
Abstract
Aims:
Short height and low educational level are associated with increased risk of myocardial infarction. We aimed to investigate the relationship between height and myocardial infarction in women and men with subsequent analyses by educational levels in a Norwegian population.
Methods:
Data from 30,167 participants (born 1930–1977), who attended The Tromsø Study between 1979 and 2016 with follow-up until 31 December 2021, were used in this study. We used Cox proportional hazards regression models to estimate hazard ratios and 95% confidence intervals for the associations between height and incident myocardial infarction. Additionally, we estimated hazard ratios with restricted cubic splines and conducted analyses stratified by educational level.
Results:
Height as continuous and categorical variables was inversely associated with risk of myocardial infarction in both sexes. One standard deviation taller height was associated with 18% lower risk of myocardial infarction in women, and 13% lower risk in men (p=0.02). Similarly, the taller height categories had lower myocardial infarction risk compared with the shorter height categories. Adjustments for traditional cardiovascular risk factors as possible mediators slightly attenuated these associations. We found no difference in associations between height and myocardial infarction across educational levels.
Conclusions:
Background
Cardiovascular disease (CVD) is a common cause of morbidity and mortality worldwide [1], with several biological and lifestyle factors associated with increased risk of CVD [2,3]. Height is the combined result of genetic and early-year living conditions [4]. Poor early-year living conditions are associated with shorter height and increased risk of CVD in adulthood [5,6]. Higher risk of coronary heart disease (CHD) in short men was first reported in 1951 by Gertler et al., where participants diagnosed with CHD were 4.8 cm shorter than study controls [7]. The inverse relationship between height and myocardial infarction (MI) in women was first reported in 1990 [8]. Similar associations with CVD are reported in multiple subsequent studies [9 –16].
Height at population level increased gradually throughout the 20th century as a result of improved living conditions [17]. Height differences between educational groups have been found in several European countries, with lower mean height in women and men with low education levels compared with women and men with high education levels [18]. Low education level has also been associated with increased risk of CVD morbidity and mortality [2,19].
The inverse relationship between height and CVD in a Norwegian population was first presented in 1984 by Waaler [20]. Igland et al. reported in 2014 that MI was more prevalent among low education participants compared with high education participants in Norway [21]. Inverse associations between height and CVD risk factors by educational level in Norway have been shown previously [22]. However, solid investigations on associations between height and MI according to sex and educational level in a Norwegian population are lacking. Thus, the aim of this study was to investigate sex-specific associations between height and incident MI, and to assess whether possible associations were modified by educational level.
Methods
Study design and data material
We used data from The Tromsø Study, which consists of seven health surveys conducted in Tromsø, Norway between 1974 and 2016. Our baseline cohort consisted of data from the second survey (Tromsø2, 1979–1980) up to the seventh survey (Tromsø7, 2015–2016), while data from Tromsø1 (1974) was not included since participation in this survey was limited to men only. Baseline data consisted of measurements of height, systolic blood pressure (SBP), diastolic blood pressure (DBP), serum total cholesterol (TCH), serum triglycerides and questionnaires for self-reported educational level and smoking status. Data on participant age and sex was obtained from the national 11-digit personal identification number maintained by the Norwegian National Population Registry. More in-depth descriptions of the data collection and cohort profile of The Tromsø Study have previously been published elsewhere [23,24].
To identify incident fatal and non-fatal MI, we linked baseline data from Tromsø2–7 to the local cardiovascular disease registry of The Tromsø Study and the national Norwegian Myocardial Infarction Registry and The Norwegian Causes of Death Registry using the Norwegian unique 11-digit personal identification numbers. The local and national registries provided follow-up data on incident fatal and non-fatal MI up to 31 December 2021. A more detailed description on the local and national registries has been published previously [25].
Participants
Inclusion and exclusion of participants are presented in Figure 1. Consistent with our previous studies using data from Tromsø2–7, a total of 59,722 women and men were invited to participate. There were 44,154 people who participated in a least one survey between 1979 and 2016. We opted to include participants from the first survey; they were aged 30–49 years. This was done to reduce the impact of height loss with increased age [26].
