
Abstract
Aim:
In increasingly market-oriented welfare regimes, public procurement is one of the most important instruments for influencing who produces which services. This article analyses recent procurement regulations in four Nordic countries from the point of view of addiction treatment. The implementation of public procurement in this field can be viewed as a domain struggle between the market logic and the welfare logic. By comparing the revision of the regulations after the 2014 EU directives in Denmark, Finland, Norway, and Sweden, we identify factors affecting the protection of a welfare logic in procurement. We discuss the possible effects of different procurement regulations for population welfare and health.
Data and theoretical perspective:
The study is based on the recently revised procurement laws in the four countries, and adherent guidelines. The analysis is inspired by institutional logics, looking at patterns of practices, interests, actors, and procurement as rules for practices.
Results:
Procurement regulations are today markedly different in the four countries. The protection of welfare and public health aspects in procurement – strongest in Norway – is not solely dependent on party political support. Existing service providers and established steering practices play a crucial role.
Conclusion:
In a situation where market steering has become an established practice and private providers are strongly present, it can be difficult to introduce strong requirements for protection of welfare and population health in procurement of social services.
Keywords
Introduction
In increasingly market-oriented welfare regimes, public procurement is regarded as one of the most important instruments for decision-makers to regulate who produces services and which services are produced. Some argue that the expectations on procurement in this respect have been too high (M. Ukkola, Senior Ministerial Secretary, Finnish Ministry of Economic Affairs and Employment, interview, April 11, 2017). Others have pointed out that the procurement of social services and the like may involve specific challenges from a welfare perspective (Schneider, Karlsson, & Stenius, 2016). This, in turn, may influence a service system’s potential to have a positive impact, in our case on substance use problems, at both individual and population levels (Babor, Stenius, & Romelsjo, 2008; Storbjörk & Stenius, 2019).
With this in mind, and because there has been virtually no research attention to procurement regulation in service systems which have previously not been governed by market forces, such as the Nordic welfare models, this article analyses how four Nordic welfare countries have regulated and used public procurement as a steering instrument in a subfield of health and welfare services. Our specific point of departure is the system for addiction treatment, primarily located within the field of social services (but also handled within healthcare), hence the special focus on social services and social service professions in this article. The implementation of public procurement in this field can be viewed as a domain struggle between two competing logics: the market logic and a welfare state logic. We aim to describe how this struggle has evolved in Denmark, Finland, Norway, and Sweden, identify some of the factors and arguments behind the differences in the developments, set out the current state, and briefly discuss the possible effects on welfare and public health of the different Nordic applications of the EU procurement directives on addiction treatment.
Research on contemporary health and social care institutions has identified different core logics that define their development. In an analysis of the US healthcare system in the 1990s, Scott, Ruef, Mendel, and Caronna (2000) found three fundamental logics: the logics of the market, of the democratic state, and of the medical profession. These differ in relation to the core actors/professionals, the goals and norms (conceptions of phenomena), and means/methods or practices, including regulations of the field. Adapting the conceptualisation of Scott et al. to the Nordic welfare states, we identify three logics within addiction treatment: the welfare state logic, the logic of the social work profession, and the market logic.
The welfare state logic can be described as a merger of political (democratic) and bureaucratic logics. The perspective clearly includes the welfare of society as a whole and is concerned with the common good and public health. The universal Nordic welfare policy regards provision of financial benefits and social services to those in need as a route to general social security, social equality, and a participatory society. The logic also stresses the rights of more marginalised citizens to the services they need – even if these services are at times conditional on needs assessment. The welfare of citizens is a public responsibility. Services are tax funded and redistributed both horizontally (across the life course) and vertically (towards the least well off) by political decisions according to acknowledged needs, in a politically planned and cost-conscious way and with the help of a bureaucracy that acts according to transparent rules (laws and other regulations) (see Bergqvist, Yngwe, & Lundberg, 2013; Esping-Andersen & Myles, 2011), and with professional expertise.
In a welfare state system, the public sector has the primary responsibility for provision of social services, including those of addiction treatment. In the Nordic countries, with a central locus in the municipality, the public provision has, in a corporatist tradition, and since the establishment of a welfare system, been complemented with provision by third sector (non-governmental, non-profit) organisations. These tend to have a background in civil society, in religious or voluntary organisations, focusing particularly on citizens with special needs (Bjøru et al., 2019; Stenius, 1999).
With the growth and increasing complexity of the welfare systems, more attention has been directed towards developing treatment systems. In addiction treatment systems, the treatment emphasis has been on professional expertise safeguarded by evidence-based methods and a systematic collection of professional experiences. Apart from this, the development efforts have focused on the availability and accessibility of services, particularly stressing outpatient treatment and diversity of services, continuity and integration of various services for complex problems, and user involvement. These emphases correspond to requirements for service systems that will serve public health, as described by Babor et al. (2008) in the conceptual model of population impact of treatment systems (further elaborated in Babor, 2015; and Babor & Poznyak, 2010).
Social work, with a focus on the problems and the immediate circles of the often less-resourced individuals and the community as a whole (Lindqvist & Nygren, 2016), is the profession par excellence that carries the logics of the local Nordic welfare system and its bureaucracy. This social work professional logic is, however, today influenced not only by welfare politics and goals, through legislation and professional ethics, but is also increasingly under the influence of New Public Management (NPM) in institutional settings (Dellgran, 2016; Storbjörk & Samuelsson, 2018). Stricter economic frames, more measurements of workflows and outputs, increasing specialisation, and fragmentation of treatment organisations challenge the holistic or population perspectives of social work.
Ideally, according to the market logic, where procurement practices have their roots, cost-efficient and high-quality services are best produced in a market where private providers compete as freely as possible with each other, and at times also with not-for-profit and public providers. In a quasi-market, which is funded by public money, the market is steered by purchasers or through autonomous customer choice. The field is regulated either by contracts between public purchasers (politicians/officials) who define what they want to purchase, and providers (private and public) who have an economic interest in providing requested services in a cost-efficient way, or, in the case of consumer choice, by accreditation of producers. The functioning quasi-market presupposes non-discrimination of competing service providers, well-informed purchasers with clear specifications of what they want, and/or autonomous customers who can make an informed choice as customers. It is believed that bad providers will run out of business when purchasers or customers choose other services (Bjøru et al., 2019; Freidson, 2001; Klingemann & Storbjörk, 2016).
The perspective of the market that became stronger in the wake of the European Union enlargement to include Finland and Sweden in the 1990s does not include direct references to the well-being of all citizens or a common good. It does not specifically address the abilities or needs of less resourced citizens. It does not require that private providers have a societal focus, and accepts that for-profit providers promote the interests of their owners, for example by aiming for profit. The market perspective focuses on contractual relations between purchasers and providers concerning specific services or on individuals’ personal choices. In a purchasing procedure, and recognising that not all social service users are ordinary, well-resourced customers, the public purchaser has the responsibility to define the various needs within the population, to specify accordingly what services they want to buy with public funding, and hope for acceptable bids from providers that properly can meet individual and population-level needs.
Aims and data
In this article, we will look at how Norway, Finland, Sweden, and Denmark have accommodated the market ideologies and European Union (EU) requirements for a free market for services with the social welfare and highly linked public health perspectives. More specifically, the article looks at how these countries have adopted the EU directives on public procurement, specifically the latest Directive 2014/24/EU of the European Parliament and of the Council of 26 February 2014 on public procurement. To what extent have national procurement legislations and guidelines which are grounded in a market logic included welfare perspectives? With what arguments? How can the differences between the countries in this respect be explained by the existing organisation of services and by the strength of different actors? By comparing four countries and their adoptions of the EU directive, we can get a picture of which factors facilitate and prevent a continuous defence of the welfare and public health arguments in Nordic service and healthcare systems, within steering mechanisms that are rooted in market logics. We will also point to the possible effects of different procurement regulations for future welfare and public health.
