
Abstract
Aims:
While it is documented that substance use harms others than the user, less is known about which substances people experience most harm from, and who the victims and perpetrators are. The aims were: (i) to estimate the prevalence of and overlap in self-reported harm from others’ alcohol, cigarette, and illegal drug use; (ii) to examine potential differences in the prevalence of harm from close relations’ and strangers’ use; and (iii) to examine how the prevalence of harm varies according to demographics and the respondents’ substance use.
Methods:
Population surveys conducted among 16–64-year-old Norwegians in 2012 and 2016 (N = 3407) assessed self-reported harm from others’ alcohol, cigarette and illegal drug use with identical measures, demographic variables and the respondents’ substance use.
Results:
Experience of harm from others’ alcohol use was most common, followed by others’ smoking. For all three substances, a higher proportion experienced harm from close relations’ use. Nearly half had experienced harm from others’ use of at least one substance. Women and younger participants were more likely to report harm from others’ alcohol and cigarette use. While alcohol and illegal drug users were more often harmed by others’ use of these substances, smokers reported being less often harmed by others’ smoking.
Conclusions:
Self-reported harm from others’ alcohol, cigarette and illegal drug use corresponds with the prevalence of use of these substances in Norway. For all three substances, close relations’ use accounted for more harm than strangers’ use. Own substance use was an important correlate of experienced harm.
Substance use has negative health consequences and causes social problems (Babor et al., 2010; Nutt, King, Saulsbury, & Blakemore, 2007). While cigarette smoking and alcohol use constitute the most significant problems in terms of the global burden of disease (Forouzanfar et al., 2016), it has been estimated that alcohol and illegal drugs account for a more substantial fraction of the social problems (Nutt, King, & Phillips, 2010; Nutt et al., 2007; Van Amsterdam, Opperhuizen, & Koeter, 2010).
Substance use may also harm others than the user. Harm from others’ substance use refers to a broad range of negative consequences, from being bothered by others’ use to being physically hurt by others’ substance use. To what extent are people negatively affected by others’ use of alcohol, cigarettes, and illegal drugs? Few studies have addressed the relative contribution of harm from others’ alcohol-, cigarette- and illegal-drug use (see Nutt et al., 2010; Van Amsterdam et al., 2010). Moreover, these studies are based on experts’ evaluations of harm (i.e., Nutt et al., 2010; Van Amsterdam et al., 2010). With the exception of a Swedish report (Ramstedt, Sundin, Landberg, & Raninen, 2014), no previous studies have compared the prevalence of self-reported harm from others’ use of alcohol, cigarettes, and illegal drugs in a Nordic context. Hence, knowledge is limited about which of the three substances people in the general population report experiencing most harm from, and how this compares with experts’ evaluations of harm from others’ substance use. The quantification of experience of harm from others’ substance use is important in order to produce a complete picture of the harms related to substance use. The results may also have policy implications regarding which efforts to prioritise in prevention work.
Moreover, little is known about who the victims of such harm are, and whether close relations’ or strangers’ substance use most often contribute to harm. The current study addresses these questions by presenting data on the prevalence of self-reported harm from close relations’ and strangers’ use of alcohol, cigarettes and illegal drugs in Norway.
Previous research on harm from others’ substance use in the Nordic countries
In recent years, alcohol’s harm to others has received renewed interest in Norway and the other Nordic countries, both among politicians and researchers. For example, alcohol’s harm to others was highlighted as a prioritised area in the last White Paper on alcohol and drug policy in Norway (St. Meld. Nr 30, 2011–2012), and in a thematic issue published by the Nordic Welfare Centre the same year (Nordens velferdssenter, 2012). The renewed interest has resulted in a number of studies on alcohol’s harm to others in Norway (e.g., Lund, Moan, & Storvoll, 2016; Moan, Storvoll, & Lund, 2017; Scheffels, Moan, & Storvoll, 2016; Storvoll, Moan, & Lund, 2016) and in the Nordic countries (e.g., Huhtanen & Tigerstedt, 2012; Moan et al., 2015; Ramstedt et al., 2015; Seid, Grittner, Greenfield, & Bloomfield, 2015). The harm cigarette smoking cause others than the smoker was an important argument for introducing smoke-free hospitality venues in Norway in 2004 (Lund, 2006), and there was some research on second-hand smoking prior to the introduction of the new law in Norway and the Nordic countries (Lund, Helgason, & Andersen, 2004; Lund, Skrondal, Vertio, & Helgason, 1998a, 1998b). However, little research has been conducted to address this topic in recent years. While harm from others’ illegal drug use has been widely studied in some subgroups of the population, e.g., the consequences of substance use during pregnancy and parental substance use (e.g., Imer, Teasdale, Nielsen, Vedal, & Olofsoson, 2012; Nygaard, Slinning, Moe, & Walhovd, 2016; Raitasalo, Holmlia, Autti-Rämö, Notkola, & Rapanainen, 2015; Reitan, 2018), the research addressing self-reported harm from others’ illegal drug use on a population level in the Nordic countries is scarce (but see Melberg et al., 2011).
Survey research on harm from others’ substance use consists of two research traditions. The first focuses on concrete incidents of harm from others’ alcohol use (Casswell, You, & Huckle, 2011; Laslett et al., 2011; Lund et al., 2016; Mäkelä et al., 1999; Moan et al., 2015; Rossow & Hauge, 2004; Storvoll et al., 2016), cigarette smoking (e.g., Sivri, Lazuras, Rodafinos, & Eiser, 2013) and illegal drug use (Melberg et al., 2011). Examples of harms assessed within the first tradition are whether the respondents have been physically harmed by, whether they had been afraid of, or verbally abused by people who had been drinking. Typically, in these studies, the prevalence of such harms in the general population and subgroups of the population are estimated. This study belongs to the second tradition, which applies global measures of self-reported harm from others’ substance use to determine the prevalence of harm in the population. Global measures of harm from others’ substance use assess whether and to what extent respondents have been negatively affected by the substance use of people known to the respondent and strangers, without specifying how they were affected. A few studies within this tradition have investigated the prevalence of self-reported harm from others’ alcohol use (Laslett et al., 2011; Ramstedt et al., 2015), and one study has estimated the prevalence of harm from others’ illegal drug use (Melberg et al., 2011).
