
Abstract
Aim: To investigate validity of widely recommended anthropometric and total fat percentage cut-off points in screening for cardiovascular risk factors in women of different ages. Methods: A population-based sample of 1002 Swedish women aged 38, 50, 75 (younger, middle-aged and elderly, respectively) underwent anthropometry, health examinations and blood tests. Total fat was estimated (bioimpedance) in 670 women. Sensitivity, specificity of body mass index (BMI; ≥25 and ≥30), waist circumference (WC; ≥80 cm and ≥88 cm) and total fat percentage (TF; ≥35%) cut-off points for cardiovascular risk factors (dyslipidaemias, hypertension and hyperglycaemia) were calculated for each age. Cut-off points yielding high sensitivity together with modest specificity were considered valid. Women reporting hospital admission for cardiovascular disease were excluded. Results: The sensitivity of WC ≥80 cm for one or more risk factors was ~60% in younger and middle-aged women, and 80% in elderly women. The specificity of WC ≥80 cm for one or more risk factors was 69%, 57% and 40% at the three ages (p < .05 for age trends). WC ≥80 cm yielded ~80% sensitivity for two or more risk factors across all ages. However, specificity decreased with increasing age (p < .0001), being 33% in elderly. WC ≥88 cm provided better specificity in elderly women. BMI and TF % cut-off points were not better than WC.
Keywords
Background
Overweight, obesity and associated cardiovascular risk factors, including hypertension, dyslipidaemia and hyperglycaemia, are increasing, even among younger populations [1], accelerating cardiovascular disease. Therefore, healthy lifestyles need to be promoted at the population level and among higher-risk individuals [2]. Anthropometric measurements such as waist circumference (WC) and body mass index (BMI; body mass in kg/height in m2)) are recommended to identify individuals who are more likely to have cardiovascular risk factors and who may benefit from weight reduction [3,4]. BMI cut-off points for overweight (≥25) and obesity (≥30) [5] and the corresponding respective WC cut-off points (80 cm and 88 cm, respectively, for women) [6,7] are widely recommended. Other recommended anthropometric cut-off points for women include waist–hip ratio (WHR, WC/hip circumference) ≥0.85 [8] and waist–height ratio (WHtR, WC/height) ≥0.5 [9]. Furthermore, estimated total body fat (TF) ≥35% for women is sometimes claimed to be superior to anthropometric cut-off points [10]. These recommended anthropometric and TF% cut-off points will be referred to as fatness cut-off points in this paper.
On the other hand, the impact of age on the validity of recommended fatness cut-off points to identify adults with cardiovascular risk factors correctly has been less studied. Correlations and odds ratios between anthropometric indices, TF% and cardiovascular risk factors were severely attenuated with increasing age in Danish and US NHANES population samples [11,12], suggesting that screening validity may vary with age. Discrimination of individuals having cardiovascular risk factors by anthropometry, according to area under receiver operating characteristic (ROC) curves was significantly lower in older than in younger Japanese and Iranian adults [13,14]. Age differences in sensitivity and specificity of widely recommended cut-off points for cardiovascular risk factors were reported from Canadian, US and Iranian population samples [4,15–16]. The statistical and clinical significance of the age differences in these latter studies was not clarified.
In this paper, we further explore the validity of recommended anthropometric and TF% cut-off points as a first-step tool to screen for cardiovascular risk factors in a population sample of younger, middle-aged and elderly women from Gothenburg, Sweden. Women who did not report hospital admission for cardiovascular disease were considered for the present analysis. Validity was evaluated in the public health context. Hence, 70–80% sensitivity for cardiovascular risk factors was considered a first prerequisite. Second, valid cut-off points also had to yield at least 50% specificity.
Design and methods
A systematic random sample of women aged 38 (n = 343), 50 (n = 503) or 75 (n = 791) was selected, based on dates of birth, from population registries in Gothenburg, Sweden. They were sent a letter of invitation for free health examinations. Of 1637 potential participants, 152 could not be reached due to wrong address, lack of listed telephone, and so on. Thirty-three per cent of those who received the invitations declined to participate. Seven women who did not speak Swedish were excluded. This left 1002 women who provided informed consent for study participation. Recruitment took place during 2004–6 for 38 and 50 year olds and during 2005–2006 for 75 year olds [17,18]. The Regional Ethics Committee in Göteborg approved this study.
