
Abstract
Aims:
The aims were to investigate whether baseline characteristics and problematic substance use were related to change in mental distress over time in patients with substance use disorders during an 18-year period.
Method:
This was a prospective, longitudinal study of patients followed for 18 years after entering specialised treatment for substance use disorders. A sample of 291 patients was recruited in 1997 and 1998. Mental distress was measured using the Hopkins Symptom Checklist 25 at baseline, and at six and 18 years. Lifetime psychiatric disorders and substance use disorders at baseline were measured using the Composite International Diagnostic Interview, while personality disorders were measured using the Millon Clinical Multiaxial Inventory II. At the six- and 18-year follow-ups, substance use was measured using the Alcohol Use Disorders Identification Test and the Drug Use Disorders Identification Test. Linear mixed model was estimated to assess the overall level of mental distress over 18 years for participants with complete data at baseline (n = 232).
Results:
In an adjusted model, problematic substance use assessed simultaneously with mental distress, having lifetime affective, anxiety and personality disorder at baseline were associated with greater levels of mental distress over the 18-year period. The change in mental distress from baseline to the six-year, but not to the 18-year, follow-up was significantly larger among females than among males.
Conclusion:
The results suggests a reciprocal relationship over time between substance use and mental health problems. Also, there seems to be an additive effect between ongoing problematic substance use and lifetime mental disorders on greater levels of mental distress. This addresses the importance of integrated treatment for both substance use disorders and mental disorders to improve the long-term course for patients with these comorbid disorders.
Epidemiological studies have documented substantial comorbidity of substance use disorders (SUDs) and other mental disorders (Lai et al., 2015; Regier et al., 1990). This comorbidity is higher in clinical than general populations (Andreas et al., 2015; Landheim et al., 2002), and patients with SUDs have higher psychiatric comorbidity than patients with psychiatric disorders have comorbidity with SUDs (Morisano et al., 2014). Patients with severe SUDs, as in poly-substance use, also have more mental health problems than do those with less severe SUDs (McCabe & West, 2017), and patients tend to have poorer outcomes if a mental disorder occurs before SUDs (Najt et al., 2011). In addition, females in treatment for SUDs have higher psychiatric comorbidity than males, particularly in terms of mood and anxiety disorders (Brady & Randall, 1999; Landheim et al., 2003; Zilberman et al., 2003).
In general, there are few longitudinal studies of clinical cohorts of patients with SUDs. Longitudinal studies typically examine the course of substance use and risk factors for substance use relapse (Heyman, 2013; Hser et al., 2015; Moos & Moos, 2006) or mortality (Degenhardt et al., 2011; Giraudon et al., 2015; Roerecke & Rehm, 2013). Mental disorders are among the most studied and documented risk factors for poor long-term outcomes in patients with SUDs (Bradizza et al., 2006; Landheim et al., 2006). However, studies rarely focus on the long-term course of mental health and the prospective relationship between substance use and mental health over time in patients with a history of SUDs (Andreas et al., 2015). Repeated-measurements analysis has shown an association over time between increased psychiatric symptom load and increased substance use during a nine-year observation period in persons seeking treatment for SUDs in the US (Chi & Weisner, 2008). In another repeated-measurements analysis of a Norwegian cohort of patients with SUDs, both the levels and development of mental distress over time were related to the number of substances used during a 10-year observation period (Andreas et al., 2015). We have previously found that six years after entering treatment for SUDs, mental distress was stable relative to baseline in patients with active problematic substance use (Bakken et al., 2007). By contrast, those with no current problematic substance use, and especially females, reported a significant decrease in mental distress compared with baseline. In that study, we also found that lifetime mental disorders, personality disorders, and substance use factors measured at baseline were predictors for having greater levels of mental distress at the six-year follow-up (Bakken et al., 2007).
The associations between SUDs and mental health problems and development over time are complex and are not fully understood (Swendsen et al., 2010). Several explanations have been offered, but no single explanation accounts for all of the variance (Morisano et al., 2014). We know that this comorbidity reduces quality of life (Colpaert et al., 2012), and can lead to poor treatment adherence (Weiss et al., 2002) and treatment outcome (Bahorik et al., 2013), including more frequent substance use relapse and hospitalisation (Morisano et al., 2014). Understanding the reciprocal relationship between mental health problems and substance use over time in different SUD sub-groups and stages is important for the development of effective tailored treatment and relapse-prevention programmes.
The present material is from a longitudinal 18-year follow-up study of a heterogeneous cohort of patients who sought treatment for SUDs. The patients had long-lasting and severe SUDs with a high comorbidity for lifetime mental disorders. The aims were to investigate whether sex, age, psychiatric diagnosis, or substance use factors at baseline and problematic substance use at follow-ups assessed longitudinally were related to change in mental distress over time in patients with SUDs during an 18-year period.
