
Abstract
Background
Over 45% of firefighter deaths are attributable to sudden cardiac death related to coronary artery disease (CAD), with many of these deaths attributed to comorbidities. The purpose of the study is to determine the prevalence of coronary artery disease (CAD) risk factors in firefighters in the City of Cape Town (CoCT).
Design and methods
The study used a quantitative, cross-sectional and descriptive design. A total of 124 full-time firefighters were conveniently recruited between September and November 2019 from the City of Cape Town Fire and Rescue Service.
Results
The most prevalent CAD risk factors among firefighters were hypertension (33.1%), obesity (37.1%), cigarette smoking (39.5%) and dyslipidaemia (40.3%). A total of 41.9% of firefighters were categorized as low-risk, 54.8% as moderate-risk, and 3.2% as high-risk for CAD.
Conclusion
The majority of firefighters had at least one CAD risk factor, with older males having the highest prevalence of multiple CAD risk factors. Compared to other regions of the world, the (CoCT) firefighters have higher prevalence of dyslipidaemia and cigarette smoking. Preventative behavioural strategies and education on CAD should be promoted to mitigate the development of CAD.
Introduction
Significance for public health
This paper adds new knowledge on coronary artery disease (CAD) risk factors in firefighters, in the City of Cape Town Fire and Rescue Service. This study also provides valuable research into a scarcely studied research field. This article highlights the high prevalence of CAD risk factors present in firefighters and the general community of Cape Town, and the need for immediate corrective measures including behavioural modification to reduce these risk factors, and education on preventative measures. There is a high prevalence of CAD risk factors among firefighters, both male and female, in the Fire and Rescue Service in the City of Cape Town that likely contributes to premature morbidly and mortality in this population.
Over 45% of firefighter deaths are due to sudden cardiac death, with many of these deaths attributed to comorbidities. 1 Firefighting is a hazardous occupation that involves firefighters in life-threatening situations, where they are exposed to severe temperatures, tremendous cardiovascular workloads and hazardous chemicals and fumes.1,2 These severe conditions necessitate that firefighters wear protective clothing and rescue equipment that is heavy and insulated, which puts tremendous strain on the cardiovascular system.2,3 The majority of firefighters (67%-85%) have at least one coronary artery disease (CAD) risk factor.1,4-6 Many firefighters have multiple CAD risk factors, thus, increasing the risk of premature morbidity and/or mortality, while on duty.1,6,7 Previous studies found that an alarming number of firefighters were hypertensive (27%), dyslipidemic (33.3%), cigarette smokers (38%), physically inactive (49%) and obese (63%).3,6,8-10 Viewed collectively, the hazardous conditions of firefighting, together with the excess weight of the firefighting equipment and the multiple CAD risk factors present in many firefighters, increase the likelihood of a sudden cardiac event.1,5,6 Appropriate and timely screening of CAD risk factors will highlight the firefighters at risk, and provide data to aid in reducing firefighter casualties and the associated loss of life and property.1,6
Design and Methods
This study used a quantitative, cross-sectional and descriptive design. A total of 124 full-time firefighters, males and females, were conveniently recruited from the City of Cape Town Fire and Rescue Service. The demographic characteristics included were age, gender, marital status, family history of CAD, smoking and ethnicity using a researcher-generated questionnaire. The International Physical Activity Questionnaire (IPAQ) was used to measure physical activity. Ethnicity was self-reported by each participant, based upon the historical South African classification system, i.e., Black, mixed ethnicity, White, Indian, and other. Ethnicity was included to encompass all demographic characteristics in the Cape Town metropolitan area. The study took place between September and November 2019. All subjects gave their informed consent for inclusion before they participated in the study. The study protocol was approved by the Ethics Committee of the Biomedical Research Ethics Committee (BMREC) at the University of the Western Cape (Ethics reference number: BM19/4/3). The study was also approved by the Chief Fire Officer of the City of Cape Town Fire and Rescue Service, as well as the Director of Policy and Strategy of the City of Cape Town. All the information obtained from the participants remained confidential. No personal information of the participants will be disclosed to the Fire Department that could compromise the confidentiality of the participants. All information regarding this research is stored securely in the SRES department, with access available to the researcher and supervisor only.