Participants completed a self-administered questionnaire providing demographic, medical and other health-related information. Blood pressure was measured with a mercury manometer in the seated position after five minutes’ rest. Self-reports on medication intake for hypertension, dyslipidaemia or diabetes were obtained during a physician or nurse interview. Blood samples were obtained after overnight fasting and analysed using standard protocols.
Body weight and height were measured, to the nearest 0.1 kg by balance scale, with the participant standing erect, arms at her side and feet together. Height was measured to the nearest 0.5 cm. WC was measured to the nearest 1 mm, midway between the lower rib margin and the iliac crest, using a steel tape measure, at the end of expiration. Hip circumference (HC) was measured, using the same tape measure, to the nearest 1 mm at the widest point between the hip and buttocks. WC and HC were measured with the subject standing. BMI, WHtR and WHR were subsequently calculated.
TF was estimated in 670 women. This was performed by Bioelectrial Impedance Spectroscopy (BIS), using a Xitron 4200 Hydra system (Xitron Technologies, Inc.), with the participant supine on a non-conductive examination table without a pillow, legs and arms slightly apart, as described previously [19]. Electrode pairs (Conmed® Corporation) were appropriately positioned at the middle of the dorsal surfaces of the hands and feet, according to the manufacturer’s instructions. Bioimpedance was measured using 50 logarithmically spaced frequencies from 5 kHz to 1 MHz, and intracellular water, extracellular water and fat-free mass were estimated using the instrument software. The manufacturer’s BIS equation incorporated weight, height, body density, a shape factor and sex-specific resistivity, but not age. Women who underwent Bioimpedance were similar to the women that did not undergo bioimpedance in distribution of all indices of fatness (independent samples t-test p > .1). TF% was calculated as (fat mass/body mass) × 100.
Major cardiovascular and metabolic risk factors were defined according to the National Cholesterol Education Program (NCEP) ATP III criteria [20]. Hypertension was defined as ≥140/90mm Hg; high serum LDL cholesterol as ≥3.36 mmol/L; low serum HDL cholesterol as <1.29 mmol/L; high serum triglycerides as ≥1.7 mmol/L; and hyperglycaemia as fasting plasma glucose ≥6.1 mmol/L. Women taking medication for the above conditions were classified as positive for the particular condition, regardless of their test results.
Statistical analysis
Participants who did not report hospital admission for cardiovascular disease were included (98% of younger and middle-aged women, and 71% of elderly women). The prevalence of overweight, obesity and so on was calculated according to the above-mentioned recommended fatness cut-off points. The prevalence of hypertension, dyslipidaemias, hyperglycaemia, as well as of one or more, two or more, and three or more assessed risk factors, was calculated.
Women who exceeded recommended fatness cut-off points were identified as being more likely to have cardiovascular risk factors. One recommended fatness cut-off point was considered at a time. In a hypothetical screening situation, only these women would be selected for lifestyle intervention or, possibly, to undergo confirmatory tests (i.e. blood pressure and blood tests for lipids and glucose). Sensitivity and specificity of each recommended fatness cut-off point for one or more or two or more risk factors was calculated. Of all women with risk factors, the percentage who would also be identified as ‘overweight or obese’ (or test-positive) would constitute sensitivity. Correspondingly, of all women without the risk factors under consideration, the percentage who would be identified as ‘not overweight or obese’ (or test-negative) would constitute specificity [21]. Ninety-five per cent confidence intervals (CI) were calculated according to Openepi [22]. All analyses were age stratified. Statistical significance of age trends was calculated using the Extended Mantel–Haenszel Chi-Square Test for linear trend. The sensitivity and specificity for three or more risk factors was calculated only in the elderly group, as its prevalence was low in the other age groups.
Effectiveness is defined as the capability to produce the intended results, which in the case of anthropometric screening is to minimise the use of the more expensive confirmatory tests. Thus, anthropometric screening may be considered to be effective, first, when most women with risk factors are ‘test positive’ and, second, if the fraction of women selected to undergo confirmatory tests is reasonably low (percentage of women above the fatness cut-off point, as in Table I). We evaluate screening effectiveness as defined above, by using a Figure to compare sensitivity yield against the fraction of women selected by WC ≥80 cm for confirmatory tests.
Prevalence of cardiovascular risk factors and overweight/obesity in women who did not report hospital admission for cardiovascular disease.