The article is part of the research project “Benefits, tensions, and inconsistencies in the health and welfare system: The case of New Public Management in Swedish substance abuse treatment” funded by the Swedish Foundation for Humanities and Social Sciences (No. P14-0985:1). The rationale for the current analysis arose at a Nordic workshop on public procurement (arranged by the Nordic Welfare Centre, NVC, in collaboration with our research project, on December 8–9, 2016) with researchers and local and central administration representatives from the four Nordic countries. Interesting, and to the participants unknown, differences between the Nordic countries in how procurement is used in practice became visible and inspired this closer comparison of the Nordic procurement regulations and how each country responded to the latest EU directive revision. The article is based on written documents, including legislation, and interviews with key persons in central and local administrations in the Nordic countries. Laws and guidelines are continuously revised, and we cover important revisions made by the end of 2018.
Addiction treatment systems and the Nordic welfare frame
The addiction treatment systems in Norway, Finland, and Sweden all have histories that date back almost a hundred years; the Danish developments are more recent. Today, the four countries’ systems have important similar features. Treatment is, with exceptions for a very small group of privileged clients, financed with tax money and with no or reasonable costs for clients. The local level, the municipalities, have a central responsibility for ensuring provision of treatment according to the needs of citizens. Addiction problems have primarily been regarded as social problems, handled within the social services, by social workers and with lay persons’ involvement in decision-making, rather than as medical problems. Alcohol problems in Denmark have been a medicalised exception. In Norway, since 2004, the responsibility for specialised addiction treatment lies with four state healthcare organisations within a multiprofessional frame, while prevention in a broad sense, (often) care initiation, aftercare, follow-up, and social support responsibility rest with the municipality. Different civil society and third sector associations have had a crucial role both as innovators and as collaborators and providers of publicly financed treatment in all countries (Bjøru et al., 2019; Stenius, 1999). The main goals and values in addiction treatment can be economically pictured by citing the social service laws in the four countries.
The Norwegian social service law (Lov om sosiale tjenester i arbeids- og velferdsforvaltningen (sosialtjenesteloven) LOV-2009-12-18-131) states in §1 that social services shall “improve the living conditions for those who have difficulties,” and “contribute to social and economic security,… “social inclusion” and “active participation”. In the law for municipal health and social care (Lov om kommunale helse- og omsorgstjenester m.m. (helse- og omsorgstjenesteloven) LOV-2011-06-24-30) it is laid down in §3 -1 that all persons who live in the municipality shall be offered sufficient health and social care. According to §3-10, the municipality shall guarantee “that representatives for the patients and users be heard in the planning of services,” and that “the municipality shall cooperate with user and voluntary organisations”.
The Finnish social service law (Sosiaalihuoltolaki 1301/2014) declares in §1 that the purpose of social services” is to “promote welfare and security,… reduce inequality,… and guarantee sufficient and good quality services on equal conditions” In addition, social services shall “promote client centredness and the clients' right to good services”.
The Swedish social service law (Socialtjänstlag 2001:453) states in Chapter 1 §1 that social work shall “promote social security, equal living conditions, and active participation” in society, and in Chapter 2 §1 that the municipality has “the final responsibility for providing individuals with the support and help they need”. As an example, the social services shall, in accordance with Chapter 5 § 9, “actively ensure that people with substance use problems get the help and treatment they need to recover from addiction problems”.
The Danish social service law (Lov om social service, Børne- og Socialministeriets. lov nr. 573 af 24/6 2005) has a somewhat different tone. The preamble states that the purpose of the law is “to provide advice and support to prevent social problems,… to provide services that may also have preventive effects,…and to meet needs caused by disabilities or special social problems”. This help is “to promote the individual's ability of developing him/herself and to be self-sustaining or…get a better quaility of life”. Subparagraph 3 of the first paragraph stipulates that the support should “build on the individual’s responsibility to develop him/herself and use his/her potentials, as far as possible”. Help is given based on individual assessment and in cooperation with the individual, and decisions are made based on professional and economic considerations. These lines indicate the somewhat more liberal and individual-centred welfare ideology in Denmark.
Market influences and public procurement in health and social services
From the late 1980s onward, and inspired by ideologies and administrative models from the US and the UK, we see in varying degrees market-influenced steering and New Public Management in the Nordic social services, including addiction treatment systems: competition in the health and welfare sectors; purchaser–provider models; increasing performance measurement and payment models; decentralisation, economisation, and depolitisation of treatment planning; and a “customer” focus (Hood, 1995; Pollitt & Sorin, 2011; Storbjörk & Stenius, 2018, 2019). The overall pace of these developments in the Nordic countries has been somewhat different and shaped by national characteristics (Bjøru et al., 2019; Meagher & Szebehely, 2013). Another common influence on Nordic addiction treatment has been the emphasis on evidence-based methods (Edman & Stenius, 2007), simultaneously narrowing the discretion of treatment staff and increasing the professionalisation of treatment. With these new influences, and the increased availability of alcohol and other drugs, the treatment systems have become more and more complex and differentiated. All Nordic countries have experienced organisational reforms, with reallocations of the treatment responsibility and new providers.
As Nordic addiction treatment has, from the beginning, been provided by a mix of service producers, the municipalities and regional authorities have a long tradition of collaborating with and purchasing services from the third sector. Contracts per se are thus nothing new in the Nordic countries, nor is the existence of a multitude of providers. What is new is that when public administrations/local elected representatives choose to buy treatment as opposed to producing the services in house, the purchases now happen on quasi-markets, with competition as a guiding principle (Storbjörk & Samuelsson, 2018). With the EU directives on procurement and the emphasis on free movement of goods and services within the European economy, international competition has emerged as a potent factor, and new actors have also entered the Nordic welfare states.
Sweden first introduced public procurement legislation in 1992, which formalised contracts on the service market. This legislation was revised after directives from the EU, when services in addition to goods were included in the EU procurement directives from 2004. A new Swedish procurement law came into force in 2007, and the present one in 2016 (Lag om Offentlig Upphandling, LOU 2016: 1145) followed the EU Directive 2014/24/EU. While Norway is not a member of the EU, it does follow the EU directives as a member of the European Economic Area. The first Norwegian procurement law came into force in 1999, and a new one was introduced in 2016 (Lov om offentlige anskaffelser, LOV-2016-06-17-73). Finland’s first procurement law was enacted in 2007, and was equally revised in 2016 (Laki julkisista hankinnoista ja käyttöoikeussopimuksista 1397/2016). Denmark introduced a procurement law in 2005 (Lov om indhentning af tilbud på visse offentlige og offentligt støttede kontrakter C231 – 03. Lov nr. 338 2005) but it is only with the procurement law of 2015 (Udbudsloven, Lov nr 1564 af 15/12/2015) that the use of procurement within social services is seriously considered. EU directives on public procurement have thus now been adopted in all the four Nordic countries.
The core principles of the EU directives on public procurement are transparency in the process, equal treatment of all providers, open competition, and sound procedural management. The procurement regulations are designed to achieve a market for goods and services that is competitive, fair, open, and well regulated. With fair competition and a rational procurement process it is believed that public funds will be used efficiently, with the optimal relation between price and quality on goods and services (see European Commission, 2019).