Research measures
Stature was measured using a portable stadiometer, standing barefoot on the level plastic plate with the heels together, and the heels, buttocks and upper back aligned to the stadiometer rod in the Frankfort plane. Body mass was measured with the participant wearing minimal indoor clothing and measured to the nearest 50 grams using a precision electronic scale. Blood pressure was measured using a standard blood pressure sphygmomanometer and stethoscope, with the appropriate cuff size. The standard auscultatory method of blood pressure measurement was used. 11 Total cholesterol and non-fasting blood glucose were measured using the finger-prick method and analysed with an AcuTrendR Plus GC meter. Waist circumference was measured at the point of the umbilicus, 11 between the lower costal border and top of the iliac crest, perpendicular to the long axis of the trunk. Hip circumference was taken at the level of the greatest posterior protuberance of the buttocks. Waist and hip circumferences were measured to the nearest 0.1 cm at the end of normal expiration. 11 The crosshand technique was used to measure all circumferences, using a steel tape measure. 11 The research instruments used for data collection were calibrated, prior to testing. A minimum test-retest reliability coefficient of 0.8 was required prior to the commencement of the study and only one tester was used in the study. 11
Analysis
All data was captured by double-entry into a Microsoft Office Excel spreadsheet, and then cleaned of errors. Thereafter, it was exported to the Statistical Package for the Social Sciences version 26 for descriptive data analysis. Firefighters were then separated into gender, age and ethnic groups. Firefighters were categorized into CAD risk categories using the ACSM guidelines ninth edition. 12 Mann-Whitney U and Kruskal-Wallis H was used to determine statistical differences between groups and a p-value of less than 0.05 was used to indicate statistical significance.
Results
The mean age of the firefighters was 37.53±9.05 years, and the mean body mass and stature were 87.4 kilograms (kg) and 172.6 centimetres (cm), respectively. The majority of firefighters were male (79.0%), and 20.9% were female. The mean age, body mass and stature were 37.8±9.8 years, 87.8 kg and 174.7 cm for males, and 36.4±5.4 years, 85.9 kg and 164.8 cm for females. When all participants were separated into age-group categories, the agegroup 20-29 years represented 19.4% of the participants in the study, the age-group 30-39 years had the highest with 44.4%, the age-group 40-49 years had 24.2%, and the age-group 50-65 years had the lowest with 12.1%. The majority of firefighters were of mixed ethnicity (56.5%), followed by Black firefighters (25.8%), and then White firefighters (16.9%).
In the study, 41.9% of firefighters were categorized as low-risk (≤1 CAD risk factor), 54.8% were moderate-risk (≥2 CAD risk factors), and 3.2% were high-risk (diagnosed with known CAD or presented with signs and symptoms of CAD) (Table 1). Based on gender, firefighters categorized as low-risk were 50% and 39.8% for females and males, respectively, and firefighters at moderaterisk were 50% and 56.0% for females and males, respectively. Only male firefighters were categorized as high-risk (4.1%). Firefighters at moderate-risk for CAD increased with age, with the age-group 20-29 years reporting 29.2% at moderate-risk, the agegroup 30-39 years with 47.3%, the age-group 40-49 years with 76.7%, and the age-group 50-65 years with 80.1%. Only the agegroups of 20-29 and 50-65 years were at high-risk for CAD, with 8.3% and 13.3%, respectively. Black firefighters reported the lowest prevalence of moderate risk for CAD with 37.5%, followed by firefighters of mixed ethnicity with 60.1%, and White firefighters with 66.7%. Firefighters categorized as high-risk for CAD were 2.9% and 9.5%, for mixed ethnic and White firefighters, respectively.
CAD risk stratification in firefighters.

One firefighter was excluded from the ethnic groups, because he was of Indian descent.
Diabetes was the CAD risk factor least prevalent (8.9%) in firefighters (Figure 1) and was prevalent amongst male firefighters only (Table 2). Based on age-group, diabetes was absent in the youngest group 20-29 years, while the age-group 30-39 years had 1.8%. The age-group 40-49 years had a diabetes prevalence of 26.7%, and the age-group 50-65 years had the highest with 33.4%. The prevalence of diabetes among the various ethnic groups was 6.3% in Black firefighters, 9.5% in White firefighters, and 10.0% in firefighters of mixed ethnicity.