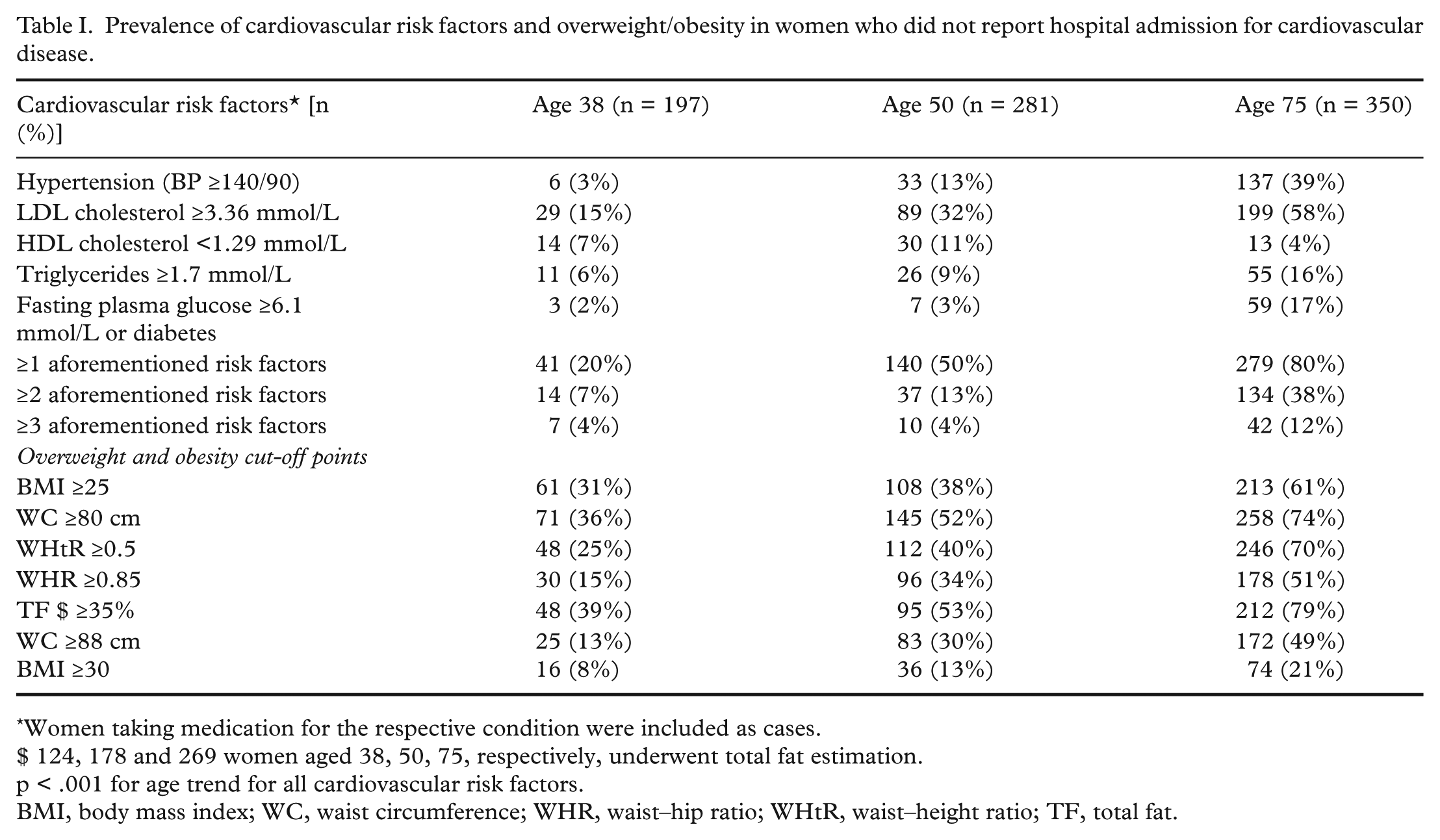
Women taking medication for the respective condition were included as cases.
$ 124, 178 and 269 women aged 38, 50, 75, respectively, underwent total fat estimation.
p < .001 for age trend for all cardiovascular risk factors.
BMI, body mass index; WC, waist circumference; WHR, waist–hip ratio; WHtR, waist–height ratio; TF, total fat.