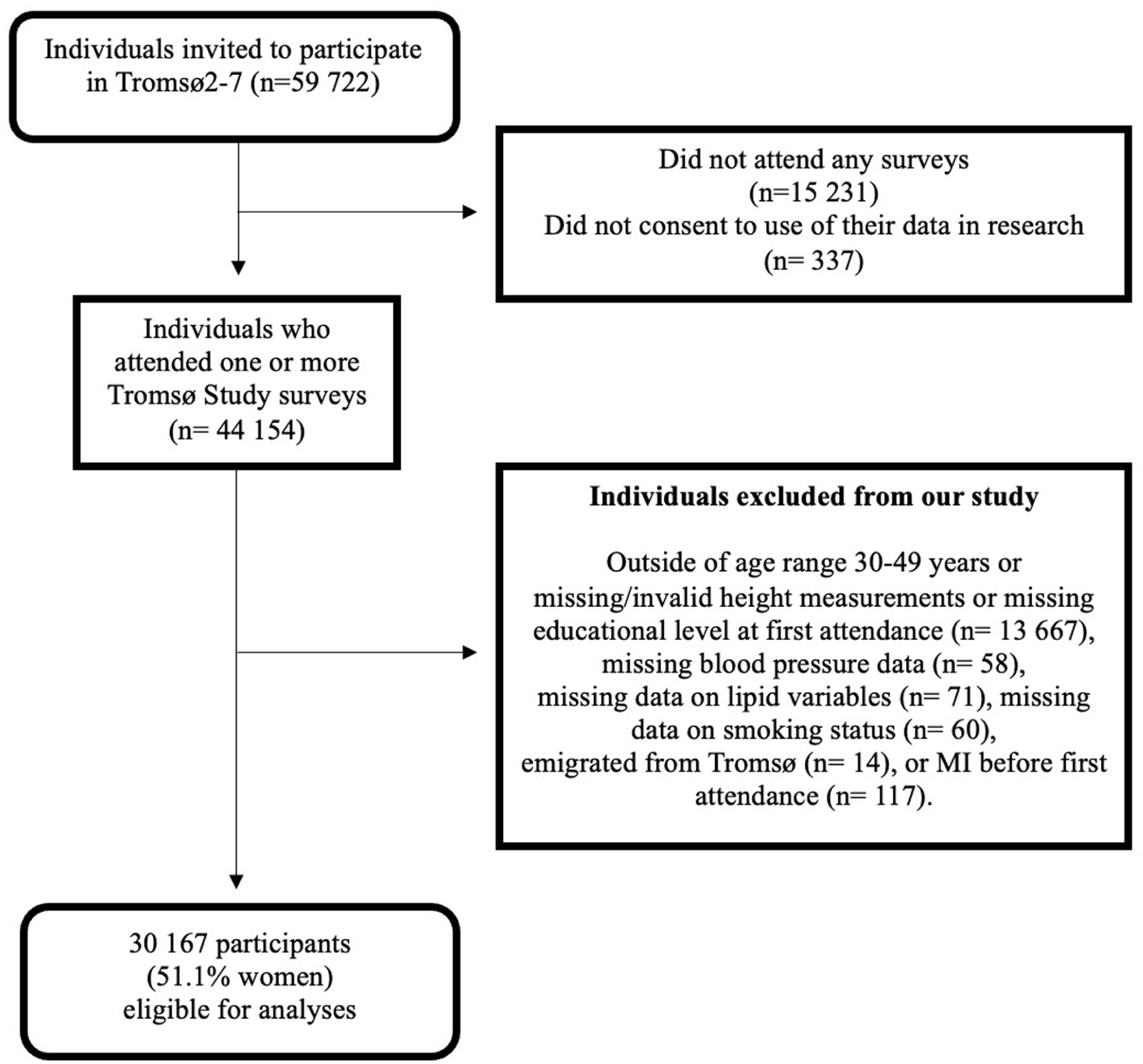
Flow chart of study participants.
We excluded those who were outside of the age range of 30–49 years or had invalid measurements of height (missing measurement, height measured wearing shoes or headwear (n= 13,667). Participants with missing data on blood pressure (n= 58), lipid variables (n= 71), smoking status (n= 60), who had emigrated from Tromsø before date of attendance (n= 14), or had prevalent MI (n= 117) were also excluded. Thus, our final study sample consisted of 30,167 participants (51.1% women).
Measurements
The main exposure variable in our study was height, measured with the participants standing upright wearing light clothing and no footwear. In Tromsø2–4, height was measured to the closest 1 cm using a measuring band. In later surveys (Tromsø5–7), height was measured to the closest 0.1 cm using an automatic electronic scale (Jenix DS 102 stadiometer, Dong Sahn Jenix, Seoul, South Korea).
The outcome variable of incident fatal and non-fatal MI was collected from several sources, previously described in detail by Varmdal et al. [25]. The MI events dated up to 2015 were sourced from the local cardiovascular disease registry of The Tromsø Study, while events from 2015 to 2021 were obtained from national registries of MI and causes of death [25].
MI in the local registry was identified through linkage to the diagnostic records of the University Hospital of North Norway and the National Causes of Death Registry. Event cases were ascertained by reviewing medical records with ICD-10 discharge diagnoses of I20–I25, I46–I48, I50, I60–I69, G45, G46, G81, R96, R98, or R99. Hospitalised and out-of-hospital events were adjudicated by experienced physicians using the Modified World Health Organization Monitoring Trends and Determinants of Cardiovascular Disease (MONICA)/MONICA Risk, Genetics, Archiving and Monograph [25].
