
Abstract
Aims:
Sleep difficulties among adolescents are of a significant concern given its associations with adverse health outcomes. The aims of the present study were to examine trends and predictors of self-perceived difficulties in getting to sleep among adolescents in the Nordic countries.
Methods:
The study was based on cross-sectional data from 10- to 17- year-olds (N = 139,799) from six Nordic countries (Sweden, Iceland, Norway, Denmark, Greenland, and Finland) participating in the international Health Behaviour in School-aged Children (HBSC) study, collected via six survey rounds in the period 2002–2018.
Results:
Since 2002, the prevalence of self-perceived difficulties in getting to sleep has risen in all Nordic countries. However, from 2014 to 2018, the trend of adolescents reporting difficulty more than weekly increased in Denmark, Finland, Greenland, and Norway, whereas it was mostly stable in Sweden, and Iceland showed a reduction. Predictors of difficulties in getting to sleep varied across countries, but younger age, reduced life satisfaction, decreased physical activity, feeling low, and feeling nervous were common predictors across the six countries. Gender and perceived family wealth had different effects on difficulties getting to sleep in different countries.
Conclusions:
Keywords
Introduction
Sleep difficulties among adolescents have become a significant public health concern, especially in Nordic countries. Numerous studies have established a strong link between sleep problems and various adverse outcomes, including a decline in mental health [1, 2]. It should be noted that there may be a bidirectional causal relationship between sleep and mental health. In the present study we focus on mental health as a predictor of difficulties in getting to sleep, but clearly sleep problems may be causing mental health problems. Despite this, there is limited research focusing on the specific personal and sociocultural factors in the Nordic context that exacerbate sleep difficulties among adolescents. This study aimed to address the gap in understanding how Nordic socioenvironmental factors contribute to difficulties in getting to sleep among adolescents by employing a comprehensive comparison of the respective countries over time and identifying key predictors. These insights will not only advance the scientific understanding of adolescent sleep problems but also inform public health policies and school interventions tailored to mitigate sleep difficulties in Nordic contexts.
Sleep and mental health
In recent years, more research has focused on the relationship between the sleep behavior of adolescents and their mental function. Worryingly, a substantial proportion of adolescents is failing to achieve the recommended 8–10 hours of sleep per night and experiences sleep difficulties. A study examining sleep quality and quantity among adolescents in three countries (Estonia, Iceland, and Spain) reported that about half of the adolescents (44% of boys and 53% of girls) experienced poor sleep-quality, and more than two-thirds did not get 8–10 hours of sleep per night [3]. A previous study by the present research group [4] showed that around a quarter of Nordic adolescents reported difficulties in getting to sleep and that this rose between 2002 and 2014 among adolescents within the Nordic countries, other than Norway. As a result, Thorsteinsson et al. suggested that sleep trends need to be monitored more closely and that future studies need to include predictive factors of sleep difficulty [4].
Inadequate sleep during adolescence is associated with negative outcomes, including somatic and psychosocial health, poor school performance, and risk-taking behavior [5], self-reported emotional and behavioral problems [6], as well as loneliness [7] and lower quality of life [8]. Sleep problems (e.g., continuity, depth) in adolescents, as well as in older adults, have been found to be associated with mental health problems such as anxiety, eating disorders, borderline personality disorder, and schizophrenia [9]. Poor sleep-quality obviously contributes to fatigue [10], but may also mediate the relationship between depression and fatigue [11, 12]. The presence and direction of a causal relationship between sleep and mental health may not be clear. It is most likely to be bidirectional, that is, poor sleep can be a symptom of mental health problems but can also be a cause of them.
In parallel to the observed increase in difficulties in getting to sleep among Nordic adolescents, 2002–2014 [4], trends of decline in reported life satisfaction (measured on the Cantril Scale) were shown for the same population [13]. The present study therefore employed three measures of mental health: life satisfaction, feeling low, and feeling nervous.
Sleep and physical activity
Physical activity is another factor that should be considered when studying the decline in adolescent sleep hours, as many adolescents seem to be physically inactive [14] and research suggests an association between physical activity and mental health [15]. Furthermore, there may be a bidirectional relationship between physical activity and sleep. A meta-analysis of randomized control trials among adults showed that both physical activity, such as walking, and mind–body activity such as yoga, can improve sleep quality significantly [16]. Thus, given the potential links between physical activity and mental health [17] and the link between physical activity and sleep, it is important to consider physical activity as a factor of interest in studies of adolescent sleep.
Sleep and socioeconomic circumstances
Even in the supposedly equalitarian and welfare-orientated Nordic countries, it is of pivotal importance to consider the effects of socioeconomic status (SES) on all aspects of health, including difficulties in getting to sleep. Adolescents from lower SES backgrounds often face greater sleep disturbances due to heightened stress, inadequate sleep environments, and higher exposure to family conflicts [18]. Studies also indicate that financial stress and lower parental education levels are associated with shorter sleep duration and poorer sleep-quality [19].
