
Abstract
Background:
Prenatal ultrasound examinations are important to detect placental dysfunction. Several ultrasound-detected abnormalities can be managed during pregnancy or childbirth, thus improve health outcomes. Maternal birth country is known to influence the risk of placental dysfunction, but little is known about the possible mechanisms of this relation.
Aims:
(a) To estimate the proportion of non-registered prenatal ultrasound examinations; (b) to examine associations between non-registered ultrasound examinations and adverse perinatal outcomes, by migrant-related factors, in women giving birth in Norway.
Methods:
Individually linked data from the Medical Birth Registry of Norway and Statistics Norway, 1999–2016, comprising 999,760 singleton pregnancies to immigrants (n=196,220) and non-immigrants (n=803,540). Crude and adjusted odds ratios (aORs) with 95% confidence intervals (CIs) were estimated using logistic regression with robust standard error estimations, adjusted for year of childbirth, maternal age, parity, maternal smoking, educational level and Norwegian health region at birth.
Results:
Compared with non-immigrants, immigrant women had a higher proportion of non-registered ultrasound examinations (2.3% vs. 4.3%; aOR 2.0 (95% CI 1.9, 2.0)). Compared with women with ultrasound examination, the aOR for perinatal mortality for women with non-registered ultrasound was 2.27 (95% CI 1.85, 2.79) for immigrants and 3.61 (3.21, 4.07) for non-immigrants. Non-registered ultrasound examination was also associated with placental abruption (aOR 1.32 (1.08, 1.63)) for non-immigrant women, but it was not associated with preeclampsia.
Conclusions:
Tweetable abstract
Women without ultrasound examinations during pregnancy have an increased risk of perinatal mortality.
Keywords
Introduction
Prenatal ultrasound examinations play an important role of antenatal care to detect possible foetal abnormalities or placental dysfunction during pregnancy. The examination includes inspection of the number of foetuses, estimation of gestational age, assessment of foetal anatomy and development, as well as placental location and function. If diagnosed, several ultrasound-detected foetal and placental abnormalities can be managed during pregnancy or childbirth [1, 2], thus improving health outcomes, and even preventing perinatal mortality [3, 4].
Depending on the individual’s country of birth, previous studies show that immigrant women have an increased risk of placental dysfunction – for example, preeclampsia, placental abruption, preterm birth and stillbirth, compared with women in the receiving country [5–8]. Although factors such as country of birth and reason for immigration are known to influence the risk of placental dysfunction in immigrant women [8–11], little is known about the possible mechanisms of these relations. In this study, we hypothesise that the increased risk of adverse perinatal outcomes in immigrant women in part might be caused by undetected placental dysfunction due to unsatisfactory use of, for example, prenatal ultrasound examinations. We suggest that not attending an ultrasound during pregnancy could be a direct cause of undetected and untreated adverse placenta-related outcomes. Furthermore, as ultrasound examinations are performed by a midwife or an obstetrician, not attending the examination will reduce the possibility to secure adequate information on reasons for medical procedures in pregnancy follow-up, and potentially lead to poor understanding of medical recommendations for preventing other health-related outcomes in pregnancy.
To the best of our knowledge, few studies have investigated the role of prenatal ultrasound examinations in antenatal care for immigrant women. We thus aimed to: (a) estimate the proportion of non-registered prenatal ultrasound examinations; (b) examine associations between non-registered ultrasound examinations and adverse perinatal outcomes, by migrant-related factors, in women giving birth in Norway.
Materials and methods
Study design
This national population-based study was based on data from the Medical Birth Registry of Norway (MBRN) and Statistics Norway between 1999 and 2016. The MBRN comprises a mandatory, standardised notification of all live and stillbirths in Norway from 16 weeks of gestation since 1967 and from 12 weeks of gestation since 2001. The notifications are based on the information registered by midwives and medical doctors on a standardised antenatal care form during pregnancy. Data contain information on maternal and infant health during pregnancy and childbirth [12]. Statistics Norway collects, processes and disseminates official statistics about all individuals who are or have been Norwegian residents [13]. Linkage of data between the MBRN and Statistics Norway was possible through the national identity number assigned to all residents in Norway.
Perinatal outcomes
The perinatal outcome variables investigated in this study were: (a) perinatal mortality; (b) placental abruption; and (c) pre-eclampsia. The diagnoses were all recorded by a check box or in open text on the standardised MBRN notification form.