All Norwegian hospitals are required to register diagnosed MI patients in The Norwegian Myocardial Infarction Registry [25]. Inclusion criteria for MI were patients with ICD-10 codes I21 and I22 that were admitted to hospital within 28 days after onset of symptoms. Deaths with ICD-10 codes I21–I24, I25.2, I46, or R96 combined with I20 or I25 as the underlying or contributing cause of death were defined as MI events. Data of out-of- hospital fatal incident cases of MI were provided by The Norwegian Cause of Death Registry. A 2021 validation study reports that MI diagnoses from the local and national registries in 2013–2014 were consistent and valid [25].
In all six Tromsø study surveys, SBP and DBP were measured two or three times in a seated position. Blood pressure (BP) in Tromsø2 was measured manually using a mercury sphygmomanometer, while the Dinamap Vital Signs Monitor (Critikon Inc., Tampa, Florida, USA) was used in Tromsø3–5, and the Dinamap ProCare 300 (GE Medical Systems Information Technologies, Tampa, Florida, USA) was used in Tromsø6–7. We used the second BP measurement from Tromsø2 and calculated mean SBP and DBP based on the second and third BP measurements in Tromsø3–7.
Lipid data (TCH and triglycerides) were obtained from non-fasting blood samples analysed at the Department of Laboratory Medicine, University Hospital of North Norway.
Educational attainment was obtained from questionnaires across The Tromsø Study. In Tromsø2, 3 and 5, participants reported their education as number of years, while Tromsø4, 6 and 7 used questions with fixed answer categories ranging from primary to long tertiary education [22].
We aligned our education categories with the categories used in Tromsø7 by recoding data from the earlier surveys into four standardised levels: primary education (up to nine years of education), upper secondary education (10–12 years of education), short tertiary education (13–15 years) and long tertiary education (more than 16 years of education). The answering options of vocational school and upper secondary school from Tromsø4 and Tromsø6 were merged into the upper secondary education category.
The questions related to smoking status varied between surveys. In Tromsø2–3, participants reported their current smoking status using three options (cigarette smoker, smoker but not cigarettes, or never smoker). In Tromsø4, participants were asked whether they smoke cigarettes daily, with two answer options (yes or no). Participants in Tromsø5–7 were asked whether they smoked daily, with three answer options (yes now, yes previously, never). To harmonize these questions, we constructed a new variable for smoking status (non-smoker or smoker). The following participants were categorized as non-smokers, never smokers from Tromsø2–3, no daily cigarettes in Tromsø4 and the yes previously and never smokers from Tromsø5–7.
Statistical analyses
All statistical analyses were sex-specific unless otherwise specified and were performed using version 18.5 of STATA (StataCorp., College Station, Texas, USA). Descriptive characteristics are presented using means and standard deviations (SDs) for continuous variables and number and percentage for categorical variables. Statistical significance level was set to 0.05.
Follow-up time ranged from the day of study entry to the date of first fatal or non-fatal MI, participant censoring owing to emigration from Norway or emigration from the municipality of Tromsø, death, or the end of follow-up (31 December 2021), whichever came first.
Cox proportional hazards regression models were used to estimate hazard ratios for the associations between height and incident fatal or non-fatal MI. Height was standardised to sex-specific z-scores and sex differences was assessed by adding a two-way cross product term between height and sex to a separate model with height and sex as main effects.
In separate models, height was split into sex-specific height categories. Our height categories were based on a combination of height categories used in Germany by Krieg et al. [12] and the cut-off values for short participants in the 2010 meta-analysis by Paajanen et al. [9]. To follow up on the height categorisation, we also conducted sensitivity analyses in models where height was split into quartiles.
To investigate possible non-linear relationships between height and incident MI, hazard ratios were also modelled using restricted cubic splines with six knots along the height distribution in both sexes. Furthermore, the association between height and MI in each level of education was estimated by adding two-way cross product terms between height and indicator variables of education to a model including the main effects of height and educational level. In separate models we have also in a similar manner assessed possible interaction between height and birth cohorts. We used likelihood-ratio tests to test the above mentioned interactions with educational levels and birth cohorts. The proportional hazard assumption was verified by log minus log survival plots over height as a categorical variable.
All above mentioned models included age at baseline and indicator variables of five birth cohorts (1930–1939, 1940–1949, 1950–1959, 1960–1969 and 1970–1977) as possible confounders. Additionally, SBP, DBP, TCH, triglycerides and smoking status were added as mediators in separate models.
Results
The study sample consisted of 15,408 women and 14,759 men, aged 30–49 years at baseline (1979–2016), followed up until 31 December 2021, contributing with 660,514 person-years of follow-up. Median observation time was 25.9 years, with 2027 MI cases diagnosed during the follow-up period.
Descriptive baseline characteristics of participants by sex are presented in Table I. Mean age and height at baseline were 37.9 years and 164.9 cm in women and 38.2 years and 178.2 cm in men. Mean BP and lipid levels were slightly higher in men compared with women, smoking status was similarly distributed and upper secondary education was the most frequent educational level in both sexes.