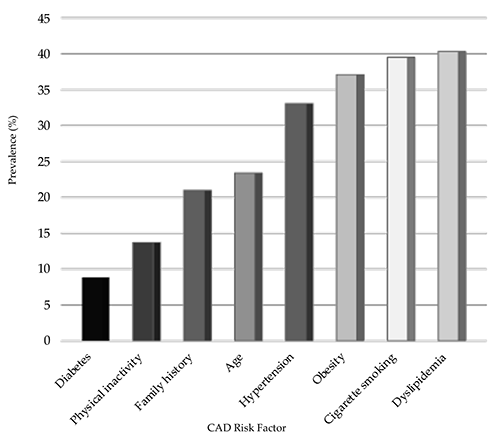
Prevalence of CAD risk factors in firefighters.
Prevalence of CAD risk factors among firefighters according to gender, age-group and ethnicity.
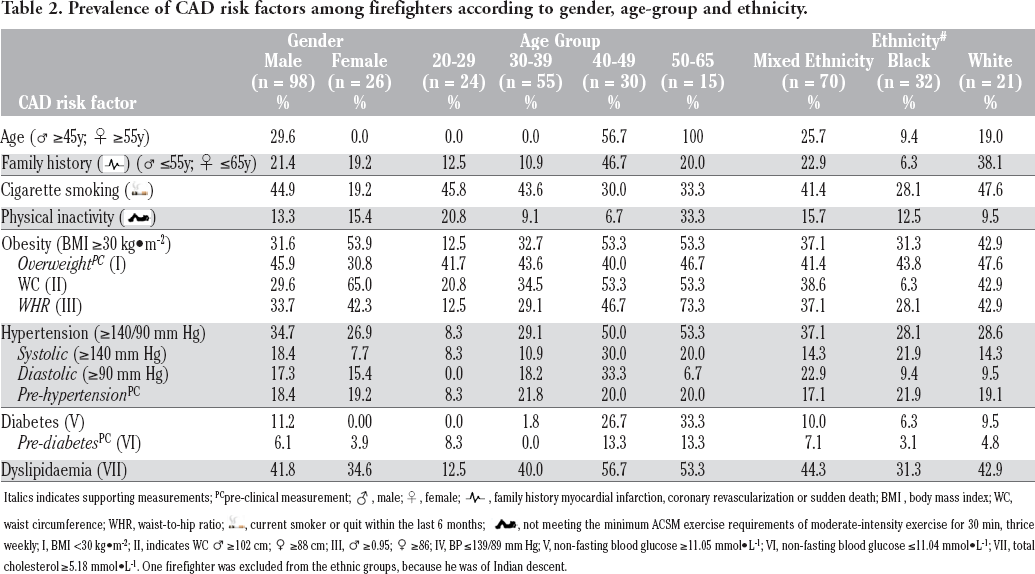
Italics indicates supporting measurements; PCpre-clinical measurement;, male; ♀, female;  , family history myocardial infarction, coronary revascularization or sudden death; BMI, body mass index; WC, waist circumference; WHR, waist-to-hip ratio;
, family history myocardial infarction, coronary revascularization or sudden death; BMI, body mass index; WC, waist circumference; WHR, waist-to-hip ratio;  , current smoker or quit within the last 6 months;
, current smoker or quit within the last 6 months;  , not meeting the minimum ACSM exercise requirements of moderate-intensity exercise for 30 min, thrice weekly; I, BMI <30 kg•m-2; II, indicates WC ♂ ≥102 cm; ♀ ≥88 cm; III, ♂ ≥0.95; ♀ ≥86; IV, BP ≤139/89 mm Hg; V, non-fasting blood glucose ≥11.05 mmol•L-1; VI, non-fasting blood glucose ≤11.04 mmol•L-1; VII, total cholesterol ≥5.18 mmol•L-1. One firefighter was excluded from the ethnic groups, because he was of Indian descent.
, not meeting the minimum ACSM exercise requirements of moderate-intensity exercise for 30 min, thrice weekly; I, BMI <30 kg•m-2; II, indicates WC ♂ ≥102 cm; ♀ ≥88 cm; III, ♂ ≥0.95; ♀ ≥86; IV, BP ≤139/89 mm Hg; V, non-fasting blood glucose ≥11.05 mmol•L-1; VI, non-fasting blood glucose ≤11.04 mmol•L-1; VII, total cholesterol ≥5.18 mmol•L-1. One firefighter was excluded from the ethnic groups, because he was of Indian descent.