Perinatal mortality was based on the definition of the World Health Organization [14], and we defined foetal mortality as intrauterine foetal death from 22 completed weeks of gestation to death of a live-born infant before seven completed days post-partum [14, 15].
Placental abruption is defined as a detachment of the placenta before delivery [16]. In this study, the diagnosis was based on coding according to the International Statistical Classification of Disease and Related Health Problems, 10th revision (ICD-10): O45, including both partial and complete detachment of the placenta before childbirth.
Pre-eclampsia was based on coding according to the ICD-10: O14 – that is, an increase in blood pressure (⩾140/90 mmHg) combined with proteinuria (⩾300 mg in a 24 h urine collection) after 20 weeks of gestation.
Prenatal ultrasound examination
Since 1986, prenatal ultrasound examination has been provided free of charge in the second trimester (to estimate gestational age, inspect the number of foetuses, assess foetal anatomy and development, as well as placental location and function), and on a medical indication at any time during pregnancy, to all pregnant women resident in Norway [17]. Prenatal ultrasound examination has been registered in the MBRN since 1999. It is registered in free text on a standardised form used for ultrasound examinations and, furthermore, is checked in a check box on the standardised antenatal form by the midwife or obstetrician performing the examination. In this study, registration of the examination in pregnancy included prenatal ultrasound examination irrespective of indication and gestational age. Women were classified as having performed prenatal ultrasound examinations if the following information was registered on their antenatal form: (a) ultrasound and gestation determination; (b) ultrasound other reason; (c) embryo transfer; (d) ultrasound unspecified reason; (e) other. Non-registered perinatal ultrasound examinations included no registration in the above-mentioned categories, or if notification in one of the following categories was registered: (f) Naegele’s rule (expected date of delivery by last menstrual period); (g) ultrasound is not performed.
Migration-related factors
The prevalence of non-registered ultrasound was examined by maternal country of birth, reasons for immigration and length of residence.
Maternal country of birth was categorised and analysed according to the seven super regions defined by the Global Burden of Disease (GBD) study: (a) Central Europe, Eastern Europe and Central Asia; (b) high income; (c) Latin America and Caribbean; (d) North Africa and Middle East; (e) South Asia; (f) Southeast Asia, East Asia and Oceania; (g) sub-Saharan Africa. The high-income region comprised women from the following regions: Southern Latin America, Western Europe, North America, Australasia and high-income Asia Pacific [18].
In brief, foreign nationals must apply to the Norwegian Directorate of Immigration for residence in Norway. The reason for immigration is recorded if a positive decision for residence is obtained and may, or may not, be in accordance with the original and personal reason for immigration [19]. We used the variable derived by Statistics Norway comprising education; family reunion/establishment; refugee; work; unspecified/other [20]. Women from the Nordic countries (i.e. Sweden, Denmark, Finland and Iceland) may move freely and without application across the Nordic countries [19], and were included as a separate category (Nordic immigrants).
Statistics Norway also provided data on the maternal level of education (no education, primary school, secondary school, university/college), and year of maternal official residence permit in Norway. Based on the above-mentioned data, we calculated the length of residence (<1 year, 1–4 years, ⩾5 years) as the difference between year of childbirth and the year of maternal official residence permit in Norway.
Other variables
The MBRN further provided information on maternal age at birth (years), parity (0, 1, 2, 3, ⩾4 previous births), maternal smoking in pregnancy (yes, no), year of childbirth and Norwegian health region at childbirth (south/east, west, mid-Norway, north).
Study population
We analysed singleton pregnancies of immigrant (foreign-born women with two foreign-born parents) and non-immigrant women (Norwegian-born women with at least one Norwegian-born parent) between 1999 and 2016. Data were restricted to pregnancies from 22 completed weeks of gestation, which is considered the viable age of a foetus [14]. Exclusions were made for multifoetal pregnancies, missing data on maternal country of birth, Norwegian-born women with foreign-born parents (i.e. second-generation immigrants), and foreign-born women with Norwegian-born parent(s) (Figure 1).
