
Abstract
Background:
Intimate partner violence against pregnant women is an important public health concern and human rights issue. According to the various findings of previous studies, this study was conducted to assess the pooled prevalence of intimate partner violence against Iranian women.
Methods:
In this systematic review and meta-analysis, a literature search was conducted in databases such as PubMed, Scopus, Web of Science, MagIran, and Scientific Information Database without a time limit. Heterogeneity was assessed by Cochrane Q test statistics and the I2 test, and the results were incorporated into a random effects model to estimate the prevalence of intimate partner violence. Data analysis was performed using R software version 4.3.2.
Results:
The overall prevalence of intimate partner violence was reported to be 51.5% (95% confidence interval (CI) 45.0–58.1), and the prevalence rate of physical, sexual, and psychological intimate partner violence was 18.0% (95% CI 15.1–20.9), 22.1% (95% CI 17.7–26.60) and 43.2% (95% CI 36.6–49.8), respectively. The lowest level of physical, sexual, and emotional intimate partner violence rate was observed in district 1 of Iran (includes Tehran, the capital of Iran and the surrounding provinces). The rate of physical and sexual intimate partner violence prevalence decreased with the increased mean age of the husband (P=0.005) and the mean age of the wife (P=0.035), respectively.
Conclusions:
Introduction
Violence against women is defined as physical, sexual and emotional abuse as a means used by men to control and dominate the female partner or other family members [1]. Violence against women is a widespread and devastating human rights violence [2], as well as a serious social, legal and health problem, associated with social, psychological and economic consequences. Furthermore, it strongly affects the quality of life and dignity of humans [3, 4]. Violence against women has been recognised as a major concern since the 1980s onwards when local and international groups of women were organised to draw public attention to the issue. In the early 1990s, comprehensive laws were enacted specifically to combat gender-based violence [5].
While violence against women may occur before, during and after pregnancy, women are more vulnerable during pregnancy due to emotional, social and physical changes in this period [6]. Several studies have shown that intimate partner violence (IPV) during pregnancy increases the risk of miscarriage, premature labour, low birth weight and neonatal birth [7–9], thereby leading to depression during and after pregnancy, posttraumatic stress syndrome and even suicide [10–12]. As IPV is a largely hidden crime, it mostly goes unreported due to cultural status, economic barriers, fear of losing children, distrust of the healthcare system and insufficient knowledge [13].
Worldwide, one-third of women experience IPV in their lifetime, with significant regional diversity, with the lowest rates in East Asia, western Europe, and North America, and the highest rates in central sub-Saharan Africa [14]. In the meta-analysis of Bazyar et al. (2018), reviewing articles published up to 2015, only the prevalence of sexual violence against pregnant women was examined [15]. In the meta-analysis of Karimi et al. (2016), the prevalence of emotional and physical violence against pregnant women was estimated [16]. The studies in Iran have yielded different findings, with the prevalence of IPV reported to vary from 10.7% to 88% [17, 18].
While observational studies conducted in Iran report violence in general, sexual, physical and emotional. Therefore, in order to provide a clear picture of violence against pregnant women, it is necessary to pay attention to all these types of violence, and to estimate the pooled prevalence, all these studies should be analysed. Health decisions are made based on the findings of these studies, and the more comprehensive, complete and valid these studies are, the more effective decisions can be made based on them. The present study aimed to evaluate the cumulative prevalence and outcomes of IPV against Iranian pregnant women.
Methods
The study has been registered in the international prospective register of systematic reviews (PROSPERO) as number CRD42021249587. This study was a systematic review and meta-analysis of published studies, so it was not necessary to obtain ethics approval or informed consent.
Search strategy
This systematic review and meta-analysis was performed based on the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). A literature search was conducted in the international databases of Scopus, PubMed and Web of Science, as well as the national databases of MagIran and Scientific Information Database (SID) without time limit using various keywords, including intimate partner violence, domestic violence, family violence, spousal assault, battered women, partner assault, spousal abuse, wife abuse, partner abuse, femicide, domestic homicide, wife assault, pregnancy, gestation, Iran, and all the possible combinations (Supplemental Table I). Our search was from the inception to January 2021. During this period, these articles were found, the most recent of which was related to 2020. For access to more articles, the references of the selected papers were also reviewed.
