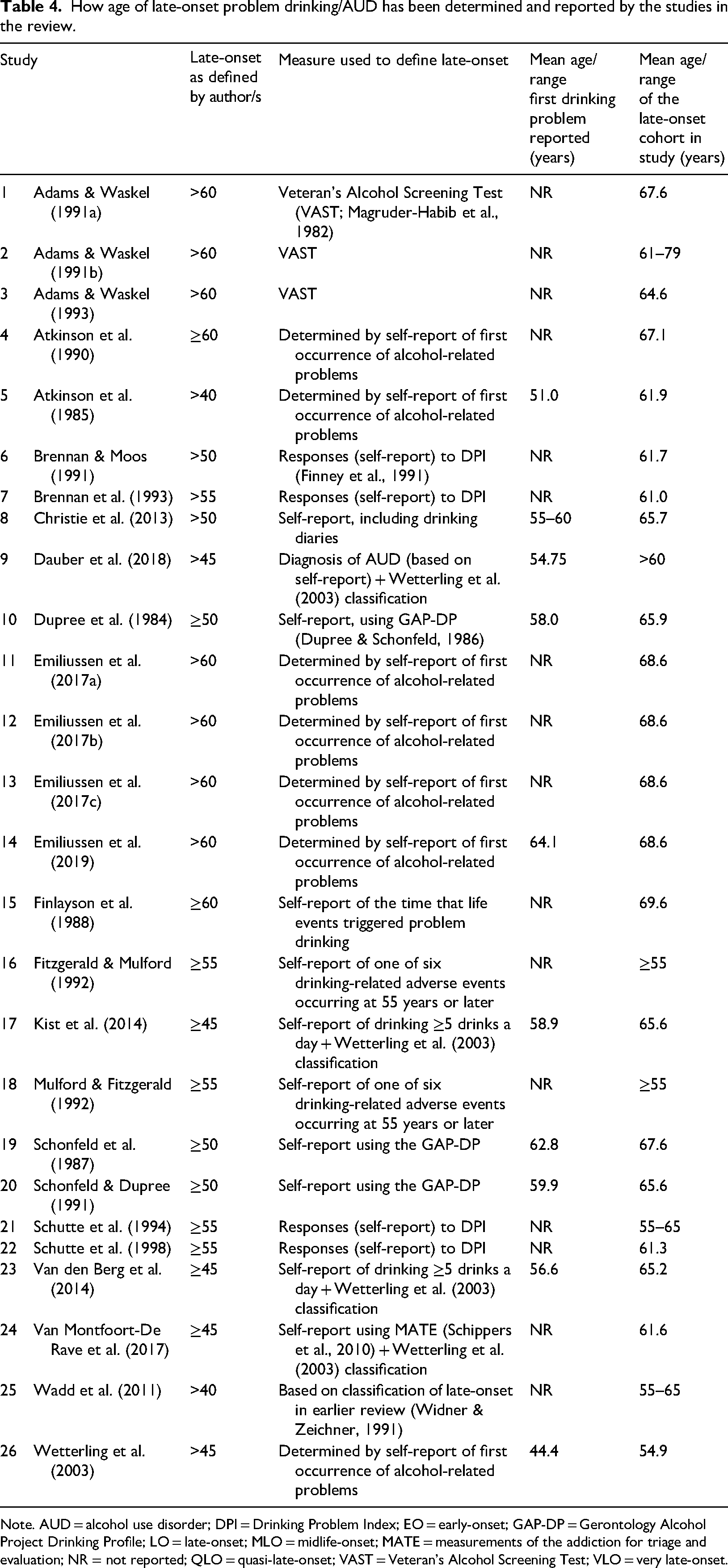
Note. AUD = alcohol use disorder; DPI = Drinking Problem Index; EO = early-onset; GAP-DP = Gerontology Alcohol Project Drinking Profile; LO = late-onset; MLO = midlife-onset; MATE = measurements of the addiction for triage and evaluation; NR = not reported; QLO = quasi-late-onset; VAST = Veteran's Alcohol Screening Test; VLO = very late-onset.
How the studies in the review categorise onset ages of problem drinking/AUD.