Results
The proportions of women with overweight, obesity or central overweight/obesity showed the expected increases with increasing age (Table I). The prevalence of individual and multiple risk factors also increased with increasing age, as anticipated. At all three ages studied, high serum LDL cholesterol was most prevalent (15%, 32% and 58%, respectively), followed by hypertension (3%, 13% and 39%, respectively). Nine per cent of elderly women were diabetic (1% at other ages).
Table II presents sensitivities and specificities (with 95% CI) yielded by each recommended anthropometric and TF % cut-off point, by age. First, considering validity to screen for one or more risk factors, the maximal sensitivity achieved in younger and middle-aged women was 45–60% (using BMI ≥25, WC ≥80 cm, WHtR ≥0.5 or TF ≥35%). Obesity (BMI ≥30) exhibited the lowest sensitivity (~20%). Sensitivity for one or more risk factors in elderly women was generally higher (70–80% using WC ≥80 cm, WHtR ≥0.5 or TF ≥50%) than in younger women. The linear age trend in sensitivity for all cut-off points except BMI ≥30 was statistically significant (p < .05). In contrast, specificity decreased from younger to middle age to elderly (p < .05 for all cut-off points).
Sensitivity (% [95% CI]) and specificity (% [95% CI]) of studied anthropometric and TF% cut-off points for cardiovascular risk factors in Swedish women, by age.
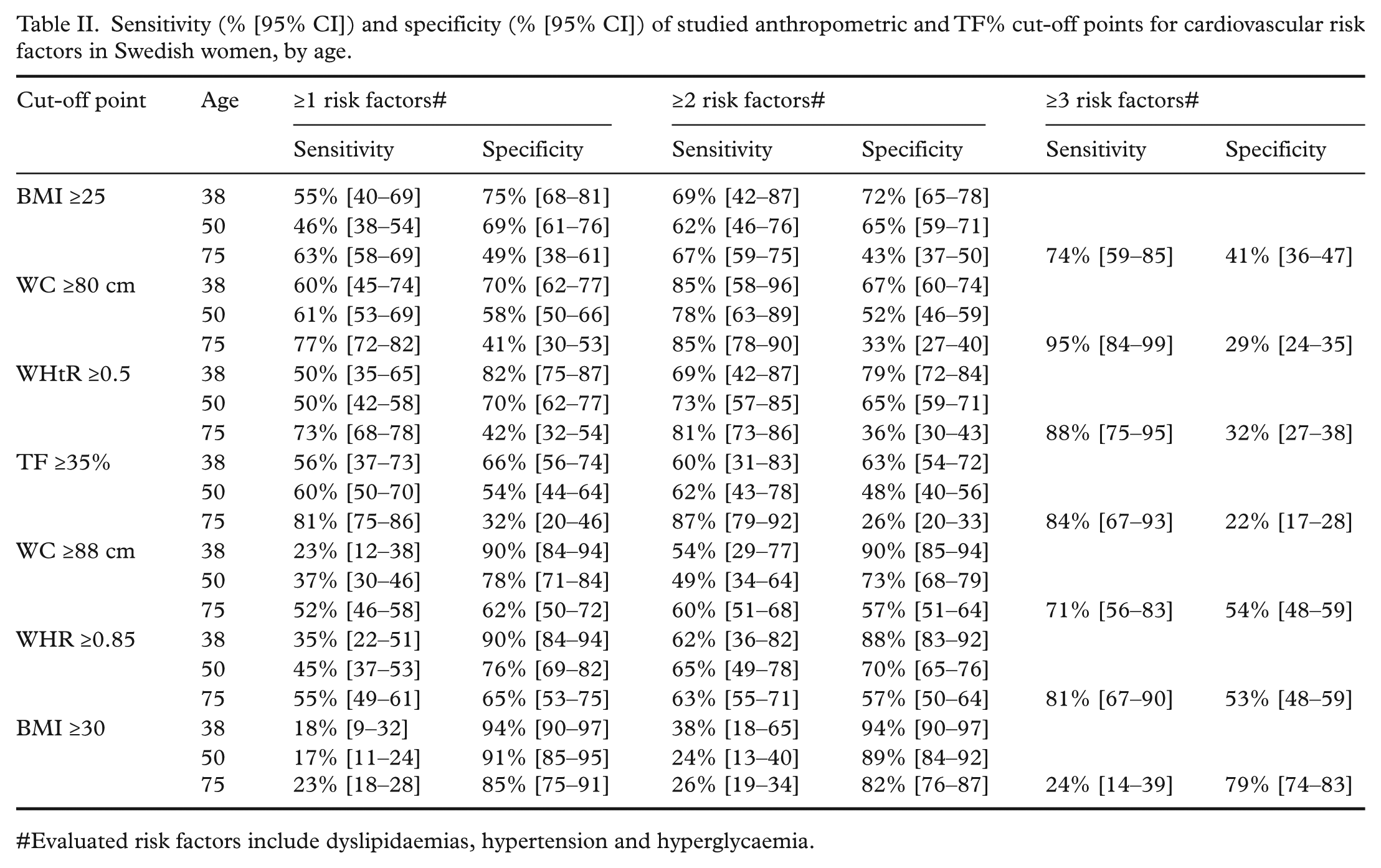
Evaluated risk factors include dyslipidaemias, hypertension and hyperglycaemia.