Material and method
Design
This was a longitudinal cohort study with three measuring points over a period of 18 years. Patients entering specialised treatment for SUDs in public facilities in two Norwegian counties in 1997 and 1998 were invited to participate in the study (T0). Follow-up measurements were conducted by mailed questionnaires to living participants about six years (T1), and 18 years later (T2).
Sample
At T0, 291 patients (mean age 38.3 years, standard deviation [SD] = 11.4 years; 72% male) from three outpatient (42%) and six inpatient (58%) units were recruited. The mean time since the first onset of SUD at T0 was 13.8 years (SD = 8.8 years), and 46% had experienced onset of a SUD before the age of 18 years. The prevalence of lifetime psychiatric symptom disorders other than SUDs at T0 was 91%; 83% had a lifetime anxiety disorder, 65% had a lifetime affective disorder, and 63% had three or more lifetime psychiatric disorders. Among the recruited patients, 291 (100%) had one or several SUDs both in their lifetime and during the past 12 months; 130 (45%) had lifetime alcohol use disorder (AUD) alone, and 161 (55%) had poly-SUDs. This latter group had an average of 3.6 (SD = 2.0) lifetime SUDs (the term “poly-SUDs” is not entirely accurate, as 18 patients [11%] had only one lifetime SUD other than AUD: six had only opiate, six had only cannabis, four had only sedative, and two had only stimulant use disorder). Among the patients with poly-SUDs, 53% had lifetime opioid dependence, 49% lifetime stimulant dependence, 50% lifetime sedative, hypnotic, or anxiolytic dependence, 41% lifetime cannabis dependence, and 65% lifetime alcohol dependence. Patients with AUD alone more often tended to be males (77% vs 67%, p = .055), to be older (45.8 vs 32.1 years, p < .001), to have fewer lifetime psychiatric disorders (3.2 vs 3.9, p = .027), and to be less likely to have lifetime affective disorders (57% vs 69%, p = .047), lifetime anxiety disorders (76% vs 88%, p = .010), and current personality disorders (63% vs 80%, p = .003) at T0 compared with patients with poly-SUDs.
At T1, 33 (11%) patients had died, 160 participated, and 98 did not (14 declined, 23 could not be located, and 61 did not respond). At T2, 96 (33%) patients had died, 91 participated and 104 did not (22 declined, 14 could not be located, and 68 did not respond). Participants who responded at T2 received 400 Norwegian kroner (∼43 euro).
Measurements
T0.
The Composite International Diagnostic Interview (CIDI), Norwegian computer version, a structured personal psychiatric interview based on Diagnostic and Statistical Manual of Mental Disorders, 4th Edition criteria, and the corresponding lifetime non-hierarchical diagnoses in the International Classification of Diseases, 10th Edition (ICD-10) (Robins et al., 1988) were used. Lifetime ICD-10 diagnoses from F30 to F34 were clustered into “Affective disorder lifetime T0”, and all lifetime ICD-10 diagnoses from F40 to F44 were clustered into “Anxiety disorder lifetime T0”. SUDs, dependence or abuse, were measured with the CIDI both as lifetime diagnoses and during the previous 12 months at T0. The Millon Clinical Multiaxial Inventory II (MCMI-II), a self-report psychiatric diagnostic (Diagnostic and Statistical Manual of Mental Disorders, 3rd Edition, Revised) inventory (Choca et al., 1992) was used on personality disorders, where diagnoses were given using a cut-off base-rate score of 85 or higher. The Hopkins Symptom Checklist-25 (HSCL-25), a self-report instrument composed of 25 items on a four-point scale was used to measure mental distress during the past week (Derogatis et al., 1974; Strand et al., 2003). The mean of all items on the HSCL-25 is called the Global Severity Index (GSI).
T1
The HSCL-25 was repeated. The Alcohol Use Disorders Identification Test (AUDIT) (Saunders et al., 1993) and the Drug Use Disorders Identification Test (DUDIT) (Berman et al., 2004), both self-report screening instruments for identifying problematic use of substances during the past 12 months were also used. The AUDIT is composed of 10 items; cut-off scores of 8 or more for males and 6 or more for females were used. The DUDIT has 11 items; cut-off scores of 6 or more for males and 2 or more for females were used.
T2
The HSCL-25, the AUDIT and the DUDIT were repeated. National identity numbers for all patients (n = 291) were merged with data from the Norwegian Cause of Death Registry, providing dates of death until 31 June 2016.
Definition of problematic substance use
All participants had one or several SUDs during the past 12 months at T0 measured with the CIDI, and were defined as having “problematic substance use” at T0. Participants at T1 and at T2 were divided into those with “no problematic substance use” (AUDIT < cut-off and DUDIT < cut-off during the past 12 months at T1 or T2 accordingly) and participants with “problematic substance use” (AUDIT ≥ cut-off and/or DUDIT ≥ cut-off during the past 12 months at T1 or T2 accordingly).
