
Abstract
Background and aims:
Problematic internet use (PIU), and kindred concepts such as internet addiction (IA), make up a growing research field, partly due to the suggested inclusion of internet gaming disorder in a future DSM-6 as well as the fact that gaming disorder is on its way to being included in the ICD-11. Conclusions from research are far from unified. This study aims to synthesise the research field of problematic internet use/internet addiction/gaming disorder, with a focus on the reporting of prevalence and change.
Methods:
Longitudinal studies of PIU/IA formed the basis for a scoping review. Systematic searches of Web of Science, Scopus and Proquest, for peer-reviewed and published articles based on empirical data collected at a minimum of two time points for studies, and with an end point set at 2017, led to the inclusion of 97 studies. Endnote X7 was used to organise the results and NVivo 11 was used for synthesising the results.
Results:
Analyses focused on prevalence and change. Findings show variation among measures and prevalence as well as in reported outcomes relating to social life and other problems. Most studies reported relations between PIU/IA and other problems in life, but no specific time order could be established. Furthermore, many studies did not present data on prevalence or change even though using a longitudinal survey design.
Discussion and conclusions:
In summary, the research field is plagued by a lack of consensus and common understanding, regarding both measures, perceptions of the problem, and findings.
Ever since the internet began revolutionising work, social life, leisure time and communication, it has been met with both optimism and concerns. Some people have a hard time limiting their use, to the extent that it influences their lives negatively. This has sparked a wide field of research, ranging from psychology and sociology to neurobiology. Several labels have been used to describe the problem, of which internet addiction (IA), problematic internet use (PIU) and gaming disorder are among the most common.
There is no universal consensus about the definition of addiction (Room, Hellman, & Stenius, 2015), but Heather (2016a) describes the concept well through its most basic features: as a struggle in which one keeps having trouble quitting a repeated behaviour, despite awareness of harmful consequences, and where the repeated behaviour is guided by disordered choice (p. 465); positioned somewhere in between the voluntary and the involuntary, coming both from inside the individual and as a reaction to external structures. This simple definition leaves room for explanations on social as well as psychological or biometric levels and includes trouble quitting, repeated behaviour and harmful consequences/problems, as its main pillars.
The term internet addiction was established by Young (1998a) to describe many types of excessive internet use, but has largely been replaced by more specific definitions, with gaming as the focal point of parental worries and researchers’ interest (Bergmark & Bergmark, 2009). This problem was picked up by the two arguably most influential organisations in the field of psychology and mental disorders. In the most recent edition of its Diagnostic and statistical manual of mental disorders, Fifth Edition (DSM-5), the American Psychiatric Association (APA) presented internet gaming disorder as a possible future inclusion as a non-substance-related addictive disorder, given that it be supported by enough good research (APA, 2013). The World Health Organization (WHO) went further, and introduced gaming disorder in the latest edition in its International Classification of Diseases, 11th revision, ICD-11 (WHO, 2018). In the DSM-5, internet gaming disorder is described as an addictive behaviour, in line with Young’s (1998a, 1998b) ambitions. Similarly, it is classified in the ICD-11. Even though some details about the inclusion in the ICD-11 are yet to be revealed, and the term addiction is avoided, the WHO also adapts criteria that are usually associated with diagnosing addiction (WHO, 2018).
The development of defining problematic gaming as an addictive disease has been met with criticism, where some experts argue that labelling this problem as an addiction, and the inclusion in the manuals is premature, atheoretical and lacking empirical evidence to support it (Van Rooij et al., 2018). One of the core aspects of addiction is that it is persistent (Heather, 2016b), meaning that one does not stop behaviour (more than momentarily) even when aware of negative consequences that arise. Key to examining persistence is using longitudinal study designs, allowing researchers to follow individuals for a longer period of time. Although some research on problematic internet use does assess persistence, results are inconclusive. 1
Systematic reviews are often used in order to target a research field in the search for, e.g., evidence-based measures and interventions. For an unarticulated field such as “problematic internet use”, such a review tends to result in an overload of hits/studies to include. The research field of problematic internet use has exploded during the last decade and resulted in many, many studies of varying value for conceptual development (see, e.g., Stensson, 2015). Techniques for scoping reviews have later been developed (Arksey & O’Malley, 2005), making possible scans of more “elusive” research fields such as ours. In order to further approach a fruitful depiction of measures and eventual relationships to other life problems, a limitation to only include longitudinal studies in such a review seems like a good strategy.