Physical inactivity was prevalent in 13.7% of firefighters (Figure 1). Both male and female firefighters had a similar prevalence for physical inactivity, 13.3% and 15.4%, respectively (Table 2). The youngest age-group 20-29 years had physical inactivity in 20.8%, the age-group 30-39 years had 9.1%, the age-group 40-49 years had 6.7%, and the age-group 50-65 years had the highest with 33.4%. According to ethnic groups, White firefighters had physical inactivity in 9.5%, Black firefighters with 12.5% and firefighters of mixed ethnicity with 15.7%.
A total of 20.9% of firefighters reported a positive family history of CAD (Figure 1). Males and females reported a similar prevalence of family history in 21.4% and 19.2%, respectively (Table 2). According to age-group, family history was prevalent in 12.5% of firefighters aged 20-29 years, in 10.9% of firefighters aged 30-39 years, in 46.7% of firefighters aged 40-49 years, and in 20.0% of firefighters aged 50-65 years. A positive family history was present in 6.3% of Black firefighters, in 22.9% of firefighters of mixed ethnicity, and in 38.1% of White firefighters.
A total of 23.4% of firefighters had age as a CAD risk factor (Figure 1), and they were all male (29.6%) (Table 2). Age, as a CAD risk factor, was absent in the age groups 20-29 years and 30-39 years, while the age-group 40-49 years had 56.7% with age as a risk factor, and the age-group 50-65 years had all firefighters with age as a risk factor. Age was a risk factor in 9.4% of Black firefighters, in 19.0% of White firefighters and in 25.7% of firefighters of mixed ethnicity.
A total of 33.1% of firefighters had hypertension as a CAD risk factor (Figure 1). Among male firefighters, 34.7% had hypertension, and among female firefighters, 26.9% had hypertension (Table 2). In the age-group 20-29 years, 8.3% had hypertension, the age-group 30-39 years had 29.1%, the age-group 40-49 years had 50.0%, and the age-group 50-65 years had the highest with 53.3%. Black and White firefighters had a similar prevalence of hypertension in 28.1% and 28.6%, respectively. Firefighters of mixed ethnicity had the highest prevalence of hypertension in 37.1%. Among all firefighters, 18.6% were pre-hypertensive and 48.4% were normotensive (Table 2).
A total of 37.10% of firefighters were obese (Figure 1). Male firefighters had obesity in 31.6% and female firefighters had obesity in 53.9% (Table 2). The age-group 20-29 years had obesity in 12.5%, followed by the age-group 30-39 years with 32.7%. The older two age-groups, 40-49 years and 50-65 years, had the same obesity prevalence of 53.3% each. Obesity was prevalent in 31.3% of Black firefighters, in 37.1% of firefighters of mixed ethnicity and in 42.9% of White firefighters. Furthermore, central obesity was prevalent in 29.6% of male firefighters and in 65.0% of female firefighters (Table 2). Central obesity was least prevalent in the youngest age-group 20-29 years with 20.8%, followed by the group 30-39 years with 34.5%, and the two older age-groups i.e., 40-49 years and 50-65 years, with 53.3% each. Central obesity was prevalent in 28.1% of Black firefighters, in 38.6% of firefighters of mixed ethnicity and in 42.9% of White firefighters.
A total of 39.5% of firefighters were categorized as current cigarette smokers (Figure 1). Among the male firefighters, 44.9% were smokers, compared to 19.2% of female firefighters who smoked (Table 2). Among the smokers, 36.7% smoked less than 5 cigarettes per day and were classified as light smokers, 51.0% smoked 6 to 19 cigarettes a day and were classified as moderate smokers, and 14.3% smoked 20 or more cigarettes a day and were classified as heavy smokers. The youngest age-group of 20-29 years had the highest prevalence of smokers (45.8%), followed by the age-group 30-39 years with 43.6%. The age-group 40-49 years had the lowest prevalence of smokers with 30.0%, and the group 50-65 years had 33.3%. Cigarette smoking was prevalent in 28.1% of Black firefighters, in 41.4% of firefighters of mixed ethnicity and in 47.6% of White firefighters.
Dyslipidaemia was the most prevalent CAD risk factor amongst the firefighters and was present in 40.3% of firefighters (Figure 1). Dyslipidaemia among male and female firefighters was prevalent in 41.8% and 34.6%, respectively (Table 2). Dyslipidaemia was least prevalent in the youngest age-group 20-29 years with 12.5% and increased rapidly in the group 30-39 years to 40.0%, and increased even further in the group 40-49 years to 56.7%, and in the 50-65 years it stabilized at 53.3%. Dyslipidaemia was prevalent in 31.3% of Black firefighters, in 42.9% of White firefighters and in 44.3% of firefighters of mixed ethnicity.