Selection of studies and data extraction
The observational studies investigating the frequency or prevalence of IPV against women during pregnancy were reviewed. Some studies reported the overall prevalence rate, while the others reported the prevalence rate of violence in different dimensions (sexual, physical, psychological and financial). Interventional studies, review studies, qualitative studies, letters to the editor, duplicate studies, irrelevant studies and those with an unavailable full text were excluded from the review. The literature search and article review were performed by two authors independently, and lack of consensus was resolved by a neutral third party. At this stage, the required data were extracted from the selected articles and recorded in a pre-designed file, including data on the name of the corresponding author, year of publication, sample size, mean age of wife/husband, mean gestational age, study setting and prevalence of violence (general, physical, sexual, financial and psychological).
Quality assessment
In addition, the methodological quality of the studies was assessed based on 10 items selected from the STROBE checklist, which were the title and abstract, objectives and hypotheses, research setting, inclusion criteria, sample size, statistical methods, descriptive data, interpretation of the findings, research limitations and funding [19]. Each article was scored one or zero in the case of finding and not finding each item, respectively. Accordingly, the articles were divided into three categories of low quality (0–5), moderate quality (6–8) and high quality (9–10).
Statistical analyses
In the meta-analysis, the variance of each study was calculated based on binomial distribution, and a weighted mean was used to combine different studies; corresponding weight was considered as the inverse variance of each study. Moreover, the heterogeneity of the selected studies was assessed by Cochrane Q test statistics and the I2 test, considering I2 greater than 50% and P-0.1 Cochrane-Q less than 0.01 as significant heterogeneity. According to I2, heterogeneities were divided into three categories of less than 25% (low heterogeneity), 25–75% (moderate heterogeneity) and greater than 75% (high heterogeneity). In the case of significant heterogeneity in all the models, a random effects model would be applied to combine the studies and estimate the cumulative prevalence of IPV. In addition, the frequency of the total score of IPV and its dimensions were evaluated based on scale, region and language using subgroup analysis. In 2014, the provinces of Iran were divided into five regions according to the factors of proximity, geographical location and commonalities. Region 1 includes Tehran (the capital of Iran and surrounding provinces), which is in a better position than other regions in terms of facilities and facilities. Regions 2 and 5 have several large and industrial provinces, and regions 3 and 4 include the provinces located in the northwest, west and southwest.