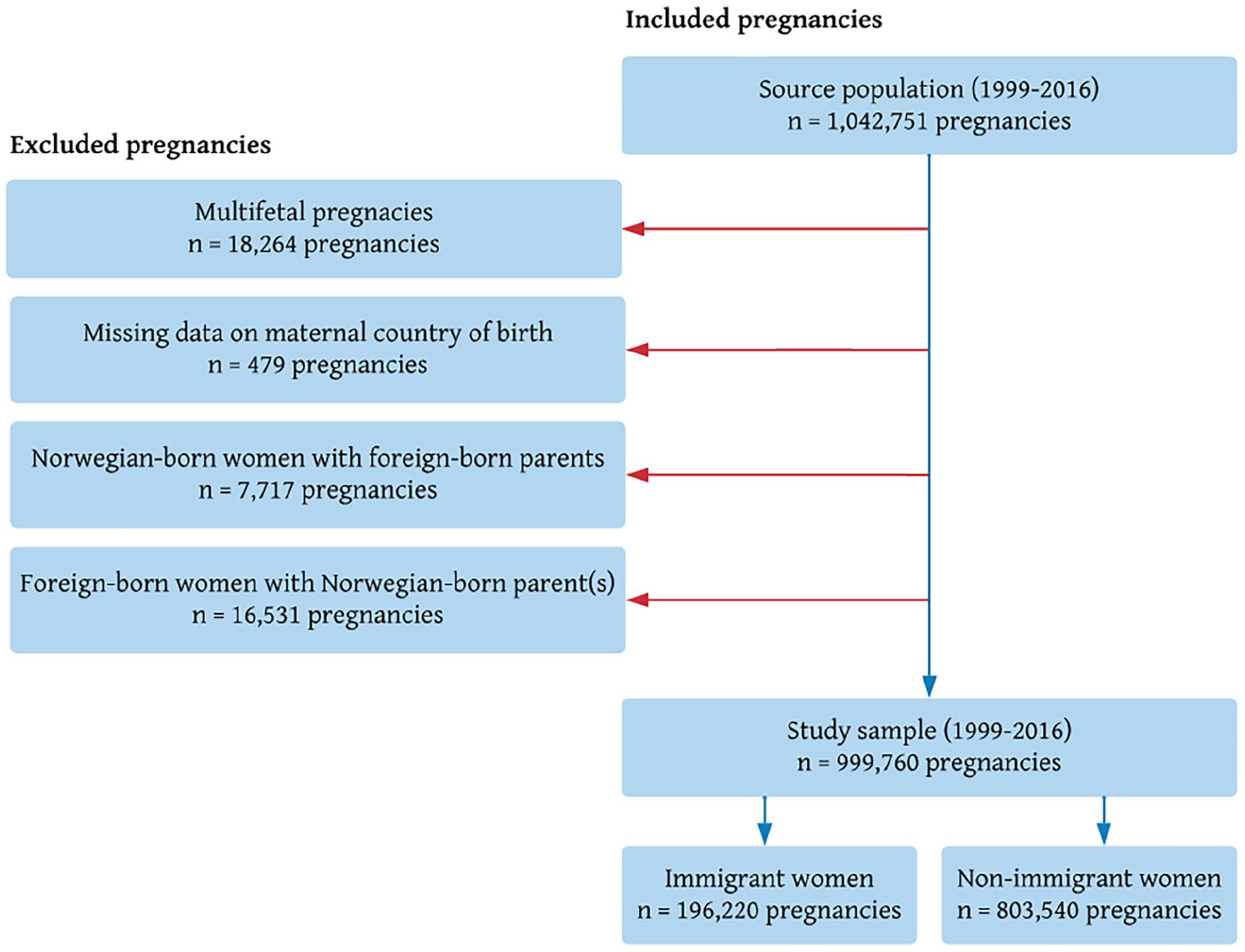
Derivation of the study sample, Norway, 1999–2016.
Statistical analyses
To investigate possible associations between migrant-related factors and non-registered ultrasound examinations in pregnancy, crude and adjusted odds ratios (aORs) with 95% confidence intervals (CIs) were estimated using logistic regression with robust standard error estimations to account for within-mother clustering. We investigated prenatal ultrasound examinations by maternal GBD region of birth (seven super regions), reason for immigration and length of residence using non-immigrant women as reference.
To investigate possible associations of non-registered ultrasound examinations with perinatal mortality, placental abruption and pre-eclampsia (Figure 2), we estimated crude and aORs with 95% CIs using women with registered ultrasound examinations as reference. The analyses were stratified by immigrant and non-immigrant women overall. Due to small numbers, analyses for maternal region of birth, reason for immigration and length of residence were not performed.