Prevalence of and overlap in harm from others’ substance use
The prevalence of self-reported harm from others’ substance use is likely to correspond with the prevalence of substance use in the population. A recent Norwegian population survey showed that during the past 12 months, 83% of respondents aged between 16 and 79 years had consumed alcohol (Bye, 2018), both daily and occasional smoking was reported by 10% (Vedøy, 2018), and 6.5% had used illegal drugs (Sandøy, 2018). Since alcohol is the most commonly used substance in Norway, one can expect that more people experience harm from others’ alcohol use than from others’ cigarette smoking and illegal drug use. On the other hand, the tolerance towards substances perceived as common may be higher than towards more rarely used substances (Slovic, 2000). A study showing that the tolerance for alcohol use in Norway has increased in accordance with an increase in alcohol consumption supports this reasoning (Nordlund, 2008). In contrast, the sharp decline in the prevalence of smoking in Norway (Gartner et al., 2016) and the recognition of tobacco as an important cause of several diseases, may have contributed to a lower tolerance of smoking (Cummings & Proctor, 2014).
Another question of interest is whether people experience more harm from the substance use of close relations, e.g., family and friends, or from strangers. Previous studies using global measures of harm have examined to what extent people report being harmed by close relations’ alcohol use (Laslett et al., 2011; Ramstedt et al., 2015) and illegal drug use (Melberg et al., 2011). One study estimated the prevalence of harm from strangers’ illegal drug use (Melberg et al., 2011). In a Swedish report, the prevalence of self-reported harm from close relations’ problematic use of the three substances was estimated (Ramstedt et al., 2014). However, no previous studies have examined self-reported harm from close relations’ and strangers’ alcohol, cigarette and illegal drug use applying comparable measures in the same sample.
In addition to estimating the prevalence of self-reported harm from others’ use of each of the substances separately, we wanted to examine whether there is an overlap in experience of harm from others’ substance use. Among those who experience such harm, is there a tendency to report harm from all substances, or is the experience of harm from others’ use substance specific?
Correlates of harm from others’ substance use
Who experiences most harm from others’ substance use? Women seem to experience a greater burden of harm from others’ drinking (Laslett et al., 2011; Ramstedt et al., 2015) and illegal drug use (Melberg et al., 2011). How harm from others’ substance use varies according to age is less clear. While harm from others’ alcohol use is more common among young people (e.g., Laslett et al., 2011; Ramstedt et al., 2015), no significant age difference was found for self-reported harm from others’ illegal drug use (Melberg et al., 2011). Whereas alcohol and illegal drug use can cause a range of acute effects such as aggressive behaviour and overdoses (Babor et al., 2010; Nutt et al., 2010; Nutt et al., 2007), serious harm caused by cigarette smoking, e.g., lung cancer and ischaemic heart disease, occurs several years after exposure (Lund, 1995; Öberg, Jaakkola, Woodward, Peruga, & Prüss-Ustün, 2011). Hence, compared with acute and serious harm from others’ use of alcohol and illegal drugs, one may expect serious harm from others’ cigarette smoking to be more prevalent among older individuals.
Individuals who are living with a partner may be less exposed to some forms of harm from others’ alcohol consumption. Those not living with a partner visit licensed premises more frequently (Bye, Amundsen, & Lund, 2013), and the likelihood of experiencing harm from others’ drinking is higher among those who frequently drink at licensed premises (Moan, Brunborg, & Storvoll, 2019). However, a recent study found no significant relationship between partner status and self-reported harm from others’ drinking (Ramstedt et al., 2015). The association between partner status and experience of harm from others’ smoking will, of course, depend on the partner’s smoking habits. Studies have shown that never-smokers who were exposed to second-hand smoke at home were more likely to die from cardiovascular diseases, all circulatory diseases and coronary heart disease compared with never-smokers who were not exposed to a partner’s smoking (e.g., Gallo et al., 2010). As far as we know, no previous studies have examined the relationship between partner status and harm from others’ illegal drug use.
Few studies have explored the association between parenting status and harm from others’ substance use. Parents may have a lower threshold for reporting harm than non-parents, possibly resulting in a higher prevalence of reported harm among parents. On the other hand, parents may be more protective of themselves and their children and avoid situations that may cause harm. A recent study found no support for an association between parenting status and self-reported harm from others’ drinking (Ramstedt et al., 2015). We were not able to identify any studies that have addressed the association between parental status and harm from others’ cigarette smoking and illegal drug use.
The research literature is also limited regarding the possible association between educational level and the likelihood of experiencing harm from others’ substance use. Studies including data from northern European countries found no significant association between education and self-reported harm from others’ drinking (Ramstedt et al., 2015), or others’ illegal drug use (Melberg et al., 2011). People with a low level of education are overrepresented among smokers in Norway (Lund, 2015). There are social disparities in second-hand smoke exposure and participants with the lowest level of education seem more likely to be exposed than those with the highest educational level (e.g., Gan, Mannino, & Jemal, 2015; Lund et al., 2004; Orton, Jones, Cooper, Lewis, & Coleman, 2014).
Harm from others’ substance use may also vary according to the respondents’ substance use. Persons who frequently use substances often do so with others (Bye et al., 2013). This may increase the likelihood of experiencing harm from others’ substance use. However, frequent users may have a higher tolerance for others’ substance use and a higher threshold for reporting harm. Thus, whether own use is related to more or less harm from others’ use of the same substance is not apparent.
