
Abstract
Addiction treatment services have been available in Greenland for many years, but a significant change occurred in 2016 with the introduction of Allorfik, a dedicated addiction treatment service. The implementation of Allorfik reflected an ongoing commitment to addressing addiction and alcohol-related issues in Greenland. The balance between the necessity of restrictions of the availability of alcohol – as was seen during the colonial time – versus the protection of individuals vulnerable to addiction problems and to the social consequences of the alcohol use was constantly on the political agenda the 60s, 70s, 80s and 90s (Poulsen, 2012). Heavy drinking has been an issue since the commercial release of sales of alcohol in the early 1950s, with a peak in intake levels at around 22 L of pure alcohol a year per adult person (aged 15+ years) in the late 1980s (Aage, 2012; Bjerregaard et al., 2020). In 2013, addiction problems were still considered the largest problem for health and social well-being in Greenland (Departement for Sundhed, 2012). Estimates of problematic use of alcohol have been high, with National Population Health Surveys reporting that approximately 50% of the adult population engaged in binge drinking at least once a month and approximately 30% were considered to have potentially harmful alcohol consumption in the years 2003, 2008, 2010, 2011 and 2016 (Bjerregaard & Aidt, 2010; Bjerregaard & Dahl-Petersen, 2011; Bjerregaard et al., 2003, 2008; Dahl-Petersen et al., 2016). The high per capita intake of alcohol in recent decades has also resulted in a significant proportion of people reporting that they grew up in homes with alcohol-related problems (Larsen et al., 2018). Furthermore, the use of cannabis has become a growing issue, with approximately 10% of the adult population reported as regular users in 2016 (Larsen et al., 2018). Since cannabis is an illegal drug, it has been confiscated frequently in Greenland (Grønlands Politi, 2023). However, the drinking and addiction pattern is not unique to Greenland as similar trends have been observed in other indigenous and Arctic populations (Allen et al., 2011; Brett et al., 2016; Gray et al., 2018; Lee et al., 2019).
Social inequality in Greenland is high, particularly among those who drink the most (Departementet for Sundhed og Infrastruktur, 2014). In 2014, it was estimated that approximately 13 deaths each year were directly caused by alcohol, and hospital stays caused by alcohol were estimated to cost 8.7 million DKK each year (ibid). The extent of addiction problems within certain parts of society and across generations was revealed that, among individuals attending addiction treatment, 97.5% had grown up in homes with addiction issues and 89% had siblings who also had addiction problems (ibid). The cost of addiction problems in Greenlandic society in 2013 was estimated to be in the range of 271–338 million DKK per year, accounting for not only healthcare costs but also the added expense of social services, productivity and crimes (Departement for Sundhed, 2015). Addiction problems have consequently drained resources from various regions of Greenland and its population for decades.
Over time, addiction treatment services in Greenland have evolved in various forms and been a subject of political debate (Rosenqvist, 2001). Initially, public healthcare facilities across the country only offered detoxification for alcohol withdrawal symptoms and pharmacological treatment (e.g., Disulfiram) to promote abstinence (Niclasen & Poulsen, 2020). In 1985, the AA movement was initiated by private individuals in south Greenland, which eventually led to the establishment of a certain level of partnership between the government, municipalities and private treatment organisations in Denmark and Iceland to secure access to treatment services based on the 12-step model for treatment (Humphreys, 2002). In 1995, the Greenlandic government opened the first treatment facilities in Qaqiffik, in the towns of Nuuk (the capital) and, for a short period, in Ilulissat. The treatment in these facilities was also based on the 12-step model of addiction treatment and treatment services were offered in collaboration with a private treatment institution from Denmark. However, in 2011, based on a call for tenders, the public healthcare system on behalf of the government terminated the collaboration (Niclasen & Poulsen, 2020). From 2012, the responsibility of addiction treatment was appointed to another private facility in Nuuk offering treatment for addictions, albeit still treatment based on the 12-step model of addiction. The municipalities became responsible for referrals and payment of the treatment, while the healthcare system paid for travel (from other places) to and accommodation in Nuuk. This setup left the availability and direct access to treatment unchanged, as only the residents of Nuuk (30% of total population) had direct access to treatment. The treatment gap remained large, since the number of patients referred to treatment in Nuuk was only approximately 2000–300 a year (Departement for Sundhed, 2015; Departementet for Sundhed og Infrastruktur, 2014), while the estimates from the population health surveys indicate that 36% of all participants wished to change their alcohol intake (Larsen et al., 2018).
In 2016, the government thus introduced a new addiction treatment service, Allorfik. Allorfik had the goal of providing easily accessible treatment for problems with addiction to alcohol, cannabis and gambling, and to be situated locally, closer to the population. This resulted in an introduction of a new treatment methodology and five new treatment centres over the course of 2.5 years and as such was a radical change to the previous ways of organising addiction treatment services with only one treatment facility available in Nuuk in addition to sporadic treatment courses by traveling counsellors outside Nuuk. The introduction of Allorfik and the improved accessibility of treatment had a notable impact on the demographics of treatment seekers. Compared to those attending the central treatment facility in Nuuk, individuals seeking treatment at local Allorfik centres were predominantly women who were employed and had families. In contrast, the central facility in Nuuk primarily treated unemployed men without families (Flyger et al., 2019).
Aim of the present study
The present study poses the research question: what happened in Greenland at a political and civil servant level that led to a new strategy for addiction treatment in 2016? The aim of the study was thus to explore the publicly available documents on addiction problems (with alcohol, cannabis and gambling) that described the needs of and wishes to change how treatment is offered (i.e., government and academia) leading up to the government decision to implement the current national strategy for treatment of addiction in Greenland.