The most recent EU regulations on procurement acknowledge, however, that in healthcare and social services there is often only limited cross-border interest. 1 The arrangements of service production must take into account national traditions and organisational features. For these reasons, countries are given more liberty in choosing public procurement or not. The financial threshold for compulsory procurement in these sectors is higher (750,000 euros recommended). There is also more flexibility in terms of procurement models above this threshold; this is the so-called “light regime”. Transparency and fairness in procurement should nevertheless always be guiding principles. Procurements within the light regime can be of different kinds apart from the formalised open procedure: they can take place as direct procurement from a specific producer; as competitive procurement with negotiation (a possibility to negotiate the contracts between purchase and provider); as innovative partnership for a maximum of three years, where the task to develop a new kind of service is given to a specific producer; or as reserved contracts, where the purchaser reserves the contract for certain providers (for instance non-profit providers). Procurement can be defined in volume or kind, for instance as purchasing a fixed number of beds or interventions per year or by adopting so-called frame agreements, where a provider is accepted onto a list of possible service providers that the purchasing authority can choose between.
Laws on public procurement are statutes regulating the relations between purchasers and providers. These laws amount to procedural legislation, which aims to ensure a fair and consistent application of the procurement procedure. They are not concerned with the definition of quality or quantity based on perceived public need for a service, nor with the results in terms of bad or good services (M. Ukkola, Senior Ministerial Secretary, Finnish Ministry of Economic Affairs and Employment, interview, April 11, 2017). Users of services or ordinary citizens are not parties in the contracts and cannot appeal “bad” procurement. However, as procurement is a steering instrument for national, regional, or local government, social aspects need to be considered in public procurement (Ahlberg & Bruun, 2010).
Schneider et al. (2016) produced an overview of Nordic legal regulations and information steering of procurement with relevance for addiction treatment before the recent revisions of the procurement laws. The authors concluded that before the latest revision of EU directives, the official guidelines for the purchasing of social services such as addiction treatment were fairly similar in all four Nordic countries. The procurement documents stressed that procurement should aim to purchase the best possible services with limited resources. The national legislation for health and social care, as well as national guidelines on quality care and treatment, should be decisive for defining the expected quality.
Procurement was required to be a part of the strategy for the services, implying considerations of when procurement should be chosen and what kind of procurement should be used. Also mentioned was the importance of paying attention to the clients’ experiences and expectations. Several guidelines emphasised the role of networking and negotiations in procurement processes and more evaluations of procurement processes.
The report (Schneider et al., 2016) did not address the actual practice of public procurement. There is very little research or even basic data on public procurement practices in the welfare sector in the Nordic countries (see also Vähätalo & Kallio, 2017). However, the 2016 report by Schneider et al. noted that public procurement of addiction treatment had been a challenge for many local authorities. Quality and costs were difficult to define. Procurement was not always integrated in the strategic treatment planning. Costs seemed often to guide procurement more than treatment needs. The situation for persons with complicated addiction-related problems could be particularly threatened in systems steered by procurement. On the other hand, there were also good examples of public procurement where clients had been involved in the process and the contracts were decided through negotiations between the purchaser and the providers (Schneider et al., 2016).
In the following, we will turn to a description of each of the four countries’ present use of procurement and organisational frame, the implementation of the latest EU directives on procurement (with or without references to health and social legislations and with guidelines), and the actors and arguments behind the latest regulations.
Procurement in Norway: Political protection of the welfare state, the third sector, and the service users
In Norway, the four state healthcare corporations purchase around 40% of the specialised addiction treatment from other providers (Bogen & Grønningsæter, 2016). In 2017, about half of the municipalities purchased institutional psychiatric or addiction treatment from private providers. Municipalities more commonly purchased from third sector organisations, but the increase was larger in terms of purchases from so-called commercial providers (see Bjøru et al., 2019). Purchases from commercial providers usually had the form of a frame agreement and were more common in bigger municipalities (Osborg Ose & Kaspersen, 2017). There is no overall picture of the extent to which municipalities buy prevention or outpatient services. Generally, however, the extent of commercial enterprises in the addiction treatment system is notably smaller than in Sweden or Denmark.
In 2004, the Norwegian government negotiated an exception with the EU in the national procurement law that enabled the public purchaser to reserve the procurement of social and healthcare services for third sector organisations only. Open competition was viewed by the government as a potential threat to the third sector, which was regarded as representing civil engagement and a tradition of cooperation with the public sector that should be protected from competition from commercial actors (Bogen & Grønningsæter, 2016). Commercial actors have a significant role as providers of hospital services and laboratories, while voluntary and third sector organisations focus on rehabilitation of persons with substance use related problems.
Within the specialised addiction treatment system, Norwegian third sector providers have until now often had long-term, even continuous, contracts in addiction treatment. This continuity has been a political priority. As specialised healthcare is a state activity, the government is able to directly influence the purchases of these services (while the municipalities have the freedom to make their own decisions). The long third sector contracts within specialised care have, however, been discussed, as they have prevented new actors from entering the market. The protection has also sometimes implied expensive contracts, but unlike in the other Nordic countries, demands to cut spending have not been pronounced in Norwegian addiction treatment.
While the negotiated exception of protecting the third sector in relation to the EU directive ended in 2014, it did not end the Norwegian political resistance to open competition with commercial actors within the health and social sectors. The government commissioned a special report on the legal possibilities to continue third sector protection in health and social care. The report (Fløistad, 2017) concluded that if procurement and competition are used, the purchasers have to carefully justify reserving contracts for non-profit providers in terms of availability and quality of the service. Also, any positive economic result should be re-invested in such a way as would benefit the users. Procurement reserved for third sector organisations will have to be justified, built on national traditions and political priorities, and be declared from the beginning of the procurement process. National guidelines on how to argue for special treatment of non-profit organisations would, the report concludes, strengthen the likelihood of their acceptance by EU legislative authorities.
Efforts to protect the third sector are also reflected in the new law on public procurement from 2016 (Lov om offentlige anskaffelser, LOV-2016-06-17-73). Compared to the other Nordic procurement laws, the Norwegian law is very short, comprising only 18 paragraphs. The preamble clause (§1) states that “The law shall promote an efficient use of public resources. It shall also contribute to the public sector’s acting with integrity, and ensure that the general public can trust that public procurement is performed in a way that benefits society” (our emphasis). Procurement is clearly seen as important for society as a whole, with general political implications, not only as a technical instrument. As to procurement of health and social care, paragraph 7a briefly states that the ministry will provide special regulations about procurement of these services which will emphasise the specific characteristics of the services and promote important aspects such as variation, quality, continuity in treatment, and user involvement.
The recent guidelines by the Agency for Public Management and eGovernment (Difi) for procurement of health and social services (Direktoratet for forvaltning og IKT, Difi, 2018) is a lengthy document (101 pages). The aim is to inform about the special possibilities for procurement within this sector under the new EU directives, with a particular focus on the municipalities. The guidelines start by reminding the reader of the health and social care legislation that frames these services. Public procurers are then told to bear in mind their special duty laid down in paragraph 5 of the procurement law: they should consider the environment, human rights, and other social considerations in procurement. Public contracts should acknowledge innovations as well as working and social conditions, and the latter “shall not be interpreted in a narrow sense”. The readers are also reminded of §7a of the 2016 law on public procurement and of the special quality requirements for procurement within this service field.
The guidelines go on to note that procurement in health and social care has special challenges. Procurement shall be based on a clear description of what the purchaser wants to buy and how the different bids will be rated. However, it is noted that it is not always possible to describe exactly what one wants to buy in the health and social service sector, nor what criteria are decisive for the final choice of provider. Thus, the final choice cannot always be based on written bids, but must be more flexible (p. 3).