Sensitivity analysis was carried out using the leave-one-out method. A Funnel plot based on Egger’s regression was used to evaluate the potential effects of small studies and publication errors on the IPV prevalence rate. We also explored a univariate meta-regression to determine the correlations between IPV prevalence and variables such as the year of implementation, sample size, mean age of men and marital age. The odds ratios reported in the studies were also combined based on the heterogeneity level using the Mantel–Haenszel method (fixed/random) to measure adverse pregnancy outcomes. Data analysis was performed using R software version 4.3.2.
Results
The initial search yielded 461 potentially relevant studies, nine of which were repetitive. Then the titles and abstracts of the remaining 452 studies were reviewed and 385 studies were deleted due to irrelevance and the non-observational nature of the study. Then the full text of the remaining 67 studies was reviewed. Finally, 58 articles were selected for further analysis based on the inclusion and exclusion criteria. Figure 1 shows the detailed process of article screening and selection.
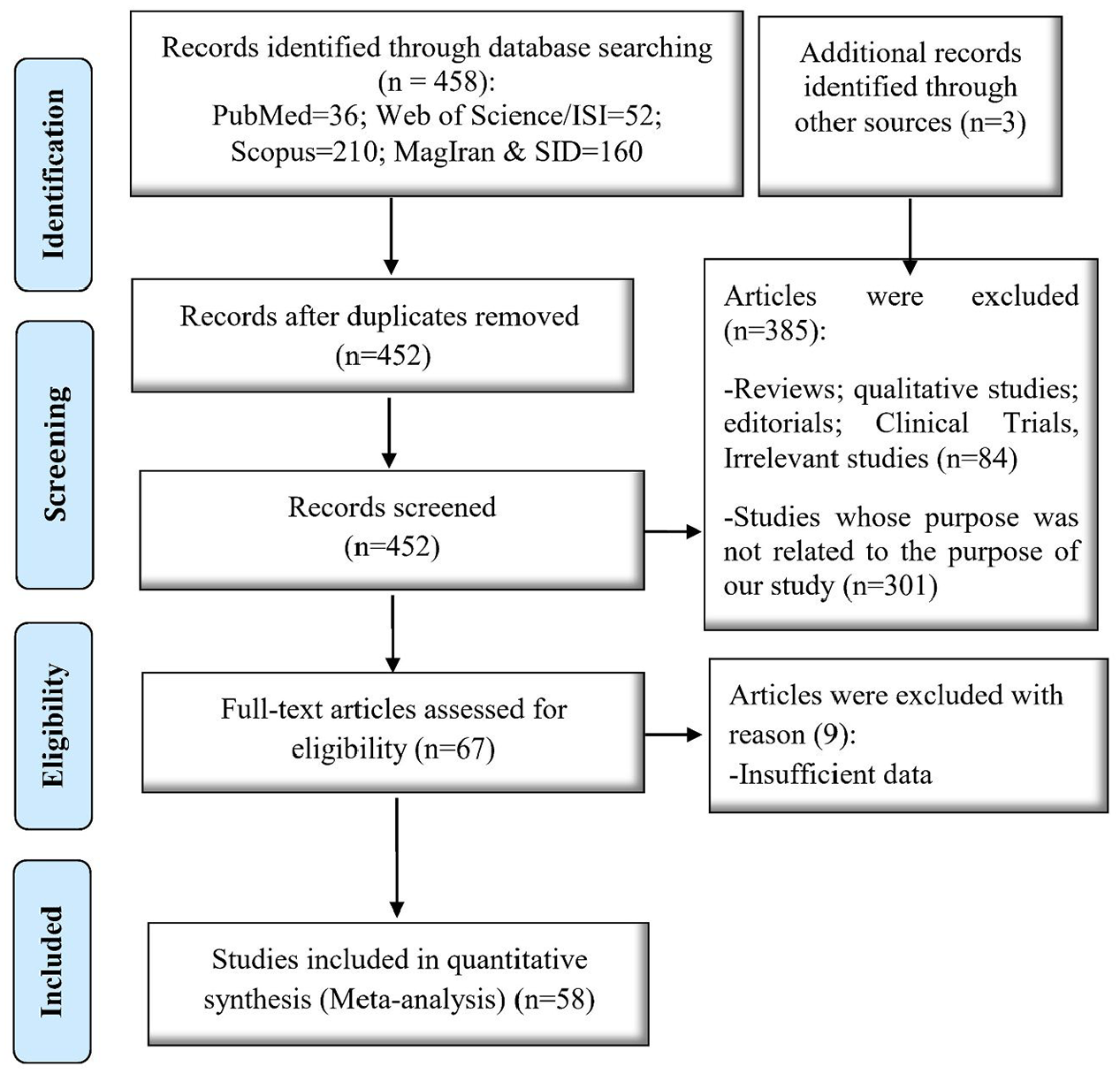
Flow diagram of the search and screening processes.
In the initial search, 461 articles were retrieved, of which nine were duplicate articles. Then the titles and abstracts of the remaining 452 articles were evaluated by two independent authors, 385 unrelated articles were deleted. Finally, the full text of the remaining 67 articles was reviewed. At this stage, nine studies were excluded due to not reporting the prevalence of violence. In total, 58 articles with a sample size of 36,438 were analysed. Based on the findings, most of these studies (n = 17) were performed in district 3 of Iran. Researcher-made questionnaires were used in 37 studies to assess the IPV prevalence rate. Furthermore, most of the studies were performed in the year 2017 (n = 6), and the largest and smallest sample sizes were in the studies conducted by Faramarzi et al. (n = 3275) [20] and Shakerinezhad (n=132), respectively [21]. In four studies, the samples were divided into two groups, and IPV frequency was measured in each group separately. In the studies by Ebrahimi et al. (2017) [22] and Kordi et al. (2013) [23], the samples were divided into two groups with and without pre-eclampsia. In a study by Mohammad-Alizadeh-Charandabi et al. (2016), the IPV prevalence rate was measured in two groups of adolescents and adults [24], while Baheri et al. (2012) [25] assessed this issue in two groups of favourable and unfavourable pregnancy outcomes. In selected studies, different scales (with different questions and different scores) were used to estimate the prevalence of IPV, but the final outcome was all the same, so the prevalence reported in each study was recorded as the final outcome. All selected articles had good methodological quality. Table I shows the features of the selected studies.
The characteristic of selected papers.