Loss of participants and missing data
Figure 1 shows a flow diagram illustrating participation and loss of participants during the 18 years of observation, as well as the foundation for the data analysis. Except for the loss of participants to death and non-participation, there were few missing data. The exceptions were at T0, the HSCL-25 was not answered by 37 (13%) participants and the MCMI-II was not answered by 27 (9%) participants. Four participants (1%) did not complete all sections on affective disorders, and eight (3%) participants did not complete all sections on anxiety disorders in the CIDI at T0. Missing single values at T1 and T2 on the HSCL-25, AUDIT and DUDIT were handled by calculating the mean of the remaining items if missing items comprised < 20% (only one HSCL-25 score at T1 was excluded because of missing values). Among the 291 recruited participants, 232 (80%) participants had complete data, that is, no missing values on all assessed covariates, at T0.
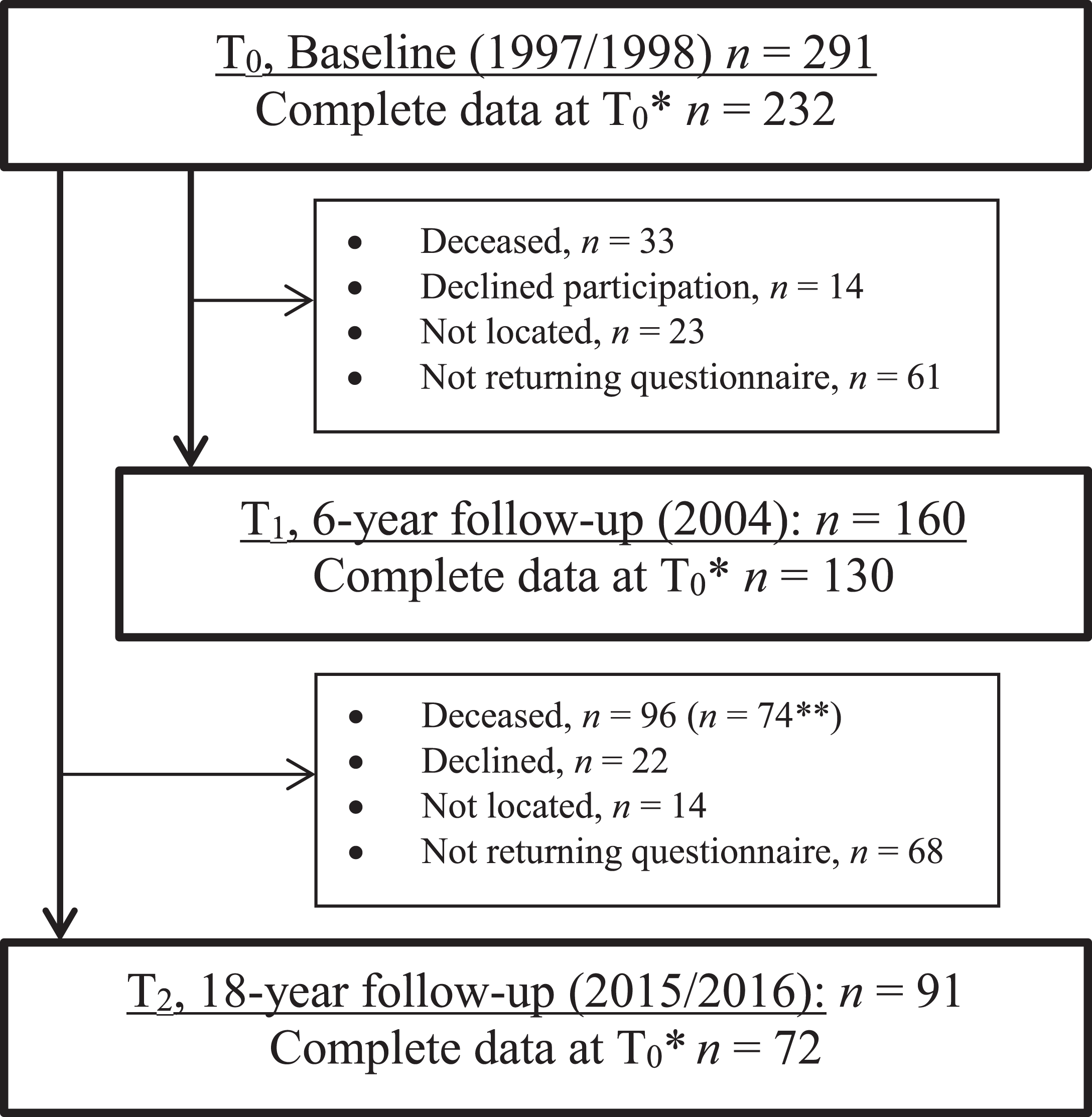
Flow diagram of the participants, data collection and analysed data.