This statement is followed by a list of characteristics that are especially important and sometimes challenging to consider when purchasing social and healthcare services. Quality is the first: it is difficult to describe in a contract as it is dependent on what the provider offers at the time and in the situation in which the service is delivered. The provider is often more informed than the purchaser about the needs of the user, about the quality of the service, and about costs. It is especially difficult to fully describe the expected quality when it comes to vulnerable users. Quality in relation to costs must also be evaluated in the long run rather than in the short term. Continuity in services is an important feature, especially for persons with chronic problems. Accessibility and acceptable prices are important. Integration of services is crucial when the service needs are complex and require collaboration between different providers. Competence and experience among the staff are other vital factors. Competition based on price may erode professional competence. User-oriented organisations can improve the service, give lower costs, improve empowerment, and reduce the need for services. User involvement is stressed. Service users’ involvement in society is often a road to rehabilitation. Voluntary support can enhance this, and it is a bonus if the provider’s service is complemented with voluntary workers. In ensuring a variety of services for different users’ needs, it is not always possible to choose only the cheapest providers. There can be competition between public production and the purchased services, but the need for purchased services must be considered in relation to what the public sector produces itself. The list ends with a description of innovative partnership.
The next section in the guidelines describes the different actors that offer health and social services. Commercial actors are present in many fields, including addiction treatment, and the reader is referred to a website presenting these actors.
The presentation of third sector organisations is much longer. The report notes that they have historically been important in the development of the welfare state, and helped to build services for less resourced citizens. It is these services that the public sector has taken over, developing new services, often stressing user influence and participation from the local society (p. 7). The third sector cannot in the same sense as commercial actors collect a surplus from their work. Many of these providers declare social policy goals and have strong connections to civil society.
In short, the guidelines are detailed and instructive, even educational. They do not in any way stress the positive impacts of market competition, but instead stress the challenges and the importance of securing good quality for often chronic and complex problems. They give a very positive picture of the role of the third sector in service production. They also emphasise the role of the service user, more than in any of the other countries.
The same picture emerges from the 2018 state budget for health and welfare. The government will add NOK 350 million earmarked support to strengthen the addiction treatment system. The government wants to increase the role of the third sector and has established a cooperation agreement between this sector and the state and the municipalities. According to the budget document, the new procurement regulations enable a focus on quality aspects that the third sector organisations traditionally have represented (Helse- og omsorgskomiteen, 2018; Statsbudsjettet for Helse og Velferd, 2018).
In a parallel development, the Norwegian Directorate of Health has introduced an accreditation system for specialised addiction healthcare. Norway implemented a system of choice in healthcare in 2015, and by the end of 2018 it was noted that addiction treatment together with mental health services made up the largest (NOK 207 million) part of the system of choice payments (Bjøru et al., 2019; Helsedirektoratet, 2019 and July 2, 2019). So far, seven non-public treatment providers have been accepted for specialised addiction treatment, fulfilling criteria for staffing, economic transparency, documentation and follow-up requirements, user involvement, and cooperation with other treatment providers. Patients within specialised healthcare are, after needs assessment, able to choose between the accredited public and private providers, with information about waiting times for each unit.
With only four purchasers of specialised addiction services – four state healthcare corporations – procurement may rather easily exceed the threshold level for health and social care procurement. The established cooperative relations between the third sector and the public providers, giving the third sector providers a strong position, together with the government policy and strict accreditation requirements, has so far prevented commercial providers from obtaining a prominent role in the regional market of specialised addiction treatment, although the situation may be different in some municipalities. On the whole, the combination of a political and economic priority of addiction treatment with the new procurement legislation and guidelines seems to protect the third sector’s strong role and a restricted influence of for-profit provision in Norway in the near future. The arguments for this are treatment quality, empowerment, and civil engagement but also have to do with (long-term) economic gains. There is also the prominent role given to service users in Norwegian procurement (backed up by the social service laws; see above), as well as the declaration that procurement shall in a broad sense serve society, downplaying a narrow economic aspect.
Procurement in Finland: With social/public health concern towards a major marketisation?
The Finnish Association of Local and Regional Authorities (Kuntaliitto in Finnish) estimated a few years ago that around 43% of addiction treatment was purchased from private actors (J. Törnroos, Public Procurement Lawyer, Association of Finnish Municipalities, interview, December 8, 2016). There is a great deal of local variation in the number of services purchased. For-profit provision of addiction treatment was until recently almost non-existent, but commercial providers had established a number of housing facilities. However, in 2018, the biggest third sector provider of addiction treatment, the A-Clinic Foundation (A-klinikka in Finnish), moved all its treatment units to the new A-Clinic Oy (a limited company). In a similar way, the important Deaconess Foundation (Diakonissalaitos) transferred its addiction facilities to a new limited Hoiva Oy company in 2016.
These moves were triggered by the planned reform of the Finnish health and welfare systems. Finland has for some ten years been preparing for a major change, which would centralise all treatment responsibility to 18 regions (from 300 municipalities), with treatment financed by state taxes (instead of municipal taxes as now). Until the end of 2017, the plan was also to transform all public provision into public corporations to enable fair competition with private, for-profit or non-profit providers on 18 treatment markets. This radical proposal has now been withdrawn, but it clearly triggered the corporatisation of third sector organisations. In addition, the rules for support from the state lottery company (Veikkaus in Finnish) put pressure on associations to turn their service production into limited corporations. Only if they clearly separate service production from other activities can they get state support for the latter (e.g., information or development activities) (M. Pulkkinen, Ministerial Adviser, Finnish Ministry of Social Affairs and Health, interview, April 12, 2017). The upcoming marketisation has also activated (multinational) for-profit providers of health and social care in general in Finland. Bigger service companies have been buying smaller ones, and international actors prepare to enter the market.
We do not know to what extent Finnish municipalities (about 300) with responsibility for the provision of addiction treatment today use public procurement, but it is common among the bigger ones (Schneider et al., 2016).
The Finnish procurement law (Laki julkisista hankinnoista ja käyttöoikeussopimuksista 1397/2016), with 174 paragraphs, states in §2, the preamble, that the goal of the law is the use of public money in a more efficient way, to guarantee fair possibilities for companies and other organisations to offer goods and services, to take into account environmental and social aspects in procurement, and to enable small and medium-sized companies and organisations to take part in procurement.
The law has a designated section of nine paragraphs regulating procurement of health and social care and other special services. The section includes specific requirements on the procurement process: it must consider the users’ special needs and their views as regulated in other laws (social and healthcare legislation). Further, the procurement unit must consider the quality of the service, continuity, accessibility, comprehensiveness, and pay attention to special needs, user involvement, and users’ opportunities to influence the service. The time frame for the contract shall also be in accordance with the needs of the service users. These principles are also found in the fairly brief and formal government handbook for procurement of social services and other special services above the threshold (Valtiovarainministeriö, 2017).
These additions were the result of a discussion in parliament and its committees and especially the activity from the umbrella organisation for non-profit organisations in the health and welfare field. They were concerned, partly because of the upcoming reform of the overall treatment system, that the quality requirements in the social and healthcare legislation would be neglected in procurement processes and that the price alone would be too decisive. The procurement law is a procedural law and does not deal with the content or result of the procurement process. A solution that could satisfy all parties was to add paragraphs that pertained to the health and social care legislation. An unsatisfied user of services can now refer to these paragraphs and complain over an unsatisfactory result of procurement within the health and social care legislation. The future will show how this solution will work (M. Ukkola, Senior Ministerial Secretary, Finnish Ministry of Economic Affairs and Employment, interview, April 11, 2017; M. Pulkkinen, Ministerial Adviser, Finnish Ministry of Social Affairs and Health, interview, April 12, 2017).