Present study
The aims of the present study were twofold. First, to document trends in sleep difficulty (i.e., difficulties falling asleep) among Nordic adolescents from 2002 to 2018 to see whether the general increase in difficulties getting to sleep from 2002 to 2014 continued to grow. Second, to identify possible relations between difficulties in getting to sleep and mental health (measured by life satisfaction, feeling low, and feeling nervous), physical activity, and perceived family wealth. It was expected that difficulties in getting to sleep would be negatively associated with increased life satisfaction, physical activity, and family SES, while it would be positively associated with increased levels of feeling low and feeling nervous.
Method
Participants
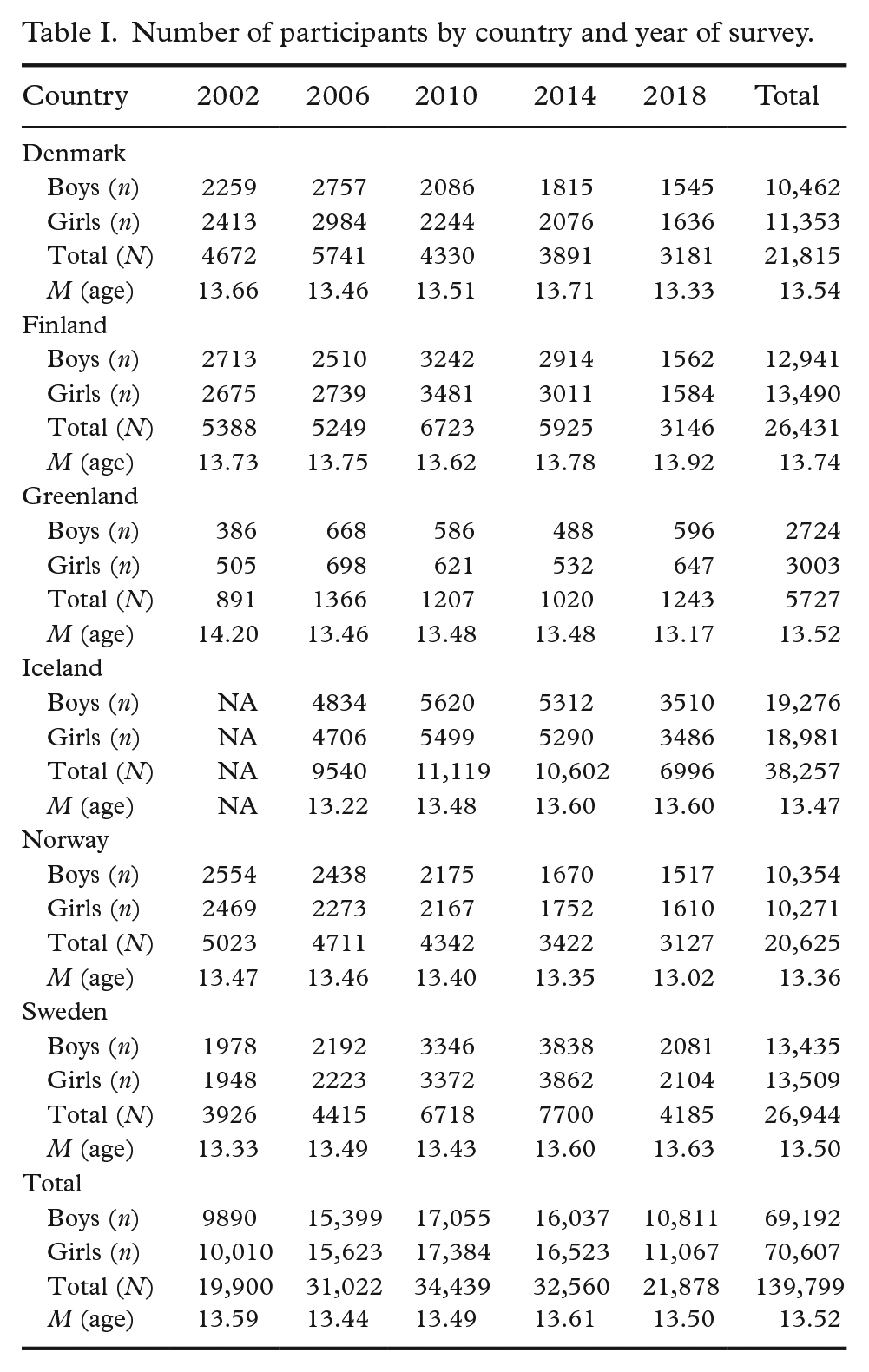
The present study employed cross-sectional data from 139,799 participants (69,192 boys and 70,607 girls) from 10.5 to 17.3 years of age (M = 13.5, SD = 1.7). The data were collected as part of the Health Behaviour in School-aged Children (HBSC) study, which is a World Health Organization collaborative international survey [20] collected in Denmark, Finland, Greenland, Iceland, Norway, and Sweden. The data collections take place every fourth year: 2002 (Iceland was not included in this particular year), 2006, 2010, 2014, and 2018. The sample size by country and year ranged from 891 to 11,119 (see Table I).