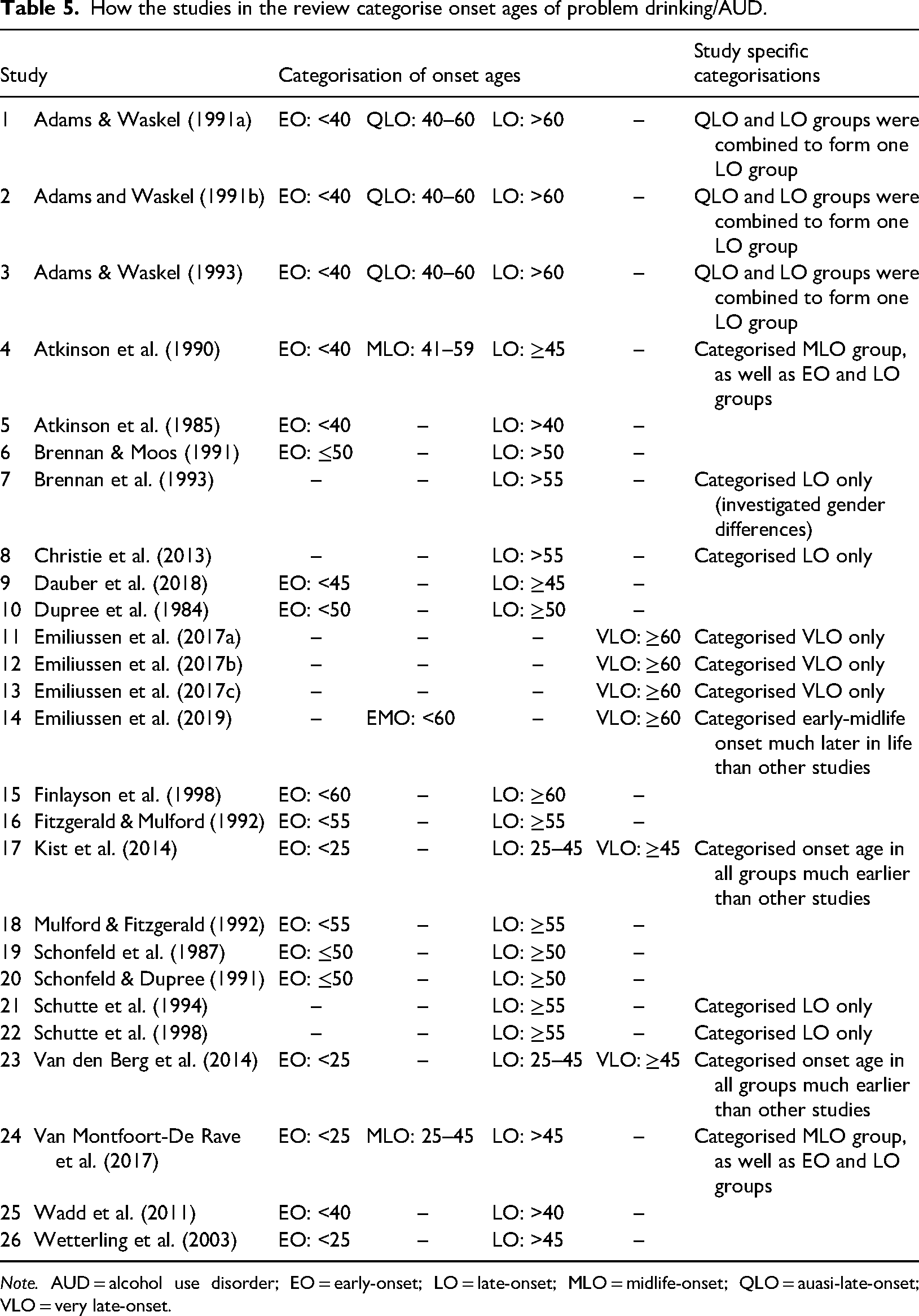
Note. AUD = alcohol use disorder; EO = early-onset; LO = late-onset; MLO = midlife-onset; QLO = auasi-late-onset; VLO = very late-onset.
Gender differences
It has become increasingly common for women to drink more heavily as they grow older (e.g., Epstein et al., 2007; Gell et al., 2015). According to the NHS (2016), 16% of women in England are drinking more than the recommended guidelines (14 units of alcohol a week), the highest prevalence (24%) being among women aged 55–64 years. Moreover, the rate of female alcohol-related NHS hospital admissions increased by more than 30% in the years between 2008–2009 and 2014–2015 (Office for National Statistics [ONS], 2016). In addition, women are more at risk than men of being adversely affected by alcohol. As they age, their vulnerability to gender-specific risk factors associated with excessive alcohol consumption increases (Epstein et al., 2007; Al-Otaiba et al., 2012), and although only 11 papers in the current review considered gender as a risk factor, significant differences were reported.