The aim of this scoping review (Arksey & O’Malley, 2005; Peters et al., 2017) was to present a map of longitudinal studies on problematic internet use. Particular interest will be devoted to the reporting of prevalence and change in problematic internet use. The WHO (2018) and APA (2013) single out gaming as its main focus, while terms such as internet addiction or problematic internet use cover several types of excessive behaviours that are mediated by the internet or computers, including gaming but also including social media use and other types of computer-specific behaviour. This review sets out to examine both gaming and general internet use. As a decision from the APA still lies ahead, the call for more research on these matters is still an open call; research aiming at more clarity and understanding of these matters should continue to be prioritised.
Survey of the field
Although the WHO (2018) and APA (2013) both single out gaming as a main focus, it is predated by such umbrella terms as IA or PIU, covering several types of excessive behaviours that are mediated by the internet or by computers, including, but not limited to, gaming. Not all excessive or problematic internet activities are alike (see, e.g., Chou, Condron, & Belland, 2005; Pawlikowski, Nader, Burger, Stieger, & Brand, 2014; Starcevic & Billieux, 2017; Van Rooij, Ferguson, Van de Mheen, & Schoenmakers, 2017). Identifying idiosyncrasies is paramount for a proper understanding and handling of the problem. Therefore, this review sets out to examine gaming as well as general and other problematic types of internet use. The term PIU is predominantly used in an attempt to avoid prematurely narrow definitions, thus allowing for the whole spectrum of problems. If other terms are used, this is to correctly reference another author’s choice of label.
One debated issue is which level of prevalence that can be expected: what percentage of a total population suffers from problematic internet use? Which of course is also dependent on context, such as internet density. In a review of trends in prevalence of internet gaming disorder during 1998–2016, Feng, Ramo, Chan, and Bourgeois (2017) found it to range between 0.7–15.6%, mostly including samples from Europe, Asia and North America (n = 27 studies). Different sampling techniques were applied and studies differed in demographics, scales and cut-offs, making it hard to make straight comparisons between studies. However, prevalence was not higher in studies with data collected earlier in the time period than data collected later. Since internet density was on a steady rise during that time period, one could have expected an increase in problematic use. Consequently, in a review of epidemiological studies of internet gaming disorder, Mihara and Higuchi (2017) found prevalence to range between 0.7% and 27.5%. The authors also accredit the large differences to the variety of methodologies, and argue that much surrounding the problem is still uncertain.
Another debated issue is whether overuse of, e.g., gaming leads to problems, or if problems lead to an “escape” into game worlds, i.e., as a coping strategy for life problems (Ballabio et al., 2017; Kardefelt-Winter, 2014). The time order is not established, for this more research is needed, but some research describes this in terms of being a vicious circle (King & Delfabbro, 2018) without clear entry or exit. One perspective on this is that PIU may act as a mediator for other problems, so that instead of being an isolated phenomenon, it may function as an escape from other problems, such as anxiety or life dissatisfaction (Douglas et al., 2008; Griffiths, 2008; Kuss, Griffiths, Karila, & Billieux, 2014). Furthermore, De Leo and Edelgard (2013) suggest that PIU is more associated with depression and being socially anxious than is substance misuse. In line with this perspective, Kardefelt-Winther (2014) proposes a focus on motivations, arguing that they mediate between psychosocial well-being and PIU. Kuss and Griffiths (2012) identified dysfunctional socialisation and personal dissatisfaction as risk factors for PIU; and among high-frequency online gamers, conscientiousness and extraversion appeared as protective factors against developing problematic behaviour (though it is hard to assess causality and direction of the correlation).
In a cross-disciplinary review on video game addiction, Hellman, Schoenmakers, Nordstrom, and van Holst (2013) cover research from social and cognitive as well as theoretical backgrounds, arguing for the concept video game addiction due to its similarities with other, more established addictions. Additionally, they acknowledge that magnitude, persistence, social costs and symptoms are still under-researched and may differ from those of substance addictions. Finally, the authors propose a de-medicalisation of addiction, due to their internal similarities being greater than with other diseases.