Finally, in addition to examining whether the correlates are different for each of the three substances, we examine the characteristics of individuals who report harm from others’ use of all three substances.
To gain more knowledge about these issues, general population surveys conducted in Norway in 2012 and 2016 included identically phrased questions about the experience of harm from close relations’ and strangers’ alcohol, cigarette and illegal drug use. The questions were asked separately for each substance. This allows for analyses of the prevalence of and overlap in self-reported harm from others’ use of three substances and the prevalence in subgroups of the population, and the data enable analyses on who the perpetrators are.
Aims
The aims were: (i) to estimate the prevalence of and overlap in self-reported harm from others’ alcohol, cigarette, and illegal drug use; (ii) to examine potential differences in the prevalence of self-reported harm from close relations’ and strangers’ substance use; and (iii) to examine how harm varies according to demographic variables and the respondents’ substance use.
Methods
Procedure and respondents
The data stem from annual surveys on alcohol, tobacco and drug use conducted in Norway by Statistics Norway. Questions on harm from others’ substance use are included every fourth year, i.e., in 2012 and 2016. In both study years, 3000 individuals aged 16–79 years, and an additional sample of 700 16–30-year-olds, were drawn from The Norwegian Population Register (random one-stage selection). Computer-assisted telephone interviews were used for data collection. Before the interviews, the individuals and parents of individuals younger than 18 years received a letter giving information about the study. The average response rate was 55% (53% in 2012, 56% in 2016) and the total sample comprised 4015 respondents. The main reason for non-response was that Statistics Norway was unable to reach the individuals. Individuals aged 16–64 years were asked questions about illegal drug use. Thus, the subsample used in this article comprised 3407 respondents (N in 2012 = 1668 and 2016 = 1739), 49% were female (M = 39.7 years, SD = 13.9). The sample was somewhat underrepresented in the age group 21–40 years and in the group with low education. The sample was weighted to correct for differences between the respondents and the Norwegian population in distribution of age, gender, educational level, and geographic region (see Høstmark, 2014; Lagerstrøm, 2018, for method reports). Survey year was not statistically significantly associated with the six outcome measures, gender, or age.
Measures
Harm from close relations’ substance use was measured similarly for the three substances with the following question asked separately for each substance: “During the past 12 months, to what degree has the alcohol use/cigarette smoking/illegal drug use of a member of your family, a girlfriend/boyfriend or another person you know had negative consequences for you?” The response options were: “To a very high degree” (4), “To a high degree” (3), “To some degree” (2), “To a small degree” (1) and “Not at all” (0). The harm measures were dichotomised because few respondents reported having experienced harm “To a high degree” or “To a very high degree”, i.e., the first four categories were coded as 1 (experienced harm), and the last category was coded as 0.
Harm from strangers’ substance use was also measured similarly for the three substances with the following question asked separately for each substance: “During the past 12 months, to what degree has the alcohol use/cigarette smoking/illegal drug use of people you do not know had negative consequences for you?” The response options were the same as for the measures above and dichotomised the same way.
Demographic variables
Women were coded as 1, men as 0. Age was grouped into five categories: 16–24, 25–34, 35–44, 45–54, and 55–64 years. Partner status was measured using the question “Are you married or a cohabitant?” with the response options: 1. “Yes, married/partner”, 2. “Yes, cohabitant”, 3. “No”. The measure was dichotomised into “living with a partner” (0) and “not living with a partner” (1). Respondents with children aged 0–18 years were coded as 1, and those without children as 0. Educational level was dichotomised to “High” (0; college or university) and “Low” (1; other).
Substance use
Two measures of the respondents’ drinking habits during the past 12 months were used – drinking frequency and intoxication frequency – with response categories ranging from “None” to “Several times a week or more often”. Drinking frequency was categorised into five categories: “None” (0), “A few days a year” (1), “Monthly” (2), “Weekly” (3) and “2 days a week or more often” (4). Due to its distribution, intoxication frequency was re-coded into a four-category variable: “None” (0), “A few days a year” (1), “Monthly” (2) and “Weekly” (3). The frequency of cigarette smoking was categorised as “Never” (0), “Occasional smoking” (1) and “Daily” (2). Use of illegal drugs (separate questions for cannabis, cocaine, ecstasy, amphetamine, heroin, GHB or other substances) during the past 12 months (yes/no) was coded “No” (0), and use of one or more substance was coded “Yes” (1).
Analyses
We first examined the prevalence of self-reported harm from others’ alcohol, cigarette, and illegal drug use, and whether there were differences in the prevalence of self-reported harm from close relations’ and strangers’ substance use (Table 1). Second, we examined the possible overlap in self-reported harm from others’ substance use by computing eight mutually exclusive groups consisting of all possible combinations of those who had experienced/had not experienced harm from others’ substance use, allowing us to calculate the proportion of respondents in each group (Table 2). Third, bivariate associations between the outcome measures and demographic variables and substance use were analysed using cross-tabulations with Pearson’s χ2 test (Table 3). Binary logistic regression analyses were conducted to examine how harm varied according to each of the demographic variables and own substance use when controlling for the other variables (Table 4). The correlation between the two drinking variables was relatively strong (r = 0.40) (Cohen, 1988). Since the likelihood of experiencing harm from others’ drinking is likely to be greater among people when they binge-drink than when they drink per se, we only included intoxication frequency in the regression analyses. We conducted analyses in STATA, version 15. For descriptive purposes we used weighted data; for the regression analyses we used unweighted data.
Prevalence (%) and degree of self-reported harm from close relations’ and strangers’ substance use in the past 12 months. Weighted data.