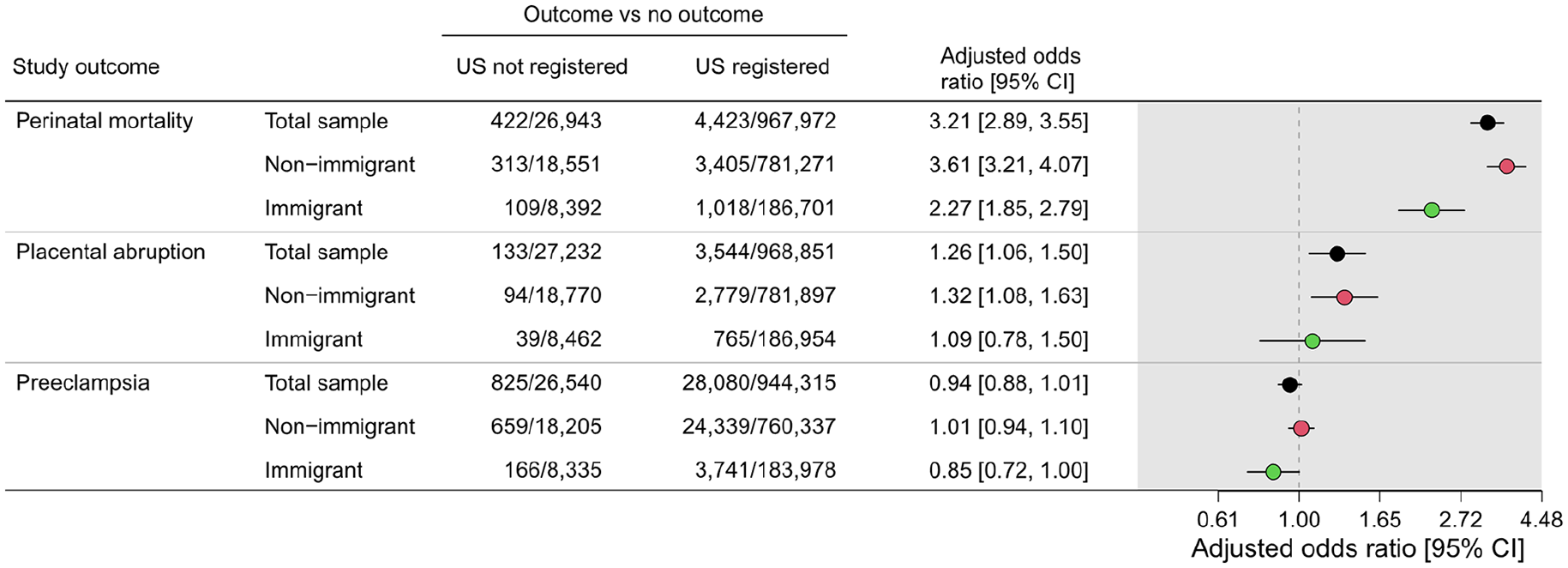
Adjusted odds ratios with 95% confidence intervals for perinatal mortality, placental abruption and pre-eclampsia in immigrant and non-immigrant women with non-registered data on prenatal ultrasound examinations in pregnancy, Norway, 1999–2016. Adjusted for year of childbirth, maternal age, parity, maternal smoking during pregnancy, educational level and Norwegian health region at birth. Registered ultrasound examination was used as the reference category. CI: confidence interval; US: ultrasound examination.
In all analyses, adjustments were made for year of childbirth, maternal age, parity, maternal smoking during pregnancy, educational level and Norwegian health region at birth for all analyses. Because some of these risk factors may act as mediators on the causal pathway for the associations between maternal region of birth and non-registered ultrasound examinations, the estimated aORs for these analyses should be interpreted as controlled direct effects rather than total effects [21].
Variables containing missing values were imputed using the multivariate normal model with five imputations [22]. The imputations were performed separately for each exposure–outcome analysis and comprised the same variables as in the analytical regression models. Rubin’s combination rules, adjusted for the variability between imputation sets, were used to obtain pooled odds ratios with 95% CIs across the five imputed datasets.
Analyses were performed using Stata IC version 16 (Stata Statistical Software, College Station, TX, USA).
Ethical approval
This study was approved on 1 August 2014 by the South-East Regional Committees for Medical and Health Research Ethics in Norway, reference number: 2014/1278/REK South-East Norway. Data were used under licence for this study.
Results
The total source population from the MBRN (1999–2016) contained data from 1,042,751 pregnancies from 22 completed weeks of gestation (Figure 1). Of these, we analysed 999,760 singleton pregnancies, of which 20% (n=196,220) were to immigrant women (foreign-born women with two foreign-born parents) and 80% (n=803,540) were to non-immigrant women (Norwegian-born women with Norwegian-born parent(s)). We excluded multifoetal pregnancies (n=18,264), pregnancies with missing data on maternal country of birth (n=479), pregnancies to Norwegian-born women with two foreign-born parents (n=7717), and pregnancies to foreign-born women with Norwegian-born parents (n=16,531) (Figure 1).