There is no agreed-upon gold standard for measuring or labelling PIU, partially due to insufficient knowledge and its status as not yet included in influential diagnostic catalogues. Systematic reviews (Bergmark, Stensson, & Bergmark, 2016; Kuss & Griffiths, 2012) unveil a lack of common definitions and a widespread use of non-representative or convenience samples as well as confirmatory approaches, thus raising questions about the validity of inference and results. In an effort to identify all existing measures, Laconi, Rodgers, and Chabrol (2014) found 45 different tools and attempted to evaluate the different scales, mainly through construct validity: relating the scale at hand to other measures, expert opinions and other variables considered relevant to the problem, such as depression and frequency of use. In a systematic review of epidemiological research and IA during the years 2000–2013, Kuss et al. (2014) found 21 different assessment instruments and cut-off criteria, along with scattered results. Among the critique against existing scales was the lack of a temporal dimension measuring persistence, and that conceptual frameworks were atheoretical and based on a priori criteria. Kuss and Griffiths’ (2012) review revealed that the diagnostic frameworks were most commonly based on criteria for pathological gambling, substance dependence or a combination of both. Tokunaga and Rains (2016) identified three main traditions of thought about the origins and fit of PIU: (i) a pathology related to substance dependence, (ii) an impulse control disorder much like pathological gambling, and (iii) a social phenomenon as an effect of deficits in offline relationships. Studies based on the relational resource deficit perspective found weaker associations between PIU and time spent online, as well as for loneliness and depression, partially through omitting questions about tolerance and withdrawal. Thus, different measures and preconceptions produced different results (Tokunaga & Rains, 2016).
Methods
Systematic reviews are often used to establish consensus in research field quests, e.g., for evidence-based measures and interventions. For an unarticulated phenomenon like PIU, such a review tends to result in many hits/studies to read, while very few remain for main analyses after scrutiny. Also, as the research field covering PIU is both wide and conceptually weak, and adding the multitude of studies claiming relevance for the field, a scoping review was decided to be best practice in order to settle on both concepts and measures. Scoping review techniques have been developed for wider research questions, still employing a rigorous database search but with more generous inclusion criteria (Arksey & O’Malley, 2005; Daudt, van Mossel, & Scott, 2013; Levac, Colquhoun, & O’Brien, 2010; Peters et al., 2015).
The process of identifying relevant studies for the review involved systematic searching of electronic databases as well as hand-searching reference lists and key journals. A heavy emphasis was put on searching electronic databases, which produced the vast majority of articles included in the study. Although grey literature is often proposed for scoping or systematic reviews (Daudt et al., 2013), this study specifically aimed to find general traits of the research field. The “landscape” of a research field is a priori defined by its publications, defined as peer-reviewed research in academic journals. Thus, grey literature was by default excluded.
To enhance the breadth of results, three internationally recognised databases were used: Web of Science, Scopus and Proquest. 2 Preliminary searches indicated that these three databases delivered results that were sufficiently unique for all to be included. The final search string listed all keywords and synonyms we could identify in previous research, plus terms indicating a longitudinal study design.
The search had no lower time limit, but an upper time limit was set at 2017. The articles had to have been published in a peer-reviewed journal (excluding conference papers, book chapters, debate articles) as proper studies and contain their own empirical analysis of data collected at a minimum of two time points. Studies focusing on brain structures and neural responses were excluded, as were treatment studies; for although covering the same topic, these represent a separate research field warranting their own reviews, with separate criteria. Studies focusing on gambling and sexual behaviour on the internet were also excluded, as they form separate research fields that are older than the internet, and are generally considered non-internet-specific behaviours (Pawlikowski et al., 2014; Starcevic & Billieux, 2017).
The software Endnote X7 was used to organise the results. The search rendered a total of 744 hits (see Figure 1). After removing doubles, reading titles and abstracts, hand-searching in three journals (Addiction, Computers in Human Behavior and Cyberpsychology & Behavior) as well as reference lists of other reviews (Anderson, Steen, & Stavropoulos, 2017; Feng et al., 2017; Kuss et al., 2014; Mihara & Higuchi, 2017), a corpus of 181 articles remained which were read in full text, resulting in 97 studies. A sample 10 of these studies’ reference lists were read to find more studies, but yielded no results. For extracting data on Outcomes and key findings, as recommended by Levac et al. (2010), a content analysis approach (Lundman & Hällgren Graneheim, 2012) was applied, using the computer program NVivo 11 to synthesise the results. Due to the wide scope of the review, double publication was accepted if the studies’ analyses were distinct from each other. However, it is accounted for in Table 1.