Statistical Analysis
Data are presented by appropriate descriptive statistics. We compared participants with complete data on all assessed covariates at T0 (n = 232) with those excluded because of one or more missing values at T0 (n = 59), and among those with complete data at T0 living (n = 158) with deceased (n = 74) participants at T2 by independent samples t-test for continuous and χ2 test for categorical variables. A linear mixed model (LMM) was estimated to assess differences in levels of the HSCL-25 GSI from T0 to T1, and T0 to T2 among participants with complete data at T0 (n = 232). Fixed effects at each time point were included, with T0 as the reference. Random intercepts for participants were included to account for within-participant correlations due to repeated measurements. An autoregressive covariance structure was employed. Unadjusted models with main effects for time and each pre-defined covariate (sex, age, problematic substance use at T0, T1 and T2, lifetime affective disorder at T0, lifetime anxiety disorder at T0, personality disorder at T0, first onset of SUD before 18 years of age, and having only AUD at T0) and interactions between time and each covariate were estimated first. Interaction between time and problematic substance use could not be estimated because zero participants had “no problematic substance use” at T0 and were therefore not included. Next, an adjusted model containing time, all covariates and interactions between time and each covariate was estimated and reduced by applying Akaike’s Information Criterion (AIC), where the smaller value means better model. Age and sex were kept in the adjusted model regardless of the value of AIC. The results were presented as regression coefficients and standard errors (SE).
The LMM assumes a non-informative censoring, i.e., that death and outcome of interest are not associated. Due to the high number of deaths in the given data set, it is not unlikely that death cannot be treated as non-informative, in which case the LMM might produce biased estimates of regression coefficients and SEs. To assess this issue in detail, the joint model with longitudinal process modelled by the LMM and survival process modelled by Weibul proportional hazards survival model was estimated. Unadjusted and adjusted joint models did not show any statistically significant association between the two types of outcomes (longitudinal and survival). Moreover, SEs of coefficients as well as variances of random effects were similar to those obtained from the LMM. Hence, death could be treated as non-informative and only the results of the LMM were presented.
All analyses were employed using SPSS for Windows (version 25.0; IBM SPSS, Armonk, NY), SAS version 9.4, STATA version 16 and R version 3.6.0 (ISNI package version 1.1).
Results
As shown in Table 1, the baseline characteristics did not differ significantly between participants with complete data at T0 (n = 232) and those excluded from further analysis because of missing values at T0 (n = 59). Among the participants with complete data at T0, 74 had died at T2. The participants who died during the observation period were older, had more seldom experienced onset of first SUD before 18 years of age, were more likely to have only AUD compared with poly-SUDs, and had less lifetime affective disorders measured at T0 compared with participants still living at T2 (n = 158).
Baseline characteristics of participants with complete data at T0*, excluded participants and deceased participants in the follow-up 18 years after treatment.
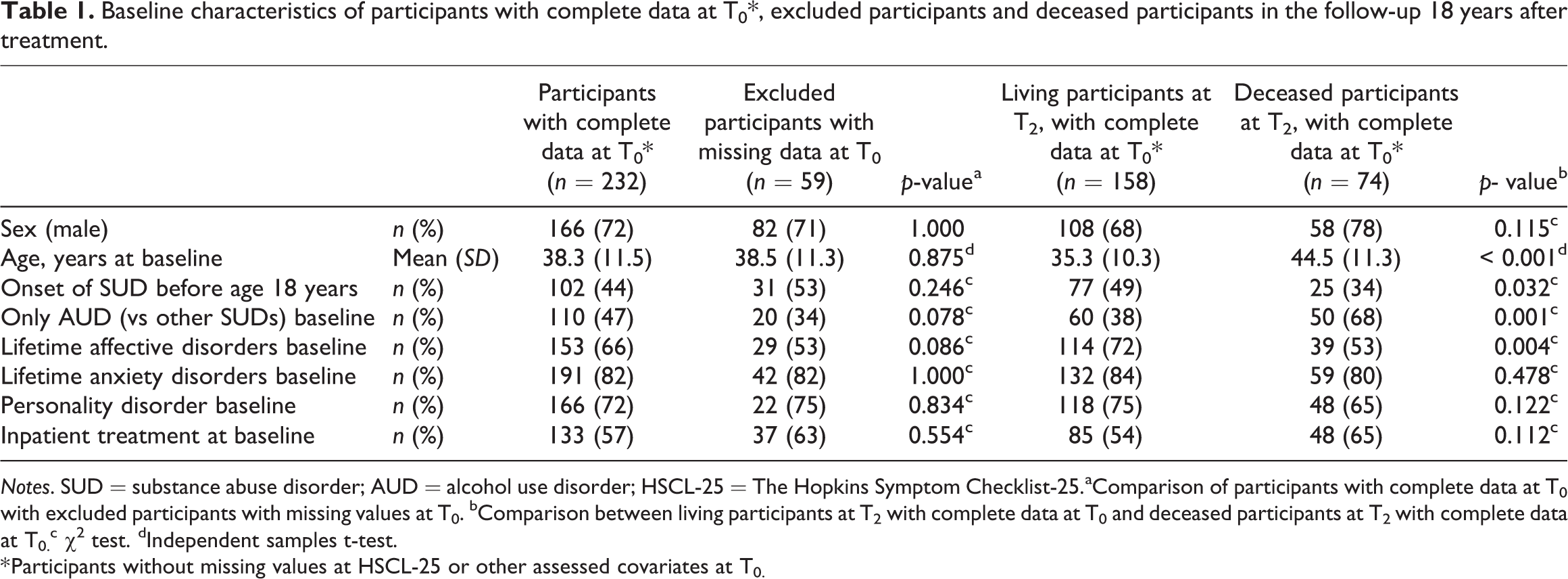
Notes. SUD = substance abuse disorder; AUD = alcohol use disorder; HSCL-25 = The Hopkins Symptom Checklist-25.aComparison of participants with complete data at T0 with excluded participants with missing values at T0. bComparison between living participants at T2 with complete data at T0 and deceased participants at T2 with complete data at T0. c χ2 test. dIndependent samples t-test.