Figure 1 compares sensitivity yielded by WC ≥80 cm (from Table II) against the fraction of women who tested positive for WC ≥80 cm (from Table I). Thus, confirmatory tests in 36% of younger and 52% of middle-aged women would identify ~60% with one or more risk factors at either age (Table II). In contrast, in the elderly, confirmatory tests would be required in 74% to identify 77% with one or more risk factors.
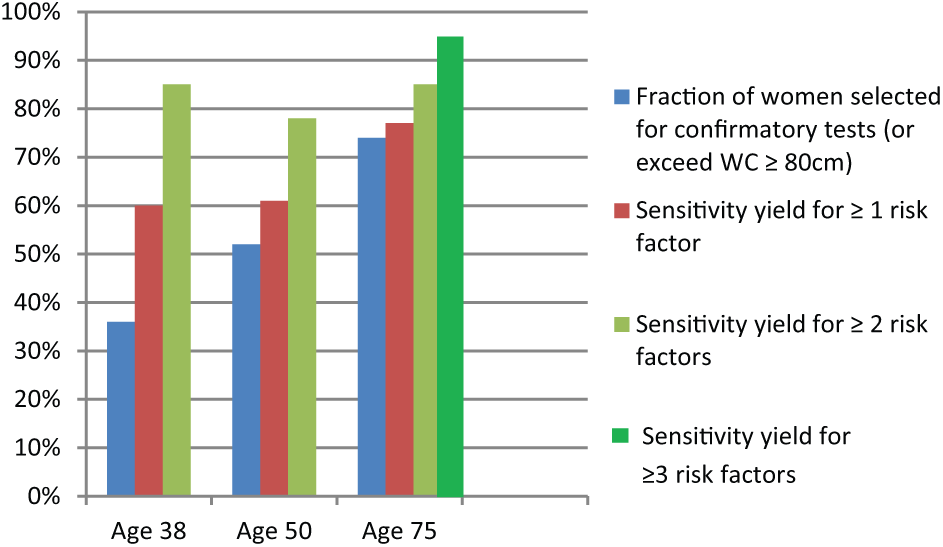
A comparison of screening effectiveness in 38-, 50- or 75-year-old Swedish women, using waist circumference (WC) ≥80 cm to screen for cardiovascular risk factors.
Sensitivity yield for two or more risk factors (Table II) was ~60–70% with BMI ≥25, and ~70–80% with WC ≥80 cm or WHtR ≥0.5. These sensitivities did not differ significantly by age. However, specificity decreased significantly with increasing age (p < .0001 for all cut-off points; Table II). The percentage of women selected for confirmatory tests by WC ≥80 cm was 36% [95% CI 30–43] in younger women; 52% [95% 46–57] in middle-age women; and 74% [95% CI 69–78] in elderly women, to identify ~80% with two or more risk factors at all ages (Figure 1). Thus, a potentially larger reduction in the use of confirmatory tests is obtainable with anthropometric screening in younger women, while this advantage (screening effectiveness) diminishes in middle-aged and elderly women.