Studies included in the review.
Note. BAM-VG = Behavioral Addiction Measure-Video Gaming; CIAS = Chen Internet Addiction Scale; CIUS = Compulsive Internet Use Scale; CSAS = Computerspielabhängigkeitsskala (Eng. Video Game Addiction Scale); DSM-IV = Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition; GAS = Game Addiction Scale; GPIUS = Generalized Problematic Internet Use Scale; GIU = general internet use; IAT = Internet Addiction Test; IGDS-SF9 = Nine-item Internet Gaming Disorder Scale Short Form; IU = internet use; LC-PIU = Lifestyle Changes in Regard to Problematic Internet Use; MPOGQ = Motivation to Play in Online Games Questionnaire; MPPUS = Mobile Phone Problem Use Scale; MPU = mobile phone use; N/A = not available; PIU = problematic internet use; PVGU = Pathologic Video Game Use; SAMNCC = social app/media, networking communication, chat; VAT = Video Game Addiction Test; YDQ = Young Diagnostic Questionnaire.
* Children < 10, Adolescents 15 +/- 4 yrs, Young Adults 18–24, Adults 18+, All ages.
Search process.
Results
The first study found measuring PIU was published in 2006. 3 Studies per year started to increase after 2009, seemingly levelling off around 2016 (Figure 2). The most used research design is the survey, applied in 93 studies, while four utilised other types of design (mixed methods, app use data, qualitative interviews, experimental design). Note that the intention of this scoping review was to assess longitudinal research, not to assess all available treatment studies, of which there are probably several not included in this review.
Published longitudinal studies on problematic internet use, 2006–2017.
The main area of interest, comprising 65 studies, is general internet use, representing studies that use broad definitions and measurements, such as IA or PIU. The second largest category first appears in 2011 and comprises 28 studies on gaming. Seven studies focus on the social aspects of PIU such as social app, social media, social networking, communication and chatting, while three studies aim mainly at mobile phone or smartphone use. Six studies focused on more than one topic and are thus counted twice.
The duration of time between first and final data collection for the studies varied. Six studies used five months or less. Sixteen studies were around half a year long, while the most common (n = 38) was one year. Thirty-three studies comprised two to four years, and five were five years or more. One article contained two different studies and is counted twice.
The most popular scales are created by Young (1998a, 1998b). Twenty-seven studies use her Internet Addiction Test, her Young Diagnostic Questionnaire or adaptations thereof. This is not surprising, considering Young’s impact on the research field and that these scales were presented as early as the 1990s (Young, 1998a, 1998b). Second is S. H. Chen’s Chinese/Chen Internet Addiction scale, used in 14 studies, exclusively on East Asian populations. Third comes the Compulsive Internet Use Scale (CIUS) with 13 studies. Fourth is the Game Addiction Scale (GAS), eight studies. Fifth the GPIUS2, five studies. Six studies did not use a scale, but focused on frequency of use or other methods. Three studies used an adaptation of the DSM-IV gambling criteria. Gentile’s scales were used five times, and Davis’ scale three times. CSAS/CSAS II, LC-PIU, and Lee et al. (2002) were applied twice. Additionally, 15 other scales were used just once. Most are self-administered questionnaires with Likert-style responses and a cut-off at a certain value. As scales get modified and develop over time, different cut-offs may be used for the same scale. In this review, modified scales are grouped together with the original. 4 The main content of the most used scales are summarised in Table 2.
Diagnostic elements in most frequently used scales.
Note. CIAS = Chen Internet Addiction Scale; CIUS = Compulsive Internet Use Scale; GAS = Game Addiction Scale; CSAS/CSAS II = Computerspielabhängigkeitsskala (Eng. Video Game Addiction Scale); GPIUS2 = Generalized Problematic Internet Use Scale 2; LC-PIU = Lifestyle Changes in Regard to Problematic Internet Use; PIUQ = Problematic Internet Use Questionnaire.