Number of participants by country and year of survey.
Each country selects a nationally randomized representative sample of boys and girls aged 11, 13, and 15 years old, while adhering to the international HBSC study protocol [21]. That said, the sampling unit varies by country. National cluster sampling from school classes was employed in Finland, Norway, and Sweden [22]. The entire population was targeted for the ages in question in Greenland and Iceland. In Denmark, the sampling unit was the school.
The study questionnaire consists of over 100 items, some of which are mandatory while others are optional or country specific. Parents, school administrators, and teachers were informed of the study in advance. Adolescents were able to opt out and were offered the opportunity to decline participation. All of them were informed that their participation in the study was voluntary and their responses would be anonymous. In participating schools, teachers supervised the adolescents as they completed the questionnaires in their usual classrooms. All countries followed the national research ethics requirements, which in some countries included obtaining approval from ethical authorities.
The data from the present study were collected during school hours, ensuring there was enough physical space between students to secure anonymity. In the first waves of the study, the questionnaire was answered using pen and paper, however, development in the later waves has been more toward computerized forms, which most countries had adopted completely in the last wave. All six countries used the same mandatory HBSC questions; further details on the HBSC survey methodology are available [23, 24].
Measures
Four key demographic measures were assessed: 1) gender (boys and girls), 2) year of investigation (2002, 2006, 2010, 2014, and 2018), 3) country (Denmark, Finland, Greenland, Iceland, Norway, Sweden), and 4) age in years at the time of data collection.
Difficulties in getting to asleep
This was assessed based on one item from the HBSC multiple health complaints checklist [25], which consists of eight items covering different health complaints. The list of items was preceded by the question, “In the last 6 months: how often have you had the following . . .?” followed by eight complaint items, one of which was “difficulties in getting to sleep.” Response options were presented on a 5-point frequency scale, reversing the order of the original scoring, that is, the scores increased with increased sleep difficulty: 1 = rarely or never, 2 = about every month, 3 = about every week, 4 = more than once a week, and 5 = about every day. In the present study, participants were split into two groups based on the frequency of experiencing difficulties in getting to sleep: Group 1 with a lower frequency of difficulties in getting to sleep (i.e., “about every week,” “about every month,” and “rarely or never”), and Group 2 reporting difficulties in getting to sleep at least once a week (i.e., sleep difficulties “about every day” or “more than once a week”). This dichotomy was done to facilitate comparisons with previous research [4] and for our logistic regression analysis.
Mental health
One way of measuring mental health is to look at self-reported life satisfaction. The HBSC assesses life satisfaction using the simple, visual Cantril Scale [26]. The students are asked “Where in this ladder is your life now” using an 11-point visual scale from 0 (“worst possible life”) at the bottom of the ladder to 10 (“best possible life”) at the top of the ladder. The Cantril ladder has shown good reliability and convergent validity among adolescents [27], and has been found to broadly assess adolescent psychosocial health [28]. This single-item assessment has been shown to have similar validity as a multi-item assessment of life satisfaction among adults [29] and adolescents [30].
We used two items from the HBSC symptom checklist to further assess mental health: (a) feeling nervous and (b) feeling low. Both were measured on a 5-point frequency scale. In our analysis, the scores were reversed from the original data, so that they increased with increased feelings of nervousness and of feeling low: 1 = rarely or never, 2 = about every month, 3 = about every week, 4 = more than once a week, and 5 = about every day. Participants were then split into a low group consisting of those who generally do not feel low and do not feel nervous (i.e., “rarely or never” and “about every month”) respectively, and those who feel low or nervous more frequently (i.e., “about every week,” “more than once a week,” or “about every day”). The HBSC multiple health complaints symptom checklist measure has been shown to have acceptable test–retest reliability and internal consistency [31–33]. The checklist has also been validated across various cultures and contexts, demonstrating good psychometric properties, including both convergent and discriminant validity [25, 34–36]. The same applies to the use of individual items that were used in the current study such as sleeping difficulties and feeling nervous or low [33].
Physical activity
Physical activity was assessed with a question on moderate to vigorous physical activity: “Over the past 7 days, on how many days were you physically active for a total of at least 60 min per day?” with response options ranging from 0 (“0 days”) to 7 (“7 days”). The item has shown reasonable validity and moderate reliability [37, 38].
Perceived family wealth
Perceived family wealth was based on the question “How well-off do you think your family is?” on a scale of 1 = not at all well-off, 2 = not very well-off, 3 = average, 4 = quite well-off, and 5 = very well-off, after reverse coding the original. In Denmark in 2018, this question was adjusted to read “How rich is your family?” answered on a scale from 1 (“very poor”) to 5 (“very rich”) after reverse coding. The present analysis does not include measures of perceived family wealth for Denmark in 2018 nor for Iceland in 2002 and 2018.