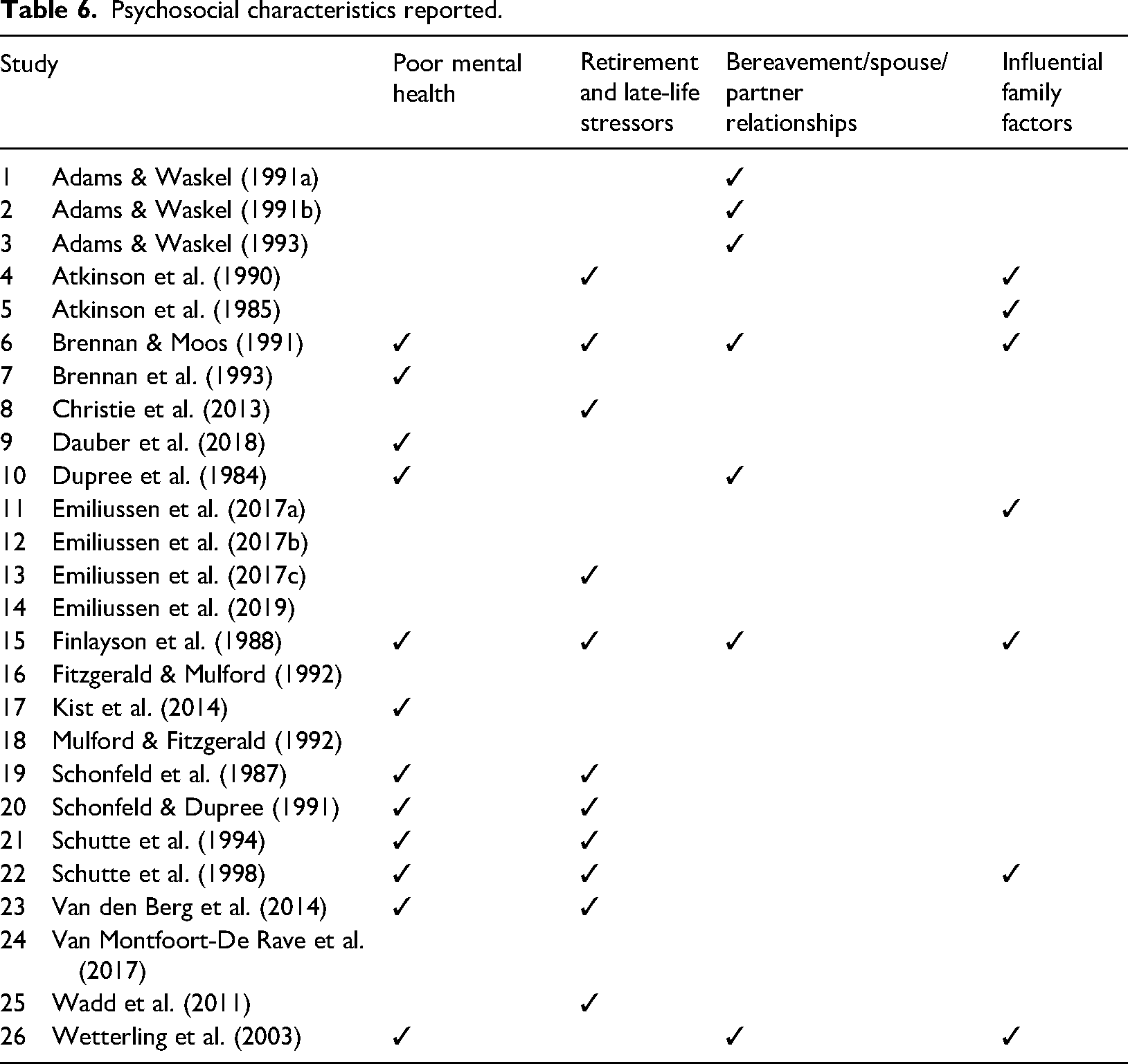
Van Montfoort-De Rave et al. (2017), for example, reported that, proportionally, there were more women than men among the late-onset drinkers compared to the early onset cohort in their study, as did Brennan and Moos (1991) and Brennan et al. (1993). The findings of these studies, who all harvested data from large samples (see Table 6), correspond to findings from earlier studies on elderly drinking in general (e.g., Blow & Barry, 2000), suggesting that the risk of women developing problematic drinking increases significantly with age. Moreover, the high prevalence of co-morbid alcohol misuse and mood disorders reported by Brennan and Moos (1991) was greater among women participants. Brennan and colleagues (1991) also reported that late-onset problem drinking women felt more stigmatised than men, as did Dauber et al. (2018) and Wadd et al. (2011), who suggest that stigma may act as a barrier to older women seeking treatment.
Psychosocial characteristics reported.
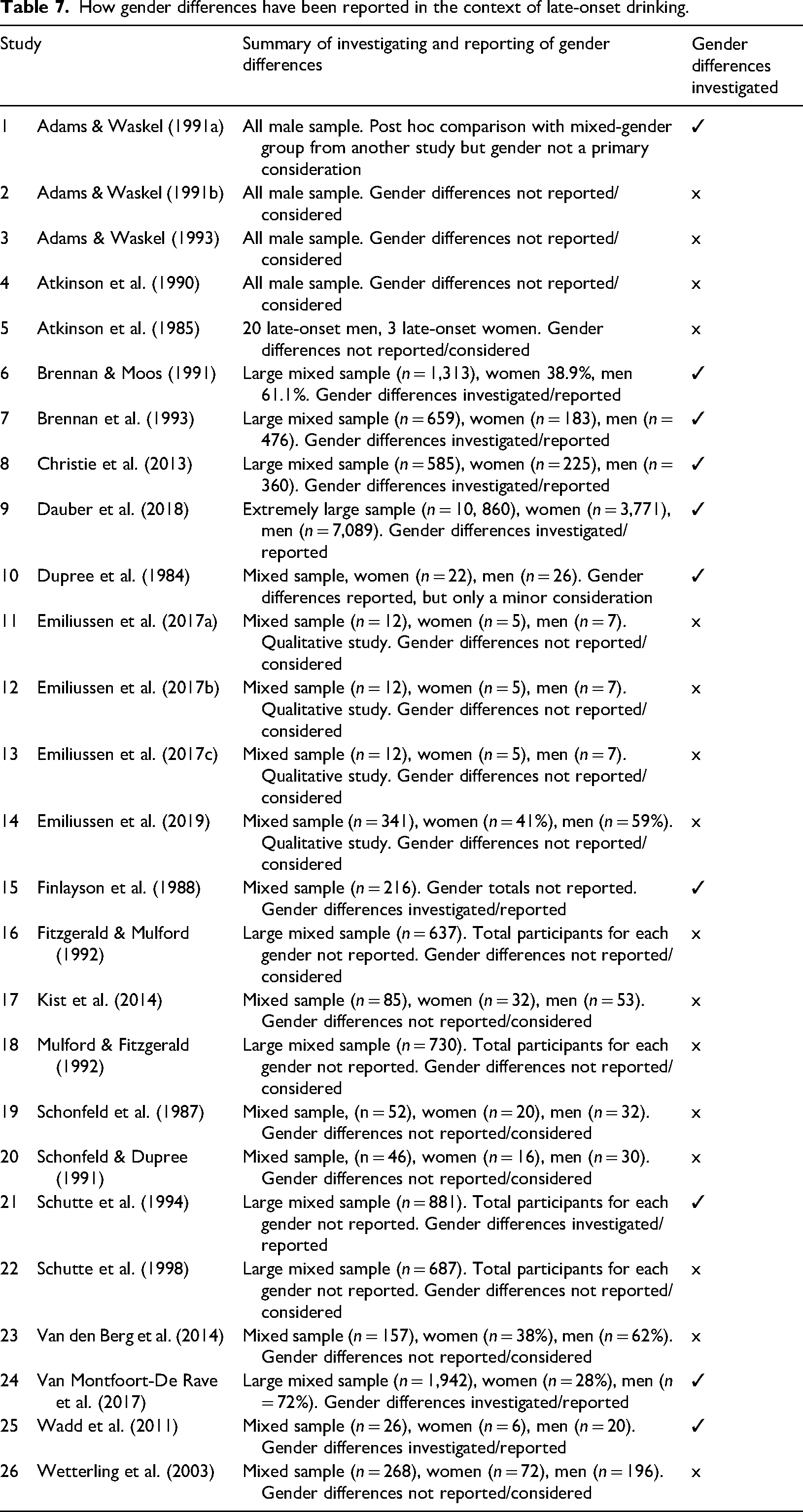
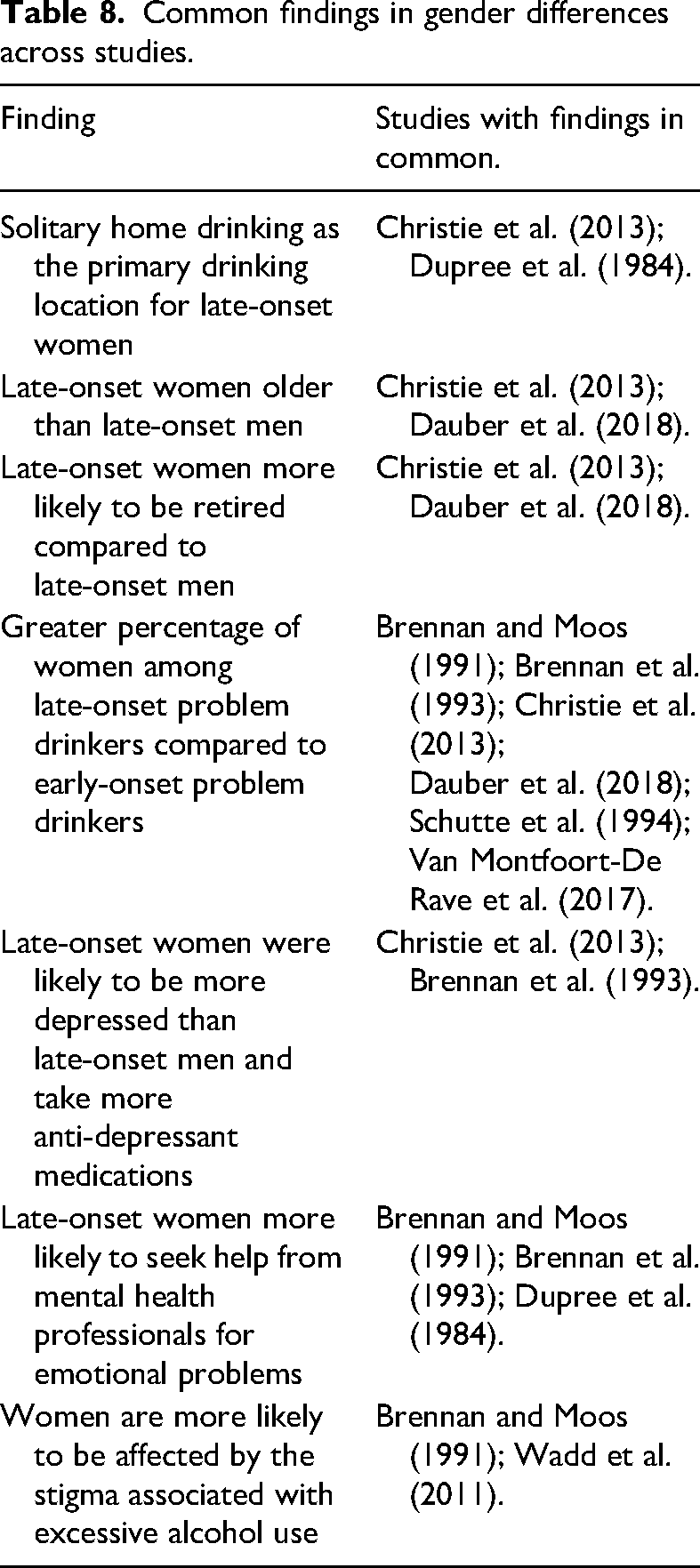
Brennan et al. (1993) additionally reported that late-onset problem drinking women were less likely to acknowledge their problems as being alcohol-related, viewing them instead as mental health or emotional problems. That said, Brennan et al. (1993) did find a higher prevalence of mental health problems (i.e., depression) among late-onset women compared to late-onset men. Christie et al. (2013) reported statistically significant gender differences for age, employment and marital status, finding that, typically, late-onset problem drinking women were older and are more likely to be retired than late-onset problem drinking men (73% and 57%, respectively). Reflecting current knowledge regarding later-life co-habitation, Christie et al. (2013) reported that more late-onset problem drinking men were married or co-habiting (57%), compared to late-onset problem drinking women (44%). In common with other studies, Dauber et al. (2018) also reported considerable differences in gender ratios between early- and late-onset problem drinkers (i.e., a greater proportion of women than men among late-onset drinkers compared to early-onset drinkers). The papers that investigated gender differences, along with the participant gender ratio of each study, are presented in Table 7 and summarised in Table 8.