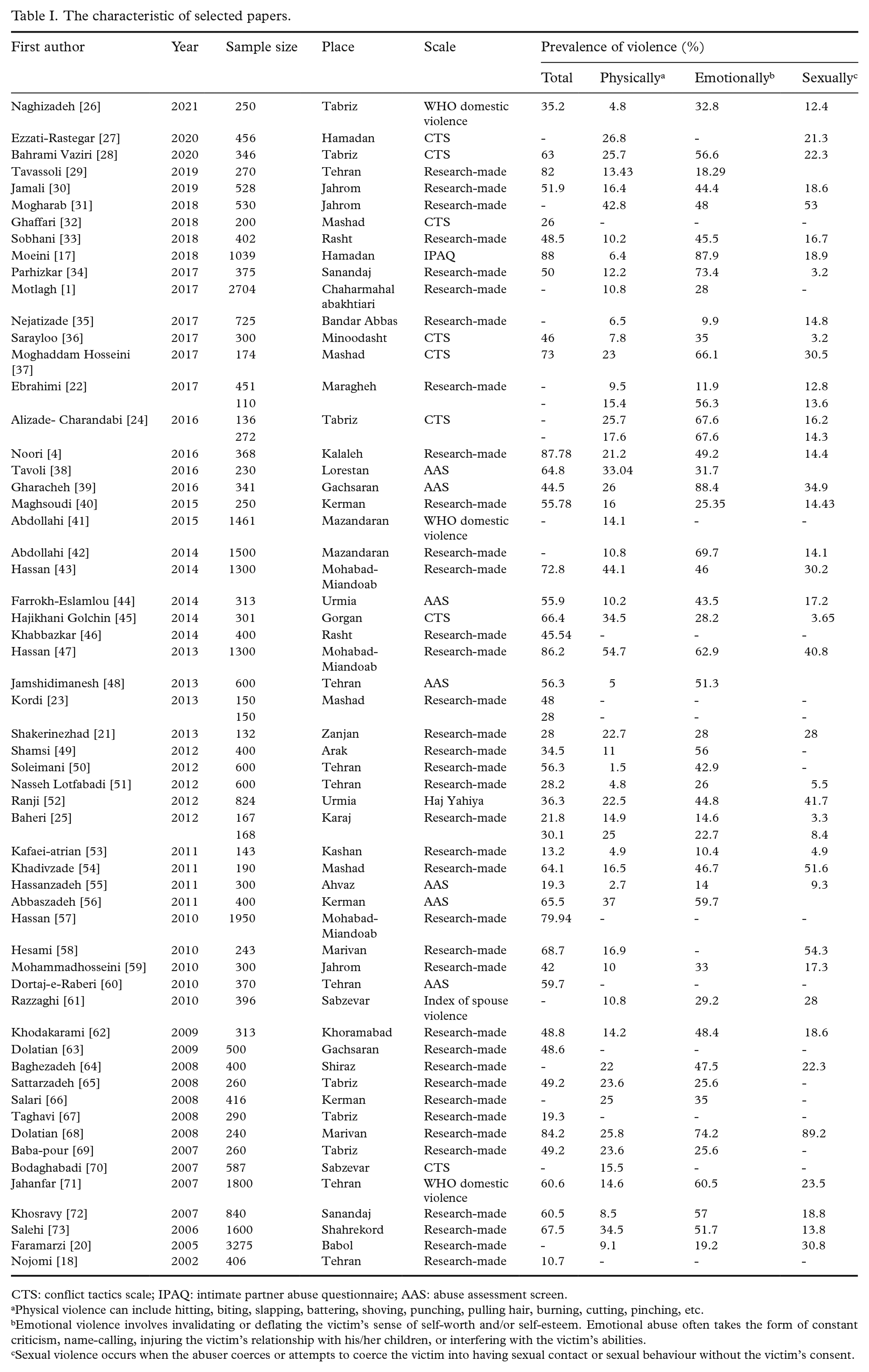
CTS: conflict tactics scale; IPAQ: intimate partner abuse questionnaire; AAS: abuse assessment screen.
Physical violence can include hitting, biting, slapping, battering, shoving, punching, pulling hair, burning, cutting, pinching, etc.
Emotional violence involves invalidating or deflating the victim’s sense of self-worth and/or self-esteem. Emotional abuse often takes the form of constant criticism, name-calling, injuring the victim’s relationship with his/her children, or interfering with the victim’s abilities.
Sexual violence occurs when the abuser coerces or attempts to coerce the victim into having sexual contact or sexual behaviour without the victim’s consent.
According to the results obtained, the total prevalence of IPV in pregnant women in Iran is 51.5% (95% confidence interval (CI) 45.0–58.1), and the highest and lowest IPV prevalence rates have been reported in district 3 (54.9%; 95% CI 44.8–65.1) and district 2 (44.7%; 95% CI 29.8–59.6). Moreover, the prevalence of physical, psychological and sexual violence has been reported to be 18.0% (95% CI 15.1–20.9), 43.2% (95% CI 36.6–49.8) and 22.1% (95% CI 17.7–26.60). In terms of the districts in Iran, district 1 accounts for the lowest IPV prevalence rate in the physical dimension (13.1%; 95% CI 9.7–16.3), psychological dimension (36.5%; 95% CI 23.6–49.4) and sexual dimension (11.9%; 95% CI 4.4–16.4). On the other hand, district 5 accounts for the highest IPV prevalence rate in the physical dimension (20.7%; 95% CI 13.4–28.1), psychological dimension (48.2%; 95% CI 39.1–57.3) and sexual dimension (30.9%; 95% CI 17.0–44.9). Regarding the data collection scales, the highest overall prevalence rate of IPV (54.9%; 95% CI 39.1–70.6) and the physical prevalence rate (20.0%; 95% CI 13.5–26.5) have been measured by the conflict tactics scale. On the other hand, the highest psychological IPV prevalence rate (48.1%; 95% CI 24.5–61.8) and sexual IPV prevalence rate (23.9%; 95% CI 17.5–30.3) have been measured by the abuse assessment screen. Furthermore, the overall, physical and psychological IPV prevalence rates were observed to be higher in English articles compared to the Farsi papers (Table II).