Statistical analysis
SPSS (v28.0.1.0) was employed for statistical analysis. Difficulties in getting to sleep (i.e., “about every day” or “more than once a week”) were plotted by country across the different years of investigations, 2002–2018, to show the trend over time and to enable comparison with previous trend analyses.
A binary logistic regression was employed in predicting difficulties in getting to sleep: Group 1 (coded as 0) with lower frequency of difficulties in getting to sleep (i.e., “about every week,” “about every month,” and “rarely or never”), and Group 2 (coded with 1) with higher frequency (i.e., had difficulties in getting to sleep “about every day” or “more than once a week”). Predictors included year of investigation, age, gender, life satisfaction, physical activity, perceived family wealth as a measure of SES, feeling low, and feeling nervous.
Given the large sample sizes for different countries in the present study the Hosmer–Lemeshow test of model fit was biased [39] and thus was given limited attention. Nagerlkerke’s R2 has a range of values from 0 to 1, but cannot be interpreted as a proportion of variance explained as with R2 for linear regression analysis. The Cox and Snell R2 also has a range of values from 0 to a maximum value of less than 1 even for a perfect model.
Results
Sleep difficulty
Figure 1 shows that from 2002 to 2006 there was a trend of increased prevalence of difficulties in getting to sleep among adolescents in Denmark, Finland, and Norway, while this prevalence declined in Greenland and Sweden. From 2006 to 2010 trends were stable, except for Greenland where it increased from 17.6% to 21.4%. This trend continued for Greenland with a further increase from 2010 to 2014 of almost 7 percentage points. Over the same period (2010–2014) difficulties in getting to sleep among Swedish adolescents increased by more than 9 percentage points, by 5 percentage points in Iceland, and by 2 percentage points in Finland. Norway was the only country with a reduction in difficulties in getting to sleep (more than 4 percentage points), while Denmark remained stable from 2010 to 2014. From 2014 to 2018, Greenland continued its trend of worsening difficulties in getting to sleep, with 39.5% of adolescents experiencing difficulty more than weekly. Denmark, Finland, and Norway had some increase, while Sweden was mostly stable, and Iceland showed a reduction.
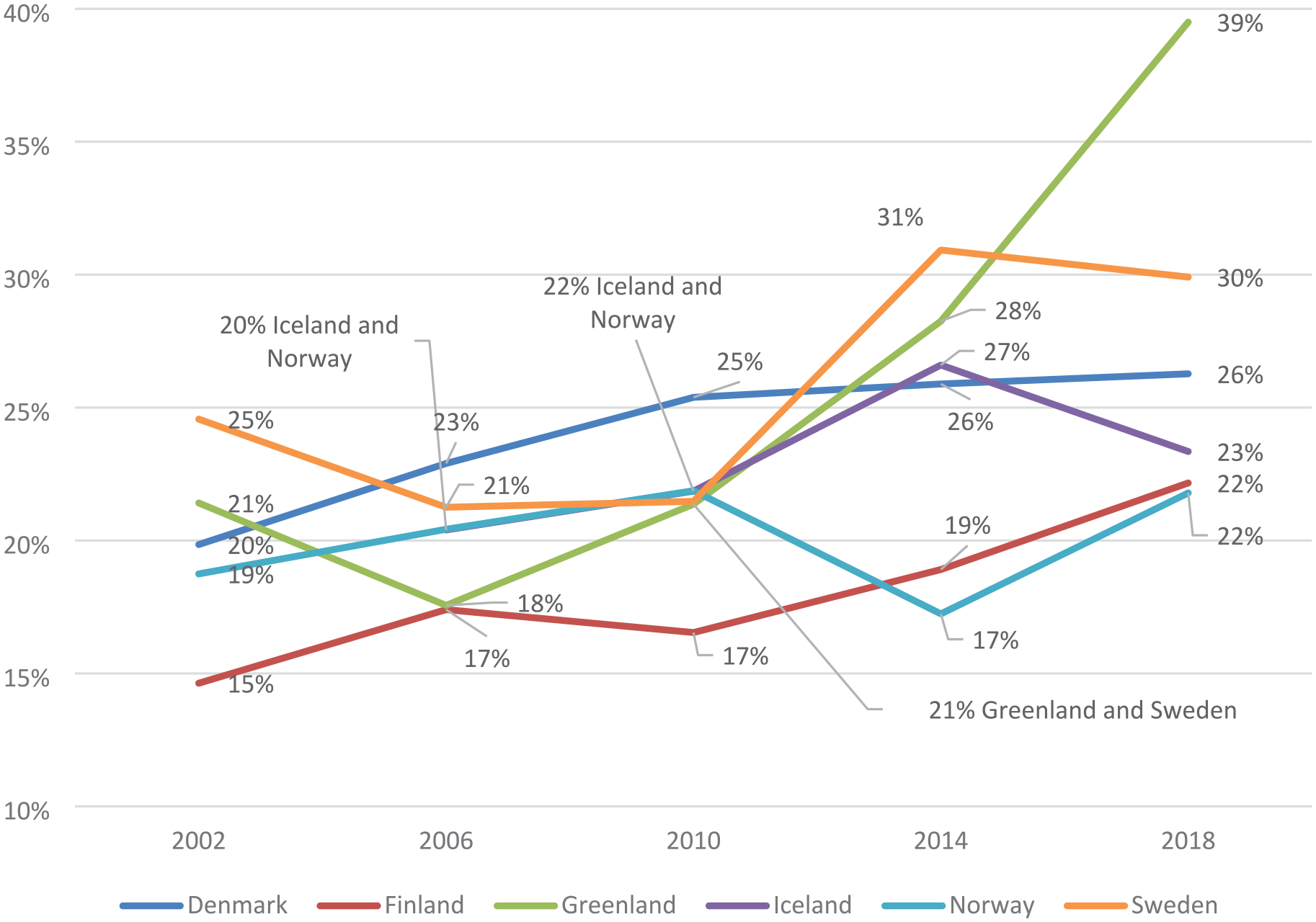
Percentage of more than weekly difficulties in getting to sleep by country and year of investigation.