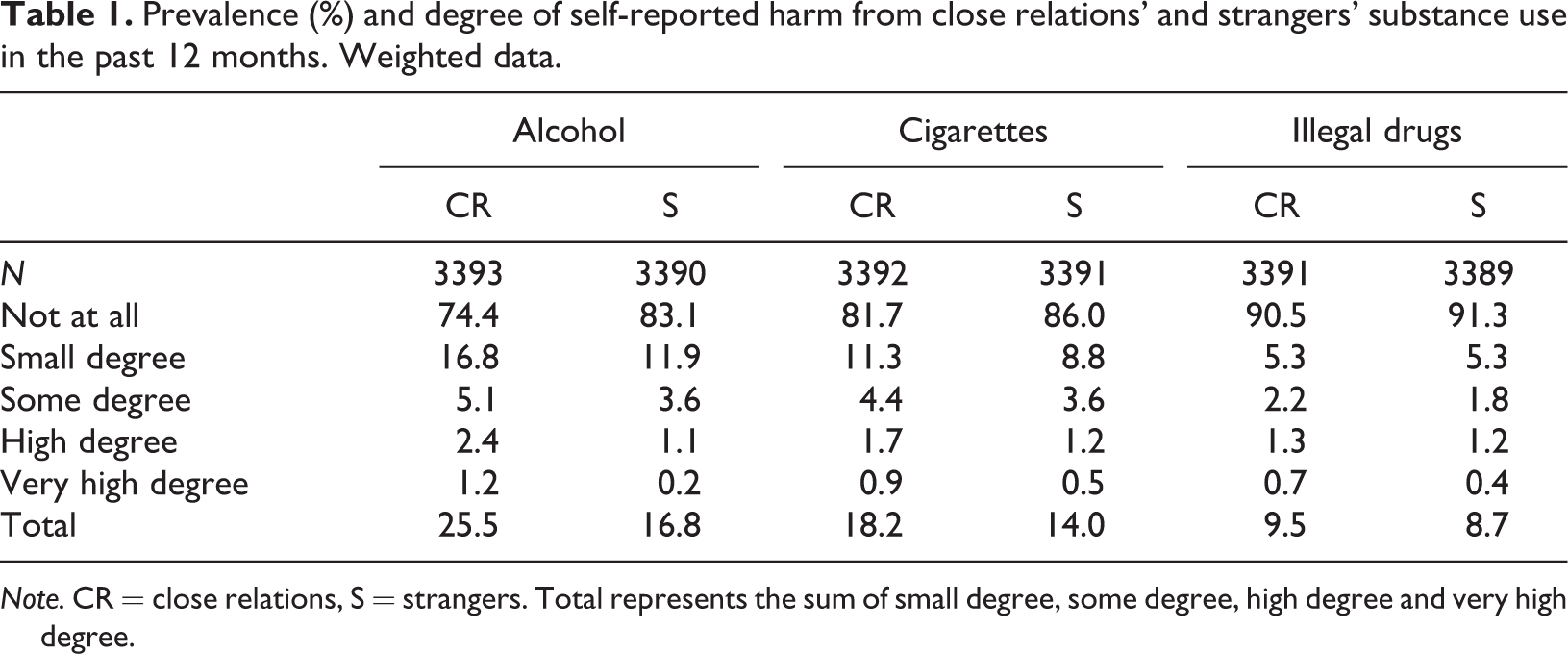
Note. CR = close relations, S = strangers. Total represents the sum of small degree, some degree, high degree and very high degree.
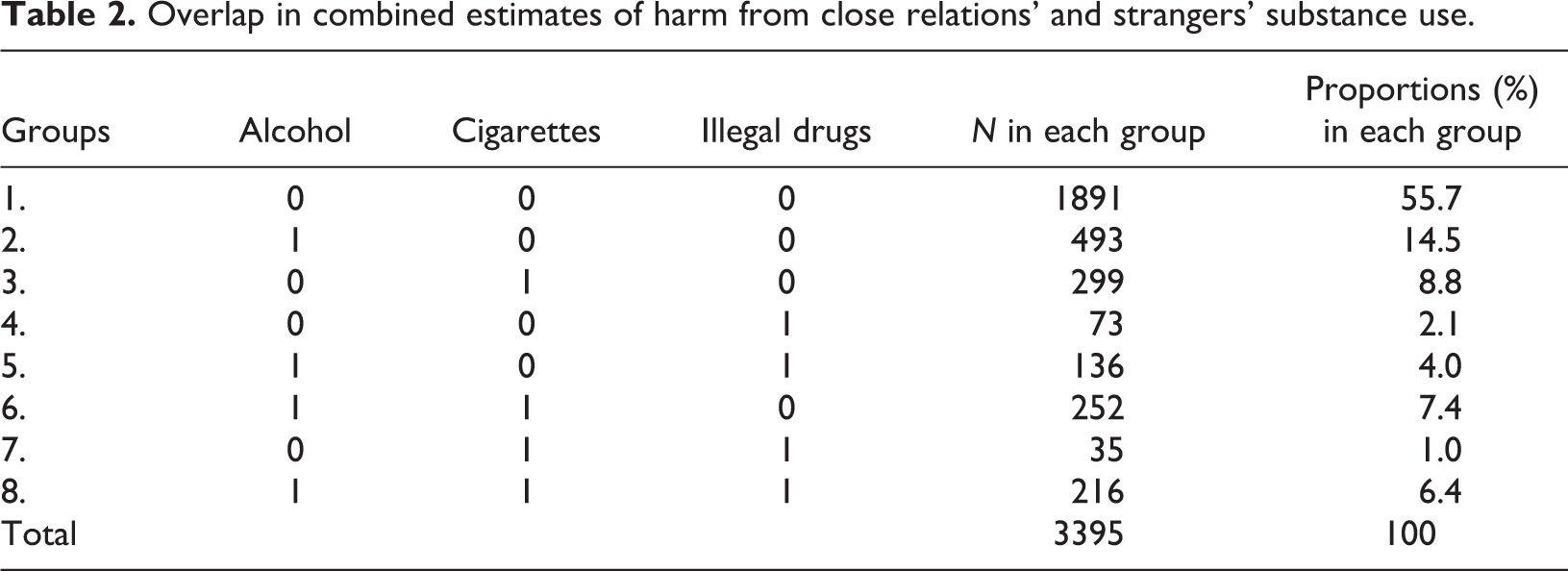
Overlap in combined estimates of harm from close relations’ and strangers’ substance use.