The mean BMI for all firefighters was 29.31±5.65 kg•m−2 (Table 3), and for male firefighters 28.66±5.30 kg•m−2, and for female firefighters 31.72±6.34 kg•m−2. There was a significant difference in BMI between male and female firefighters [U = 889.00, p=0.018]. The mean BMIs for the age groups 20-29 years, 30-39 years, 40-49 years, and 50-65 years were 25.65±3.56, 28.99±5.38, 31.38±5.38, and 32.18±6.36 kg•m−2, respectively. There was a significant difference in BMI between age groups [H(3) = 20.41, p<0.001]. The mean BMIs for White, mixed ethnicity and Black firefighters 30.79±5.88, 29.11±5.75, 28.94±5.44 and kg•m−2, respectively. There was no significant difference in BMI based on ethnicity [H(2) = 1.87, p=0.392].
CAD risk factor measurements according to demographic characteristics.

n=123 due to one firefighter not falling into the three-ethnic group
statistically significant differences <0.05
statistically significant differences <0.01.
The mean WC for all firefighters was 96.41±14.2 cm (Table 3), and for male firefighters 96.09±14.21 cm, and for female firefighters 97.59±14.37 cm. There was no significant difference in WC between male and female firefighters [U = 1229.50, p=0.785]. The mean WC of firefighters increased with age, with the age-group 20-29 years having 86.32±9.80 cm, the 30-39 years with 94.62±13.10 cm, the 40-49 years with 102.49±13.17 cm, and the 50-65 years with 106.90±14.39 cm. There was a significant difference in WC by age group [H(3) = 28.55, p<0.001]. The mean WCs for White, mixed ethnicity and Black firefighters were 100.63±13.48, 97.14±14.25, and 92.36±14.04 cm, respectively. There was no significant difference in WC based on ethnicity [H(2) = 5.92, p=0.052].
The mean WHR for all firefighters was 0.90±0.09, and for male and female firefighters, 0.91±0.08 and 0.85±0.66, respectively. There was a significant difference in WHR between male and female firefighters [U = 679.00, p<0.001]. The mean WHRs were age-related, and for age groups 20-29 years, 30-39 years, 40-49 years and 50-65 years they were 0.85±0.06, 0.88±0.65, 0.93±0.11 and 0.97±0.05, respectively. There was a significant difference in WHR between age groups [H(3) = 30.41, p<0.001]. The mean WHR for mixed ethnicity, White and Black firefighters were 0.92±0.09, 0.92±0.07 and 0.85±0.07, respectively. There was a significant difference in WHR between ethnic groups [H(2) = 15.99, p<0.001].
The mean SBP for all firefighters was 121.69±15.15 mm Hg, and the mean DBP was 77.10±11.69 mm Hg (Table 3). The mean SBPs for male and female firefighters were 123.06±15.29 mm Hg and 116.54±13.70 mm Hg, respectively, and the mean DBPs for male and female firefighters were 78.10±11.46 mm Hg and 73.31±11.95 mm Hg, respectively. There was no significant difference in SBP [U = 978.00, p=0.069] or DBP [U = 97.00, p=0.056]. The mean SBP and DBP for the age-group 20-29 years were 117.50±11.62 and 71.92±10.26 mm Hg, respectively. In the agegroup 30-39 years the mean SBP and DBP were 119.16±13.73 and 75.75±11.47 mm Hg, respectively. In the age-group 40-49 years the mean SBP and DBP were 127.93±16.73 and 83.33±12.04 mm Hg, respectively. And, in the age-group 50-65 years the mean SBP and DBP were 125.20±18.34 and 77.87±8.99 mmHg, respectively. There was a significant difference in both SBP [H(3) = 7.82, p=0.050] and DBP [H(3) = 12.44, p=0.006] based on age-group. The mean SBP and DBP for White firefighters were 123.24±13.78 and 77.62±8.73 mm Hg, mixed ethnicity firefighters were 121.63±14.89 and 78.89±11.86 mm Hg, and for Black firefighters were 121.19±16.99 and 72.81±12.36 mm Hg, respectively. There was no significant difference in SBP [H(2) = 0.51, p=0.774] or DBP [H(2) = 3.64, p=0.162] based on ethnic groups.