The Finnish Public Procurement Information Unit (Julkisten hankintojen neuvontayksikkö, JHNY, in Finnish, within the Association of Local and Regional Authorities) was established in cooperation with the Ministry of Economic Affairs and Employment in 2016. In December 2018 the unit posted special recommendations for procurement of health and social care (Julkisten hankintojen neuvontayksikkö, 2018). The recommendations follow closely what is laid down in the law. Procurement shall consider the needs of the users and involve the user as stated in health and social care legislation. A list of the laws that must be considered is presented. Also, the users or user representatives must be heard in the procurement process concerning the service need, the planning of services, the decision-making, and the organisation of services. The quality of the service shall be in accordance with the users’ needs and promote their participation as well as innovation. Some examples are given of how this can be done, such as that the user can be offered alternative services by the provider. The length of the contract shall be defined by the user’s needs. It is stressed that the legislation does not say anything specific about the length of the contract and that in many cases it would be possible to have a further contract.
By referring to health and social care legislation and, recently, by advising about how the users’ needs and participation can and shall be secured, the Finnish procurement regulation has emphasised the welfare aspects and given citizens more of a say in procurement. The law also mentions the protection of small providers and organisations.
Some other solutions in the Finnish procurement legislation may increase the marketisation and favour big service producers. Some specific changes were made bearing in mind the upcoming reform of the health and social care systems. According to paragraph 106, if the conditions of an ongoing contract change substantially – if, for instance, the contract moves from a municipality to a region – a new procurement process will have to start. This will favour bigger companies that are waiting to enter the market. Another specific change that was decided in parliament after a vote where the centre-right government won over the opposition, was to limit each in-house public provider from selling more than 5% to other purchasers (other municipalities/regions) than the owner. This decision was unique in the entire EU area: the directive’s limit was 20%, and only Poland has decided on a stricter line (however, setting the limit at 10%). This decision is a clear sign that Finland’s government wanted to limit the role of the public sector in service production. Also, the national threshold (400,000 euros) for public procurement according to the directives in the health and welfare sector in Finland is the lowest in the European Union; the EU directives suggest 750,000 euros.
To summarise, the Finnish solution has been a double strategy. On the one hand, there are system reforms, nationally decided thresholds, and paragraphs in the procurement law that may strengthen the position of private commercial actors. On the other hand, detailed requirements have been brought in to pay attention to user involvement and to health and social care legislation that will enable service users, too, to complain over “bad” procurement results, not in the market court but in the administrative court. There is a general declaration to protect the possibilities for users to take part in procurement in the law, but the guidelines say nothing about how this can be achieved. 2
Procurement in Sweden: Late regulation efforts in a developed market
Swedish addiction treatment has, since the 1990s (Stenius, 1999), as a complement to in-house public production, been produced in a decentralised quasi-market. The implementation of market models has been encouraged by centre-right governments, but has also more or less been accepted by social democrats in many municipalities. Public procurement of addiction treatment has become the norm for the steering of municipal addiction treatment. Today, around 60% of institutional care and 30% of outpatient care are purchased, and for-profit providers dominate among the non-municipal providers. While the third sector is losing ground in the Swedish addiction treatment system, large for-profit providers have become important players. A recent phenomenon is the establishment of service producing companies owned by investment or venture capitalists (Storbjörk & Stenius, 2018). The trend is towards big, even nationwide, procurements where a number of municipalities – up to 80 of a total of 290 – enter into joint frame agreements with a large number of providers. These procurement processes are coordinated regionally or nationally by a special unit of the Swedish Association of Local Authorities and Regions (SALAR; Sveriges kommuner och landsting, SKL, in Swedish).
The size of the procurements has also implied that the specification documents are very complicated, up to 60–70 pages, and difficult for smaller enterprises to respond to. Many municipalities may have 20 years of experience of procurement and may already have tried a number of different models (B. Johansson, Västerås City, Head of Procurement of Social Services, interview, December 8, 2016), but they are now joining centralised procurement processes to gain access to procurement competence, to become strong purchasers, and to lower the transaction costs involved in the time-consuming administrative work of procurement.
In the Swedish market for addiction treatment, a search for the best procurement model seems to be viewed as a primary road to guaranteeing good treatment systems. Procurement has for many years been viewed as a technical process that could and should be guided by good and competent politicians and procurement specialists. European statistics show that more complaints are lodged over procurement in Sweden than in any other country (Upphandlingsmyndigheten, 2017). This does not necessarily mean that procurements do not follow the law (only 20% of the complaints lead to corrections). The number of complaints is probably rather a sign of the importance of procurement in a country where “a significant share of public activities is performed by private providers”, as the government noted in a bill in 2018 (SOU 2018:44, p. 31).
When first implemented, the new Swedish Procurement law of 2016 (Lag om Offentlig Upphandling LOU 2016: 1145) followed the EU model closely. The law has 22 chapters and altogether 390 paragraphs, but no preamble. Health and social care procurement – and its exceptional light regime – is dealt with in chapter 19. Compared to the previous procurement law, it has a higher monetary threshold (equal to that in Denmark and Norway), and more room for alternative models.
Procurement is the rule in most Swedish municipalities and counties, and centralised enforcement (such as control agencies) helps to apply procurement in practice. There is nevertheless increasing critique of the privatisation of services, especially from the left. The lack of financial control, problems with treatment quality, with equal access, with discontinuity in treatment and fragmented systems, and with profit-seeking in treatment production have recently been linked to procurement rules and practices. In 2016, a government inquiry on the future of civil society in Sweden (SOU 2016:13) criticised the procurement regulations for preventing third sector organisations from participating in service provision. It proposed that social services should be left out of the procurement legislation, and suggested a Norwegian solution, with reservation of contracts for the third sector.
The minority social democratic government (installed in 2014) also considered a radical change of the 2016 Procurement law, possibly a separate procurement law for health and social care. One of the first measures of the government was to set up the independent procurement authority The National Agency for Public Procurement (Upphandlingsmyndigheten in Swedish) in 2016, to guide and support the municipalities in their purchases. In 2016, the government launched a Procurement Strategy, emphasising the importance of procurement as a strategic instrument not only for efficient use of public money but for ensuring social and environmental goals (Regeringskansliet, n.d.). On the very last page of this short document, the strategy addresses “The enabling of third sector organisations to take part in public contracts” (p. 23). These organisations are identified as an important resource for society and as increasing the diversity [of services]. The government wants to support their participation “on the welfare markets” (p. 23), for they contribute by developing the quality and by adapting to users’ needs and wishes; they are voices for groups that are seldom heard. Voluntary work strengthens “democracy, community, and social cohesion” (p. 23). The government also supports the use of innovative partnerships. Somewhat surprisingly, the strategy states that these third sector providers (idéburna organisationer in Swedish) are largely absent within treatment and care – a statement that is not true for addiction treatment, and which ignores the historical importance of these organisations.
Further, a large welfare inquiry in 2016 (SOU 2016:78) addressed the increasing role of for-profit providers in Swedish welfare production. It suggested the setting of a profit limit on enterprises from which the public sector can buy services, and further a special procurement legislation for the welfare sector. These reforms should ensure a more prominent role for the third sector. This report has not resulted in any reforms due to political resistance in parliament.
Besides arguments for and against marketisation, there is also a growing critique of the increased steering of public administrations and services. In 2018 came the final report of the “Trust delegation” (Tillitsdelegationen in Swedish; SOU 2018:47), which had been tasked with proposing reforms for the steering of the public sector in order to increase the beneficial use of staff competence over micro-management. This report also discusses problems with procurement, described as a laborious process that steals time from core assignments. It also takes issue with too detailed bids, which limit the freedom of professionals to use their expert discretion, and finds that trust in the public sector is threatened when bad providers win bids over better ones.