Self-reported harm (%) from close relations’ and strangers’ substance use in the past 12 months according to demographics and own substance use (lowest N). Weighted data.
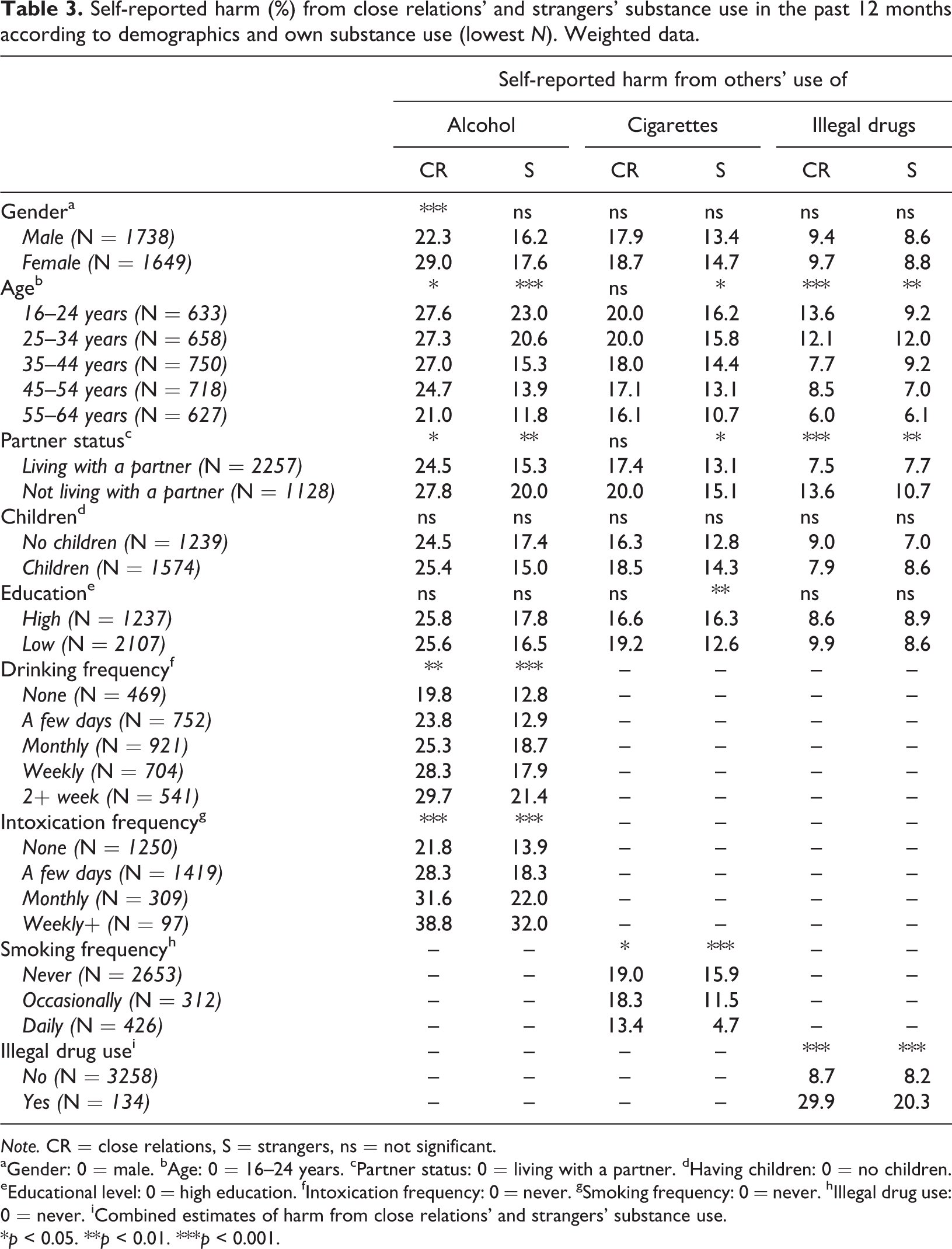
Note. CR = close relations, S = strangers, ns = not significant.
aGender: 0 = male. bAge: 0 = 16–24 years. cPartner status: 0 = living with a partner. dHaving children: 0 = no children. eEducational level: 0 = high education. fIntoxication frequency: 0 = never. gSmoking frequency: 0 = never. hIllegal drug use: 0 = never. iCombined estimates of harm from close relations’ and strangers’ substance use.
*p < 0.05. **p < 0.01. ***p < 0.001.
Correlates of self-reported harm from close relations’ and strangers’ substance use. Binary logistic regression analyses, adjusted odds ratios. Unweighted data.