* Participants without missing values at HSCL-25 or other assessed covariates at T0.
Table 2 shows the levels of mental distress as measured by the GSI in all participants with complete data at T0 (n = 232) and in different sub-groups at each time point. Participants with lifetime affective or anxiety disorder, or current personality disorder at T0, had a higher GSI than did those without these disorders at each time point. In addition, participants with ongoing problematic substance use had a higher GSI than did those with no current problematic substance use at both T1 and T2.
Description of levels of mental distress as measured by the HSCL-25 Global Severity Index (GSI) at all measuring points for participants with complete data at T0*.
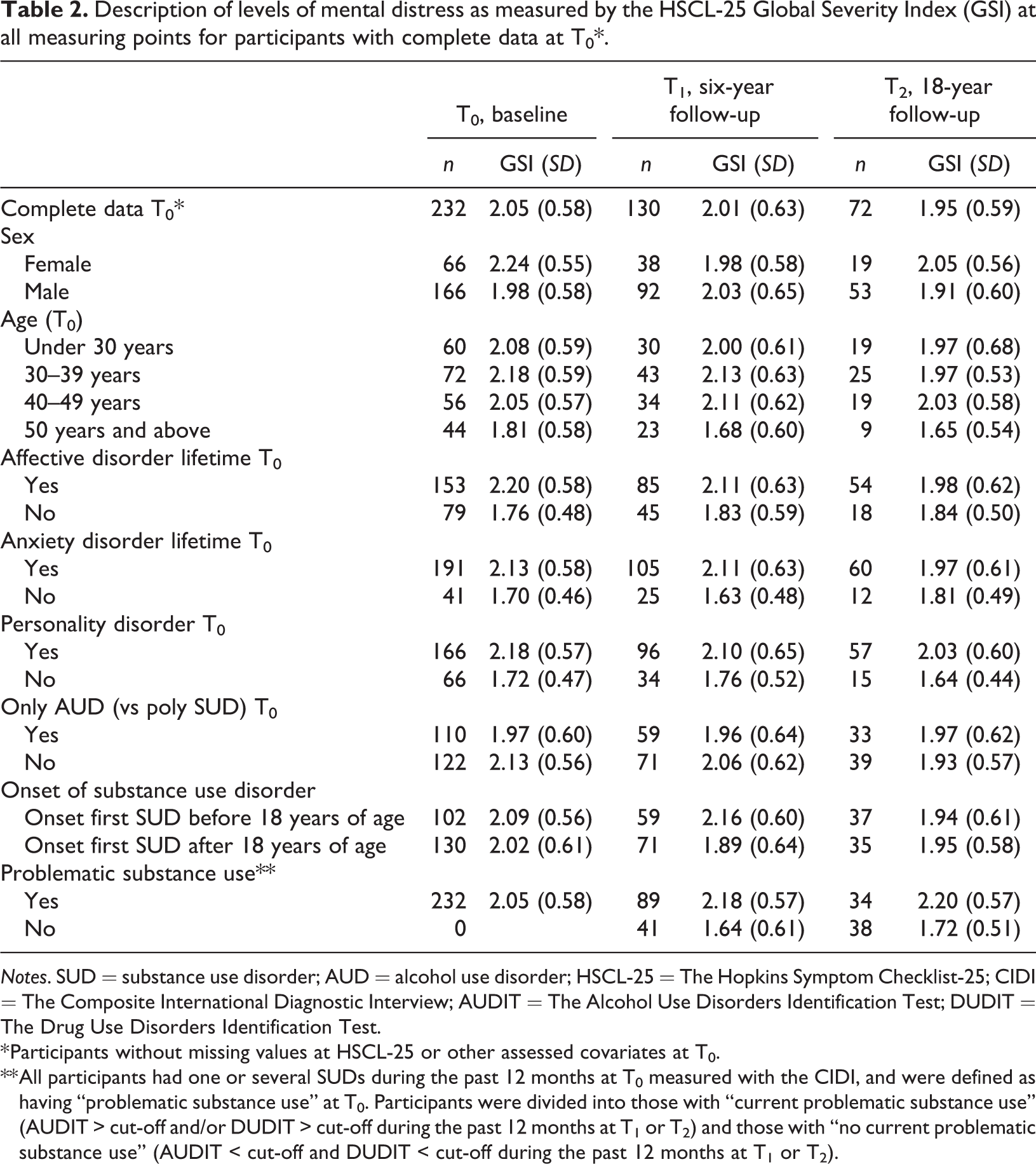
Notes. SUD = substance use disorder; AUD = alcohol use disorder; HSCL-25 = The Hopkins Symptom Checklist-25; CIDI = The Composite International Diagnostic Interview; AUDIT = The Alcohol Use Disorders Identification Test; DUDIT = The Drug Use Disorders Identification Test.