Table I shows background characteristics by maternal region of birth (as defined by the GBD study) for immigrant and non-immigrant women. The proportion of non-registered prenatal ultrasound examinations was lowest in non-immigrant women (2.3%), and highest in immigrant women from the sub-Saharan region (5.8%). Perinatal mortality was lowest in immigrant women from Latin America and the Caribbean (0.40%), and highest in immigrant women from South Asia (0.94%) (Table I).
Sample characteristics by maternal region of birth, Norway, 1999–2016.
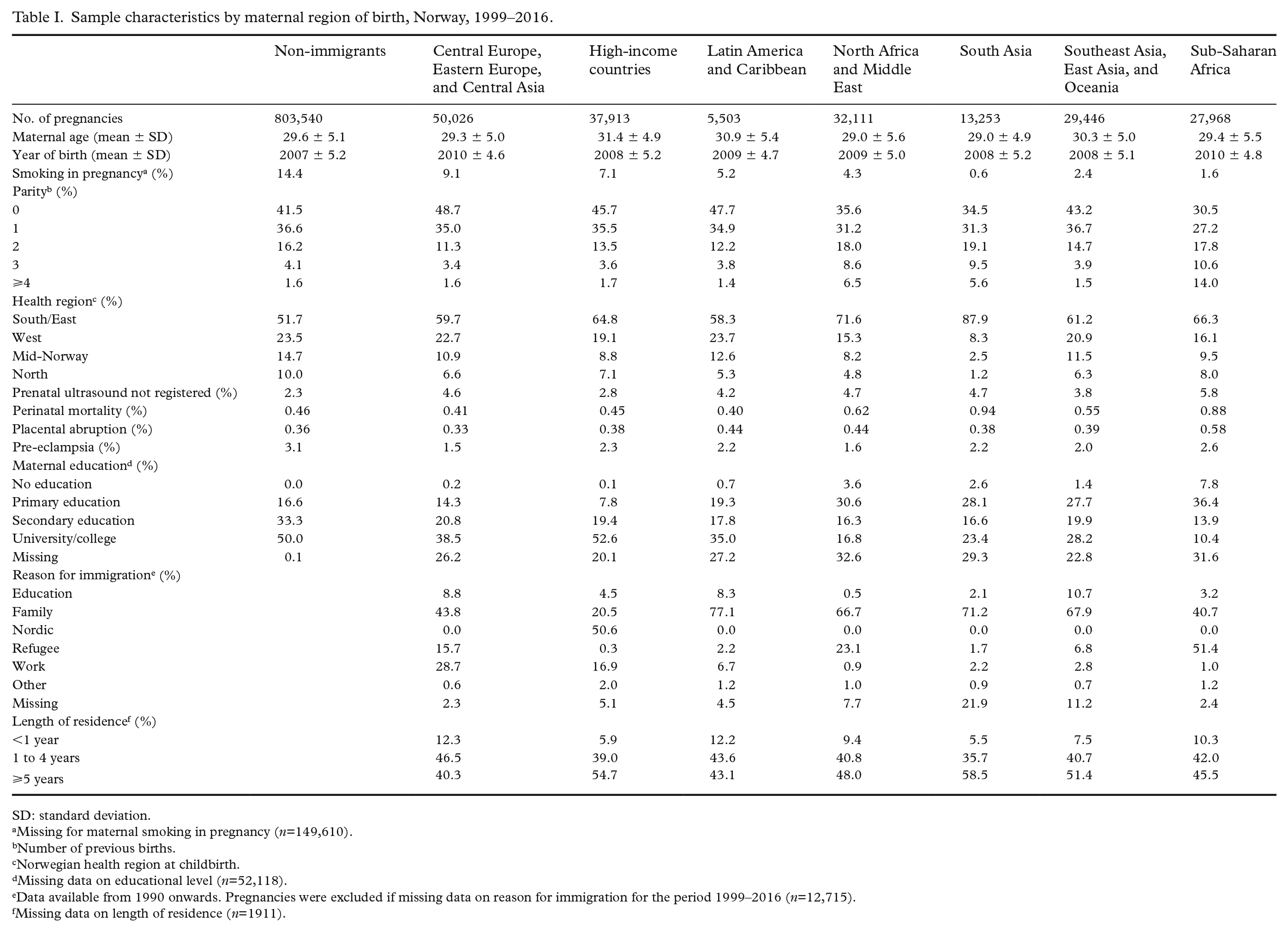
SD: standard deviation.