Descriptive characteristics at baseline by sex. The Tromsø Study 1979–2016.
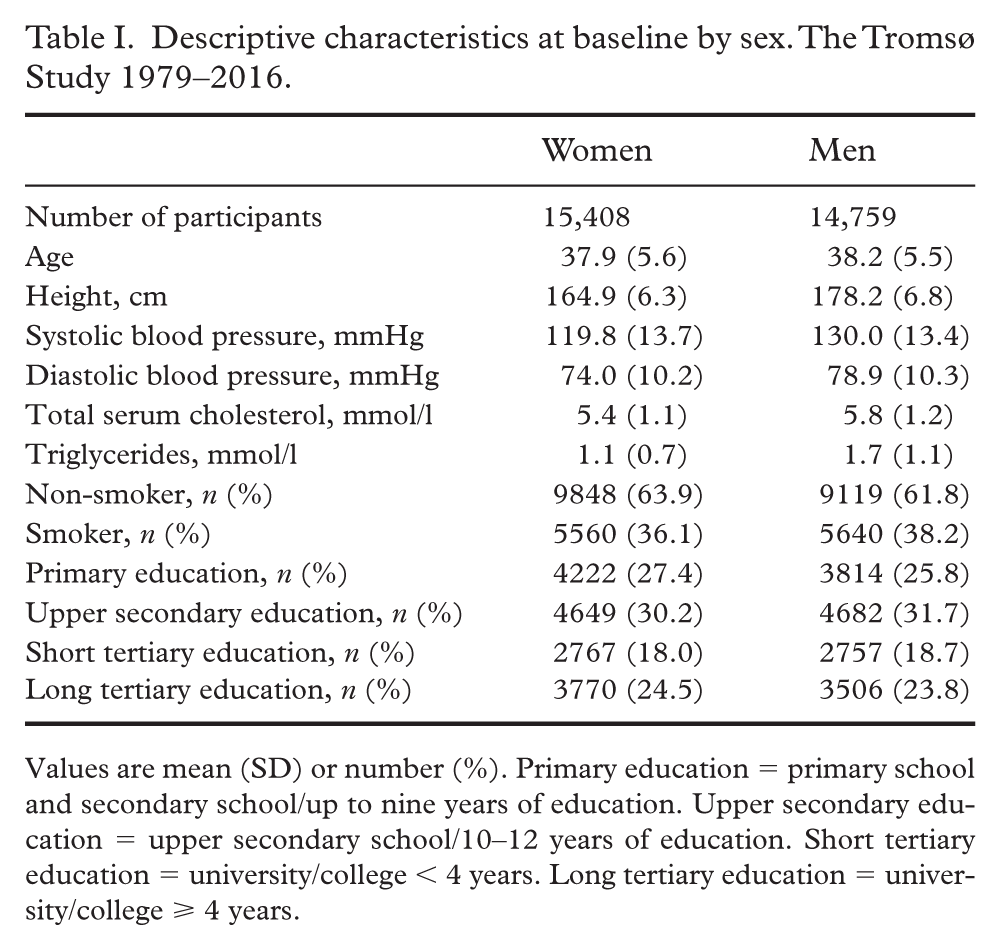
Values are mean (SD) or number (%). Primary education = primary school and secondary school/up to nine years of education. Upper secondary education = upper secondary school/10–12 years of education. Short tertiary education = university/college < 4 years. Long tertiary education = university/college ⩾ 4 years.
Hazard ratios for the associations between height and incident fatal or non-fatal MI are presented in Table II. One SD taller height was associated with 18% lower MI risk in women (hazard ratio 0.82 (95% confidence interval (CI) 0.78, 0.93)) and 13% lower MI risk in men (hazard ratio 0.87 (95% CI 0.83, 0.92)). The difference between sexes was statistically significant (p=0.02).
Hazard ratios for incident myocardial infarction according to height as continuous or categorical variables in women and men. The Tromsø Study 1979–2021.