Context
Greenland has a population of approximately 56,600 people with roughly 60% living in one of the five main cities in each of the five municipalities; 25% live in smaller cities and approximately 15% live in remote villages. The infrastructure in Greenland is difficult, with no roads connecting cities or villages. Transportation between inhabited areas is thus organised by airplane, helicopter or boat. This difficult infrastructure also makes access to, for example, healthcare services, difficult and very dependent on the residential area, with the only major hospital located in the capital, Nuuk, and larger healthcare facilities located in each of the five biggest cities and small facilities with only a nurse or healthcare assistant present in smaller inhabited areas (Niclasen & Mulvad, 2010). Greenland's culture is rooted in Inuit heritage, with hunting and fishing remaining integral to daily life for the majority, and many Greenlanders are employed in the fishing industry today (Andersen, 2008). This is also reflected in the way health and well-being are perceived more holistically with, for example, mind, body and spirit, and local Greenlandic food as important determinants for health (Departement for Sundhed, 2020).
Greenland, a self-ruling part of the Danish Realm (i.e., the Kingdom of Denmark) since 2009, previously held the status of a Danish colony. In the transition from colony to first home rule in 1979 and later to self-rule in 2009, different government departments have transferred from Danish authority to Greenlandic authority, e.g., the healthcare system in 1992 (Statsministeriet, 2023). At the time of the handover of the national healthcare system, addiction treatment services were not initially implemented in Greenland and it remained the responsibility of the Greenlandic Government to introduce these services (Niclasen & Poulsen, 2020; Poulsen, 2012)
Today, Greenland operates as a representative democracy with three levels of government: municipal; national; and the Danish parliament. In national elections for the Danish parliament, Greenland elects two representatives from a single constituency. Municipally, elections occur every 4 years, with constituencies corresponding to the five municipalities. At the national level, members of the Greenlandic parliament, Inatsisartut, are elected for 4-year terms from a single constituency. Shortly after parliamentary elections, a constituent assembly convenes to elect the Inatsisartut chairman, government (Naalakkersuisut), and schedule the two annual parliamentary sessions (spring and fall assembly) (Inatsisartut, 1994). Over the years, Greenland has seen the presence of various political parties. One of the most dominant parties historically and presently is Siumut, a social democratic party. In the election leading to self-rule in 2009, the Inuit Ataqatigiit (IA) party, a democratic socialist party, secured the majority vote and took leadership of Naalakkersuisut (Dahl, 2010). Today they again hold the majority of vote and the chairmanship of Nalakkersuisut (Press, 2021).
Methods
The present study was inspired by the stages of a scoping review framework (Arksey & O’Malley, 2005) and performed the following steps: identified the research question; identified relevant documents and selected these; and charted the documents in tables and reported these in the results section as prescribed in the framework (ibid). It was very clear from the beginning that the study had to rely on many different types of literature e.g., journal articles, reports, government and political documents, and thus could not follow the original thoughts of a scoping review as prescribed by Arksey and O’Malley as it could not compare peer-reviewed journal articles of different studies. Thus, the scoping review framework was used as inspiration for a step-by-step guide on how to progress and scope across different types of literature and sources.
Data
We performed a systematic search of the following databases and digital platforms: www.ina.gl; www.naalakkersuisut.gl; www.bibliotek.dk; www.peqqik.dl; PubMed; Web of Science; and Embase. We retrieved data from academic papers and reports, political documents and minutes from meetings in the parliamentary Family and Health Committee when debating addiction treatment. The political documents were retrieved from www.ina.gl, while governments documents were retrieved from www.naalakkersuisut.gl and www.peqqik.gl. For scientific documents, www.pubmed.com, www.WebofScience.com and www.embase.com were searched. We searched www.bibliotek.dk for documents in Danish and Greenlandic. The search continued using a snowball method for additional literature, i.e., all references were examined for additional relevant documents; if any were found, the references of those documents were also searched. With recurring authors, their works were also examined. The study did not include newspaper documents as there is no media-monitoring organisation in Greenland yet. As Danish and Icelandic databases do not include recent Greenlandic media, a search was not feasible. The search was limited to the years 2010–2016, when the present national strategy was decided upon and initiated.
We searched for peer-reviewed documents in the Pubmed, Web of Science, and Embase databases with the following search: (greenland) AND (((gambling OR betting OR wagering) OR (cannabis OR marijuana OR (medical marijuana) OR hemp OR cannabinoids)) OR (alcohol OR (binge drinking) OR intoxication OR (alcohol use disorder) OR (drinking pattern))). The search was limited to studies in Greenland only. We used the same search terms in Danish when searching for other documents; again, this search was limited to documents only from Greenland.
As a first step, documents were screened from the title and, if applicable, the abstract. Content relating to the treatment of other diseases was excluded, e.g., alcohol use included only as part of a dietary intake. We had several results regarding other types of healthcare treatments in Greenland but only a few were related to addiction treatment, as demonstrated in the results section. In the next step of screening, the full document was read through. We searched for documents describing the intentions and perspectives on the extent of addiction problems, future directions for addiction treatment and expectations as to what the treatment services should entail. We included documents that describe or analyse issues related to alcohol, cannabis or gambling addiction as well as addiction treatment services. We also included documents that contained perspectives on the extent of addiction problems and suggestions for addressing these issues that were not related to addiction treatment services.
Analysis
We performed a document analysis (Bowen, 2009) of the available literature detailing the addiction treatment service in Greenland for historical context. We read through each document and searched for descriptions of treatment needs, perspectives on the severity of addiction problems in society and objectives for future treatment services. We extracted data in categories and thereafter assembled the documents in three major themes and reported the different perspectives. The analysis also identified significant events and the connection between different events and important documents for the process leading to the new addiction treatment strategy.
Results
The search for documents provided the following results: WebofScience = 67; Pubmed = 54; Embase = 322; Ina.gl = 263; Naalakkeruisut = 13; and Bibliotek.dk = 137. The snowball method provided five scientific documents that were included. The screening process is illustrated in Figure 1. In total, 54 relevant documents were identified: 26 political documents; 13 government documents; and 15 scientific documents. Most of the literature was published in Danish and Greenlandic only; of the scientific publications, only nine were in English and published in peer-reviewed literature.