The mean NFBG concentration was 5.93±2.24 mmol•L−1 for all firefighters, with male firefighters having 6.01±2.48 mmol•L−1, and female firefighters having 5.65±0.95 mmol•L−1 (Table 3). No significant difference in NFBG was found between male and female firefighters [U = 126.00, p=0.961]. The mean NFBG was 5.81±0.93 mmol•L−1 in the age-group 20-29 years, 5.34±0.87 mmol•L−1 in the 30-39 years, 6.87±3.91 mmol•L−1 in the 40-49 years, and 10.63±2.16 mmol•L−1 in the 50-65 years. There was no significant difference in NFBG between age groups [H(3) = 5.56, p=0.135]. The mean NFBG concentration was highest in White firefighters with 6.47±4.08 mmol•L−1, followed by Black firefighters with 5.88±2.13 mmol•L−1, and lowest in mixed ethnicity firefighters with 5.78±1.41 mmol•L−1. There was no significant difference in NFBG between ethnic groups [H(2) = 0.28, p=0.871].
The mean TC was 4.92±0.96 mmol•L−1 for all firefighters (Table 3), and for male and female firefighters, 4.93±0.99 and 4.84±0.79 mmol•L−1, respectively. There was no significant difference in TC between male and female firefighters [U = 1255.50, p=0.909]. The mean TC concentration was 4.46±0.92 mmol•L−1 for the age-group 20-29 years, 5.03±0.92 mmol•L−1 for the 30-39 years, 5.13±0.96 mmol•L−1 for the 40-49 years, and 4.79±1.12 mmol•L−1 for the 50-65 years. There was a significant difference in TC between age groups [H(3) = 12.44, p=0.006]. Mixed ethnicity firefighters had the highest mean TC with 5.02±0.94 mmol•L−1, followed by white firefighters with 4.96±1.13 mmol•L−1, and black firefighters with 4.68±0.87 mmol•L−1. There was no significant difference in TC between ethnic groups [H(2) = 3.23, p=0.199].
Discussion
A total of 83.8 % of firefighters had at least one CAD risk factor, while 54.8% had at least two risk factors, and 36.3% had three or more risk factors. Additionally, 41.9% of firefighters were categorized as being at low-risk, 54.8% were categorized as being at moderate-risk and 3.2% were categorized as being at high-risk for CAD. Gendron et al. 4 reported a similar prevalence in Quebec firefighters, where 85% of firefighters had at least one risk factor and 59.1% reported two or more risk factors, placing them at moderate- risk. Similarly, Martin et al. 6 reported that 32.4% of firefighters in the United States (US) reported having zero or one CAD risk factor, 67.6% had two or more risk factors, and 51.4% had at least three or more risk factors. Smith et al. 1 reported 20.4% of US firefighters had zero or one risk factor, and that 45.9% of firefighters had two or more risk factors.
Among female firefighters, 38.5% reported a prevalence of one and 26.9% had two or three CAD risk factors, whereas only male firefighters had four or more risk factors. Gendron et al. 4 reported that 73% of female firefighters had at least one CAD risk factor, and 22% had at least two risk factors. Similarly, Wolkow et al. 5 reported that 46.6% and 26.6% of female and male Australian firefighters, respectively, had one or less risk factors, and that 50.8% of female firefighters had two or more risk factors compared to 68.2% of male firefighters. The present study, as well as previous literature indicate male firefighters more frequently have multiple risk factors and are at higher risk compared to female firefighters. 4,5
Firefighters categorized as moderate-risk increased with age, with the age-group 20-29 years reporting 29.2% with two or more risk factors, the age-group 30-39 years with 47.3%, the age-group 40-49 years with 76.7%, and the age-group 50-65 years with 80.0%. Byczek et al. 13 also reported that in the US, CAD risk generally increased as firefighters aged, with 74% of firefighters at moderate CAD risk in the age-group 30-34 years, 40% at moderate risk in the age-group 35-39 years, 51% in the age-group 40-44 years, 79% in the age-group 45-49 years, 67% in the age-group 50-59 years, and 87% in the age-group 60-64 years. Although Black firefighters reported the lowest prevalence of two or more CAD risk factors, the prevalence was still unacceptably high at 37.5%, followed by firefighters of mixed ethnicity with 60.8% and White firefighters with 66.7%.