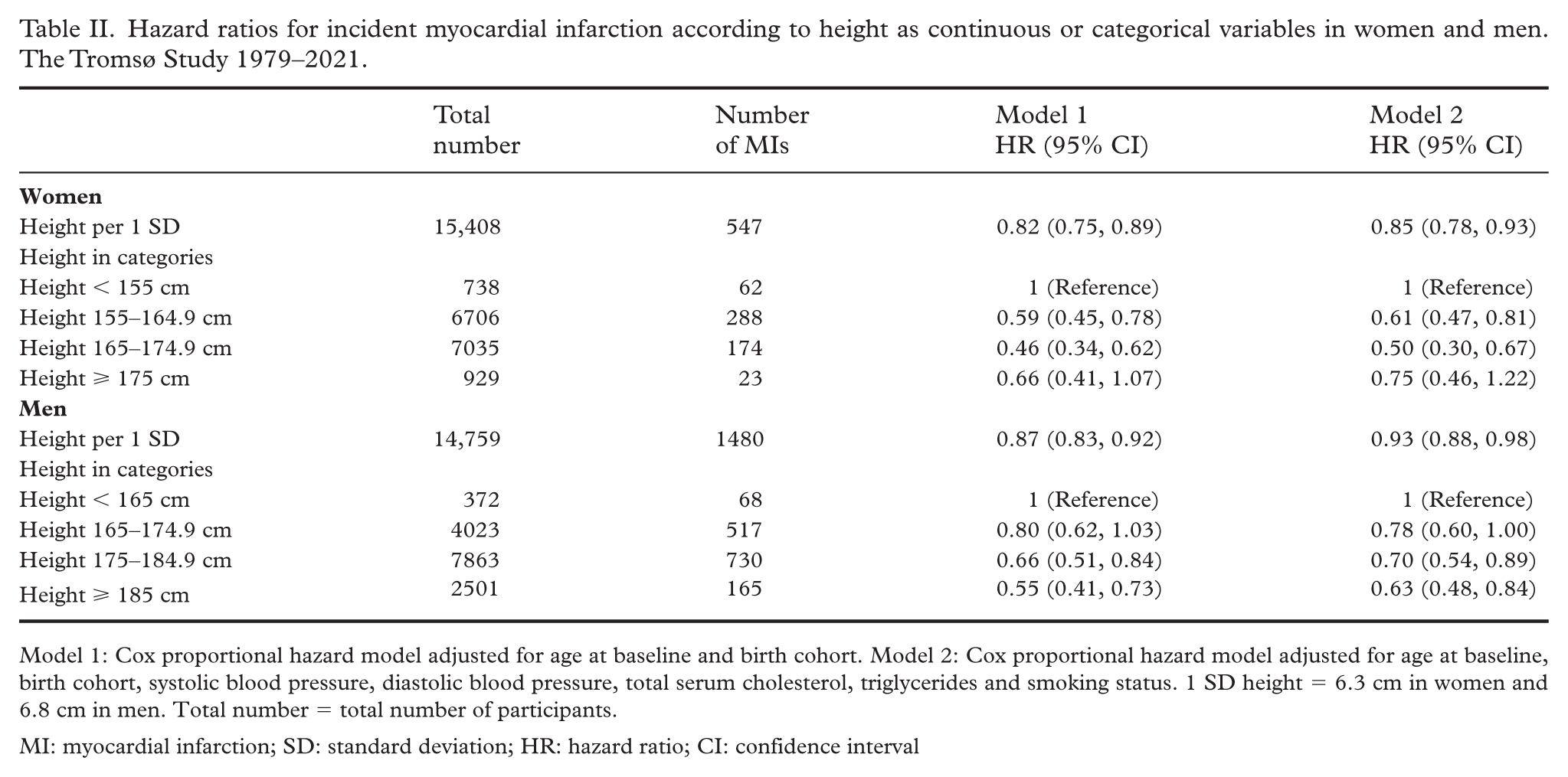
Model 1: Cox proportional hazard model adjusted for age at baseline and birth cohort. Model 2: Cox proportional hazard model adjusted for age at baseline, birth cohort, systolic blood pressure, diastolic blood pressure, total serum cholesterol, triglycerides and smoking status. 1 SD height = 6.3 cm in women and 6.8 cm in men. Total number = total number of participants.
MI: myocardial infarction; SD: standard deviation; HR: hazard ratio; CI: confidence interval
In women, height between 155 cm and 164.9 cm was associated with a 41% lower MI risk (hazard ratio 0.59 (95% CI 0.45, 0.78)) compared with the low height reference group (<155 cm). Height between 165 cm and 174.9 cm was associated with a 54% lower MI risk (hazard ratio 0.46 (95% CI 0.30, 0.67)). There was no difference in risk between the tallest height group (height ⩾175 cm) and the low height reference group (hazard ratio 0.66 (95% CI 0.41, 1.07)).
In men, there was no difference in risk between the 165–174.9 cm height group and the low height reference group (<165 cm) (hazard ratio 0.80 (95% CI 0.62, 1.03)). Height between 175 cm and 175.9 cm and height ⩾185 cm were associated with 34% and 45% lower MI risk compared with the low height reference group (hazard ratio 0.66 (95% CI 0.51, 0.84)) and (hazard ratio 0.55 (95% CI 0.41, 0.73)), respectively.