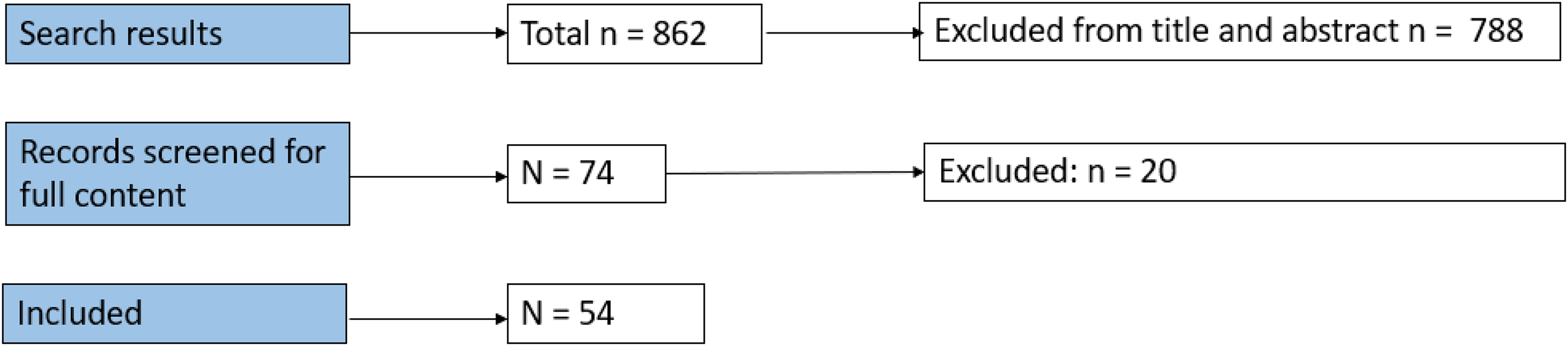
Stages of document screening and inclusion.
We identified three main themes within the available literature on addictive behaviours and the development of addiction treatment services in Greenland: the national debate on addiction problems; the strategies and action plans of addiction problems; and the mapping of addiction problems. The results are presented in this order.
The national debate on addiction problems
This theme reflects the political discussion. Table 1 shows each of the included items from the political agendas with the year, the proposer and political party, and the decision. Table 1 presents that over the years, many individuals and political parties were engaged in the discussion about addiction problems. Table 2 presents the so-called Paragraph 37 questions, 1 where questions on alcohol, cannabis, gambling and abuse problems were inquired from a member of parliament to the government. in the period between 2010 and 2016, there was a parliamentary election in April 2013 and again in November 2014.
Items on parliament agenda.
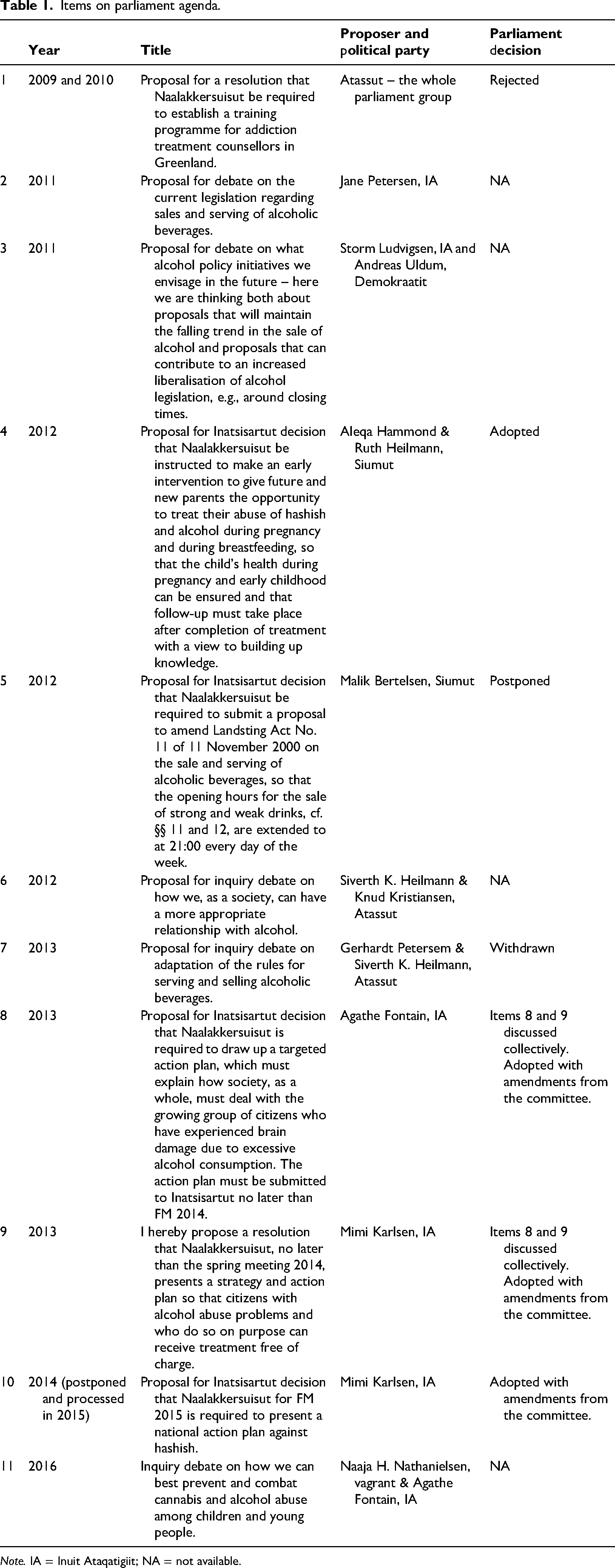
Note. IA = Inuit Ataqatigiit; NA = not available.
Paragraph 37 questions.