Diabetes was the least prevalent CAD risk factor in firefighters, and in males only, especially above the age of forty years, and unrelated to ethnicity. Savall et al. 9 reported a similar low prevalence of diabetes in French firefighters, where 3.2% of firefighters had diabetes. The present study reported an absence of diabetes in female firefighters, while Wolkow et al. 14 reported that female firefighters had a slightly lower prevalence of diabetes compared to male firefighters (3.6% vs 6.8, respectively). Studies by Gendron et al.4,15 reported similar low results for diabetes prevalence in both genders, but with female Quebec firefighters slightly higher than male firefighters (3% vs 1.7%, respectively). With regard to ethnicity, Padela et al. 16 reported a similar prevalence of diabetes in the US across ethnic groups, as did the present study. Previous studies found no significant differences between diabetes and gender or ethnicity, however, a significant association was reported between diabetes and age in firefighters.1,17-19 The prevalence of diabetes can be attributed partially to the firefighters’ variable work schedules which, in most cases, demands a maximal response when dealing with an emergency. This, invariably, leads to increased stress, both physiological and psychological, and adversely impacts blood sugar levels.20,21 In addition, indulging in fast-foods tends to be the unhealthy first choice of many firefighters that aggravates their diabetes risk.4,9,20
The minority (13.7%) of firefighters were classified as physically inactive 11 in the current study, with the age-group 40-49 years the most likely to be physically inactive, for both genders and all ethnicities. Mehrdad et al. 22 reported a slightly higher prevalence of physical inactivity in Tehran firefighters at 23.8%. Eastlake et al. 18 reported a much higher prevalence for physical inactivity in US firefighter, with 62%, respectively. The present study reported a similar prevalence of physical inactivity for males and females in 13.3% and 15.4%, respectively. Gendron et al.4,15 reported that 62% of female firefighters were physically inactive compared to 70% of male firefighters. According to ethnicity, Poston et al. 16 reported a similar prevalence of physical inactivity in firefighters across various ethnic groups, similar to the present study. Although the prevalence of physical inactivity was not high in firefighters in the current study, it remains a cause of concern from both a public safety point of view, as well as from a personal health perspective. Therefore, encouraging physical activity among firefighters, who are at risk, will help to address physical inactivity as a modifiable CAD risk factor.2,3 The current study had a much lower prevalence of physical inactivity compared to previous literature and can be accounted for by the researchers using the IPAQ questionnaire as a means to categorize activity levels of the firefighters.
For family history, 20.9% of firefighters indicated a positive family history of CAD that was similar in both genders and related to advancing age in male firefighters. Martin et al. 6 reported a similar prevalence of family history in 25% of firefighters. Smith et al. 1 reported a much lower prevalence of family history in 5.2% of firefighters. Mehrdad et al. 22 reported a similar low prevalence of family history in 6.1% of firefighters. Gendron et al.4,15 reported a similar prevalence of family history as the present study, based on gender. Santora et al. 23 reported a much higher prevalence of family history in 38% of male and in 56% of female firefighters in the US. A positive family history of CAD in firefighters varied quite broadly among studies, ranging from 5% to 56%,6,9,24 and was likely due to differences in study sample size, gender, and age.