Considering screening for three or more risk factors in elderly women (Table II), WC ≥88 cm and WHR ≥0.85 yielded the best combination of sensitivity and specificity. Though sensitivity yield of BMI ≥25 was similar to the above cut-off points, its specificity was significantly lower (Table II). The percentage of elderly selected for confirmatory tests by BMI ≥25 (61% [95% CI 56–66]) was significantly higher than that selected by WC ≥88 cm (49% [95% CI 44–54]). Lastly, validity of TF ≥35% for one or more, two or more or three or more risk factors was not superior to the anthropometric cut-off points at any age (Table II).
Discussion
The main finding of this study is that recommended anthropometric cut-off points, when used as action levels for screening asymptomatic women, show important concerns that vary with age. In younger and middle-aged women, WC ≥80 cm and WHtR ≥0.5 showed high sensitivity and modest specificity to identify two or more risk factors; positive predictive values were 15% in younger and 20% in middle-age. In elderly women, WC ≥88 cm or WHR ≥0.85 were valid to screen for three or more risk factors. Positive predictive value in the elderly using these cut-off points was 17–19% for three or more risk factors, and 13–14% for diabetes. Negative predictive values for the above conditions and cut-off points were high (93–98%). Thus, some currently recommended cut-off points were valid to identify multiple risk factors. Women more likely to have multiple risk factors are certainly a high-risk group and need immediate attention. Nevertheless, low sensitivity of recommended cutpoints for one or more risk factors in younger and middle-aged women implies that at least 40% of asymptomatic women with one or more risk factor at these ages would be missed from confirmatory tests or lifestyle intervention. On the other hand, using WHtR ≥ 0.5 would miss 50% younger or middle age with one or more risk factor. In contrast, in the elderly, low specificity for one or more or two or more risk factors was a concern. Therefore, cut-off points for screening need to be fine-tuned for the different ages.
A very limited number of population-based studies have estimated sex- and age-specific sensitivity and specificity of recommended anthropometric cut-off points for cardiovascular risk factors [4,15,16,23]. In a representative study of ~5000 women in Iran (16), BMI ≥25, WC ≥80 cm, WHtR ≥0.5 or WHR ≥0.8 yielded 70–90% sensitivity and 50–58% specificity for hypertension and diabetes at 18–39 years, and 80–90% sensitivity and 10–30% specificity at 40–74 years [16]. A similar decrease in specificity with increasing age was reported for dyslipidaemia [16]. In a representative sample of Japanese American adults from Washington, USA, reported sensitivity and specificity of recommended BMI and WC cut-off points varied with age [23]. The prevalence of overweight and statistical significance of age differences were not clear from the data presented in the latter studies [16,23]. Ethnicity in these studies [16, 23] is not comparable to ours, nevertheless, age-related variations in screening validity are comparable.
The main contributions of this study to the existing literature are fourfold. We have, for the first time, highlighted that specificity of standard anthropometric cut-off points for cardiovascular risk factors decreases significantly with increasing age, and that there are statistically and clinically significant age-related variations in sensitivity. Second, we demonstrate that the practical advantage of the standard anthropometric cut-off points in reducing the use of confirmatory tests decreases with increasing age. To our knowledge, only one previous study made this comparison between different ages, but did not report statistical tests – the population-based Canadian Saskatchewan Heart Health Survey [4] found that the WHR cut-off point ≥0.8 yielded 61% sensitivity for dyslipidaemia, and selected 25% of women aged 18–34 years for confirmatory tests, whereas in women aged 55–74 years, 58% of women needed confirmatory tests to yield 74% sensitivity [4]. Third, we have shown that the higher WC cut-off point is more valid in elderly women than the lower cut-off point. This is biologically plausible, as visceral fat deposition in women increases with age [17]. The validity of a higher WC cut-off point in older women is also supported by previous research. Optimal cut-off points of WC to identify cardiovascular risk factors was 89 cm in Japanese American women ≥56 years, whereas it was 81 cm in younger women [23]. Similar age variations were reported for cut-off points of intra-abdominal fat area [23]. In the Iowa prospective cohort study [24] of 31,702 women aged 55–69 years free of cancer, heart disease and diabetes at baseline, 79% of incident diabetes and 54% of coronary artery disease mortality after 11–12 years’ follow-up occurred in the 40% of women who had WC ≥87.3 cm at baseline. WHR ≥0.85 showed similar prevalence at baseline and disease incidence at follow-up [24]. Lastly, TF%, as estimated by bioimpedance, did not yield a better combination of sensitivity and specificity than recommended anthropometric cut-off points at the three ages studied, as has also been suggested previously [25].