In 2018, the minority social democrat government presented a report with a proposal for public procurement of social and other services below threshold values (SOU 2018:44). The primary goal was to simplify the procedure and make it more flexible, while still regulating it to safeguard both the public sector’s and the providers’ need for transparency and predictability, and to prevent corruption (p. 20).
The government proposal following the report was accepted with minor amendments in June 2018 (Regeringens proposition 2017/18:158). The Swedish solution has not, in the end, been to introduce a separate legislation for procurement of social or welfare services, but to revise the existing procurement law paragraphs. One could call it a minimal revision strategy. What motivates this solution, according to the report, is that “an absolute majority of the municipalities want to do the right thing and will seek competition in order to reach a healthy and good deal” and “the absolute majority of providers to the public sector strive towards a healthy and good deal” (p. 21). Below the threshold, the requirements of transparency and fairness are limited if there is no obvious cross-border interest. Still, all procurement has to be advertised nationally (if the value is more than SEK 2 million), and information about decisions given to providers. Documentation of the procurement is necessary (if the value exceeds SEK 100,000), and legal rights to complain remain.
The report which led to the proposal (SOU 2018:44) noted that there was marked diversity in the procurement regulation of health and social services within the EU, and also within the Nordic countries. The government did, however, find some inspiration from solutions in Norway, Finland, and Denmark (p. 22). Following a Norwegian model, dialogue between purchaser and provider is introduced as a possibility for procurement of health and social services. Direct procurement is possible for services in the light regime, but competition remains a national principle. How the principle of competition is implemented in a reasonable way in each case is up to the purchaser to decide. The simplified procedures will, according to the proposal, make it possible for third sector providers to make contracts without taking part in procurement processes. Reserved contracts for social businesses are possible, but only for three years. In the proposal, it is possible in procurement to take into account the need for “quality, continuity, accessibility, acceptability and range, different social needs of specific groups of users, including less resourced and vulnerable groups, participation and empowerment of users and innovation” (SOU 2018:44, p. 338).
The report (SOU 2018:44) considered that the procurement authority must follow requirements in other legislation, such as the social legislation on the services and the individuals’ involvement in these. In contrast to the Finnish solution, these requirements are omitted from the Swedish law. It was also pointed out that the purchasing authority must be able to make long contracts if this is necessary for the user, or for costs or other reasons. In the case of personal services, the purchasing authorities should also be able to make continuous contracts; this had already been possible before the revised law. The report noted that some EU court statements show that the principle of fair treatment of providers can in some cases be regarded as less important than to secure an individualised and specific judgement of different bids. In conclusion, the report says, public authorities have much freedom in the choice of the form of procurement for health and social care services, especially personal services. However, this does not imply that they do not have a duty to make a good business-like deal (SOU 2018:44, p. 343ff).
In Sweden, public procurement is a well-established practice in social services and addiction treatment. It is only recently that it has been linked to a critique of the effects of the privatisation of services. The latest EU directives came at the same time as the right-wing government had to give way to a minority left–green coalition. Privatisation has been heavily and heatedly debated, and several inquiries during the last two years have criticised the procurement legislation and practices, particularly for being unfavourable for the third sector. However, the legislative changes have not been dramatic in the end, even if they have pointed out and minimally increased the discretion of the municipalities to use direct purchasing and even though they have created some more room for simpler procurements that will be possible for small producers. The Swedish authorities have not produced, as in Norway, any comprehensive procurement guidelines that clearly instruct public administrations to favour the third sector, nor are there guidelines which especially stress the specific requirements for the purchasing of social services. Instead, the government report (SOU 2018:44) observes that even if health and social care legislation shall guide the procurement, the public sector has a duty to use competition and behave in a good business manner. The protection of (private) providers and their rights is strongly emphasised. Notable also is the lack of attention to user involvement, both in the law and in the guidelines. The Swedish legal reforms reflect the reality of a developed (quasi-)market, with a small third sector, and with a moderately market-critical government in a minority position.
Procurement in Denmark: Not (yet?) used, consumer choice as an alternative steering tool
Denmark has a mix of public and private providers of addiction treatment. In 2014, more than half of the Danish municipalities bought drug treatment services from private providers, and about 15% from other municipalities. According to the database of the National Board of Social Services (Socialstyrelsen in Danish), around one third all alcohol problem use-related units were offered by private providers in 2017 (Amilon, Fels Birkelund, Christensen, Gade, & Markwardt, 2016).
Public procurement of addiction treatment has not been used by the municipalities so far (besides the small municipality Tårnby kommune (2018) that at the end of 2018 had an ongoing procurement process in an attempt to lower the quickly rising costs of alcohol and drug treatment). The municipalities use their freedom to produce services themselves or buy some services from other municipalities or from private producers. Treatment units within the publicly financed system are accredited and inspected by regional authorities. Free customer choice functions primarily within outpatient treatment, where the client/patient can, without referral or assessment, turn to a public or private (approved) provider for subsidised treatment. A system of free customer choice, with accreditation, does not require procurement according to EU directives.
To improve the control of social services in institutional settings for vulnerable citizens, including inpatient and outpatient services to persons with addiction problems, a new law on “Social inspection” came into force in 2014 and was further revised in 2017 and 2018 (Lov om socialtilsyn, LOV nr 608 af 12/06/2013; Socialtilsynsloven. Bekendtg ø relse af lov om socialtilsyn. 2018LBK nr 42 af 19/01/2018). The inspection is handled in five regions by municipal authorities. All units providing services must be visited at least once a year. The inspection looks at the competence of the staff, at the goals, methods, and results of the unit, the physical surroundings, the organisation and leadership – and the economy. Each unit shall have a sound economic situation that ensures a good-quality service, the price shall be related to the quality of the service, and the economy must be transparent. Overly high compensations to the leadership or unmotivated input or output of money from one unit of a corporation to another are not accepted. If the providing unit is part of a group of companies, the flow of money within the group must be declared. Such control has probably prevented private commercial companies from abusing public money, as practices such as the following are not allowed: dumping the prices to get contracts with unfair competition and moving profits from publicly funded treatment from one unit to another within the company, or out of the country to avoid taxes (A. B. Burgaard, Copenhagen City, Social service sector, interview, December 8, 2016). This may be one of the reasons why there are so far no multinational investment company-owned providers in the Danish addiction treatment system, and much fewer in general in social services than in Sweden.
The new public procurement law from 2015 (with 195 paragraphs) states in Section 1, the preamble, that the purpose of the law is to define procedures that will enable “optimum use of public funds via effective competition”. Following the EU directives, the threshold value above which public procurement is obligatory is higher for social services, healthcare, and educational services, and it allows for more flexibility in procedures. Also, as mentioned, the free system of choice makes public procurement less relevant in addiction treatment. A special section of the procurement law details the conditions for procurement of health and social services. This section makes no mention of special consideration of healthcare or social legislation. Dealing with procurement under the threshold value, §193 lays down that procurement shall adhere to market conditions by performing a market analysis and asking for one bid, or asking for two or more bids, or advertising the bid. The decision in a choice of one between several providers must be motivated as taken according to market conditions (Konkurrence- og forbrugersstyrelsen, 2016; Udbudsloven Lov nr 1564 af 15/12/2015).