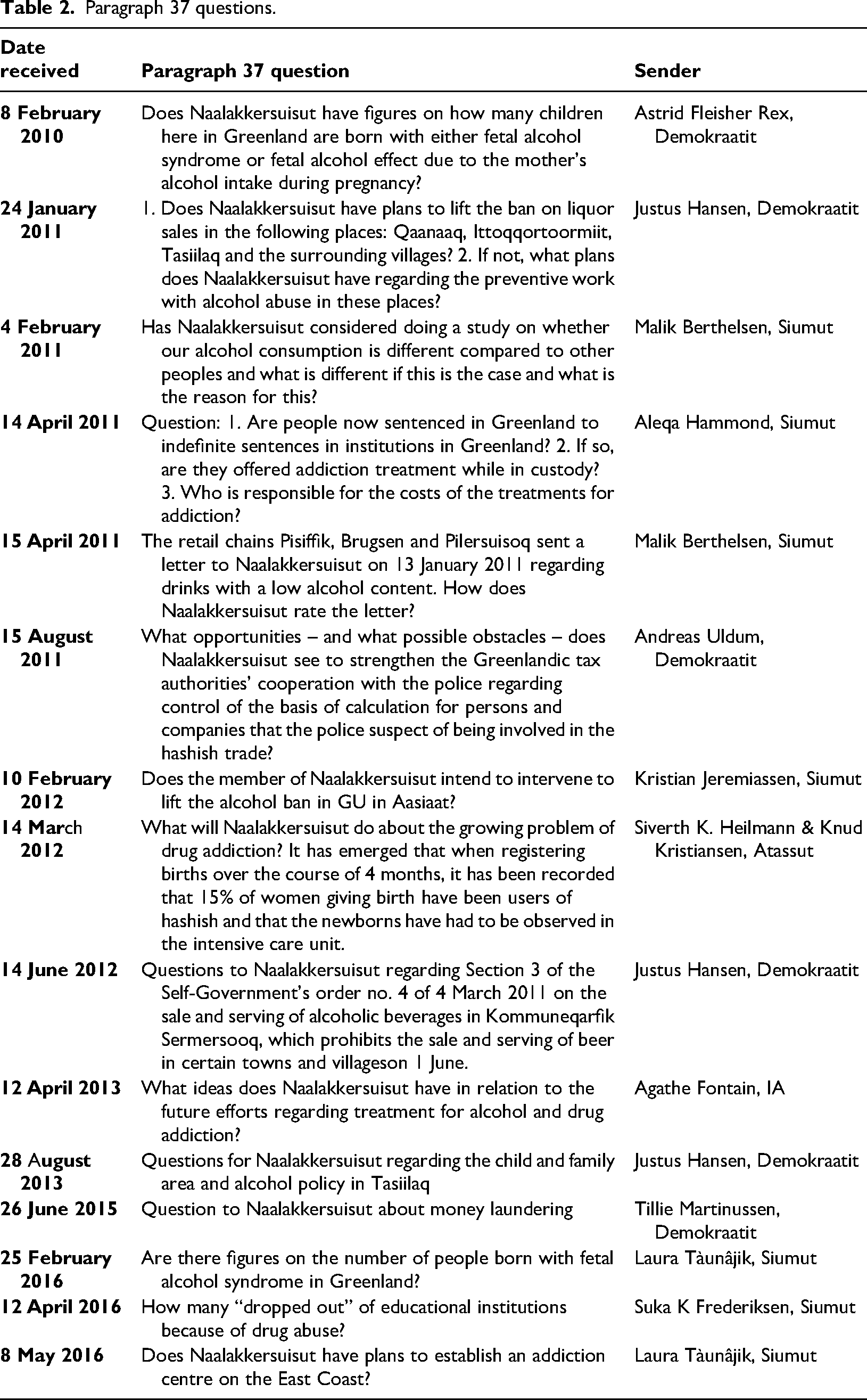
As can be seen from Tables 1 and 2, between 2010 and 2016 there were 11 items on the parliament agenda proposing debate, resolutions, decisions and/or mandating initiatives, and 15 Paragraph 37 questions for the Minister/government related to the misuse of alcohol, cannabis, abuse and/or treatment. Few of the items and questions were directly related to addiction treatment services, but all addressed the state of problematic use in part of the population and suggested or discussed different ways of offering prevention, regulation or treatment. Item 1 from 2009 and 2010 suggested mandating the government to establish a training programme for staff in, or relevant to, the field of addiction treatment in Greenland instead of using training programmes available in Denmark. At first, this suggestion was postponed, awaiting the conclusions of a government working group, and then rejected based on the argument that Greenlandic (social) education was to have extended the syllabus to cover more on addiction problems instead.
Several items and questions raised in the political debate concerned the legislation of sales and serving of alcohol. The legislation in Greenland had been quite strict since the 1980s to handle the high levels of alcohol intake back then. All political parties seemed to be concerned about the problematic use of alcohol and cannabis in a part of the population, but did, however, disagree on what effects to expect from changes to legislation and how legislation could be altered to improve the situation. Some parties were proponents of a more liberal legislation, arguing that strict policies would not alter the underlying problems of alcohol addiction while others wished for even stricter policies and arguing that addiction problems worsened all other problems in society.
Item 4 on the agenda in 2012 suggested an establishment of a treatment service or intervention aimed at vulnerable individuals (and families experiencing addiction problems in particular); this proposal was decided and left to the government to put into affect. The Paragraph 37 question from 12 April 2013 asked by Agathe Fontain focused on how to develop public addiction treatment services. The question addressed the current services and plans for adjustments but lacked background or justification, following the normal procedure. In the reply, the government briefly described a need for a more flexible treatment service for addiction but proposed no specific plans for changing the current treatment service. Agathe Fontain and her colleague, Mimi Karlsen, followed up on the question in the fall of 2013 with item 8 (from Agathe Fontain) and item 9 (from Mimi Karlsen); they suggested new initiatives on treatment for alcohol addiction. These items were discussed simultaneously as one item in both parliament and the parliamentary health committee. After being discussed twice by all members of parliament and considered by the parliamentary health committee, the proposal was adopted with amendments suggested by the health committee. The amendments to items 8 and 9 determined a process with a preceding analysis of the following: (1) the needs of the future treatment service; and (2) an analysis of the cost of not having a treatment service compared with the cost of establishing a treatment service, as well as a process including addictions other than just alcohol addiction. The government was supposed to develop a plan for a free national alcohol addiction treatment service. Thus, in the years after the adopted proposition in 2013, there were very few items on the agenda and even fewer Paragraph 37 questions for the government, indicating a kind of political peace or awaiting the outcome of the ongoing analysis preceding a proposal for an addiction treatment service model.