How gender differences have been reported in the context of late-onset drinking.
Common findings in gender differences across studies.
Psychosocial characteristics associated with late-onset AUD/problematic drinking (including mental health)
The high prevalence of psychiatric co-morbidity found in this population (e.g., Charzynska et al., 2011; Rao, 2019; Rao et al., 2021; RCPSYCH, 2018; Searby et al., 2015) points to a complex relationship between the psychosocial characteristics of late-onset problem drinkers and poor mental health (Bruce, 2002; Emiliussen et al., 2017d; Shaw & Palattiyil, 2008; Ward et al., 2008; WHO, 2020). Indeed, 12 of the papers in the current review (almost half) reported psychiatric co-morbidity in their participants (see Table 9). Anxiety, depression and loneliness (Kobayashi & Steptoe, 2018) were the most often reported antecedents and reliable predictors of late-onset drinking (e.g., Dupree et al., 1984; Schonfeld et al., 1987; Schonfeld & Dupree, 1991; Schutte et al., 1994, 1998). In addition, findings of psychiatric co-morbidity were not limited to mood disorders and included organic brain syndrome and atypical organic brain syndrome (Finlayson et al., 1988). Moreover, Kist et al.'s (2014) investigations of cognitive dysfunction between early- and late-onset problem drinkers suggests that, regardless of the age of onset, all alcohol-dependent older people may have a degree of cognitive impairment, highlighting the negative impact of alcohol on the cognitive functioning of the ageing brain.
Treatment-related themes.
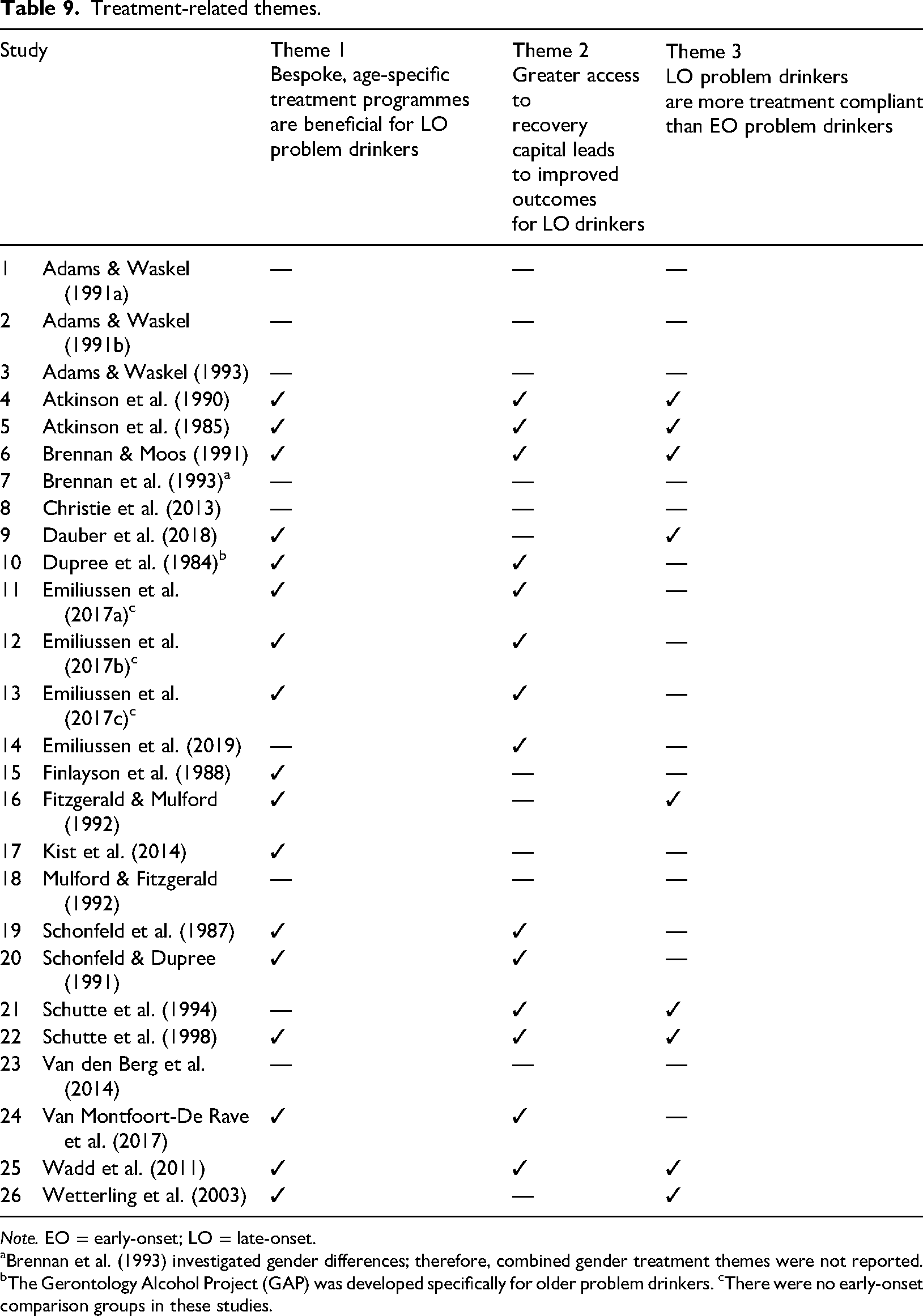
Note. EO = early-onset; LO = late-onset.