The Danish Competition and Consumer Authority (Konkurrence- og forbrugerstyrelsen in Danish) published guidelines for procurement in 2016. The last section (Konkurrence- og forbrugerstyrelsen, 2016) deals with procurement of social and other specific services below the threshold value. Procurement within this light regime can take place with a selection of specific providers chosen as suitable to present a bid, but this must be declared in advance. The exclusion of providers, such as those with a criminal record, is also possible, but again should be declared from the beginning. The criteria for the final choice of provider can be freely chosen, but must be declared, and they need not include economic criteria. Within the light regime it is also possible to use negotiated procurement without advertising. This is possible in the same circumstances that enable direct procurement, that is, when the services should be tailored to an individual’s needs and action needs to be taken quickly. Institutional care of children is mentioned as an example, and it is noted that socially vulnerable persons’ support may often demand direct procurement (p. 264). In this case, the purchaser can use an online national list (Tilbudsportalen in Danish; Socialstyrelsen, 2019) of certified service providers for family care and care for the handicapped or persons with social problems. It is also possible to use reserved contracts, even above the threshold value, for activities that aim at integration of marginalised persons, for instance those with substance use problems (Konkurrence- og forbrugerstyrelsen, 2016, p. 266). This requires, however, that one third of the staff are themselves disabled or socially less resourced. No time limit for such contracts is given.
To conclude, Denmark has a market for addiction treatment provision with private and public providers. The market is steered and controlled partly by accreditation with a system of consumer choice and partly through supervision of both the quality of the treatment and the finances of the providers, to avoid abuse of public money. As noted above, the Danish social service legislation stresses more than the that of Norway, Finland or Sweden, the autonomy and self-sustainability of the individual. Within this frame, the clash between the welfare logic and the market logic may not be as obvious as in the other Nordic countries. The new procurement law from 2015 emphasises the economic aspect of procurement. However, the guidelines give several examples of flexibility within procurement that can prevent competition based solely on economic efficiency and notes the usefulness of direct or reserved contracts for services of vulnerable groups. It remains to be seen whether the recent procurement legislation will be used in Danish addiction treatment.
Discussion
Norway, Finland, Sweden, and Denmark have, to different degrees, emphasised the welfare and public health perspectives in procurement, a steering tool stemming from a market logic and the EU directives. The differences are visible in the national implementations of the most recent EU procurement directives from 2016 and in the national guidelines for public procurement.
Table 1 summarises the empirical findings to facilitate an analysis of the existing support for market and welfare logics in the four Nordic welfare states as of 2018. The first section illustrates the support for market-focused procurement in terms of: the presence of private for-profit producers with vested interests; current proliferation of procurement; whether there is a political conservative ideology that, in theory, may favour a market logic; legislated monetary thresholds for mandatory procurement; and whether procurement regulations favour commercial actors (as opposed to the third sector).
Support for market and welfare logics in procurement laws and guidelines on health and social care, focusing on addiction treatment, in four Nordic countries in 2018.
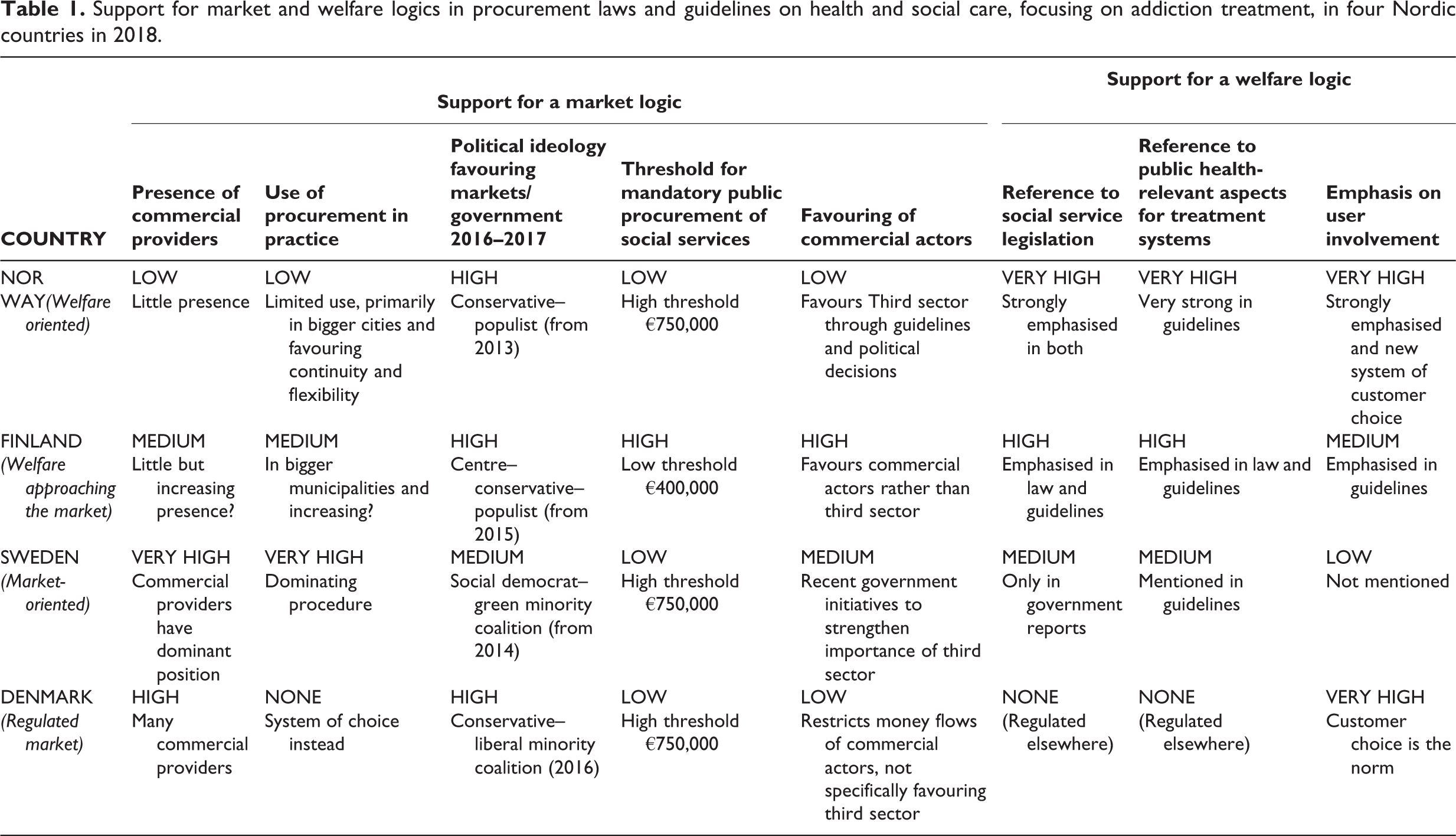
Focusing on the countries with lower support for a market logic, the first section of Table 1 shows that Norway but also Finland have a lower presence of commercial providers in addiction treatment who as collective actors support the market logic and may lobby their case (Socialtilsynsloven, 2017). Norway had only limited experience of procurement in addiction treatment; Denmark had none. Left-wing policies could be expected to limit the role of the market logic. Only Sweden had a left-wing–green government when the procurement legislations were revised. The threshold for obligatory public procurement matches the EU recommendations in all countries, except Finland, which has a lower threshold and thus gives more room for market-focused steering. Norway has in many ways sought to favour the third sector, as opposed to commercial actors, while Sweden has just recently mentioned the protection of the third sector. Danish controls have, in practice, limited the interest of commercial actors in entering this field.