Subgroup analysis of the intimate partner violence by region, scale and language.
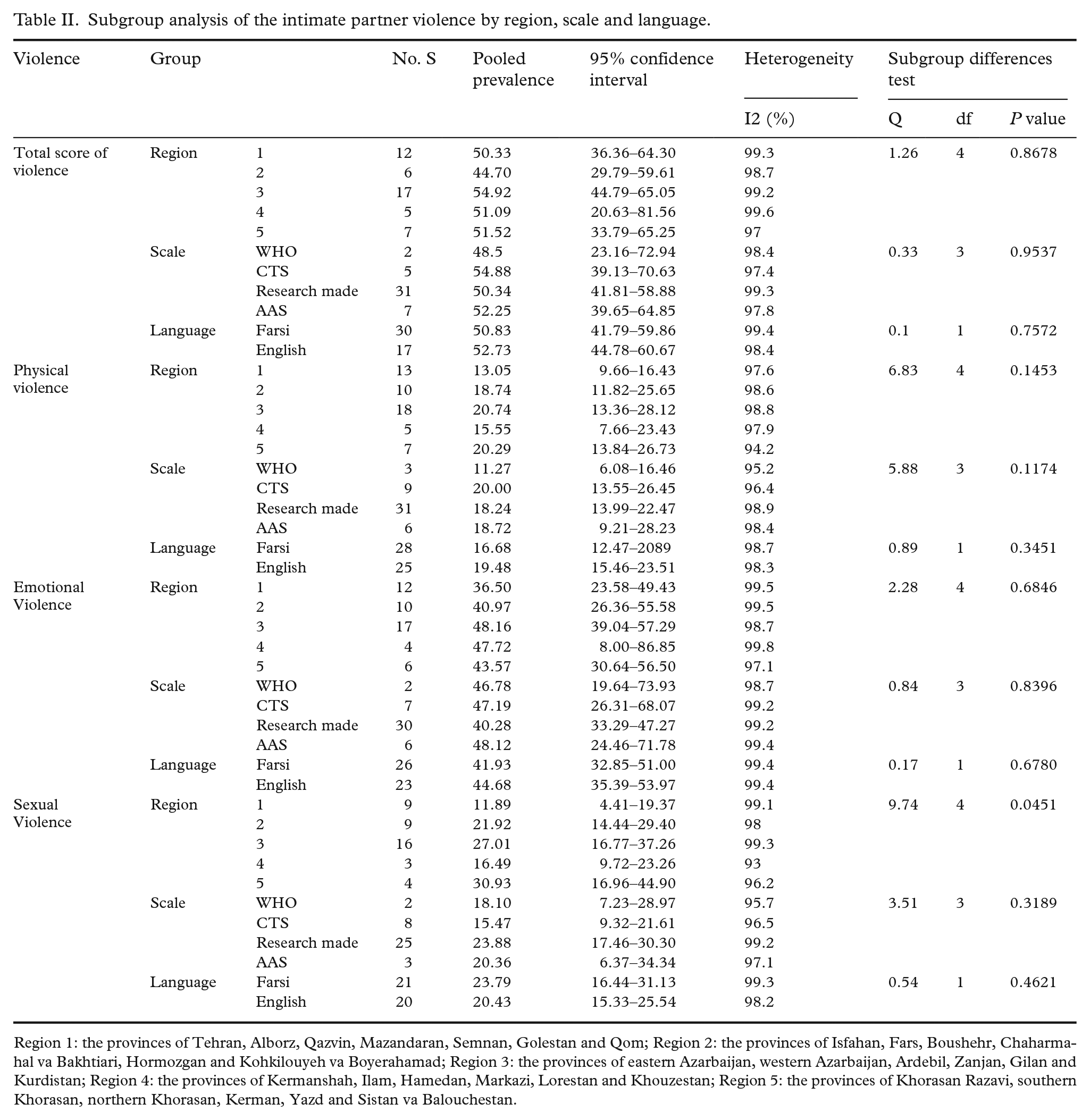
Region 1: the provinces of Tehran, Alborz, Qazvin, Mazandaran, Semnan, Golestan and Qom; Region 2: the provinces of Isfahan, Fars, Boushehr, Chaharmahal va Bakhtiari, Hormozgan and Kohkilouyeh va Boyerahamad; Region 3: the provinces of eastern Azarbaijan, western Azarbaijan, Ardebil, Zanjan, Gilan and Kurdistan; Region 4: the provinces of Kermanshah, Ilam, Hamedan, Markazi, Lorestan and Khouzestan; Region 5: the provinces of Khorasan Razavi, southern Khorasan, northern Khorasan, Kerman, Yazd and Sistan va Balouchestan.