* Participants without missing values at HSCL-25 or other assessed covariates at T0.
** All participants had one or several SUDs during the past 12 months at T0 measured with the CIDI, and were defined as having “problematic substance use” at T0. Participants were divided into those with “current problematic substance use” (AUDIT > cut-off and/or DUDIT > cut-off during the past 12 months at T1 or T2) and those with “no current problematic substance use” (AUDIT < cut-off and DUDIT < cut-off during the past 12 months at T1 or T2).
Table 3 presents the results of the LMM assessing covariates associated to changes in the GSI over time. Unadjusted for other covariates, there was no significant change in GSI from T0 to T1 (p = .215), while a significant decrease in GSI was found from T0 to T2 (p = .049). In the adjusted model, the only interaction identified was between time and sex, implying that the change in GSI from T0 to T1 was significantly different between males and females (p = .044). Also, females had significantly higher GSI at T0 than males (p = .019). The interaction is also illustrated in Figure 2. Moreover, greater level of GSI was associated with problematic substance use assessed simultaneously with GSI at T0, T1 and T2 (p < .001), having a lifetime affective disorder at T0 (p = .007), lifetime anxiety disorder at T0 (p = .001), and a personality disorder at T0 (p < .001). In the adjusted AIC-reduced model, age was not associated with GSI.