The diagnostic scales are often used along with measures for frequency of use, and/or other psychometric measures, such as depression or attention deficit hyperactivity disorder (ADHD). In that sense, this list may understate the internal variation between studies in the review. Although scoping reviews typically do not make assessments of study quality (as compared to systematic reviews), partially due to a lack of inter-comparability between studies, a review of longitudinal studies should in some way notice attrition bias. In this review, this is done by looking at follow-up rate. Follow-up rate is sample size used in the final wave of data collection divided by the sample size used in the first wave of data collection and is a way of investigating whether attrition bias might be jeopardising the generalisability of the study’s results (as in Anderson, De Bruijn, Angus, Gordon, & Hastings, 2009). Two-thirds of the studies have a follow-up rate of 70% or higher, but 13 studies did not provide enough information to assess any follow-up rate.
Out of 100 studied samples (three studies used more than one), 95 are from Eurasia or English-speaking Western countries, with a disproportionately high amount in East Asia (45 studies) while other continents are almost absent. Figure 3 presents the origin of sample populations. Three studies used two different samples from two different countries and are therefore counted twice. The most studied age group is adolescents (64 studies), but studies cover most ages. More than half of the studies use samples with roughly equal amounts of male and female respondents.
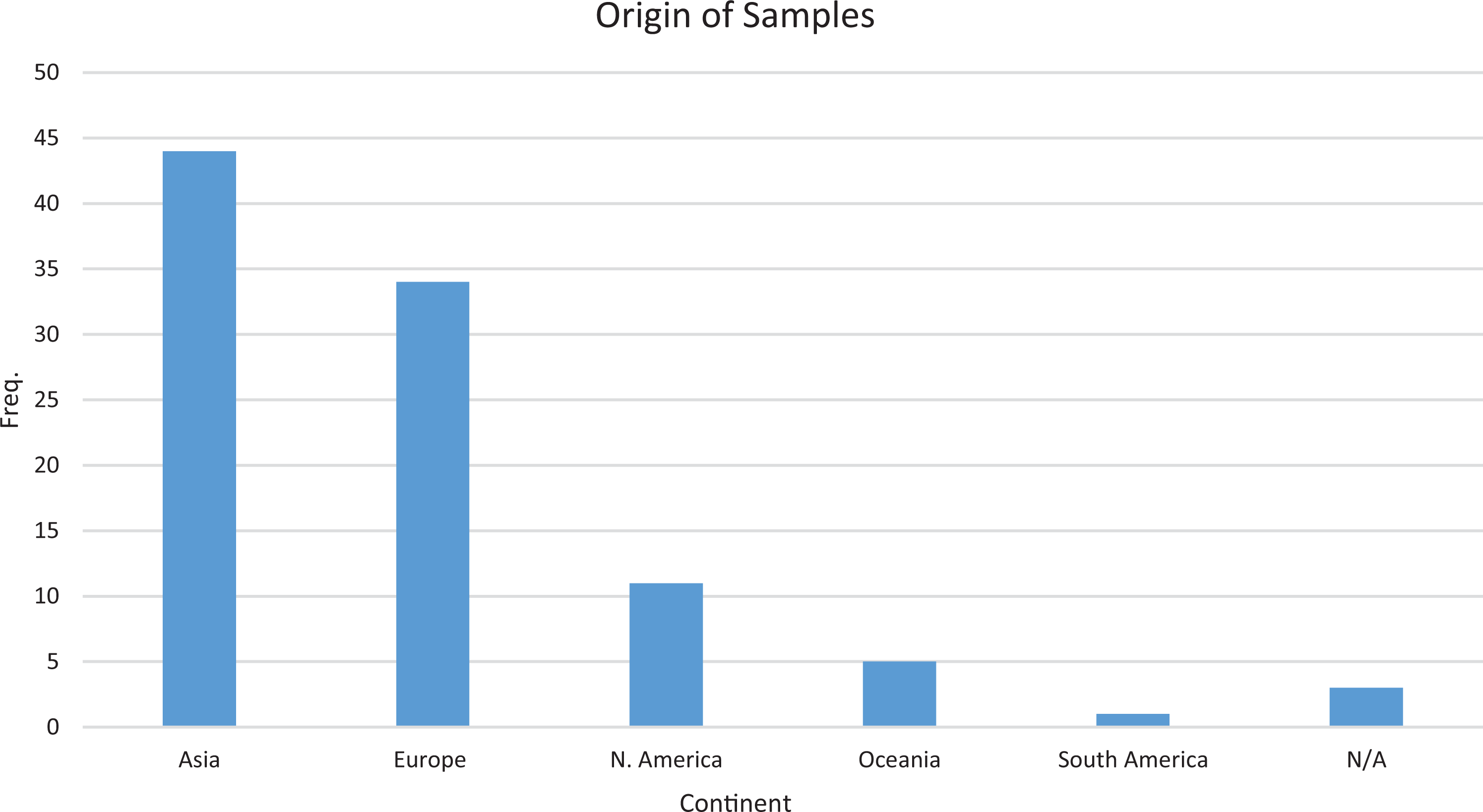
Sample origins.