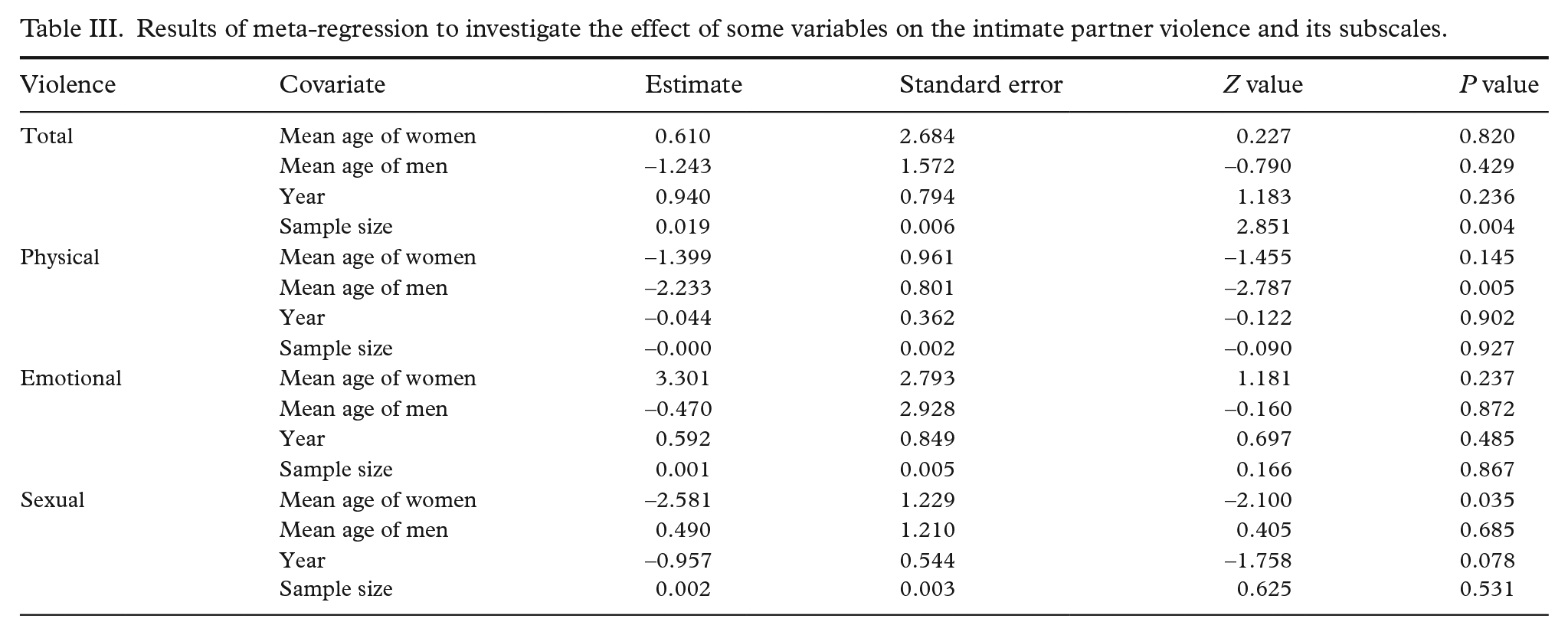
The meta-regression results indicated a correlation between physical IPV and the mean age of the husband (P = 0.0053) and between sexual IPV and the mean age of the wife (P = 0.035), and the increased age of the husband and wife was associated with a significant decrease in physical and sexual IPV, respectively. Moreover, a correlation was denoted between the overall IPV prevalence rate and the sample size (P = 0.004) (Table III).
Results of meta-regression to investigate the effect of some variables on the intimate partner violence and its subscales.