The latter part of Table 1 displays the extent to which welfare and public health aspects are taken into account in procurement regulations. Both Norway and Finland refer directly to the need for procurement to respect social and healthcare legislation; they also specify public health aspects of treatment systems that should be guiding the procurement process, and emphasise user involvement. Norway implemented a system of choice in 2015, and by the end of 2018 it was noted that addiction treatment together with mental health services made up the largest part of the system of choice payments (Bjøru et al., 2019; Helsedirektoratet, 2019, 2 July 2019). The role of individual citizens is highly emphasised in Denmark in its reliance on customer choice in addiction treatment. 3
Norway appears very “welfare-oriented” and is the country where the protection of the welfare or the public health aspect is the strongest and where the resistance towards market influence has the firmest support both politically, in terms of current actors within the systems, and in the regulations. Finland is in Table 1 labelled “welfare approaching the market” and presents a dual face, with some indicators (low threshold for procurement, increasing presence of commercial providers) favouring a market logic, but, like Norway, demonstrates a strong defence of the welfare/public health aspects in the procurement regulations. “Market-oriented” Sweden demonstrates a strong market logic, with powerful commercial actors and the longest history of using procurement, which only recently has been questioned by primarily left-wing policy-makers and involved stakeholders. So far the opposition to the development has left rather weak traces in regulations, securing welfare and public health aspects. Sweden is in a way stuck with its market. Denmark with a “regulated market” combines a liberal market tradition with the idea of empowered and resourced citizens, and a centralised regulation of the market that gives some protection for the weakest from being used by strong private interests. There is, however, no direct referral to public health aspects of treatment systems in the procurement regulations. It remains to be seen whether this Danish protection will be strong enough if procurement becomes an established practice.
By and large, the most recent regulation revisions in these countries follow earlier Nordic developments and features in terms of procurement and marketisation trends (Schneider et al., 2016). This may be explained both by path dependency and by forces set in motion that may become difficult to control. Thus, Sweden saw an early marketisation that has by now created a very strong group of commercial actors highly involved in the debate. As noted by Spolander, Engelbrecht, and Sansfacon (2016), to opt for customer choice and a devolution of the responsibility for welfare to the individuals are among the few countermeasures that are not subject to international free trade treaty agreement. Within a liberal political frame, choice can be seen as providing some defence for welfare values from the influences of marketisation and strong transnational corporations. Denmark may be a case of this overarching strategy. Norway’s healthcare is also headed towards user choice (Bjøru et al., 2019; Helsedirektoratet, 2019, July 2, 2019), but it is a devolution within a welfare state frame which clearly aims at simultaneously limiting the influence of private economic interests and protecting public responsibility and civil society involvement, with both welfare and economic arguments. Sweden and Finland seem to insist on solutions that push social and health regulations into the frame of public procurement. They seek to resolve welfare and procurement arguments in an environment where opposition to private economic interests in welfare services is not strongly articulated.
While the overarching fields of public health, such as research into health inequalities and alcohol policy – tobacco policy in particular – have started to discuss corporate interests and strategies and the “commercial determinants of health” (Buse, Tanaka, & Hawkes, 2017; Casswell, 2013; Kickbusch, Allen, & Franz, 2016), it is clear that such perspectives are basically lacking in the study of health and social care research, including that of addiction treatment systems (Klingemann & Storbjörk, 2016; Storbjörk & Stenius, 2019). The tension between private accumulation and public well-being may not be new, but Freudenberg (2014) argues that it has by now “come to shape our economy and politics in ways that profoundly threaten democracy, human well-being, and the environment that supports life” (p. viii).
There is now some empirical indication that treatment systems, if they offer accessible treatment of good quality, may contribute to a decline in addiction problems on a population level, and thus contribute to public health (e.g., Smart & Mann, 2000). Notably, Esping-Andersen and Myles (2011) point out that an important characteristic of the Nordic welfare states is the importance of service provision and not only cash benefits and redistribution. Consumption of publicly funded (health, social, and educational) services is usually not measured and is therefore left out of comparative welfare state research. It is, however, believed that such services are “the single most redistributive” feature in the Nordic countries (Esping-Andersen & Myles, 2011, p. 19). A focus on services would thus be more than warranted in Nordic welfare research.
Even if there is support for positive effects on population health and inequalities of the Scandinavian or the social democratic welfare regimes in which the Nordic countries usually are located, this research is struggling with insufficient data, methodological problems, and inconsistent findings (Bergqvist et al., 2013; Pförtner, Pfaff, & Elgar, 2019). Could one explanation for the questionable superiority of the Nordic welfare model(s) in reducing health inequalities lie in the organisation and steering of the service systems? We know now that welfare and public health aspects of social and health services may differ significantly across the Nordic countries and that they can be downplayed by a market logic. Still, welfare state research has not focused on marketisation of services, and thus the effects of this remain unknown. Even if some addiction-specific studies show that different market or NPM features may influence treatment processes for better or worse, the overall lack of evidence for outcome effects remains (Hull & Ritter, 2014; Humphreys & McLellan, 2011; Jones, Pierce, Sutton, Mason, & Millar, 2018; Mason et al., 2015; McLellan, Kemp, Brooks, & Carise, 2008; Nesvåg & Lie, 2010; Pedersen, Hesse, & Bloomfield, 2011).
We may, however, fall back upon the conceptual model of population impact of treatment systems (Babor, 2015; Babor & Poznyak, 2010; Babor et al., 2008) for some theoretical suggestions for system outcomes following marketisation. The model states that policies, both addiction treatment-specific and policies in other areas, influence both the systems’ structural resources (e.g., staff, facilities, programmes, and linking mechanisms) and system qualities such as accessibility and equity, coordination, and economy that are important for the overall functioning of the system. The resources and qualities will, in turn, be moderated by factors such as service user characteristics and determine the overall effectiveness of the system for individual service users and its impact on public health in terms of population rates of addiction problems.
Procurement is an important regulation and policy determinant, introducing the market as a (system linking) mechanism affecting both structural resources and system qualities. The overview of procurement of addiction treatment by Schneider et al. (2016) notes that public procurement is best fitted for purchasing clearly delineated and easily described services, where the costs are easy to calculate, and the quality and effects of the services are quickly recognisable and simple to measure (see also Furusten, 2015). Public procurement can also make decision-makers more interested in and knowledgeable about the services that are produced by different providers. Public procurement is motivated by beliefs that, compared to a situation with a public monopoly, competition between providers will increase cost-efficient production and innovation.
Public procurement is, however, more complicated when it comes to services like addiction treatment, which are designed for often complex and long-term problems and individual needs that require multi-professional and multiagency interventions. Coordination, cooperation, and continuity become central quality aspects. Further, purchasing happens in a market where competition is a guiding principle. Competition can disturb cooperation and lead to a fragmented system instead of the integration and continuity that would be ideal for many addiction treatment clients (Storbjörk & Stenius, 2019). There is also a risk in the procurement process that economic targets will become the primary goal instead of the goal to meet the treatment needs of the population and of single individuals, as the treatment legislations require. As recently pointed out by Bjøru et al. (2019), there are basically no marketisation and welfare outcome studies which simultaneously look at both service qualities and prices. It appears clear, though, that competition enhances segregation and disfavours those with the least resources. This lowers equality within the system and threatens the universalistic principles of the welfare system.
Conclusions
This study indicates that the protection of welfare and public health aspects in procurement is not solely dependent on party political support (see Table 1). In the Nordic treatment systems, and probably also in other systems, existing service providers and established steering practices have a crucial role. In a situation, as in Swedish addiction treatment, where market steering has become an established practice (see Svallfors & Tyllström, 2017), and private, commercial providers are strongly present, it can be difficult to introduce strict requirements for the protection of welfare and population health in the procurement of social services, such as addiction treatment. We call for more research on population welfare and health effects of marketised treatment systems.
Footnotes
Acknowledgements
The authors thank the two anonymous reviewers for important and constructive comments that helped us improve the text.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors have declared the following financial support for the research, authorship, and/or publication of this article: The article is part of the research project “Benefits, tensions, and inconsistencies in the health and welfare system: The case of New Public Management in Swedish substance abuse treatment” funded by the Swedish Foundation for Humanities and Social Sciences (No. P14-0985:1).