Other psychiatric diagnoses
A number of studies discuss PIU as related to other psychiatric diagnoses, such as anxiety (Dong et al., 2011; Ko et al., 2014; Ko et al., 2009; Selfhout et al., 2009; Stavropoulos, Gomez, et al., 2017; Yao et al., 2013), ADHD (Chen, Chen, & Gau 2015; Ko et al., 2009), autism (Chen, Chen & Gau 2015, although the relationship was inverse; Finkenauer et al., 2012; Liu et al., 2017), and substance or alcohol use (Chang et al., 2014; Gámez-Guadix et al., 2015; Lee & Lee, 2017; Schmitt & Livingston, 2015; Sun et al., 2012; Zhang et al., 2016).
Depression is well-covered and suitable for longitudinal study designs, since, as compared to ADHD and autism, it is not chronic and onset could either precede or succeed PIU. This review comprises studies that found depression to precede PIU (Burleigh et al., 2017; Chang et al., 2014; Cho et al., 2013; Guillot et al., 2016; Ko et al., 2014; Ko et al., 2009; Liang et al., 2016; Yao et al., 2013), but also the opposite (Dong et al., 2011; Gentile et al., 2011; Han et al., 2017; Liang et al., 2016; Liau et al., 2015; Muusses et al., 2014; Salmela-Aro et al., 2017; Selfhout et al., 2009; Zhong, 2014), as well as indications of bidirectional relations (Chen & Lin, 2016; Gámez-Guadix, 2014; Jun, 2016; Tian et al., 2017). To conclude, results are mixed, except that most tend to find connections between PIU and other psychiatric diagnoses.
Social factors
Family-based conflicts, low level of family support and poor social adjustment have been related to IA (Bae, 2015; Chen, Chen & Gau 2015; Ko et al., 2015; Ko et al., 2007; Zhu et al., 2015), while harmonic family life (Liau et al., 2015; Yu & Shek 2013; Van der Eijnden et al., 2010) and protective parenting styles (Chang et al., 2014; Choo et al., 2015) seem to act protectively. Lau, Gross et al. (2017) found that living with only one parent was a risk factor (see also Rehbein & Baier, 2013), while having a parent with university education was protective. However, Shek’s and Yu’s (2016) findings indicated that family intactness or family function were not significant predictors for IA, whereas a family economic disadvantage was. However, in their 2012 study, Shek and Yu found family economic status to not be significant.
Social support in school or at the workplace is also important (Chen et al., 2014; Yu et al., 2015). Gámez-Guadix et al. (2013) found that being a victim of cyberbullying at T1 would predict depressive symptoms and PIU at T2, and Liu et al. (2017) found less school connectedness to be related to increased internet gaming addiction (see also Lemmens et al., 2011b; Rehbein & Baier, 2013).
Coherent with Burleigh et al. (2017), Bleckmann and Jukschat (2015) concluded that in-game success does not fulfil real-life biographical goals, meaning that success in online activities does not fully compensate for offline failures. Along the same lines, Yao and Zhong (2014) found that online contact with friends and family did not suffice to reduce feelings of loneliness. Time spent playing games is not problematic per se, according to Brunborg et al. (2014), but if adolescents have video-game-related problems, they are likely to have other problems as well.
Prevalence and change
The main focus of this study is prevalence of and change in PIU. Some studies focus on general internet use while others specifically single out gaming; therefore, they are presented separately.