The results of linear mixed models assessing associations between the level of mental distress over the 18 years and patient characteristics associated with change in level of mental distress in time.
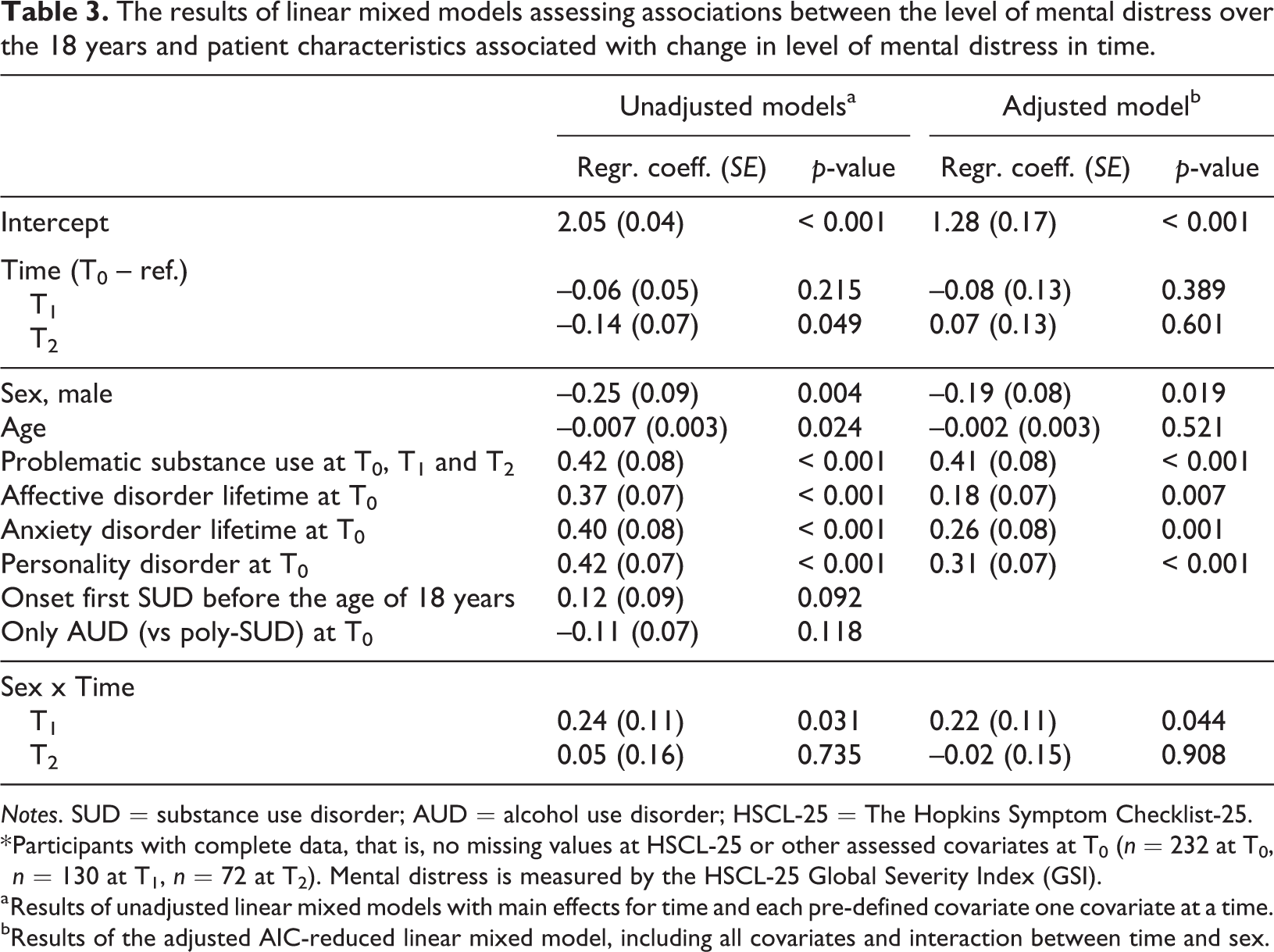
Notes. SUD = substance use disorder; AUD = alcohol use disorder; HSCL-25 = The Hopkins Symptom Checklist-25.
* Participants with complete data, that is, no missing values at HSCL-25 or other assessed covariates at T0 (n = 232 at T0, n = 130 at T1, n = 72 at T2). Mental distress is measured by the HSCL-25 Global Severity Index (GSI).
a Results of unadjusted linear mixed models with main effects for time and each pre-defined covariate one covariate at a time.
bResults of the adjusted AIC-reduced linear mixed model, including all covariates and interaction between time and sex.
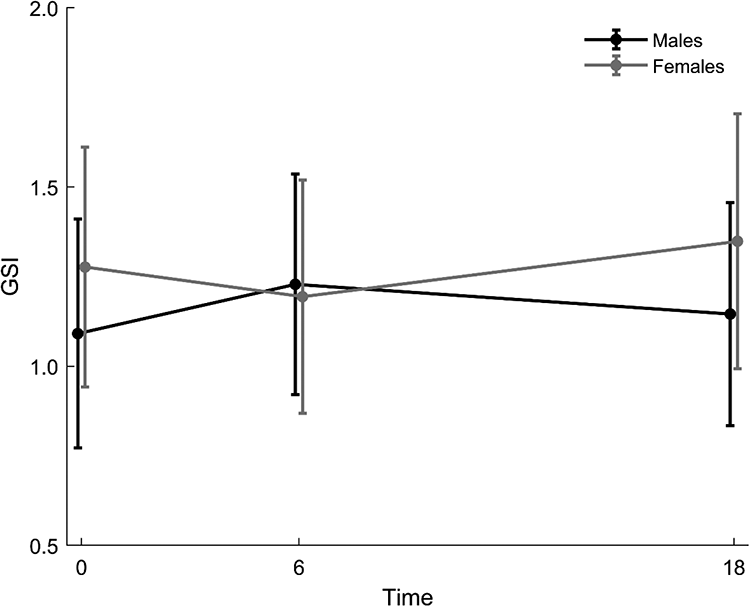
Illustration of the interaction between time and sex from the AIC-reduced adjusted linear mixed model, presented in Table 3.
Discussion
The main finding in this study was that in an adjusted model, problematic substance use assessed longitudinally, and having lifetime affective, lifetime anxiety and personality disorder at baseline were associated with greater levels of mental distress over the 18-year observation period. Also, there were significant differences between females and males in changes in mental distress from baseline to the six-year, but not to the 18-year, follow-up.