Missing for maternal smoking in pregnancy (n=149,610).
Number of previous births.
Norwegian health region at childbirth.
Missing data on educational level (n=52,118).
Data available from 1990 onwards. Pregnancies were excluded if missing data on reason for immigration for the period 1999–2016 (n=12,715).
Missing data on length of residence (n=1911).
Table II shows crude and aORs for non-registered prenatal ultrasound examinations in immigrant women, using non-immigrant women as reference. Compared with non-immigrants, women born in the sub-Saharan GBD region (2.3.% vs. 5.8%; aOR 2.7 (95% CI 2.6, 2.9]), refugees (2.3% vs. 5.5%; aOR 2.6 (2.4, 2.7)), and women with less than one year of residence in Norway (2.3% vs. 12.5%; aOR 6.3 (6.0, 6.6)) had the highest aORs of non-registered ultrasound in pregnancy.
Odds ratios with 95% confidence intervals for pregnancies with non-registered ultrasound examinations in pregnancy, by maternal region of birth, reason for immigration and length of residence, Norway, 1999–2016.
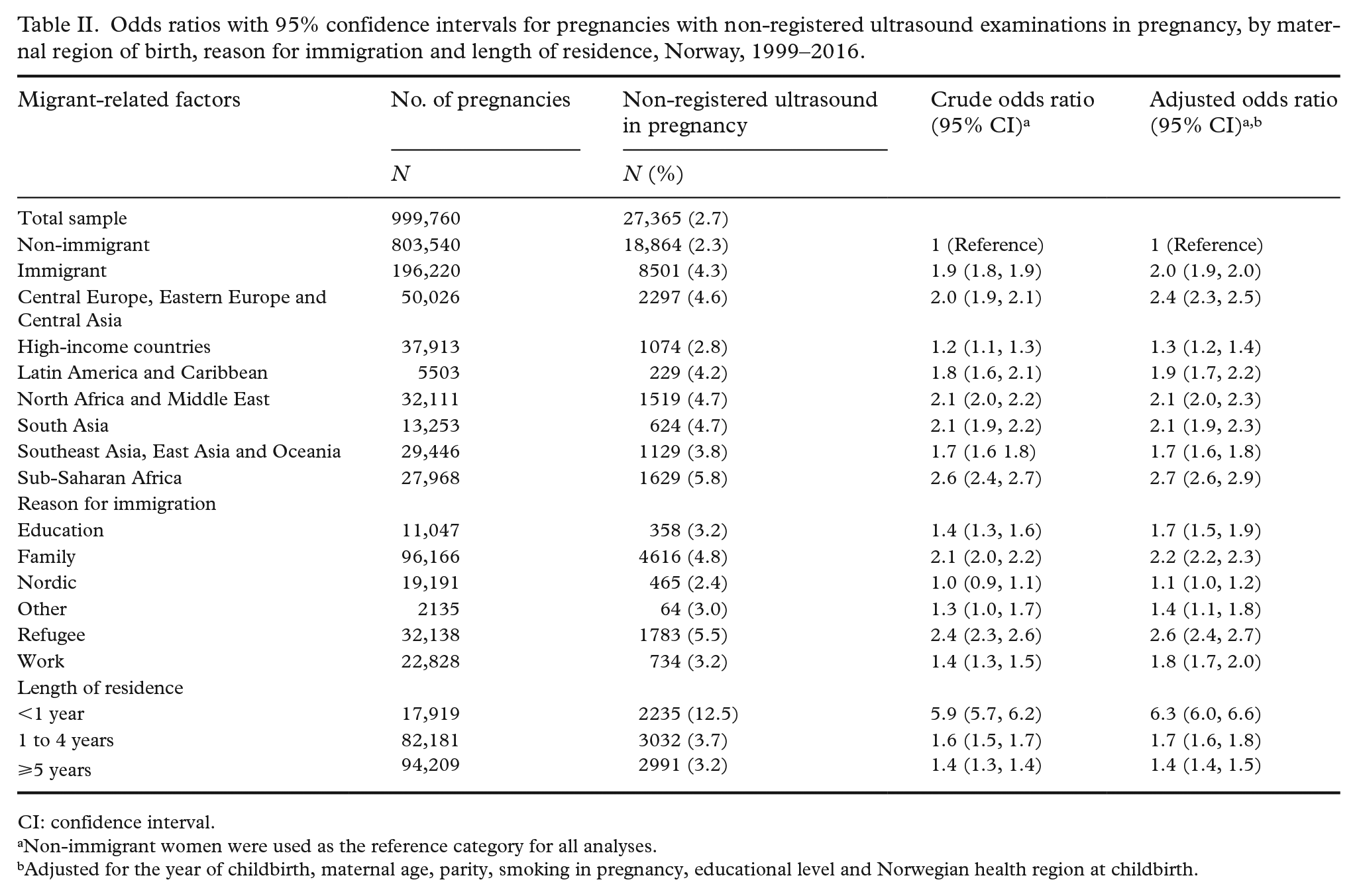
CI: confidence interval.