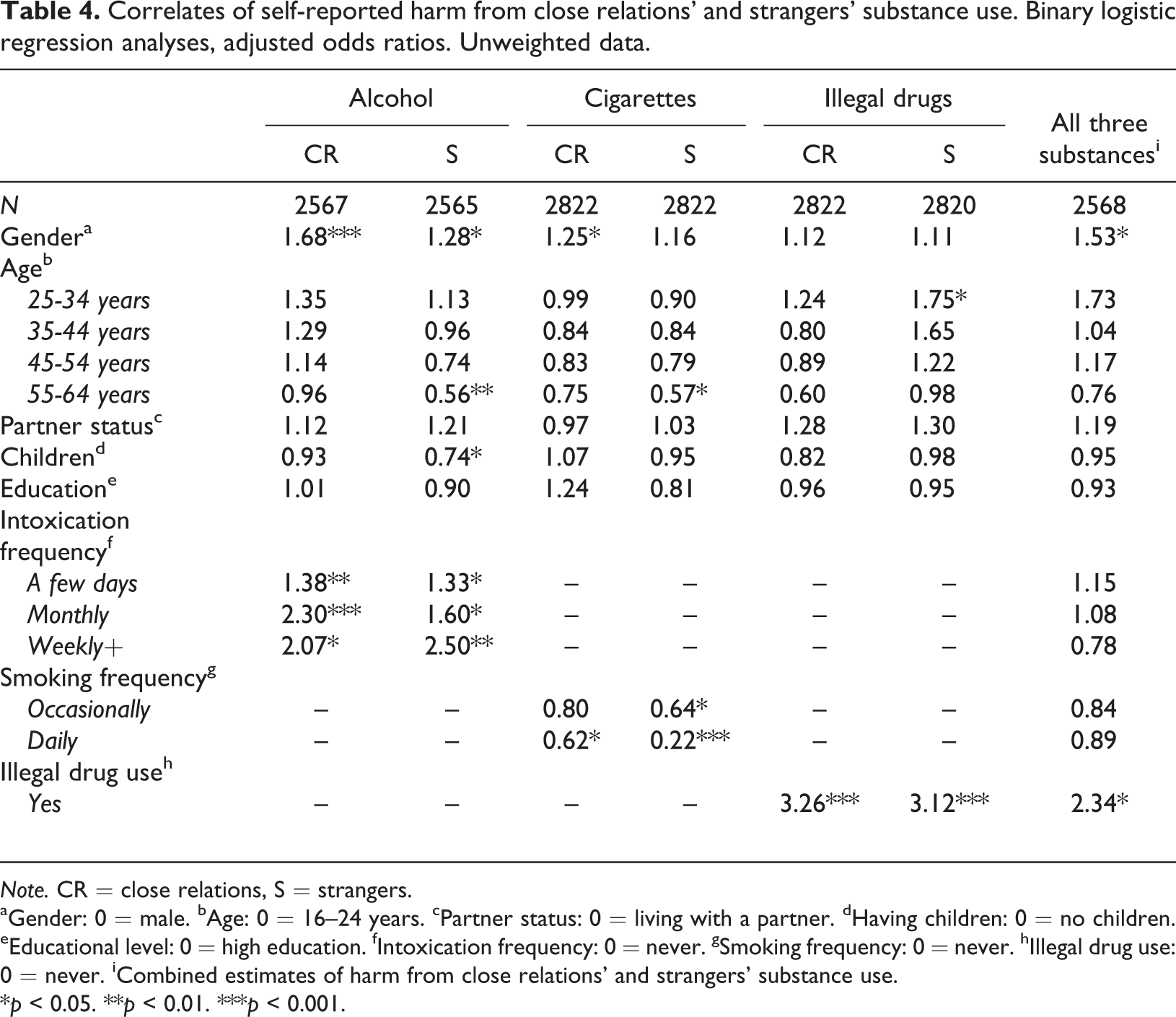
Note. CR = close relations, S = strangers.
aGender: 0 = male. bAge: 0 = 16–24 years. cPartner status: 0 = living with a partner. dHaving children: 0 = no children. eEducational level: 0 = high education. fIntoxication frequency: 0 = never. gSmoking frequency: 0 = never. hIllegal drug use: 0 = never. iCombined estimates of harm from close relations’ and strangers’ substance use.
*p < 0.05. **p < 0.01. ***p < 0.001.
Results
Prevalence of and overlap in harm from others’ substance use
Self-reported harm from others’ alcohol use was most common (32.7%), followed by harm from others’ cigarette use (24.0%). Self-reported harm from others’ illegal drug use was least common (13.6%). As shown in Table 1, harm from close relations’ substance use was more common than harm from strangers’ use for all three substances. It should be noted that most of those reporting having experienced harm from others’ substance use had experienced this to a small degree.
Table 2 shows the overlap in self-reported harm from others’ substance use. More than half (55.7%) did not report experiencing any harm from others’ substance use. Experiencing harm solely from others’ alcohol use was most common (14.5%), followed by experience of harm only from others’ cigarette smoking (8.8%), and experience of harm from both others’ alcohol and cigarette use (7.4%). Experience of harm from others’ use of all three substances was reported by 6.4%.
Correlates of harm from others’ substance use
Table 3 shows that self-reported harm from close relations’ alcohol use was significantly more common among women than men. Harm from close relations’ alcohol and illegal drug use, and harm from strangers’ use of all three substances was more common among young participants. Moreover, harm from close relations’ and strangers’ alcohol and illegal drug use, and from strangers’ cigarette use, was more common among those living alone. A larger proportion of participants with a high level of education reported being harmed by strangers’ cigarette use. Finally, harm from others’ alcohol and illegal drug use increased with frequency of own alcohol and illegal drug use, while harm from others’ cigarette smoking decreased with increased frequency of own smoking.
The logistic regression analyses (Table 4) showed that the prevalence of self-reported harm from close relations’ alcohol and cigarette use was significantly higher among women than among men when adjusting for the other demographic variables and own substance use. Women were also more likely to have experienced harm from strangers’ alcohol use. Younger respondents were more likely than older respondents to report harm from strangers’ use of all three substances. Parents were less likely to experience harm from strangers’ alcohol use compared with non-parents. The likelihood of reporting harm from others’ alcohol and illegal drug use increased significantly with an increase in own use of alcohol and illegal drugs, respectively. The opposite pattern emerged for cigarette smoking: the likelihood of reporting harm from others’ cigarette smoking decreased with an increase in own smoking frequency.
Finally, the likelihood of reporting harm from others’ use of all three substances was significantly higher among women than among men, and among individuals using illegal drugs.