Item 10 from the agendas in 2014 and 2015 was treated twice, both by parliament and by the parliamentary health committee and finally adopted with amendments. The item required the government to present a national action plan against hashish, which was presented in 2016. This content is elaborated in the next section. Item 11 on the agenda in 2016 involved a debate on preventing problematic alcohol and cannabis use among adolescents. In addition, the three Paragraph 37 questions from 2016 addressed the impact of addictive behaviours on children and adolescents and the availability of treatment for the population living on the east coast of Greenland, highlighting uncertainties and unmet needs during the initial establishment period of the new treatment service. As can be seen in Tables 1 and 2, questions and items on the agenda began to emerge again in 2016 while the establishment process was presented and initiated.
Strategies and action plans for addiction problems
In Table 3, the 11 government documents identified regarding addiction problems are presented and all reflect work within action plans, strategies and prevention work about addiction problems in society.
Government.
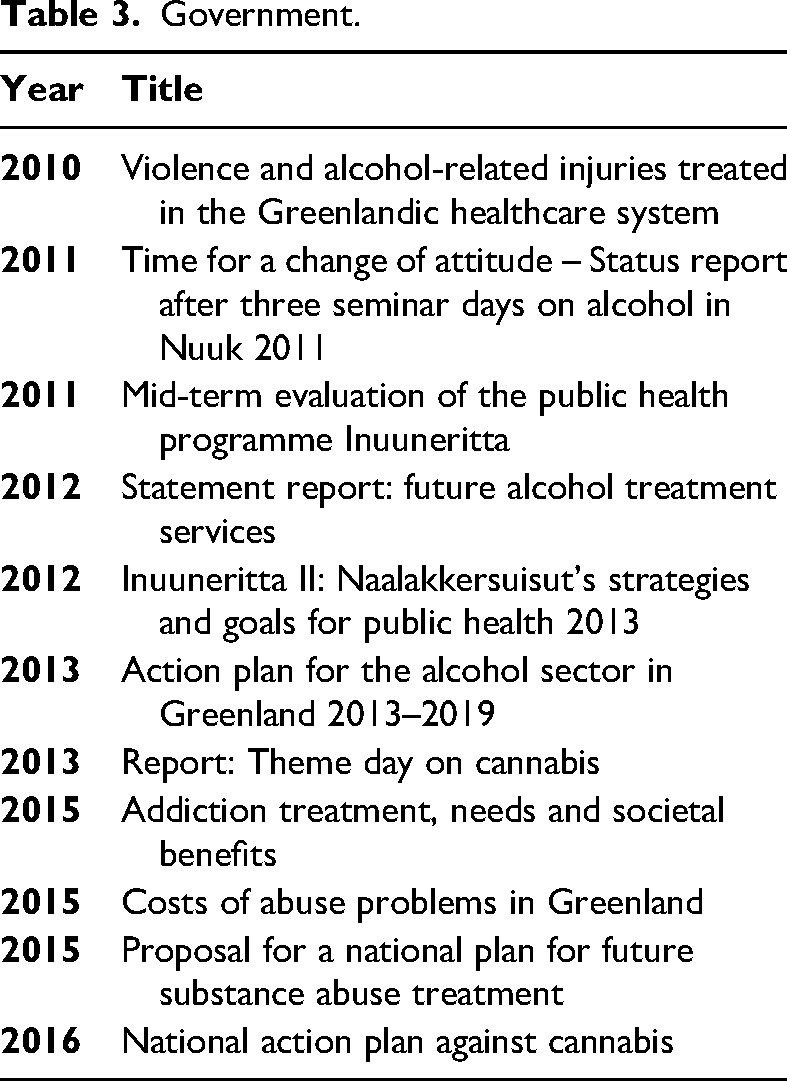
In 2010, the government published a report on violence and alcohol-related injuries treated in the Greenlandic healthcare system. The findings, analysis and conclusions from the report were also presented in a scientific peer-reviewed article (Nexøe et al., 2013), describing how violence and alcohol-related injuries put a considerable strain on the healthcare system as at least 10% of emergency visits were due to alcohol intoxication. In 2011, the government invited an interdisciplinary group of professionals to participate in a thematic meeting on alcohol. The presentations, discussions and recommendations from this meeting were presented in a report with the title ‘Time for attitude change’ (Departement for Sundhed, 2011). The 2012 statement report on future alcohol treatment services described how the structural reform (concerning the number of municipalities and their responsibilities) in 2009 was also intended to include a redistribution of the responsibility of addiction treatment from government to the five new municipalities, as the prior municipalities had wished for local treatment options. However, this work was postponed until 2010 when it was decided that members of the government and the municipalities should develop a proposal for the future services of addiction treatment; the 2012 statement report was the result of this work. The suggestions in the statement report did not alter the structure of the service but recommended a development of the treatment of addiction service based on evidence-based treatment methods, better and more uniform referral practice, establishment of an outreach team of counsellors to provide local treatment in the small living areas and the establishment of local, specialty services aimed at people with addiction problems, mental illness and social problems.
In 2013, the government presented an action plan for addressing alcohol-related issues. The action plan was presented together with the national public health strategy, Inuuneritta II (Departement for Sundhed, 2012), by the Ministry for Health and had 11 sub-goals closely connected to the goals of Inuuneritta II, with the overall aim of increasing the quality of life for the population. The action plan and Inuuneritta II both focused on primary prevention, healthy lives and well-being for the population; in particular, it focused on children and families. Inuuneritta II was built on the recommendations from the 2011 publication, mid-term evaluation of Inuuneritta, which was also the only document identified that evaluated previous work or initiatives. As part of the Inunneritta II strategy, four pamphlets were published and distributed to schools, providing information for teachers and parents on how to protect children and adolescents from the misuse of alcohol, drugs, and tobacco.