A clear association between problematic substance use and greater levels of mental distress is as expected from epidemiological studies and reviews (Lai et al., 2015; Regier et al., 1990), and from longitudinal studies of clinical cohorts of patients with SUDs followed for up to 10 years (Andreas et al., 2015; Chi & Weisner, 2008). Our finding is important because, to our knowledge, there are no longitudinal studies from clinical cohorts of patients with SUDs that have documented the association between problematic substance use and greater levels of mental distress assessed simultaneously for as long as 18 years. The finding that lifetime affective, lifetime anxiety and personality disorders are associated with greater mental distress in patients with SUDs is also consistent with other research and the results from the six-year follow-up study of the same cohort (Bakken et al., 2007). Mental distress and psychiatric diagnoses have some similarities, but differ in several aspects, and the HSCL-25 and CIDI diagnoses only partly measure overlapping dimensions of mental health problems (Sandanger et al., 1998). We assessed psychiatric disorders only at baseline and a positive significant association with greater levels of mental distress suggests that these patients also had mental disorders over long periods of time. The results suggest an additive effect between ongoing problematic substance use, and affective, anxiety, and personality disorders on greater levels of mental distress. This supports evidence that there is a reciprocal relationship over time between substance use problems and mental health problems. It also underlines the importance of adequate integrated treatment for both SUDs and mental disorders, because the long-term prognosis worsens if these comorbid disorders are left untreated or are poorly treated (Morisano et al., 2014). In this context, we note that SUDs and mental health disorders probably have a shared genetic pre-disposition (Kendler et al., 2003).
In our results, the substance use factors measured at baseline, early onset of first SUD and having only AUD compared with poly-SUDs, were not associated with greater levels of mental distress over 18 years and were eliminated from the adjusted model. By contrast, in the six-year follow-up study these covariates were predictors of high mental distress six years later (Bakken et al., 2007). This negative result for baseline substance use factors may be related to the characteristics of the cohort, as baseline differences were observed between participants with only AUD and those with poly-SUDs. Although the cohort was heterogeneous in the sense of including females and males, a wide range of ages and different SUDs, on average the patients had severe and long-lasting SUDs. This may have made it difficult to detect potential differences in substance use factors.
Several studies have shown that females in treatment for SUDs have higher psychiatric comorbidity than males, particularly for mood and anxiety disorders (Brady & Randall, 1999; Landheim et al., 2003; Zilberman et al., 2003). According to descriptive statistics in the present study we can see that females on average scored somewhat higher than males on mental distress at both baseline and at the 18-year follow-up. Perhaps more interestingly, when exploring the interaction between sex and time in the adjusted model, we found a difference between females and males in the change in mental distress from baseline to the six-year, but not to the 18-year follow-up. These results over 18 years do not support the notion raised after the six-year follow-up study, that mental distress is more strongly associated with ongoing problematic substance use in females than in males (Bakken et al., 2007). There were relatively few females in the study, especially at the follow-ups, and thus these findings on sex differences should be interpreted with caution.
Limitations
Our study is vulnerable to selection bias (Sackett, 1979) because the participants have a relatively high mean age, and both long-lasting SUDs and high comorbidity with mental disorders at baseline. Younger patients with both better and worse prognoses may have been underrepresented. A substantial decrease in the number of participants over time because of mortality and non-participation is inevitable in such a cohort, and may have led to attrition bias (Deeg, 2002). Some differences in characteristics were seen between surviving participants and deceased participants during the observation time, but no differences were found between participants with complete data and those with missing values at baseline. This non-random loss of participants over time is also a problem when applying linear mixed models. However, the joint modelling of longitudinal outcome and death, clearly indicated that death could be treated as non-informative, and that it did not bias the results in any substantial way. Having more than three measuring points during the 18 years would have provided more detailed information about the development of mental distress over time. There can also be problems in measuring mental disorders at baseline in relative temporal proximity to substance abuse, and the diagnoses can differ between those reached via structured diagnostic interviews, as used in the present study, compared with those reached by clinical experts, who likely set fewer diagnoses (Andrews & Peters, 1998). All data at the time of the six- and 18-year follow-up measurements were self-reported, and self-reported data can be prone to recall bias (Coughlin, 1990) and skewed self-presentation (Mortel, 2008), which may lead to both under and overreporting.
The main strengths of this study were the 18-year period, the heterogeneous clinical cohort with long-term problematic substance use, and the thorough diagnostic investigation with structured personal interviews at baseline. Despite limitations, this study provides unique documentation of the long-term levels of mental distress and its association with long-term problematic substance use, and mental disorders in patients with SUDs.
Conclusion
The results suggest a reciprocal relationship over time between substance use and mental health problems. Also, there seems to be an additive effect between ongoing problematic substance use and lifetime mental disorders on greater levels of mental distress. This addresses the importance of integrated treatment for both substance use disorders and mental disorders to improve the long-term course for patients with these comorbid disorders.
Footnotes
Acknowledgements
We thank all the respondents for their time and effort in participating in this study.
Ethical approval
The study protocol was reviewed and approved at baseline, the six-year follow-up and the 18-year follow-up by the Regional Committee for Medical and Health Research Ethics, Health Region South-East (ID 2014/1936 C). All participants gave their written consent before taking part in the study, and to be contacted for follow-up studies.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors declared the following financial support for the research, authorship, and/or publication of this article: This work was funded by Innlandet Hospital Trust, Norway.