Our findings were also indicative of an association between the overall IPV scores and the increased adverse outcomes of pregnancy, such as the premature rupture of membranes (PROM), unwanted pregnancy, pre-eclampsia, miscarriage, caesarean section and vaginal bleeding (Table IV).
Adverse effect of pregnancy.
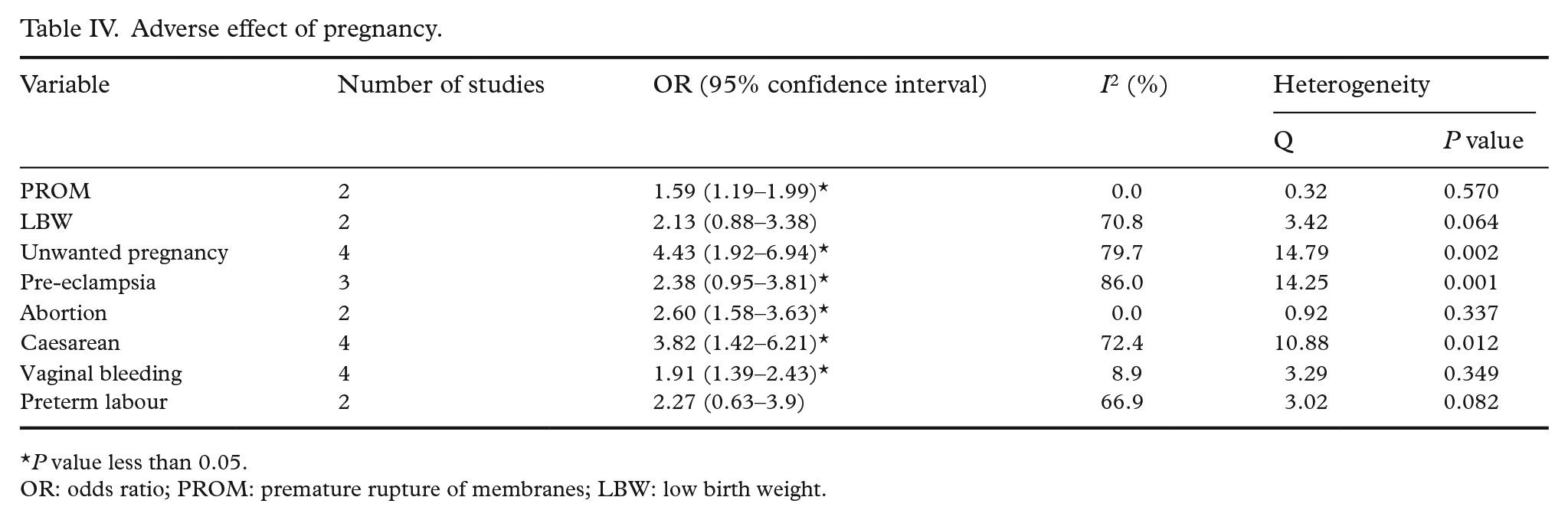
P value less than 0.05.
OR: odds ratio; PROM: premature rupture of membranes; LBW: low birth weight.
Discussion
The present study aimed to determine the IPV prevalence rate among Iranian pregnant women. The results of two meta-analyses conducted in China and Ethiopia showed that the prevalence of violence against pregnant women was 7.7% [6] and 26.1% [74], respectively. The reason for the difference in these findings can be attributed to the culture and context of these communities.
In the current review, the prevalence rate of psychological, physical and sexual IPV was observed to be 43%, 18% and 22%, respectively. In the studies performed in Bangladesh and Kenya, the prevalence rate of psychological, physical and sexual IPV against pregnant women has been reported to be 65%, 35.2% and 18.5%, respectively [75], and 29%, 10% and 12%, respectively [76]. Consistent with our findings, the results of the studies performed in Turkey and Nigeria are indicative of the higher prevalence rate of psychological IPV against women compared to physical and sexual IPV [77, 78], which could be justified by the more explicit judicial law on physical violence. On the other hand, a large number of men now considers physical violence against women an indecent act, and the victims are less likely to report physical violence to maintain their dignity and discipline [79].
Different prevalence rates in various societies could be attributed to cultural diversities; for instance, forced sexual intercourse in couples is not considered an act of sexual violence or a form of rape in some cultures, while psychiatrists refer to this incident as intermarriage rape or domestic rape [45]. According to a recent meta-analysis conducted in Iran, the prevalence rate of emotional, physical and sexual violence against Iranian women (non-pregnant) is 59%, 45% and 32%, respectively [80]. It seems that pregnancy does not protect Iranian women against violence, and sexual and physical violence could increase in this period although it is expected to decline.