Predictors of sleep difficulty
Table II shows that year of investigation had a limited effect in Denmark, Greenland, Iceland, Norway, and Sweden, predicting only a minor probability of a rise in sleep difficulty from year to year. This was supported by the results in Figure 1 that show a rise in difficulties in getting to sleep from 2002 to 2018 but with different patterns across the years for each country. Increased age was associated with fewer difficulties in getting to sleep in all countries but Greenland, where there was no significant association. Being a boy was associated with increased difficulties in getting to sleep in Denmark, Iceland, and Sweden. Being a girl was associated with increased difficulties in getting to sleep in Finland. However, in Greenland and Norway there was no effect for gender. Increased life satisfaction was associated with reduced difficulties in getting to sleep across all six nations. Physical activity reduced difficulties in getting to sleep in Denmark, Iceland, Norway, and Sweden but had no significant association in Finland and Greenland. Perceived family wealth reduced difficulties in getting to sleep in Finland, Iceland, Norway, and Sweden, while increasing it in Greenland and showing no significant association in Denmark. Feeling low and feeling nervous increased difficulties in getting to sleep across all six nations. The direction and strength of the associations between different predictors (i.e., year of investigation, age, gender, life satisfaction, physical activity, perceived family wealth, feeling low and feeling nervous) and the outcomes may vary from the corresponding prevalence rates for difficulties in getting to sleep due to potential suppressor variables among the predictors.
Predicting (odds ratio; OR) difficulties in getting to sleep from year of investigation, age, gender, life satisfaction, physical activity, family SES, feeling low, and feeling nervous by country.
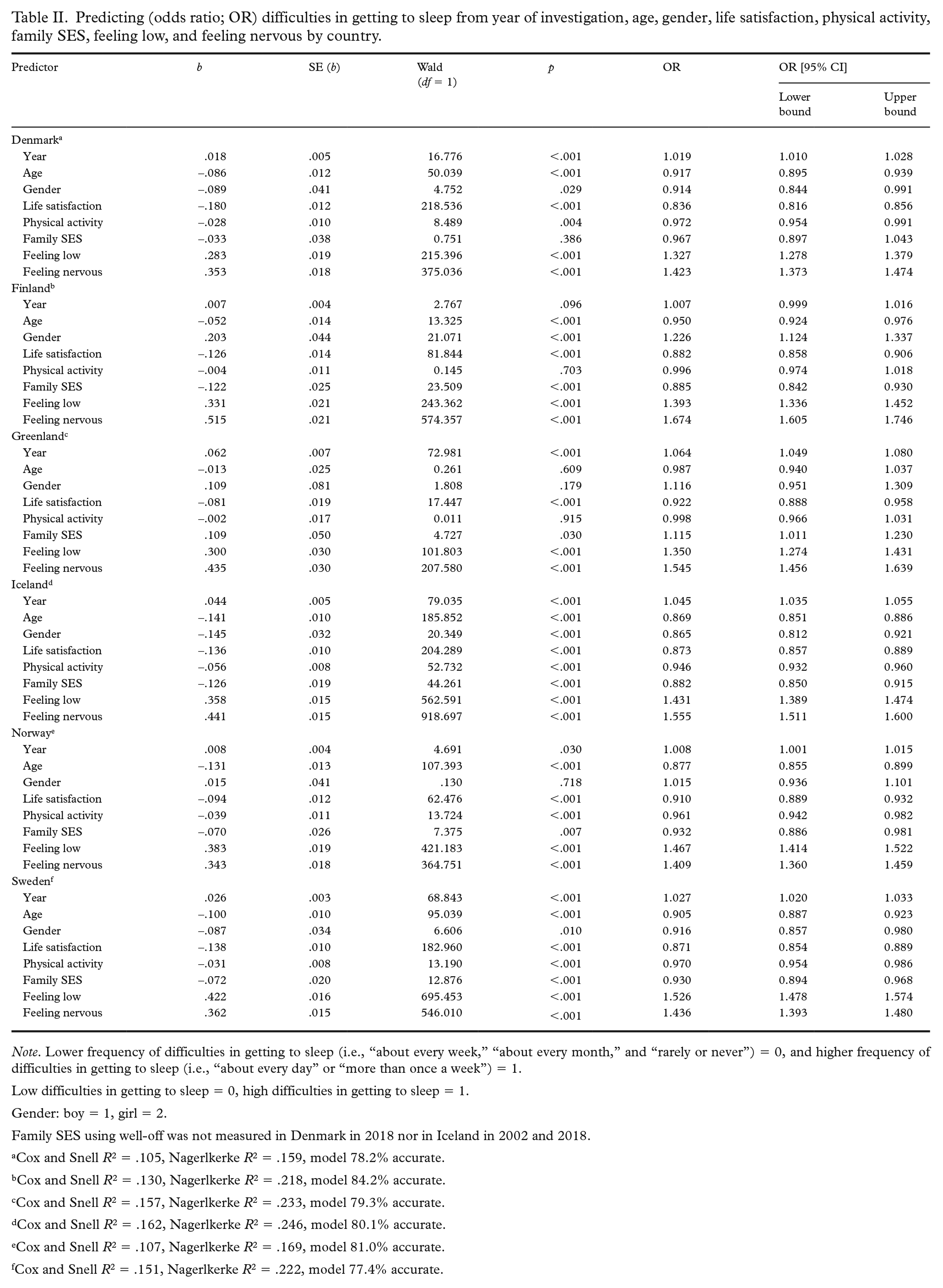
Note. Lower frequency of difficulties in getting to sleep (i.e., “about every week,” “about every month,” and “rarely or never”) = 0, and higher frequency of difficulties in getting to sleep (i.e., “about every day” or “more than once a week”) = 1.
Low difficulties in getting to sleep = 0, high difficulties in getting to sleep = 1.
Gender: boy = 1, girl = 2.
Family SES using well-off was not measured in Denmark in 2018 nor in Iceland in 2002 and 2018.
Cox and Snell R2 = .105, Nagerlkerke R2 = .159, model 78.2% accurate.
Cox and Snell R2 = .130, Nagerlkerke R2 = .218, model 84.2% accurate.
Cox and Snell R2 = .157, Nagerlkerke R2 = .233, model 79.3% accurate.
Cox and Snell R2 = .162, Nagerlkerke R2 = .246, model 80.1% accurate.