Brennan et al. (1993) investigated gender differences; therefore, combined gender treatment themes were not reported. bThe Gerontology Alcohol Project (GAP) was developed specifically for older problem drinkers. cThere were no early-onset comparison groups in these studies.
Several studies reported diminishing social networks and social resources, resulting from retirement, as major risk factors and reliable predictors for late-onset problem drinking (Emiliussen et al., 2017b; Finlayson et al., 1988; Schonfeld et al., 1987; Schonfeld & Dupree, 1991; Schutte et al., 1994, 1998; van den Berg et al., 2014). Finlayson et al. (1988, p. 766) suggest that the “statistically significant association” they found between late-life events and increases in alcohol consumption, in the late-onset cohort in their study, lends support to a stress-coping hypothesis as an explanation for late-onset problem drinking. Other major psychosocial characteristics associated with late-onset problem drinking included bereavement (spouse/partner), becoming a caregiver, chronic pain, financial worries and a lack of family support. Importantly, family support is associated with late-onset problem drinkers seeking treatment. Emiliussen et al. (2017a), for example, identified four psychosocial characteristics that motivated their late-onset cohort to seek help and enter treatment. Foremost among these characteristics was family pressure, which, in a positive light, can be viewed as a support mechanism, a social resource that is far less available to early-onset drinkers. Two other characteristics were health, and the need to be self-reliant and maintain personal agency over their lives, an indication of higher levels of abstinence self-efficacy in comparison to early-onset problem drinkers. Finally, late-onset problem drinkers who were receptive to treatment had an ambivalent and an open-minded attitude towards entering treatment.
How has meaning and purpose in life been reported in the context of late-onset AUD/problem drinking?
Of the 26 papers, only two reported explicitly on the construct: Adams and Waskel (1991a) and Emiliussen et al. (2017c). The participants in Adams and Waskel's (1991a) study completed the Purpose in Life test (PIL; Crumbaugh, 1968; Crumbaugh & Maholick, 1964); the PIL test is “a reliable and valid measure” (Crumbaugh, 1968, p. 80) developed to quantify the concept of existential frustration (Frankl, 1963, 2014). No significant differences in PIL scores were found between the early- and late-onset groups in Adams and Waskels’ (1991a) study. However, ad hoc comparisons made between the late-onset group and a group of older, non-problematic drinkers from an earlier study (Meier & Edwards, 1974) did show significant differences. From a qualitative perspective, the very late-onset AUD cohort (mean age = 68.5 years) in Emiliussen et al.'s (2017c) investigation experienced a lack of meaning and purpose in life, following a loss of identity, feelings they mostly experienced after retirement. Additionally, though not explicit, four studies highlighted the presence of boredom and apathy in their respective subjects/patients (Christie et al., 2013; Finlayson et al., 1988; Van Montfoort-De Rave et al., 2017; Wadd et al., 2011), which according to Frankl (1963, 2014) are psychological manifestations of a meaningless and purposeless life.
Treatment and recovery for late-onset drinkers: a synopsis
Discussion
Towards a standardised cutoff age for late onset AUD/problem drinking
This section considers the review's findings, in the contexts of health and social care policy, treatment and future research. Early in the review process, it became evident that there is a disparity across the literature, regarding how the cutoff age for late-onset AUD/problematic drinking has been defined. Therefore, determining an age range when late-onset AUD/problem drinking is likely to emerge was the current review's starting point. Studies of late-life events in various contexts, such as bereavement and depression (Bruce, 2002; Rosenzweig et al., 1997), stressors and problematic drinking (Brennan & Moos, 1990; Moos et al., 2005), and stressful late-life events in general (Holahan et al., 2005; Moos et al., 2006), suggest a time range of between 50 and 65 years of age. Based on a combination of that estimation, the variance in cutoff points presented in the papers in the current review (mean age = 52.69 years) and the participants’ self-reported age of onset (mean age = 56.79 years), the current review suggests that late-onset AUD/problematic drinking is likely to emerge approximately between the ages of 50 and 55 years. However, because some of the data sets in the reviewed papers are incomplete, the suggested cutoff age should be treated cautiously. For instance, only 10 of the 26 studies included the participants’ self-reported age of onset.