Model 2 showed inverse associations between height and incident MI in both sexes. Hazard ratios for MI according to restricted cubic splines of height are presented in Figure 2. Mean height at baseline was used as the reference value. Hazard ratios show a slight deviation from the linearity assumption in women. However, the hazard ratios agree with the Cox regression analysis when accounting for the 95% confidence bands and a test for non-linearity was not significant (p= 0.06)
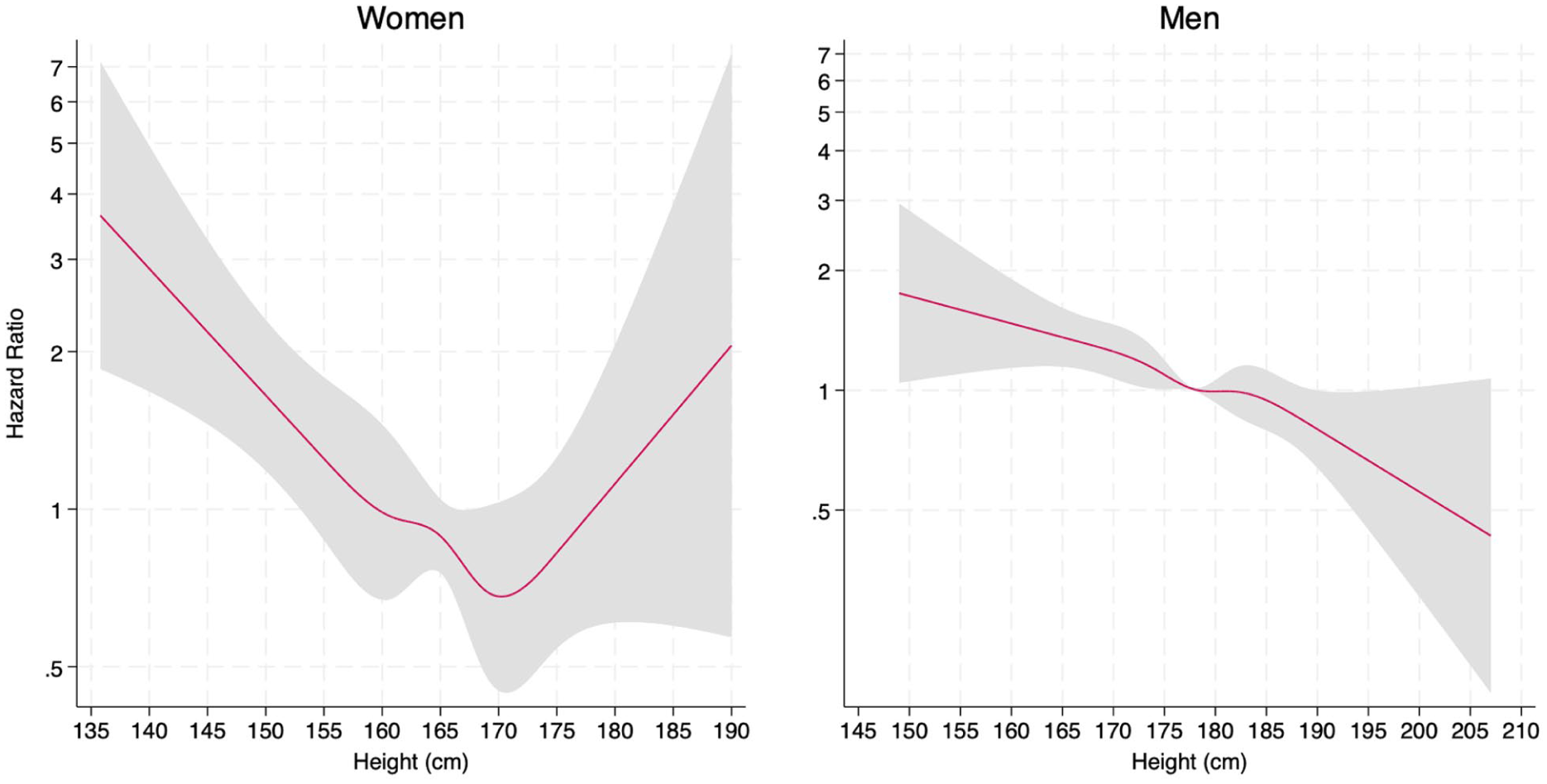
Hazard ratios for myocardial infarction according to height modelled with restricted cubic splines adjusted for age at baseline and birth cohort. The red lines correspond to central estimates, and the grey-shaded areas indicate 95% confidence intervals.
Sensitivity analyses are presented in Supplemental material Table I. In our analysis using height divided into quartiles as a categorical variable, we observed lower hazard ratios with taller height in both sexes and all findings were statistically significant, except for height Q2 in women and height Q3 in men in Model 2.
Hazard ratios for estimates of associations between MI per 1 SD increase in height by sex and educational level are presented in Table III. Hazard ratios in women ranged from 0.81 (95% CI 0.68, 0.96) to 0.87 (95% CI 0.58, 1.30), while hazard ratios in men ranged from 0.85 (95% CI 0.80, 0.97) to 0.95 (95% CI 0.88, 1.03). Likelihood-ratio tests showed no interactions between height and educational level (p=0.95 in women and p=0.27 in men) or height and birth cohorts (p=0.07 in women and p=0.76 in men). Sensitivity analyses of hazard ratios adjusted for CVD risk factors were comparable to the main model and are presented in Supplemental Table II.