Cox and Snell R2 = .107, Nagerlkerke R2 = .169, model 81.0% accurate.
Cox and Snell R2 = .151, Nagerlkerke R2 = .222, model 77.4% accurate.
Discussion
The present study aimed to examine trends in adolescent difficulties in getting to sleep from 2002 to 2018 and to examine predictors of the difficulty across six Nordic countries. In short, a rise in difficulties in getting to sleep among adolescents was found in all Nordic countries between 2002 and 2018. In Norway, the increase was small, but in the other countries it was quite profound. This increase was especially strong in Greenland. This showed the continuation of the worrying trend that was noted for the prevalence of sleep difficulties from 2002 to 2014 in the same Nordic countries [4]. The strength of the different predictors varied by country, however, feeling low, feeling nervous, and life satisfaction were consistently important predictors of sleep difficulty.
Difficulties in getting to sleep
The increasing prevalence of difficulties in getting to sleep among Nordic adolescents over recent years is a significant public health concern. This trend aligns with findings from other regions, which highlight the multifaceted nature of adolescent sleep problems. Factors identified by other studies such as increased academic pressures, extensive use of digital devices, and socioeconomic disparities contribute to this rise [40–43]. Addressing these issues requires comprehensive strategies that consider the unique cultural and environmental contexts of the Nordic countries. Interventions should target not only individual behaviors but also systemic factors such as public policies, school policies, and family support systems to effectively mitigate the adverse effects on adolescent sleep and overall well-being.
No earlier investigations have examined difficulties in getting to sleep in Greenland. Greenland is going through very rapid societal change that also puts pressure on youth in relation to a range of factors: life satisfaction, perceived health, and school satisfaction have decreased during the period [44, 45].
Predictors of sleep difficulty
When examining potential predictors of difficulties in getting to sleep, logistic regression analyses showed the impacts of life satisfaction, feeling nervous, and feeling low, which revealed the same pattern in all six countries. These results are in line with previous findings, such as by Mah and Larkings [46]. Furthermore, the results are in line with US findings [47] showing significant associations between sleep disturbance, depression, and internalizing and externalizing behaviors in a sample of pre-adolescents aged 9–10 years.