General problematic internet use
Several studies used Chen Internet Addiction Scale (CIAS) to examine Asian samples. Chang et al. (2014) found that 26.1% of the sample had IA at baseline, and one year later a 63.3% persistence among those addicted at T1, while 15.8% of the healthy group at T1 had initiated IA by then. In two other studies using CIAS (Ko et al., 2014, 2015), prevalence went up slightly after a year (9% to 12%). Similarly, Lau et al. (Lau, Gross et al., 2017; Lau, Wu et al., 2017) found that internet addiction increased from 16% to 18% after a year. Of those not having IA at baseline, 11.5% had IA at follow-up, and 46% of individuals with IA at baseline showed remission at T2.
However, other studies using CIAS found a decrease in prevalence. In a two-year-long study, Ko et al. (2009) found prevalence going from 10.8% to 5.3%. In another study (Ko et al., 2007), prevalence went down from 18% to 15% after a year, where 49% of the addicted at T1 ended up in remission in T2. Chen and Gau (2016) found prevalence went down from 11.4% to 10.6% after one semester.
Chen and Gau (2016) used data in four waves over 11 months. Prevalence, using CIAS, went down from 12.1% at T1 to 9.3% at T4. Yet, sample size also went down from 1253 to 1054 respondents, and the change in IA between T1 and T4 amounted to 54 respondents. Although not discussed in the article, one explanation for this decrease could be possible attrition bias.
Guillot et al. (2016) used several scales for the assessment of internet use and gaming. They found similar prevalence at baseline as at follow-up (21.4–21.8%). Another one-year study (Sussman et al., 2015) reported a slight increase (ever addicted 14.5–15.8%, last month 10.2–11.4%). Notable is that, of those reporting addiction at the first wave, only 43% did so at the second wave.
During a six-wave, six-year study implementing (Internet Addiction Test, IAT) (Shek & Yu, 2012, 2016; Yu & Shek, 2013), prevalence decreased continuously, from 26.2% to 17.0%, attributed to general tendencies in adolescent risk behaviour and maturation with age. Barrense-Dias et al. (2016) also applied IAT. Prevalence went down from 13.2% to 4.8% in a two-year period.
Strittmatter et al. (2016), using (Young Diagnostic Questionnaire, YDQ) in a two-year study, found prevalence to be 4.3% at T1, 2.7% at T2 and 3.1% at T3. In total, only 0.58%, or three students, had PIU throughout the whole period. Just as Shek and Yu (2016), they attribute some of this transience to adolescent risk-taking behaviour and coping.
Problematic gaming
Van Rooij et al. (2011), using the CIUS, identified 1.6% of an adolescent sample as addicted at T1, and 1.5% at T2; a comparatively low but consistent share. The addicted group made up about 3% of the total population of gamers. The authors also identified a group of heavy gamers, constituting about 3% of the total gamer population, who were not addicted.
Forrest et al. (2017) applied the GAS to a four-wave study, finding a prevalence of problematic involvement at 15.7% at T1 and 9.2% at T4, nine months later. A majority (66%) of problematic gamers at T1 were in remission at T4. Also using GAS, Henchoz et al. (2016) assessed problematic video game use to be 11.9% at baseline, 9.6% at follow-up, and video game addiction to be 2.2% at baseline and 2.3% at follow-up, after 15 months.
Scharkow et al. (2014) also used the GAS in a two-year-long, three-wave study. They found a prevalence level of problematic users at 3.7% at T1, 3.2% at T2, and 2.7% at T3. Only one respondent per data collection round fulfilled the criteria for gaming addiction, and none did it more than once. Among those fulfilling the levels for problematic use, only 26.5% persisted in problematic use between the first and final wave of data collection.
Gentile et al. (2011) based their scale on DSM-IV gambling criteria and Brown’s behavioural addiction criteria in a Singapore-based three-wave, two-year study, and found a slight decrease (9.9%, 8.8%, 7.6%) over time in pathological gamers. However, most interesting about their findings is that 84% of the pathological gamers persisted after two years, but that only 1% became pathological gamers after the first wave.
Rothmund et al. (2016) investigated excessive gaming over the course of one year, using the Gentile scale for pathological gaming. Results indicated that 10.4% were excessive gamers at T1, but only 7.1% were at T2. Only 27% of those who were excessive gamers at T1 continued to be so at T2. Consequently, the conclusions of Rothmund et al. (2016) are the opposite of Gentile et al. (2011): that excessive gaming appears to be transient, not stable.