Our study is population based with a reasonably high participation rate (~70%, albeit somewhat lower in the elderly group). We excluded women who had hospital admissions for cardiovascular disease. Thus, our results apply directly to screening of ostensibly healthy women in similar populations; and possibly to asymptomatic women visiting primary care physicians. The differing prevalence of overweight and risk factors, ethnicity; and the differential pattern of self-referral for physician care may alter screening characteristics. Nevertheless, age-related variations in screening validity of standard cut-off points are likely. We included only women who underwent anthropometric measurements, blood pressure and blood tests, thus avoiding verification bias. Though we studied only three ages, these are appropriate for study of screening. Small age-group samples resulted in wide confidence intervals. Nevertheless, age trends in specificity and fraction of women selected for confirmatory tests remain unambiguous.
Our analyses have some limitations. First, we studied validity of recommended cut-off points to identify asymptomatic women with risk factors at different ages, but not to predict future cardiovascular disease. Second, our sample size was not adequate to evaluate validity for individual risk factors at different ages. Third, the results from this female cohort cannot be generalised to men, which is an important limitation, and is a topic for further study in other cohorts. The few available studies show variation in sensitivity and specificity [4,15], and decreasing correlations, odds ratios and ROC AUCs in this context with increasing age [11–14] in men, as in women.
Our results suggest that WC cut-off points to identify asymptomatic women that have risk factors need to be established according to age. Previous studies have used varied criteria based on ROC analysis to derive age-specific cut-off points in screening for risk factors. These include cut-off points where (a) sensitivity equalled specificity [26,27]; (b) the Youden index was maximised [23]; (c) sum of sensitivity and specificity was maximised [28]; (d) the point on the ROC curve closest to (0, 1) [23], and so on. In general, whatever the criteria used, optimal cut-off points were lower in the younger age group in comparison to the older age group. In the public-health context, however, where sensitivity is of paramount importance [29], cut-off points yielding high sensitivity (at least 80%) and at least ‘modest’ specificity at each age should be chosen as optimal. It is important to note that optimal cut-off points may vary with ethnicity or other population characteristics.
Measurement of WC in primary care would compete for the limited time available, and it requires specific training. However, age-specific cut-off points that maximize sensitivity can be a feasible, inexpensive and effective screening tool to identify most asymptomatic younger and middle-aged women who can benefit from positive lifestyle changes and body weight control. In obesogenic environments, all women testing positive, whether they have risk factors or not, are only likely to benefit from positive lifestyle changes [30]. On the other hand, it is hard to justify expensive blood tests for all asymptomatic and low risk younger and middle-aged women, particularly in lower resource settings. However, the limitations and disadvantages of screening need attention. First, confirmatory tests for risk factors should not be advised routinely, based only on anthropometric screening results. Second, women testing positive should be reassured, and terms implying ‘obesity’, ‘excessive fatness’ or ‘higher risk’ should be shunned. Third, other risk factors such as smoking and family history should be considered in advising lifestyle changes. However, in older women, women having other risk conditions or symptoms suggestive of cardiovascular disease, blood pressure and lipids should be measured as per national health guidelines, or according to clinical requirement.
Conclusions
Our results show that standard cut-off points are not appropriate as screening cut-off points for asymptomatic women of different ages. Available results suggest that for younger women, cut-off points should be lowered, to improve sensitivity for one or more risk factor. In older women, cut-off points should be increased, to improve specificity. Screening cut-off points that maximise sensitivity for risk factors and yield modest specificity may be considered optimal for use in public health. Whether positive lifestyle changes in women identified by these age-specific cut-off points can reduce morbidity and mortality from diabetes or cardiovascular disease needs to be established by further study.
Footnotes
Acknowledgements
The authors thank Prof Bo Eriksson for comments on an earlier draft.
Conflict of interests
The authors declare that there is no conflict of interest.
Ethical approval
This study was approved by the Regional Ethics Committee in Göteborg (Approval number Ö 564-03, Dnr T453-04 (041104).
Funding
This work was partly funded by FAS, The Swedish Council on Working Life and Social Research (2005-0794, 2006-1506, 2004-0145, 2006-0596, 2008-1111); WISH, EpiLife (2006-1506); The Swedish Research Council (11267, 825-2007-7462), and the Bank of Sweden Tercentenary Foundation.