The effects of being a boy or girl on difficulties getting to sleep varied by country. Despite girls reporting lower life satisfaction, especially in the older age groups in all the countries investigated [22], and generally having a higher symptoms score, in Greenland and Norway no association between gender and difficulties in getting to sleep was observed. This result is consistent with some of the literature that suggests sleep problems in adolescents are influenced more by environmental and behavioral factors rather than gender [48–50]. The lack of gender disparity in our study underscored the importance of focusing on broader social determinants and lifestyle factors when addressing sleep difficulties in this population.
In the present study, SES was measured by perceived family wealth as reported by the children. The effects of perceived family wealth varied by country. In most counties, including Sweden, Finland, Iceland, and Norway, there was an association between perceived family wealth and difficulties in getting to sleep, where greater family wealth was associated with decreased odds of sleep problems. This finding agrees with those of several other studies from Nordic and Western countries and may be explained by factors such as heightened stress, inadequate sleep environments, and higher exposure to family conflicts in these groups [51, 52]. In Greenland, the opposite association was found: greater family wealth was associated with increased odds of sleep problems. However, this association might have been affected by how perceived family wealth was assessed. In Denmark, no significant association between perceived SES and sleep problems was found. This is in contrast to a previous study on trends in difficulties in getting to sleep among the same study population, where a clear social gradient was found, but where the classification of SES was based on parental occupation [52]. In Denmark, the item measuring perceived family wealth (“How well-off do you think your family is?”) was found to have problems with validity, as “well-off” does not translate into an equivalent Danish expression, which may also explain some of the variation in the results. Thus, the selection of indicators for SES may have influenced the results of the analysis of social inequalities in difficulties in falling asleep.
Study strengths
The present study has several strengths. Central to the HBSC study is a standardized protocol ensuring that data are collected using a prescribed methodology, which allows for comparison of data across countries and over time. The use of nationally representative data with a substantial number of participants enabled high-quality research and monitoring. The continuous methodological development and quality assurance of the survey’s standardized methods was also a strength with data collected since 1984 and now available for up to 48 different countries [53].
Sleep problems were captured by asking participants about difficulties in getting to sleep. Thus, other sleep-related dimensions were not assessed, such as quality or duration. Self-reported problems with difficulties in getting to sleep were used, however, self-reported difficulties may give a biased picture of the problem by underestimating it [54]. However, self-report data from a large-scale study provide more generalizable and cost-effective findings and thus are preferable to a small sample with reduced bias but limited generalizability. Furthermore, the items used in the HBSC survey have been found to be reliable [34].
Limitations and future studies
While this study highlights an important trend in adolescent health, addressing the methodological limitations and incorporating measures of symptom impairment in future research will be crucial for developing effective interventions and support systems. Understanding not just the prevalence, but also the impact of these symptoms on adolescents’ lives, is key to fostering their well-being and resilience.
There are several potential interactions and suppressor variables that were not examined in the present study and that may affect difficulties in getting to sleep, such as differences between boys and girls in different survey years in different countries. This should be noted in relation to the results for the Danish sample, where being a boy was associated with increased difficulty in the present study, whereas the opposite has also been observed within single predictor regression. However, such an examination is beyond the scope of the present study, needing detailed focus from studies within each country.
Given the association between feeling nervous, feeling low, and difficulties in getting to sleep, future studies might like to expand the examination of mental health in relation to sleep difficulty. In this study we included gender in the analysis: an in-depth analysis would be of interest considering the higher level of mental health problems found among girls.
Using single-item measures for complex constructs like sleep difficulties and mental health significantly limits the validity and reliability of the data. Single items cannot capture the multifaceted nature of these issues, therefore potentially overlooking critical aspects such as severity, frequency, and impact on daily functioning. Studies such as the HBSC are aimed at giving a broad overview of adolescent health by surveying many individuals and providing an opportunity for comparing trends across countries. However, that broad view comes at a cost, such as in the limited number of items included, to ensure that the students can complete the entire questionnaire with relative ease.
One weakness, as with other studies employing cross-sectional data, is that causality cannot be assumed where association is reported. The relationship between mental health and sleep is most likely bidirectional, that is, feeling low, feeling nervous, and low life-satisfaction can cause sleep disturbances and vice versa. One way to elaborate on this is to look at how interventions to improve sleep affect mental health parameters. In a meta-analysis of randomized controlled trials, Scott et al. found that better sleep had a significant medium-sized effect on composite mental health, depression, anxiety, and rumination [55]. Other related mental health parameters were also significantly affected but to a lesser degree.
Future studies need to examine why there are such differences between adolescents in different countries in relation to difficulties in getting to sleep. Questions such as why there has been a large increase in recent years in difficulties getting to sleep among adolescents in Greenland while their counterparts in Norway show very little change over the same period of time. Such studies may need to combine data from adolescents, adults, and society more broadly to be able to provide a clearer understanding of potential causal factors. The observed increase in difficulties in getting to sleep and mental health symptomology among adolescents may be attributed to broader societal changes influencing mental health. The correlation between sleep disturbances and mental health complaints aligns with existing literature, suggesting that inadequate sleep can exacerbate physical and psychological symptoms, creating a vicious cycle that negatively impacts overall well-being. However, it is also possible that the increase in reported symptoms may reflect greater awareness and willingness among adolescents to acknowledge and report these issues, due to the reduced stigma around mental health. This change in reporting behavior could partly account for the upward trend observed in our data.