Non-immigrant women were used as the reference category for all analyses.
Adjusted for the year of childbirth, maternal age, parity, smoking in pregnancy, educational level and Norwegian health region at childbirth.
Non-registered data on prenatal ultrasound and perinatal mortality
Figure 2 shows aORs for adverse perinatal mortality for women with non-registered ultrasound examinations, compared with women with registered ultrasound examinations in pregnancy. Compared with women with ultrasound examinations registered in pregnancy, the aOR for perinatal mortality for women without ultrasound examinations registered was 2.27 (1.85, 2.79) in immigrant and 3.61 (3.21, 4.07) in non-immigrant women.
We found a slightly increased aOR for placental abruption for those without ultrasound examinations in the overall study sample and in non-immigrant women (aOR 1.26 (1.06, 1.50) and 1.32 (1.08, 1.63), respectively), but not in immigrant women (aOR 1.09 (0.78, 1.50)). Women without ultrasound examinations registered in pregnancy were not associated with pre-eclampsia in either the total study sample, non-immigrant or immigrant women (Figure 2).
Discussion
This study showed that the proportion of non-registered ultrasounds in pregnancy was higher for immigrant women from all GBD regions, compared with non-immigrant women. Compared with women with ultrasound registered during pregnancy, we found an increased odds for perinatal mortality in both immigrant and non-immigrant women with non-registered ultrasound examinations in pregnancy. We found a slightly increased risk of placental abruption in non-immigrant women with non-registered ultrasound examinations, but no association was observed for pre-eclampsia in either immigrant or non-immigrant women.
Proportions of ultrasound in pregnancy
Consistent with previous research [6, 23], we found that immigrant women more often had non-registered data on prenatal ultrasound examinations than non-immigrants, especially immigrant women born in sub-Saharan African countries (Table I). In addition, we found a higher proportion of non-registered ultrasound examinations in refugees and immigrant women with less than one year of residence in Norway, compared with non-immigrants. Immigrant women overall have expressed low awareness of the usage of healthcare facilities [24]. They also report difficulties navigating the health system to obtain accurate information during pregnancy [23, 25]. Prenatal ultrasound examinations may be used as a proxy for the use of maternity care services during pregnancy. Challenges navigating the healthcare system have been described as one of the most important reasons for an unsatisfactory utilisation of maternity care services [23]. Our findings of a high proportion of non-registered ultrasound examinations in refugees and recently immigrated women could be due to immigration late in pregnancy (i.e. already pregnant when immigrating). However, general low attendance at postpartum follow-up [6], and the overall health-seeking behaviour in sexual and reproductive health for refugees [26] could indicate an unsatisfactory utilisation of prenatal healthcare services overall, including the attendance at ultrasound examinations.
Not attending ultrasound examinations as part of prenatal healthcare has also been reported as a conscious choice for subgroups of immigrant women [27]. Social and religious beliefs [28], uncertainty about foetal safety during an examination [29], and limited knowledge of the benefits of the examinations have been reported as arguments for not attending the examination [27].
Together with language barriers [25, 30], the above-mentioned factors might be great impediments to attending prenatal ultrasound examinations. We did not investigate the reasons for non-registered examinations in our study. However, if previously reported views on ultrasound examinations [27–29] reflect those of our study population, it could in part explain the differences in ultrasound proportion between immigrants and non-immigrants.