Discussion
This study extends previous studies by applying identical measures to estimate the prevalence of and overlap in self-reported harm from others’ use of three substances – alcohol, cigarettes and illegal drugs. We also examined who the perpetrators were, i.e., whether the respondents reported being more harmed by close relations’ or strangers’ substance use and who the victims of such harm were, i.e., whether the prevalence of harm varied between different demographic groups. First, self-reported harm from others’ alcohol use was most common, followed by others’ cigarette smoking. Second, a higher proportion reported harm from close relations’ than from strangers’ substance use. Third, nearly half of the sample had experienced harm from others’ use of at least one substance. Experiencing harm from others’ use of alcohol alone was most common, followed by those who only had experienced harm from others’ cigarette smoking. Fourth, women and younger participants were more likely to report harm from others’ alcohol and cigarette use, and parents were less likely to report harm from strangers’ alcohol use. Fifth, the respondents’ own alcohol and illegal drug use were associated with an increased likelihood of reporting harm from others’ use of these substances. In contrast, an increase in the frequency of own smoking was associated with a decrease in the likelihood of reporting harm from others’ smoking. Finally, women and individuals who reported using illegal drugs were more likely to report harm from others’ use of all three substances.
Prevalence of and overlap in harm from others’ substance use
Self-reported harm from others’ alcohol use was most common, suggesting that the prevalence of harm corresponds with the prevalence of use of the particular substances in Norway (Bye, 2018; Sandøy, 2018; Vedøy, 2018). A few studies addressing the relative contribution of harm from others’ use of alcohol, cigarettes, and illegal drugs have relied on experts’ evaluations of harm using data from England and the Netherlands (Nutt et al., 2010; Van Amsterdam et al., 2010). In this study, we addressed this question using another methodological approach and another context, i.e., by applying self-reported survey data from the Norwegian population. The results from our study correspond with findings of studies based on experts’ evaluation of harm, suggesting that alcohol accounts for the largest proportion of harm to others than the user. Moreover, Ramstedt and colleagues (2014) estimated the prevalence of self-reported harm from close relations’ problematic substance use in Sweden, and found the same pattern as revealed in the current study. Among those who reported having close relations with a problematic substance use, it was most common to report harm from close relations who drank too much (14.6%), followed by close relations who were daily smokers (13.2%) and close relations who used illegal drugs (2.8%). The findings are also in line with a study showing that others’ alcohol use caused more psychological strain than others’ use of cigarettes and illegal drugs (Moan et al., 2017). Thus, despite the different approaches used to address the relative contribution of harm from others’ substance use, the results point in the same direction – alcohol causes more harm to others than the user than cigarettes and illegal drugs.
To our knowledge, this is the first study addressing the possible overlap in the experience of harm from others’ use of three different substances. A previous study addressing the overlap in worry about others’ use of alcohol, cigarettes, and illegal drugs found that the overlap in worry was low, i.e., 2.7% reported worry about others’ use of all three substances (Moan et al., 2017). This study showed that the overlap was somewhat higher, i.e., 6.4% reported experience of harm from others’ use of all three substances. However, reporting solely being harmed by others’ alcohol and by others’ cigarette use, respectively, was more common. Thus, the results from this study suggest that the tendency to report harm from others’ substance use is mostly substance specific.
For all three substances, a higher proportion of the respondents reported harm from close relations’ than from strangers’ use. These findings are in line with studies where close relations’ alcohol use (Karriker-Jaffe, Li, & Greenfield, 2018) and illegal drug use (Melberg et al., 2011) caused more harm than strangers’ use. This seems reasonable since significant others are more likely to have an impact on how individuals think and act than more distal relations (e.g., Ajzen, 1991; Moan et al., 2017).
Correlates of harm from others’ substance use
Women and younger participants were more likely to report harm from others’ alcohol and cigarette use. The results correspond with previous studies where women experienced a greater burden of the harm from close relations’ drinking (Laslett et al., 2011; Ramstedt et al., 2015; Stanesby et al., 2018). In this study, we also found that women, to a greater extent than men, reported being harmed by strangers’ alcohol use. Moreover, reporting harm from others’ alcohol use was more common among younger than among older individuals; a finding that corresponds with results in previous studies (Laslett et al., 2011; Ramstedt et al., 2015). Although the gender differences in smoking prevalence have diminished over the past decades, a larger proportion of men in older age groups smoke. Hence, it seems reasonable that more women than men are negatively affected by a partner’s smoking. The sharp decline in smoking prevalence in Norway during recent decades (Gartner et al., 2016) may have resulted in a lower tolerance towards smoking among young people due to less experience with smokers and smoking in general. While Melberg and colleagues (2011) did not find any age difference in experience of harm from others’ illegal drug use, this study showed that young individuals reported more harm from strangers’ illegal drug use than older individuals. A possible explanation of this finding is the increase in illegal drug use in Norway in recent years, showing that more young adults report using cannabis and somewhat more ecstasy/MDMA (Sandøy, 2018).
The results from this study correspond with the findings from a recent study showing no association between parenting status and self-reported harm from close relations’ drinking (Ramstedt et al., 2015). However, this study showed that there were significantly fewer parents than non-parents who reported experiencing harm from strangers’ alcohol use. Parents probably visit licensed premises such as bars less frequently than non-parents. Moreover, drinking in licensed premises is associated with an increased likelihood of experiencing harm from others’ drinking, more so than drinking in one’s own home, someone else’s home, or outdoors (Moan et al., 2019). Partner status and level of education were not significantly associated with reporting harm from others’ use of any of the three substances when controlling for other demographic variables and own substance use. These findings correspond with results from previous studies on harm from others’ alcohol (Ramstedt et al., 2015) and illegal drug use (Melberg et al., 2011).