Recognising gender differences
The most common gender difference found was that there is a significantly higher proportion of women than men among late-onset drinkers compared to the same ratio among early-onset drinkers. Similar findings on older women drinkers in general (e.g., Blow, 2000; Cowart & Sutherland, 1998; Epstein et al., 2007; Green, 2006) support this, suggesting that the risk of women developing problematic drinking increases considerably with age. Furthermore, late-onset women tend to be older than late-onset men (Christie et al., 2013; Dauber et al., 2018). Interestingly, the review found that although women were less likely to seek treatment then men (due to stigma, shame and denial), when they did, they were more likely to engage with treatment and tended to be more treatment compliant than men. Indeed, several of the studies in the current review highlighted the need for gender-specific interventions/treatment. Moreover, from a social perspective, Dauber et al. (2018) recommended that “an integration of social aspects into treatment for older women may be useful” (p. 8), while Brennan et al. (1993) suggest that screening and treatment programmes “should be tailored more closely to the life circumstances of women with late-life drinking problems” (p. 781).
The need for a greater awareness of the psychosocial characteristics of late-onset drinkers
The presence of co-morbid alcohol dependence and mental health disorders in late-onset drinkers appeared more often than any other characteristic in the current review. The strong association between heavy alcohol use/dependence and poor mental health is well documented (e.g., Gerrits et al., 2015; RCPSYCH, 2018). The temporal order of the association is unclear; in all probability, alcohol misuse and poor mental health are mutually causative (Liang & Chikritzhs, 2011). For example, on one hand, poor mental health encourages the maintenance of heavy drinking (Bell & Britton, 2014), while on the other, the “harmful use of alcohol” is “a key risk factor for noncommunicable diseases and mental health conditions” (WHO, 2019a, p. 2). After mental health disorders, retirement was the most prevalent psychosocial risk factor reported. Although most older adults manage to maintain psychological stability and overall well-being after retirement, there are some who have difficulty coping with the new biopsychosocial challenges they are faced with (Henning et al., 2016). There are also those who simply may not be equipped with the resilience that is necessary in the transition to retirement (Murakami, 2021; Nalin & França, 2015); late-onset problem drinkers may fall into this category.
Other prevalent psychosocial risk factors included bereavement, pain, social isolation and exclusion, loneliness and boredom. Many of these risk factors tend to compound each other, i.e., bereavement can lead to loneliness and isolation, which, in turn, can lead to changes in drinking behaviour (Nicholson et al., 2017; Shaw & Palattiyil, 2008). Such risk factors often culminate in many older, late-onset problem drinkers regularly presenting at a variety of health and social care settings (e.g., primary care, social care, hospital settings and mental health services); all too often, however, they are not identified in these environments. This may be because of the individual's reluctance to talk about their drinking, which is due, in part, to stigma, shame and denial, or because of a failure on the part of professional practitioners to recognise signs of problematic drinking. Such oversights are often the consequence of poor training and/or fixed attitudes and assumptions about older people (Dar, 2006). Additionally, the diagnostic and screening protocols currently being used in health and social care are generic and inappropriate for an aging population. A greater awareness of the complex psychosocial risk factors associated with late-onset AUD/problem drinking, in tandem with adequate training, can enable professionals to recognise alcohol misuse in older adults. In this way, their elderly patients and clients can be treated more effectively. Indeed, some practitioners have called for “an age-specific approach to target more effectively, the complex needs of older people” (Shaw & Palattiyil, 2008, p. 181).
Meaning and purpose in life — a dearth in evidence
There is sufficient evidence to suggest that there is a relationship between a lack of meaning and purpose in life and alcohol dependence generally (see introduction). Moreover, re-discovering meaning and purpose in life is recognised as a key component of the recovery capital framework, a tool used by professional treatment practitioners to promote sustained recovery (United Nations Office on Drugs and Crime [UNODC], 2008), emphasising the importance of the relationship between meaning and purpose in life and problematic drinking. This relationship is evident in the process of recovery in mutual-aid support groups (Carroll, 1993; Galanter, 2007; Gomes & Hart, 2009; McInerney et al., 2021; Oakes, 2008), and recovery in general (Krentzman et al., 2015; Roos et al., 2015; Waisberg & Porter, 1994; White et al., 2006; WHO, 2020). The current review, therefore, sought to determine if and how this relationship has been reported. However, most of the papers in the current review did not investigate this dynamic; therefore, whether the association between meaning and purpose in life and late-onset problematic drinking is a significant one remains unclear.