The mandated analysis after the adoption of items 8 and 9 on the parliamentary agenda in 2013 resulted in three reports: (1) Addiction treatment: needs and societal winnings (Departementet for Sundhed og Infrastruktur, 2014); (2) Costs of addiction in Greenland (Departement for Sundhed, 2015); and (3) Proposal for the future national addiction treatment services (Departement for Sundhed og Infrastruktur, 2015), all presented in 2015. In the report on needs and societal winnings, the background information was very much reliant on the national population health surveys, surveys on health behaviours in schoolchildren, the available literature and a statistical summary of the patients treated for addiction treatment with government support for the year 2013. The report estimated that approximately half the population might have a harmful use of alcohol and that far more men than women were at risk (Departementet for Sundhed og Infrastruktur, 2014). The report also identified a significant negative social impact of addictive behaviours, noting that individuals with fewer resources tended to have a higher proportion of addiction problems. Among those receiving addiction treatment, only 2.5% had not experienced addiction problems in their childhood home (ibid). Very importantly, the report concluded that there still seemed to be a mismatch between the allocated resources to addiction treatment and the need for treatment, resulting in the majority of individuals being unable to access necessary interventions for their addiction problems. The report on the cost of addiction and harmful use of alcohol estimated that between 271 and 338 million DKK each year were attributable to addiction (Departement for Sundhed, 2015). This estimate included direct costs from healthcare, social services, wage loss and crime; however, it was not possible to include indirect costs, e.g., missed opportunities in education. The cost of extra services in schools, such as special teaching and guidance related to addiction, were not included but were estimated to be 4–8 million DKK a year. At the time of the report, the gross domestic product (GDP) of Greenland was 13.8 billion DKK; thus, the costs of addiction were assessed at being a minimum of 2% of the GDP (ibid).
The proposal for the future national addiction treatment service (Departement for Sundhed og Infrastruktur, 2015) was distributed to all members of parliament in the fall of 2015. It was subsequently included (without further political discussion) in the Finance Act negotiations, where it received the necessary funding and went into effect from 2016 onwards. The plan described an addiction treatment service directed at different age and target groups and was based on available evidence and best practice. The service was meant to include a central knowledge and management centre, local treatment centres in each municipality and outreach counsellors to provide treatment to smaller cities and villages. It was suggested that the service involve a stepped care model, which involves an evidence-based approach offering the least invasive yet effective treatment options as soon as possible. The steps in a stepped care model should increase the efforts as the severity of the problem rises (NICE, 2011). The proposed stepped care model in this case involved the following steps:
Step 1: Information about the service Step 2: Self-help materials, e.g., self-screening tests Step 3: Motivational interviewing (for all with addiction problems and some as the only service) Step 4: Outpatient treatment service or short treatment courses of 1 week with a traveling counsellor in smaller cities or with well-functioning people in bigger cities Step 5: Day treatment locally and regionally for people with more support and complex needs Step 6: Day treatment in combination with social/educational service for, e.g., pregnant families with addiction problems Step 7: Specialised treatment services for children, adolescents and adults with mental disorders
In 2015, when the report was presented, only step 5 in the proposal existed. Step 5 was at that time delivered by a private provider, hired by the government, and consequently, everything else in the stepped care model had to be developed and implemented. The plan also described how all people seeking treatment should be offered motivational interviewing (Miller, 1983) as well as a being assessed by means of the Addiction Severity Index (McLellan et al., 1992). The proposed service also contained several key elements to ensure successful outcomes for the people in treatment: the first element was a close collaboration between the healthcare system and social services. Additional elements were dissemination of information aimed at the general population and target groups, multidimensional assessment of all people in treatment, a carefully planned and structured follow-up procedure, action plans resolving the problems of individuals identified through the initial assessment, multidimensional treatment services and aftercare, self-help groups, a national addiction database collecting the information on the service allowing for quality assurance and development, and finally a training programme for the counsellors who delivered the new treatment services.
In 2016, a national action plan for the prevention of cannabis use was presented by the government. This plan was a result of the adoption of another political point from the agenda: item 10 in 2014. It also presented a broad range of prevention initiatives, including those involving the new treatment service, thereby supplementing the plan for providing addiction treatment.
Mapping of addiction problems in the population
As can be seen in Table 4, 13 scientific documents were identified in the period 2010–2016; these were mostly related to mapping (general health and) the extent of addiction problems in Greenland.
Academia.