Hazard ratios for incident myocardial infarction per standard deviation increase in height by sex and educational level. The Tromsø Study 1979–2021.
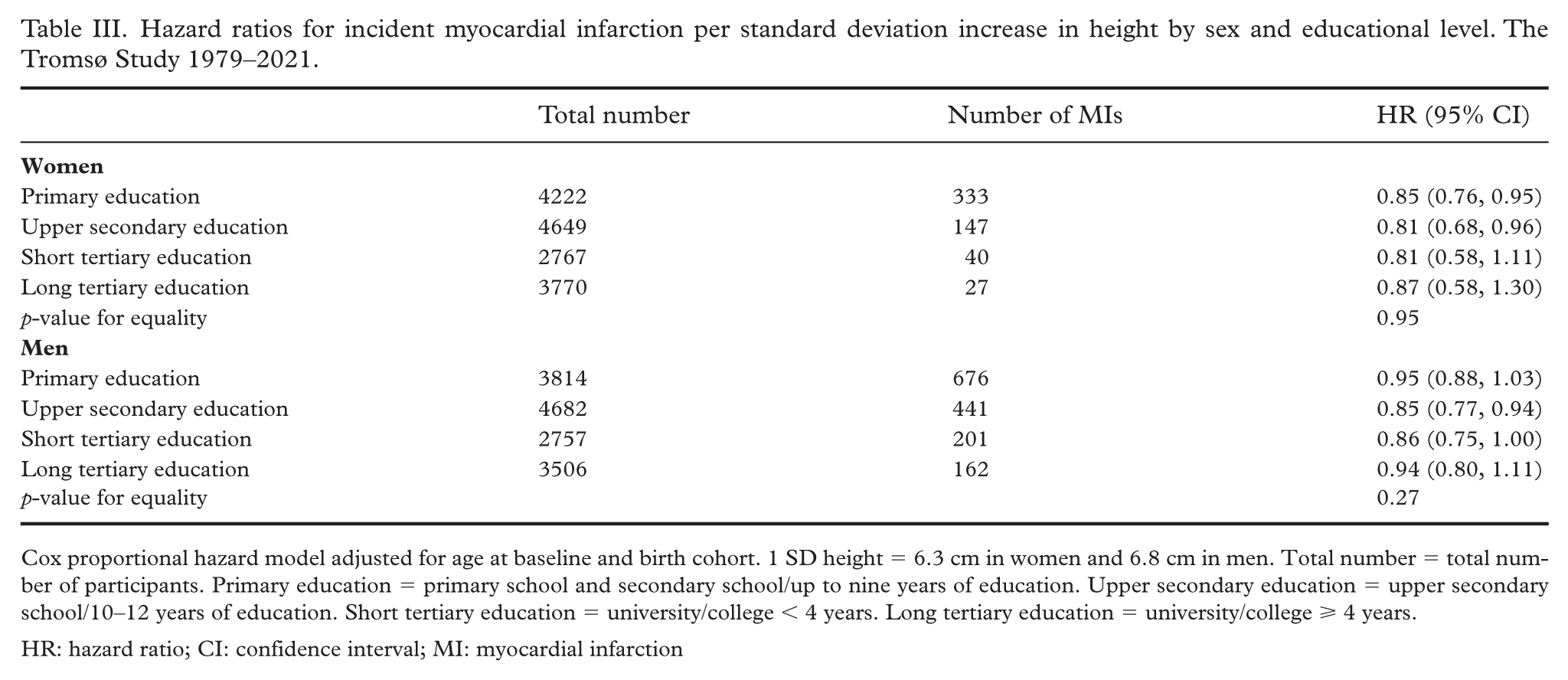
Cox proportional hazard model adjusted for age at baseline and birth cohort. 1 SD height = 6.3 cm in women and 6.8 cm in men. Total number = total number of participants. Primary education = primary school and secondary school/up to nine years of education. Upper secondary education = upper secondary school/10–12 years of education. Short tertiary education = university/college < 4 years. Long tertiary education = university/college ⩾ 4 years.
HR: hazard ratio; CI: confidence interval; MI: myocardial infarction
Discussion
Height, as continuous and categorical variables, was inversely associated with incident MI in Norwegian women and men. Adjustments for known CVD risk factors as possible mediators slightly attenuated these associations. Our findings are in line with most previous international studies of MI or CHD in women [8,10 –12] and men [7,9,12,27].
We found stronger inverse associations between height and MI in women compared with men, similar to previously reported in UK and US populations [11,16]. In contrast to our findings, Krieg et al. reported that 10 cm taller height was associated with slightly lower odds of CHD in men (odds ratio = 0.87) compared with women (odds ratio = 0.91) [12]. However, taller height is generally associated with lower MI risk [10]. Our findings suggest that taller height might be an even greater advantage in relation to MI risk in Norwegian women than in men, adding renewed sex-specific knowledge to a research field where research on male populations has historically dominated [7,27].