Recommendations
Recognised as a considerable risk factor for problematic drinking in general, it is evident from the current investigation, that further research is needed to understand the role that meaning and purpose in life plays in elderly, late-onset problem drinking. Importantly, redefining the current terminology being used to describe late-onset drinkers should be a consideration. This is because the variety of labels currently being used impact negatively on late-onset problem drinkers. These labels are not only stigmatising, they are also restrictive and are not a true reflection of the elderly, late-onset population they aim to describe; they include, for example, late-onset alcohol dependence (e.g., van den Berg et al., 2014), late-onset alcoholics (e.g., Adams & Waskel, 1991a) and even late-onset alcohol abusers (Schonfeld et al., 1987). As such, many older problem drinkers are being overlooked because they do not meet the criteria for either a DCM-V (APA, 2013) diagnosis of AUD or the International Statistical Classification of Diseases and Related Health Problems (11th ed.; ICD-11; WHO, 2019b) diagnosis of alcohol dependence, yet they still experience the negative biological and psychosocial consequences associated with harmful levels of alcohol consumption (Dufour & Fuller, 1995). Therefore, for purposes of inclusivity, the term late-onset problem drinking is recommended in preference to purely diagnostic terminology.
Additionally, there is a dearth of research on treatment options and recovery pathways for late-onset problem drinkers, and further research is needed in the area. The current review has recognised that gender differences should be a major consideration for health and social care professionals when screening for late-onset problem drinking. Moreover, and considering the role that meaning and purpose in life may play in the context of late-onset drinkers, tailored treatment programmes for late-onset drinkers, should include “meaningful daily activities” (Van Montfoort-De Rave et al., 2017, p. 144). Mulford and Fitzgerald (1992, p. 609/610), however, have cautiously pointed out that, “it will be as difficult to develop a treatment that works for all elderly problem drinkers, as it has been to find one that works for problem drinkers of all ages”. That said, the current review presents a good case for developing interventions and treatments specifically for women with late-onset drinking problems.
Limitations
It is important to recognise that the review was limited to English language journals and the data were harvested and culturally situated in the “West” (i.e., Europe, USA). In common with all reviews, there is always the likelihood that the search terms and strategies used may not have returned some of the relevant papers in the area being investigated; this was evident in the current review, and several papers included in the review were only returned after using the iterative method of reference harvesting. Why such a substantial number of relevant papers (n = 42) were not returned during database searches is worthy of discussion. It may be the case that the search strategy was not thorough enough; that said, other reasons merit consideration. The technology on many databases, for instance, is not infallible, and items may not have been comprehensively indexed. It may also be that authors did not use the appropriate key terms to describe their papers. Therefore, reference harvesting and hand searches are recommended supplementary search methods. Returning to the importance of terminology, whereas the terminology in the current review aimed to be more representative of the late-onset problem drinking population, as recommended above, many of the papers in the current review only investigated populations with diagnostic labels (i.e., AUD, alcoholism). Additionally, as noted above, only a limited number of studies investigated the important role of meaning and purpose in life, and recovery from late-onset problem drinking.
Supplemental Material
sj-docx-1-nad-10.1177_14550725221143170 - Supplemental material for Characteristics of people who have received treatment for late-onset problem drinking and alcohol use disorder: A systematic review and narrative synthesis
Supplemental material, sj-docx-1-nad-10.1177_14550725221143170 for Characteristics of people who have received treatment for late-onset problem drinking and alcohol use disorder: A systematic review and narrative synthesis by Kevin McInerney, David Best and Ainslea Cross in Nordic Studies on Alcohol and Drugs
Supplemental Material
sj-docx-2-nad-10.1177_14550725221143170 - Supplemental material for Characteristics of people who have received treatment for late-onset problem drinking and alcohol use disorder: A systematic review and narrative synthesis
Supplemental material, sj-docx-2-nad-10.1177_14550725221143170 for Characteristics of people who have received treatment for late-onset problem drinking and alcohol use disorder: A systematic review and narrative synthesis by Kevin McInerney, David Best and Ainslea Cross in Nordic Studies on Alcohol and Drugs
Supplemental Material
sj-docx-3-nad-10.1177_14550725221143170 - Supplemental material for Characteristics of people who have received treatment for late-onset problem drinking and alcohol use disorder: A systematic review and narrative synthesis
Supplemental material, sj-docx-3-nad-10.1177_14550725221143170 for Characteristics of people who have received treatment for late-onset problem drinking and alcohol use disorder: A systematic review and narrative synthesis by Kevin McInerney, David Best and Ainslea Cross in Nordic Studies on Alcohol and Drugs
Supplemental Material
sj-docx-4-nad-10.1177_14550725221143170 - Supplemental material for Characteristics of people who have received treatment for late-onset problem drinking and alcohol use disorder: A systematic review and narrative synthesis
Supplemental material, sj-docx-4-nad-10.1177_14550725221143170 for Characteristics of people who have received treatment for late-onset problem drinking and alcohol use disorder: A systematic review and narrative synthesis by Kevin McInerney, David Best and Ainslea Cross in Nordic Studies on Alcohol and Drugs
Supplemental Material
sj-docx-5-nad-10.1177_14550725221143170 - Supplemental material for Characteristics of people who have received treatment for late-onset problem drinking and alcohol use disorder: A systematic review and narrative synthesis
Supplemental material, sj-docx-5-nad-10.1177_14550725221143170 for Characteristics of people who have received treatment for late-onset problem drinking and alcohol use disorder: A systematic review and narrative synthesis by Kevin McInerney, David Best and Ainslea Cross in Nordic Studies on Alcohol and Drugs
Footnotes
Data availability statement
The data generated during and/or supporting the current review are available in the SAGE repository.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.