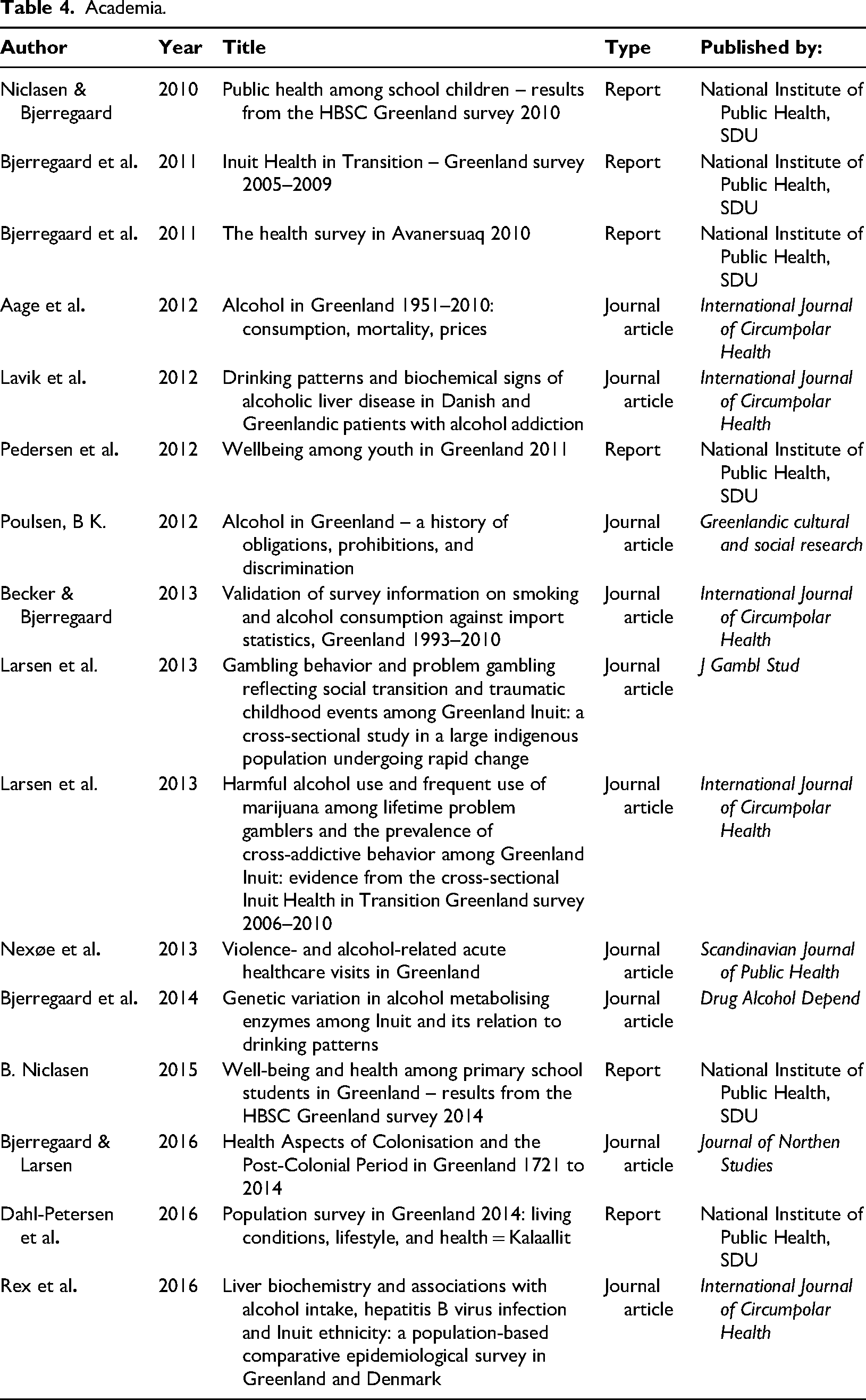
The scientific documents identified were almost all written by or in collaboration with the Center for Public Health in Greenland, National Institute of Public Health, University of Southern Denmark and relied mostly on data gathered in the National Population Health Surveys or the Health Behavior in School Children (HBSC). All documents displayed the significant proportion of addictive behaviours in the society. In the population health surveys (Becker & Ulrik, 2013; Bjerregaard & Aidt, 2010; Bjerregaard & Dahl-Petersen, 2011; Bjerregaard et al., 2003; Pedersen & Bjerregaard, 2012), many aspects of health were investigated, and alcohol intake levels were reported in each of them. In the latest survey, 8.8% of participants exceeded the recommended level of alcohol intake in a week (seven for women and 14 for men) and approximately 10% had a harmful use or depended use of alcohol (Larsen et al., 2018); however, the biggest concern was binge-drinking, as 34% reported to binge-drink in 2018 (ibid) and approximately 40%–50% of participants reported to binge-drink at least once a month in previous surveys (Dahl-Petersen et al., 2016). Aage investigated the alcohol intake levels from the 1950s and the related mortality and found an increasing trend of alcohol intake from the 1950s until the peak level in around 1987, whereafter the intake decreased. Aage also found that the mortality rate followed the intake pattern and the levels of alcohol-related liver disease mortality were lower than expected (Aage, 2012). Lavik and colleagues and Rex and colleagues also investigated liver disease in individuals with alcohol addiction problems in Greenland and Denmark; both found low levels of liver disease in Inuit (Lavik et al., 2006; Rex et al., 2016). The study by Lavik et al. was the only one related to addiction treatment services as the investigated population were patients in treatment. Becker and Bjerregaard found a significant underreporting of alcohol intake in surveys compared to import statistics (Becker & Ulrik, 2013). Larsen and colleagues investigated gambling behaviour and found gambling behaviour to be associated with adverse childhood experiences, and harmful use of alcohol and cannabis (Larsen et al., 2013a, 2013b). Nexøe and colleagues (Nexøe et al., 2013) described how alcohol-related injuries caused a high need for other types of healthcare treatment in the emergency wards. Bjerregaard and colleagues (Bjerregaard et al., 2014) investigated genetic variation in alcohol metabolising enzymes and found a genotype that is protective against heavy drinking among the Inuit. Finally, Bjerregaard and Larsen also investigated health aspects of Greenland's colonial history and found that mental health, addiction and suicide problems were related to the colonial history of Greenland (Bjerregaard & Larsen, 2016). The HBSC surveys have been carried out regularly in Greenland since 1994 and have investigated the health, behaviour and well-being in children from the 5th grade to the 10th grade in randomised samples of all schools in Greenland. The 2016 report found a decrease in alcohol intake and a later onset of alcohol intake; however, cannabis was used by 27% of the group aged 15–17 years (Trivsel og sundhed blandt folkeskoleelever i Grønland : resultater fra skolebørnsundersøgelsen HBSC reenland i 2014, 2015).