The respondents’ own substance use was strongly associated with self-reported harm from others’ use, but the associations differed across substances. While the prevalence of harm from others’ alcohol and illegal drug use increased with an increase in own use, the prevalence of harm reported from others’ smoking decreased with an increase in the respondents’ smoking. The findings suggest that people who smoke are more tolerant towards others’ smoking and smoking in general, an assumption which has received empirical support in several studies (e.g., Kaleta, Polanska, Wojtysiak, & Szatko, 2017; Salgado, Mejía, Kaplan, & Pérez-Stable, 2017). Moreover, it is reasonable to assume that persons who frequently use alcohol and illegal drugs often do so with others (Bye et al., 2013). This is likely to increase the likelihood of being harmed by others’ substance use. Finally, previous studies show that there are more social consequences related to others’ alcohol and illegal drug use than to others’ use of cigarettes (Nutt et al., 2010; Van Amsterdam et al., 2010).
Experiencing harm from others’ use of all three substances was more common among women than men, reflecting the pattern found in substance-specific analyses. Thus, there is a growing body of empirical evidence suggesting that women carry a greater burden of harm from others’ substance use (Laslett et al., 2011; Ramstedt et al., 2015; Stanesby et al., 2018). However, it may also be that women have a lower tolerance for substance use and a lower threshold for reporting harm than men. A study suggested that women had more restrictive attitudes towards alcohol use than men (Scheffels et al., 2016). However, further studies are needed to draw firm conclusions regarding this issue. Finally, the results showed that the likelihood of reporting harm from others’ use of all three substances was significantly higher among respondents who reported using illegal drugs. A possible explanation of this finding is that the relatively small group of individuals who use illegal drugs (Sandøy, 2018), as opposed to the majority of the population who use alcohol (Bye, 2018), may be more likely to be involved in other risky behaviours such as frequent drinking and daily smoking.
Methodological considerations and suggestions for future research
The strength of this study is that it is based on national surveys and that it contains comparable measures of harm from others’ alcohol, cigarette, and illegal drug use as well as measures of perpetrators and victims of harm. However, some limitations warrant attention. The prevalence of self-reported harm from others’ substance use is probably underestimated because the most frequent users, who are perhaps also more likely to be harmed by others’ substance use, are less likely to participate in surveys (Johnson, 2014). Another possible source of underestimation of harm is the application of global measures of harm. People tend to remember the most salient and severe episodes (Tversky & Kahneman, 1973) and are less likely to remember the full range of harms they may have experienced. However, most of those who reported experiencing harm from others’ substance use had experienced such harm to a small degree, indicating that also less severe episodes were included.
Self-reported harm from others’ substance use might also be biased, particularly when victims report harm from strangers, because the person perceived as “the drinker causing harm” might have been under the influence of alcohol, alcohol and illegal drugs, or none of the two (see, e.g., Rossow, 2015, for discussion). This study showed that a larger proportion of the respondents reported experiencing harm from close relations’ substance use. The relatively low prevalence of reported harm from strangers’ substance use is consistent with findings in previous studies (e.g., Laslett et al., 2011), but might be both under and over-reported. To obtain more reliable measures, future survey studies should aim to provide relevant data from both perpetrator and victim.
Moreover, future studies would benefit from specifying the harms from others’ use of the three substances, preferably using a qualitative approach to identify the significant harms (e.g., physical, psychological) and then investigate the prevalence of the identified harms using surveys (for examples of studies combining survey data and qualitative data, see Manton, MacLean, Laslett, & Room, 2014; Scheffels et al., 2016).
Further, to examine the possible impact of self-reported harm from others’ substance use on health, survey data could be combined with registry data on health-related outcomes such as depression, anxiety and sickness absence, as well as substance-use problems (Lund et al., 2015; Rossow, 2015; Rossow & Ramstedt, 2016). Providing good estimates of the impact of harm from others’ substance use is important in order to obtain a complete picture of the harm caused by substance use in society. For example, in the global burden of disease estimates (Forouzanfar et al., 2016), only a few measures of harm from others’ substance use are included, i.e., passive smoking, prenatal alcohol exposure, drunk driving, and alcohol-related violence. Hence, the harm caused by substance use is therefore most likely underestimated.
Another question of interest for future research would be to examine whether there are systematic differences between individuals according to the severity of self-reported harm from others’ alcohol use, cigarette smoking and illegal drug use. To obtain a better understanding of the differences in experience of harm from close relations’ and strangers substance use, future studies should also examine the severity of harm as well as the prevalence of harm from these groups, and the specific harms most commonly experienced from close relations’ and strangers’ use. Moreover, in this study, harm from close relations’ substance use refers to “…a member of your family, a girlfriend/boyfriend or another person you know”. While family members and partners usually represent close relations, it is more uncertain whether “another person you know” represents a close relation. Thus, to provide more detailed information about close relations as perpetrators, future studies should apply questions enabling analysis of the relative contribution of harm from specific groups of close relations.
Finally, to obtain a better understanding of the group differences in self-reported harm from others’ substance use, future studies should consider including other possible correlates of harm, e.g., the tolerance of others’ alcohol, cigarette, and illegal drug use.
Conclusions and implications
This study extends previous research on harm from others’ substance use by estimating the prevalence of and overlap in self-reported harm from others’ use of three substances: alcohol, cigarettes and illegal drugs. The results correspond with results from experts’ evaluations of harm from substance use in that people in the general population report experiencing most harm from others’ alcohol use. Nearly half of the respondents reported experiencing harm from others’ use of at least one substance, and solely experiencing harm from others’ alcohol use was most common. Thus, the potential to prevent harm from others’ substance use may be greater if interventions focus on alcohol use. For all three substances, harm from close relations’ use was more common than harm from strangers’ use. This may suggest a need for a particular focus on close relations’ substance use. The finding that young individuals and women more often reported being harmed by others’ alcohol and cigarette use should also be taken into account in future studies and when developing interventions to prevent harm from others’ substance use.
Footnotes
Availability of data
The data used for the current study are available from the corresponding author on reasonable request.
Acknowledgements
This study was funded by the Norwegian Institute of Public Health. The authors wish to thank two anonymous referees for their high-quality and constructive comments.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.