A fundamental issue with the current survey methodology is the absence of specific questions regarding symptom impairment. Knowing that adolescents experience difficulties in getting to sleep or mental health symptoms is informative, but understanding the extent to which these symptoms impair their daily lives is crucial. Assessing impairment helps to differentiate between mild, transient issues and severe, chronic conditions that significantly impact the adolescents’ quality of life. This distinction is vital for targeting interventions appropriately. This is where future studies could expand our knowledge by including medication use by adolescents both in relation to general sleep difficulty and in relation to mental health issues.
Questions regarding how the different measurements of SES may affect the relationship between SES and sleep patterns need to be examined further. Thus, future studies might examine multiple indicators of SES, as suggested by Sosso et al., to increase our nuanced understanding of how and why SES influences adolescents’ sleep patterns [51].
Adolescents’ living conditions (i.e., SES), behavioral risk factors, and mental health are closely linked to sleep health. Therefore, it is essential that clinical guidelines for this age group address these factors in the prevention and management of sleep problems, considering their broad impacts on general and mental health. Since maintaining good sleep hygiene is a vital non-pharmacological strategy, clinicians and health care professionals (e.g., health nurses in Denmark) at schools should prioritize educating adolescents on healthy sleep habits.
Future research should delve deeper into these sociocultural and environmental aspects, exploring how they interact with individual behaviors to affect sleep. By understanding these interactions, public health initiatives can be better tailored to address the root causes of sleep difficulties in adolescents. Moreover, interventions that consider the holistic well-being of adolescents are likely to be more effective. Therefore, schools and policymakers should implement comprehensive sleep health programs that address stress management, responsible digital media use, physical activity, and supportive family environments to mitigate sleep problems across the adolescent population. Schools could potentially promote evidence-based sleep hygiene by incorporating sleep education into curricula and addressing the effects of technology use before bed and perhaps consider different times of the day for the start of school. These structural changes, alongside individual behavioral strategies, could potentially significantly enhance adolescents’ sleep health and overall well-being.
Conclusion
Increased difficulties in getting to sleep is associated with an increased sensation of feeling low and feeling nervous, while increased life satisfaction is associated with reduced difficulties in getting to sleep. Other factors such as gender and perceived family wealth had different effects on difficulties getting to sleep depending on the country, with a concerning rise identified in Greenland between 2006 and 2018. These findings underscore the importance of considering multifaceted factors when developing interventions and policies aimed at improving sleep health among adolescents. Future research may delve deeper into the cultural, social, and environmental factors contributing to sleep difficulties, enabling more targeted and effective strategies for promoting healthy sleep habits in this vulnerable population.
Footnotes
Acknowledgements
The international Health Behaviour in School-aged Children (HBSC) study is carried out in collaboration with WHO/EURO. The international coordinator of the 2001/02, 2005/05, 2009/10, and 2013/14 surveys was Professor Candace Currie at the University of St. Andrews, Scotland, and the data bank manager was Professor Oddrun Samdal at the University of Bergen, Norway. For details of participating countries, see ![]() . In Denmark, data were collected by the Danish HBSC steering committee, National Institute of Public Health, SDU. Pernille Due was Principal Investigator for the data collection from 1998 to 2010, Mette Rasmussen in 2014 and 2018, and Katrine Rich Madsen in 2022. In Greenland, data were collected by HBSC Greenland, Center for Health Research in Greenland, University of Greenland. In Sweden, the data were collected by HBSC Sweden at the Public Health Agency of Sweden, and Statistics Sweden (SCB). Ulla Marklund was PI for the data collection from 1998 to 2006, Lilly Augustin in 2010 to 2014, and Petra Löfstedt in 2018 to 2022.
. In Denmark, data were collected by the Danish HBSC steering committee, National Institute of Public Health, SDU. Pernille Due was Principal Investigator for the data collection from 1998 to 2010, Mette Rasmussen in 2014 and 2018, and Katrine Rich Madsen in 2022. In Greenland, data were collected by HBSC Greenland, Center for Health Research in Greenland, University of Greenland. In Sweden, the data were collected by HBSC Sweden at the Public Health Agency of Sweden, and Statistics Sweden (SCB). Ulla Marklund was PI for the data collection from 1998 to 2006, Lilly Augustin in 2010 to 2014, and Petra Löfstedt in 2018 to 2022.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was conducted within the research project “Positive mental health among adolescents in the Nordic countries,” funded by the Public Health Agency of Sweden (grant no. 0493-2020-2.3.2), and a research project “Mental health through the adolescents’ eyes: longer term trends in Nordic countries” funded by the Swedish Research Council for Health, Working Life and Welfare (FORTE; grant no. 2022-01087).