Discussion
The reviewed documents in the present study highlight significant attention from researchers, government and politicians towards the problematic use of alcohol, other substances and addictive behaviours in Greenlandic society. The political documents demonstrated a strong and continued interest in addiction problems over the years; however, despite numerous discussions, only a few solutions were proposed. Although there was overall high interest and concern about addiction problems, an analysis of the political documents identified two more dominant opposing sides of the debate. Siumut, the largest political party in parliament, was concerned with addiction problems but did not take a firm standpoint. Rather, the party’s position was inconclusive, as their proposals and questions veered in many directions, addressing both the prohibition and expansion of sales hours for alcohol as well as early intervention for vulnerable groups. One side – led by the parties Atassut and Demokratiit – was concerned with addiction problems but believed that strict legislation had not resolved the underlying problems causing addiction. They argued for a more liberal approach to the legislation of alcohol sales and service. The opposing side – mainly led by the party IA – argued for stricter policies and the acknowledgement of addiction problems as diseases that should be dealt with through treatment service, positioning it as a government responsibility. Agatha Fontain and Mimi Karlsen, both from IA, were central figures in the debate. Before the election in April 2013, they were both members of government and hosted conferences and meetings about addiction problems; however, as shown in the analysis, they were not otherwise active in presenting new initiatives for the prevention or treatment of addiction problems. After the election in 2014 when they were no longer in government, it seemed that they seized the opportunity to propose a radical change to the treatment system.
The present review and analysis demonstrated that the government's efforts in the field were significantly determined by the adoption of items from the parliamentary agenda. For a long time, the government focus was on primary prevention initiatives and information campaigns rather than on structural changes or treatment of addiction problems. Thus, the governments seemed more engaged in the promotion of healthy lives to prevent people from developing addictive behaviours than on initiating or restructuring (more expensive) treatment of addiction problems. This could be the result of changing government and their shifting agendas; however, the responsibility for primary prevention work was largely centred in the Department of Health while the scope of prevention seemed to depend on progress in other areas, such as education, employment and housing (Bjerregaard et al., 2020; Bjerregaard & Larsen, 2016, 2018; Larsen et al., 2013b; Seidler et al., 2022).
Among the identified documents, only one tried to assess the effects or impact of an initiative: the mid-term evaluation on the public health programme Inuuneritta in 2011. This evaluation stands out as a rare instance of assessing the outcomes of an initiative within the collected literature. The scarcity of impact assessments is notable when considering the extensive number of meetings, discussions and monitoring studies conducted over the span of 6 years. This discrepancy underscores the need for more comprehensive evaluations to gauge the effectiveness and real-world impact of initiatives aimed at addressing societal issues, such as addiction and public health, within Greenlandic context. In Denmark, the obligation to offer treatment for alcohol addiction to citizens has shifted across different administrations over time; however, this responsibility was not included in the 1992 handover of the Greenlandic healthcare system from Denmark to Greenland. As a result, the initiation and management of alcohol addiction treatment were left to the Greenlandic authorities. Previous addiction treatment in Greenland was heavily linked to private treatment initiatives in Denmark, with both collaborations and education of treatment counsellors in Denmark. This treatment largely followed the 12-step model of addiction treatment (Niclasen & Poulsen, 2020). Although studies from northern Norway with Sami people (Mehus et al., 2019) and studies of Greenlanders in Denmark (Edwards et al., 2019) provide evidence that cultural safe practice have a positive impact on health, the documents in the present review revealed no significant interest in developing culturally adjusted addiction treatment in Greenland but seemed more concerned with monitoring and regulating the situation. In Alaska, a focus on addiction problems and suicide resulted in a collaboration between academia and native communities on the development of solutions to the health disparities (Allen et al., 2014). The Greenlandic process was quite different and could be related to the fact that while Greenlanders in Denmark, Sami in Norway and Alaska Natives in Alaska were all minority parts of the population, the Greenlanders were by far the majority of the population in Greenland itself. It could also be related to the transition process from colony to home rule, where decades were spent creating equal welfare opportunities in Greenland to those in Denmark (Beukel et al., 2007; Rud, 2014, 2017) and thus the foundation of the Greenlandic government and welfare system were based on Danish practices.
The present study describes the processes that led to the establishment of the current national addiction treatment service in Greenland. The inclusion of parliamentary debates and governmental reports and documents provide a broad perspective of the incentives behind establishing a new service, an insight that a search limited to scientific literature would not have provided. The scientific literature and much of the background material for the governmental documents (such as reports) relied on the national population health surveys conducted by the National Institute for Health, providing a rather limited perspective being the only source of information and performed by primarily Danish researchers. On the other hand, the population health surveys have been conducted regularly and over many years; they are thorough and methodologically sound; thus, data from the surveys can be considered reliable.
The extent to which the current strategy for addiction treatment delivery has succeeded and been implemented, and whether it has led to the expected improvements and results, needs to be investigated further. This will be the next step in the present study.
Conclusion
Across the three identified themes – the national debate, the strategies and action plans, and the mapping of addiction problems – it became evident that addiction issues held significant societal importance in Greenland. While numerous documents related to monitoring, debates, strategies and regulatory measures were found, very few focused specifically on addiction treatment. The academic documents have only focused on monitoring and the government documents were mainly mandated work from parliament.
Our analysis highlighted three key documents central to understanding the path towards a new national addiction treatment service. First, a 2012 statement report outlined the transfer of addiction treatment service responsibility to the municipalities in 2010, underscoring the subsequent ineffectiveness in addressing addiction problems. In 2013, Agathe Fontain (IA) raised a Paragraph 37 question highlighting a lack of progress. Later that same year, Agathe Fontain and her colleague Mimi Karlsen (IA) proposed two parliamentary agenda items mandating the government to develop a plan for a new addiction treatment service, provided free of charge and accessible to a larger segment of the population.
These parliamentary actions ultimately led to the implementation of the new service. The identified documents collectively highlight the challenges faced in addiction treatment, the acknowledgment of addiction problems as persistent issues within the Greenlandic society, and the essential steps taken to address these concerns through policy and legislative actions. This study thus informs future studies on addiction treatment in Greenland by situating the historical context of the changes that occurred with the introduction of Allorfik.
Footnotes
Acknowledgements
The authors would like to thank the reviewers for a very helpful review process.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.