According to our findings, the overall IPV rate increased the risk of PROM, unwanted pregnancy, pre-eclampsia, miscarriage, caesarean section and vaginal bleeding. In a systematic review by Hill et al. (2016), the risk of low birthweight and premature delivery was 1.18 and 1.42 times higher in women with a previous experience of violence compared to those with no such experience [81]. The findings of Azevêdo et al. (2013) also indicated a correlation between IPV and unwanted pregnancy [82]. In fact, victims of IPV are more exposed to forced/unprotected sex compared with other women or might not have aimed for pregnancy due to spousal conflicts [6]. In a study by Hawcroft et al. (2019), domestic violence was reported to increase miscarriage by 3.5 times [83]. In a meta-analysis by Qu et al. (2017), an association was observed between psychological stress and miscarriage [84]. Progesterone plays a key role in maintaining pregnancy, while stress inhibits progesterone secretion by inhibiting the hypothalamic–pituitary–ovarian axis and human chorionic gonadotrophin (HCG) secretion from the pituitary gland and reducing prolactin production, which stimulates progesterone production [85]. Moreover, the physical trauma caused by domestic violence is considered to be a secondary cause of trauma in pregnant women, and abdominal trauma in pregnancy directly leads to unfavourable pregnancy outcomes [86]. In line with our findings, Pastor-Moreno et al. (2020) showed an increase in the prevalence rate of PROM in the pregnancies exposed to domestic violence [87].
In the present study, a correlation was observed between the overall IPV rate and the increased risk of pre-eclampsia during pregnancy, which is in congruence with the results obtained by Hawcroft et al. (2019) [83]. Mothers exposed to domestic violence care less about their health status, and unhealthy behaviours such as smoking and alcohol consumption or improper nutrition and inadequate prenatal care have been reported to be more common in these women [71, 88, 89], which increase the risk of adverse pregnancy outcomes (e.g. pre-eclampsia). Consistent with the current review, several studies have confirmed an association between IPV against pregnant women and caesarean section, which could be due to the increased cases of caesarean section caused by adverse maternal and neonatal consequences in pregnant women [90–93]. Given the limited number of the studies regarding the adverse outcomes of IPV, the generalisation of these findings requires further investigation. One of the strengths of our study was its up-to-date and comprehensive nature, as well as the ability to assess all the studies performed in Iran without a time limit and reporting the results in detail.
Limitations
This study had several limitations: (a) One of the limitations of this study was that the included studies did not address whether the consequences of pregnancy were due to violence or not, and occurred solely for other reasons in women who were victims of violence. (b) Another limitation of this study was that the full details of the articles were not fully reported. In some studies, the prevalence of violence was reported in general, and the text of the article did not specify what type of violence was meant. In some other articles, the prevalence of one or more types of violence was presented separately. (c) Another limitation of this study was the use of the STROBE checklist to assess the quality of studies; this checklist does not seem to be able to assess bias compared to the Newcastle Ottawa checklist. It is recommended that this tool be used in future studies to assess bias. Also, in a separate study, the prevalence of violence in the COVID-19 pandemic in Iran should be assessed separately based on existing studies.
Conclusion
According to the results, the prevalence rate of IPV during pregnancy is high in Iran, and more than half of Iranian women experience violence in pregnancy. Psychological IPV was observed to be the most common form of violence against pregnant women. In addition, an association was denoted between IPV during pregnancy and adverse pregnancy outcomes.
According to national guidelines, pregnant women are referred to health centres every month to receive prenatal care. According to the national guidelines, pregnant women are referred to health centres every month for prenatal care and are visited by physicians and midwives. Therefore, investigating IPV during these monthly visits makes it possible to identify these women, introduce them to legal centres, and ultimately reduce adverse consequences for the mother and the fetus.
Supplemental Material
sj-docx-1-sjp-10.1177_14034948221119641 – Supplemental material for The prevalence of intimate partner violence among Iranian pregnant women: a systematic review and meta-analysis
Supplemental material, sj-docx-1-sjp-10.1177_14034948221119641 for The prevalence of intimate partner violence among Iranian pregnant women: a systematic review and meta-analysis by Yosra Raziani, Leila Hasheminasab, Reza Ghanei Gheshlagh, Pegah Dalvand, Vajiheh Baghi and Marzieh Aslani in Scandinavian Journal of Public Health
Footnotes
Acknowledgements
The researchers would like to express their gratitude to the Deputy of Research of the Asadabad School of Medical Sciences for acceptance and approval of this research project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Asadabad School of Medical Sciences. The funding body had no role in the design of the study, data collection or interpretation of the results or in writing of the manuscript (IR. ASAUMS.REC.1400.002).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.