We found few associations between height and MI according to educational level, with the only significant results in primary educated women and upper secondary educated women and men. There was no interaction between height and educational level in either sex, suggesting that educational level does not modify the associations between height and MI in our study population. Research that can be used for direct comparisons of our findings by educational levels is scarce. Our results contrast with findings by Silventoinen et al. [14], who showed clear gradients between educational levels in associations between height and CHD. However, they also concluded that height as an explanatory factor for social inequality in risk of CHD was limited, since the associations between height and CHD risk were not particularly strong when stratified by educational level.
Mechanisms behind the inverse relationship between height and incident MI are currently unknown. Suggested physiological mechanisms are smaller coronary arteries, lower lung volume, elevated BP and lipid levels [13]. The smaller arteries and lower lung volume in women compared with men might be an explanation for the differences between sexes observed in our study. However, the inverse associations might also partly result from early-year living conditions, impacting height and later CVD risk [5,6,8]. Birth cohort effect is a possible explanation for the lack of associations between height and MI in the tertiary educated in The Tromsø Study [28]. Most primary or upper secondary educated were born between 1930 and 1950, while most tertiary educated participants were born between 1960 and 1977. The later birth cohorts were not followed up to old age, which might have resulted in low power in the analyses for the long tertiary educated group, especially in women, considering that the median onset age of MI in Norway is 76 years in women and 67 years in men [29].
Study strengths and limitations
The main strength of our study is the comprehensive Tromsø Study data with measured height in a large population with validated MI diagnoses and long follow-up time. Diagnoses from the national register were previously validated against the local register and found valid and reliable [25,30]. Our study builds upon the 1984 findings of Waaler [20], with five decades of data from The Tromsø Study, showing the value of the long running population studies of Norway.
Our study is strengthened by the presentation of sex-specific associations between continuous and categorical measures of height and MI risk and separate analyses by educational level. This approach allows for easy dissemination of findings to the public and contrasts recent studies where sex or educational level is included as covariate in the statistical analyses.
Our study also has some limitations. Living conditions during childhood might influence height and MI risk in adulthood [5,6]; however, data on family financial situation during childhood were not included in Tromsø3 and Tromsø5. Consequently, we chose not to include these variables. Genetic factors or information on family history of CVD, which might predispose for MI, were also not available in our dataset.
Conclusion
Height was inversely associated with incident MI in Norwegian women and men. We found stronger inverse associations in women compared with men, which might suggest that taller height is a greater advantage in relation to MI risk in Norwegian women. There were no differences between educational levels, suggesting that education does not modify the inverse associations between height and MI in a Norwegian population. Future studies should strive to incorporate measures of early-year living conditions and genetic markers associated with height and MI risk.
Supplemental Material
sj-docx-1-sjp-10.1177_14034948261428946 – Supplemental material for Height and risk of myocardial infarction in The Tromsø Study 1979–2021
Supplemental material, sj-docx-1-sjp-10.1177_14034948261428946 for Height and risk of myocardial infarction in The Tromsø Study 1979–2021 by Sondre Haakonson Arntsen, Tom Wilsgaard, Kristin Benjaminsen Borch and Anne Helen Hansen in Scandinavian Journal of Public Health
Footnotes
Author contributions
This study was conceived and designed by Sondre Haakonson Arntsen, Tom Wilsgaard, Kristin Benjaminsen Borch and Anne Helen Hansen. Statistical analyses were conducted by Sondre Haakonson Arntsen and Tom Wilsgaard. The first draft of the manuscript was written by Sondre Haakonson Arntsen. All authors read, revised and approved the final manuscript.
Data availability statement
The Data and Publications committee (DPC) of The Tromsø Study has imposed strict restrictions on data sharing, including datasets to prevent the potential re-identification of de-identified sensitive participant information. Thus, we are unable to upload our dataset to a public repository or share it freely. However, the minimal dataset supporting the findings in our study can be accessed upon reasonable request by sending an application to The Tromsø Study, following the procedures outlined on their webpage: ![]() .
.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The PhD position of Sondre Haakonson Arntsen was funded internally by UiT The Arctic University of Norway. Our study is part of the Healthy Choices and the Social Gradient Project, which is funded by UiT The Arctic University of Norway and the Norwegian Research Council (NRC project grant 289440). The funding organisations had no role in the design, analyses, interpretation or write up of this study.
Ethical considerations
Our study was approved by the Regional Committee for Medical and Health Research (REC North 186065). Participants from Tromsø2–3 provided verbal consent, which was common practice at the time of data collection (Tromsø2 1979–1980 and Tromsø3 1986–1987). The use of data collected from participants who provided only verbal consent in Tromsø2–3 was approved by REC North. Written consent for the use of collected data in future research projects was provided by the participants who attended Tromsø4–7.
Supplemental material
Supplemental material for this article is available online.