Perinatal outcomes
We found a strong association between non-registered ultrasound examinations and perinatal mortality in both immigrant and non-immigrant women (Figure 2). We also found that it might influence the risk of placental abruption in non-immigrants, but no association was found with pre-eclampsia for either immigrants or non-immigrants. The inconsistent findings across these outcomes may partly be ascribed to the intended function of performing the ultrasound examination. In Norway, the examination is primarily performed to assess foetal anatomy and development, as well as placental location and function, and to estimate gestational age [17]. These are factors that may play a direct role in perinatal mortality and placental abruption but have little or no importance to predict the development of pre-eclampsia during pregnancy.
In stratified analyses, we also found a stronger association with perinatal mortality for non-immigrants than for immigrants. The stronger association for non-immigrants could in part be attributed to residual confounding in which immigrants and non-immigrant are different in both type and strength of confounding factors. In addition, the observed difference could be ascribed to a differential selection, in that reasons for not attending an ultrasound examination might be different for immigrants and non-immigrants. Therefore, a direct comparison of associations across strata of immigrants and non-immigrants is challenging, and we cannot draw a firm conclusion about whether non-registration of ultrasound examinations has more severe consequences in non-immigrants than in immigrants.
Due to small numbers, we analysed perinatal mortality, placental abruption and pre-eclampsia in immigrant women overall. This is a broad categorisation of heterogenous groups, potentially masking a great deal of variation in immigrant subgroups. However, several of the countries represented in this study are classified as long-time conflict zones. Women migrating from conflict zones have been associated with an increased risk of perinatal mortality [6]. One can only speculate if the increased odds of perinatal mortality in immigrant women in the study sample could in part be attributed to the consequences of previous stressful situations in addition to resettlement in a new country.
Strength and limitations
To our knowledge, this is the first study to investigate the association of adverse perinatal outcomes in women with non-registered ultrasound by migration-related factors. The main strengths of this study include the standardised data collection for both immigrant and non-immigrant women, and the large national population-based sample size that enabled investigations of rare outcomes.
The MBRN does not contain information on the number of antenatal care visits during the perinatal period, information on the use of interpreters during visits, or reasons for non-registered data on ultrasound examinations. Access to this information would have provided deeper knowledge of the utilisation of antenatal care services during all stages of pregnancy. In addition, as there are currently no validation studies on prenatal ultrasound examination, misclassifications cannot be excluded.
Conclusions
Immigrant women from all GBD regions had a higher proportion of non-registered ultrasound during pregnancy, compared with non-immigrant women. Women without ultrasound registered in pregnancy were associated with an increased odds of perinatal mortality in both non-immigrant and immigrant women.
Clinical implications
Adequate use of antenatal care services might increase the possibilities of detecting risk factors for adverse perinatal outcomes that might be preventable or treated. It is not possible to confirm nor to refute that undergoing a prenatal ultrasound would reduce the odds of perinatal mortality for all pregnancies, but it might serve as a proxy for lower utilisation of maternity care in general. The increased risk of perinatal mortality for women without ultrasound registration thus highlights the significance of the services. Maternity care providers should therefore aim to complete comprehensive and accurate obstetric history taking and secure intelligible information on, for example, medical procedures and follow-up, for all women during pregnancy, with a special focus on vulnerable women, to strive to increase adequate use of the services. The services should further strive to offer a culturally sensitive and responsive approach with intent to tailor services and information on the use and importance of prenatal healthcare services, including ultrasound examinations, to all women regardless of maternal country of birth. Such an approach might create a cultural bridge between immigrant women and the healthcare system in the receiving country and optimise use of the services and the quality of care provided during pregnancy and childbirth.
Footnotes
Author contributions
KSM, NHM, ES, VA and RMN contributed to the conception and design of the study. Formal analyses were performed by KSM. The first draft of the manuscript was written by KSM. All authors read and approved the final manuscript.
Availability of data and materials
The datasets used in the current study are not publicly available due to regulatory conditions concerning data usage and storage. Data might be available from the corresponding author on request and with permission from the Medical Birth Registry of Norway and Statistics Norway.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The faculty of Health and Social Sciences (Western Norway University of Applied Sciences, Norway) was the main funder for this study. Additional data costs were funded by the Norwegian SIDS and Stillbirth Society. None of the funders had any role in the study design, data collection, analysis, decision to publish, or preparation of the manuscript.
Ethics approval
This observational study was performed in accordance with the Declaration of Helsinki and was approved by the South-East Regional Committees for Medical and Health Research Ethics in Norway, reference number: 2014/1278/REK South-East Norway. The data do not contain personally identifiable information and the approval includes the use of individual record linked data from the national health registry the Medical Birth Registry of Norway and Statistics Norway.