Thege et al.’s results (2015) point in a similar direction to those of Rothmund et al. (2016). They studied online chatting and video game habits over five years using the Behavioral Addiction Measure, producing comparatively low numbers: 1.7% of the sample were excessive video gamers at T1, but after five years these respondents only made up 1.2%, of which (n = 201) none reported excessive use at all five times, and most (76.1%) did so only once. Weinstein et al. (2017) also reported low prevalence rates, applying their own nine-item checklist to gamers, seemingly based on the DSM-5 proposed checklist for Internet Gaming Disorder. At the first wave, 1.49% fulfilled five or more criteria, which at the second wave went down to 0.99%. Even fewer (0.38% at T1 and 0.30% at follow-up) reported having “suffered significant stress due to gaming in the past six months” (Weinstein et al. 2017, p. 9).
Discussion and conclusions
This review has shown a research field that is alive and growing, although plagued by a lack of consensus in methods and understanding of the problem, which hinders the drawing of general conclusions about the extent of the problem and assessment of whether the studies really measure the same thing. Many studies base their measures on the DSM scale for pathological gambling, often through Young’s (1998a, 1998b) adaptions. Others take a cognitive-behavioural, or a substance misuse perspective. The difference between a substance misuse perspective and the pathological gambling perspective, however, is unclear, and sharing theoretical foundations is no guarantee for measuring the exact same thing.
Due to this review’s broad inclusion criteria, one would expect some variation, but 28 reported scales over 97 studies is inconsistent. Further substantiating this, a comparison of the criteria of the 11 most used diagnostic scales for PIU and gaming unveiled heterogeneity among definitions of the problem: e.g., trouble cutting down was only included in three of these 11 scales, relapse in two, and some scales do not account for whether internet use causes problems for afflicted individuals. Considering that Brunborg et al. (2014) and Griffiths (2008) showed that spending a large amount of time using the internet or gaming is not necessarily problematic, this could point to an over-exaggeration of the number of problematic users. Another possible source of inconsistency to be studied in further research ventures is that this review has not accounted for differences in cut-off criteria or length of questionnaires in the diagnostic scales used in the studies.
Most studies in the review are published in Western Europe and other Western countries along with East Asia, while other populations are absent. This could partially be explained by language bias in the literature search. Additionally, countries with many studies published on the subject are all industrialised with large service sectors and high internet density, where one would expect questions and problems regarding IT use to arise.
Adolescents form the most widely studied group of respondents, two thirds of the studies. There could be several explanations for this focus. One is that adolescents have been identified as the main risk group for developing PIU. Also, adolescents are easy to survey and follow through school. This could also explain why 22 additional studies have focused entirely on young adults, mostly using college student samples.
The review indicates an association between PIU and symptoms of depression, as well as dysfunctional social relations and other psychiatric disorders, but it is unclear whether there is a pattern where one precedes the other. One alternative explanation to addiction would be that PIU and depression are both indicators of general life dissatisfaction, making coping a plausible hypothesis. Similarly, results highlight that social factors could prevent PIU, mainly through maintaining and developing strong social integration and family relationships, as well as in the workplace and in school. Thus, findings of this review indicate that it is far from an isolated problem.
Findings on prevalence and change are scattered. We could not get a good level of appreciation as similar populations and measures do not produce the same results. Most notably, estimating prevalence using the CIAS on Taiwanese adolescents varied between 27% at its highest and 5% at its lowest. For prevalence over time, results are also scattered. Among studies measuring persistence, these ranged from almost 0% to 84%, using different timespans and measures. For general PIU, prevalence rates differ widely, from almost nothing up to the high twenties. It is remarkable that around 50 studies do not measure prevalence at all.
Therefore, one of this review’s main objectives – to find an expected level of prevalence and structure in change through research synthesis – failed. The empirical validity and comparability of concepts such as IA or gaming disorder, based on empirical findings, seems low to such a degree that the concepts should be interpreted with caution.
Introducing gaming disorder in influential guidebooks will increase reliability between studies. However, since we cannot even get a stable estimation of prevalence rates at this stage, we cannot be sure that the measures being used are valid. Key elements and predictors of the problem should develop from empirical evidence rather than squeezing them into translations of existing substance use or gambling addiction scales. Otherwise, we risk labelling people as sick when they are not, and miss important aspects unique to the aetiology and solution of this problem.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.