In the present study, 23.4% of firefighters had age (45 years or older) as a CAD risk factor, especially in White firefighters and those of mixed ethnicity, but was not significantly different between gender or ethnic groups. Martin et al. 6 reported that 35.1% of firefighters had age as a risk factor. Similarly, Savall et al. 9 reported 31.9% of firefighters had age as a risk factor. In contrast, Mehrdad et al. 22 reported only 11.6% of firefighters had age as a risk factor. According to gender, Gendron et al.4,15 reported that 45.3% of male firefighters had age as a risk factor compared to only 10% of female firefighters. Soteriades et al. 17 reported that aged firefighters (45 years or older) had a significantly higher prevalence of hypertension than their younger counterparts. Similarly, Eastlake et al. 18 reported that age in firefighters had a significant association with high blood cholesterol, high blood glucose and high blood pressure. Smith et al. 25 reported that as male and female firefighters aged, both genders had a significant increase in BMI, but only male firefighters had a significant increase in hypercholesterolemia, hypertension, and hyperglycaemia. The prevalence of aged firefighters varied considerably among studies and can be attributed to the individual sample sizes and regions where data was collected.4,6,9,15,17,18,22,25
Hypertension was present in 33.1% of firefighters, especially male firefighters older than 40 years, and in all ethnic groups. In previous studies, female firefighters were reported to have a lower prevalence of hypertension compared to male firefighters.4,14,15 Choi et al. 20 reported that 10.9% of US firefighters were hypertensive. Nor et al. 26 and Soteriades et al. 27 reported a similar prevalence of hypertension in 18.1% in Korean and 18.24% in US firefighters, respectively. Choi et al. 20 reported both systolic and diastolic blood pressures were significantly higher in older United States firefighters, and that the prevalence of hypertension significantly increased proportionately with age-group from 25-34 years (1.2%), 35-44 years (6.7%), 45-54 years (17.2%) to 55-61 years (35.0%). Soteriades et al. 17 reported that hypertension was significantly associated with increased age in firefighters. Factors related to the alarm response and emergency duties, such as 24-hour shifts, night shift, sleep cycle disruption, sleep deprivation, emotional and physical stress, and altered eating patterns caused alterations in the circadian rhythm of blood pressure in firefighters.20,28 Sleep deprivation, in combination with mental and physical stress, were significant causes of hypertension, especially in firefighters working 24-hour shifts, night shifts, and multiple shifts a month and exacerbated with increased age.20,28,29
In the current study, 37.1% of firefighters were obese, especially with central obesity in both female and male firefighters aged 40 years or older, and in all ethnic groups. Choi et al. 21 and Gendron et al. 4 reported a lower prevalence of obesity in 22.8% and 23.6% of firefighters, respectively. Choi et al. 30 also reported significant correlations between BMI, WC, and age in both male and female firefighters. Eastlake et al. 18 reported a prevalence of obesity in 33% of firefighters. Leary et al. 31 and Smith et al. 1 reported a higher prevalence of obesity in 46.8% and 51.7% of US firefighters, respectively. Choi et al. 30 reported that obesity significantly increased with age-group, i.e., the age-group 25-34 years had 7.8%, the age-group 35-44 years had 25.5%, the age-group 45-54 years had 33.6%, and the age-group 55-64 years had 38.1%. Clark et al. 32 reported an obesity prevalence of 29.8% in firefighters, with 2.3% being morbidly obese. The study also reported that DBP and cholesterol were significantly higher in obese firefighters. 32 Poston et al. 16 reported that firefighters of color in the US had significantly higher body mass indexes compared to White firefighters, whereas, Choi et al.21,30 reported that a higher percentage of White firefighters were obese compared to other ethnic groups in the United States. As previously stated, firefighters tend to indulge in high caloric, fat laden, fast-foods while on active duty, augmenting the accumulation of adipose tissue.4,9,20 Muegge et al. 33 found that a lack of knowledge was the most common barrier to weight management (19%) in firefighters, as well as a lack of access to low calorie foods (15.7%). Therefore, firefighters should be educated on weight management strategies and provided with easier access to low calorie food options, where possible.
Cigarette smoking was the second most prevalent risk factor in 39.5% of firefighters, especially in male firefighters who were White and of mixed ethnicity, and particularly in the youngest agegroup 20-29 years. In contrast, Gendron et al.4,15 reported that the prevalence of cigarette smoking was higher in female firefighters. Similarly, Jahnke et al. 34 reported that in the United states more female firefighters were smokers compared to male firefighters (22.2% vs 13.6%, respectively). Yoo and Franke 35 reported that tobacco use was most prevalent (40%) in the youngest age-group of under 30 years compared to the older groups of 31-42 years (32%) and 43-69 years (19%). Lima et al. 36 reported that 8.3% of White Brazilian firefighters were smokers, 6.8% of mixed ethnicity were smokers, and 9.3% of Black firefighters were smokers. Cigarette smoking prevalence in firefighters were higher in this study than previous studies on firefighters, which is a concern, as cigarette smoking is known to reduce peak work performance in firefighters.4,15,34,35 Firefighters should be encouraged to reduce their daily cigarette use, until complete cessation is possible.
Dyslipidaemia was the most prevalent CAD risk factor in 40.3% of firefighters in both genders and in all ethnic groups and increased with advancing age. Savall et al. 9 found that 19.5% of firefighters had elevated cholesterol levels. Similarly, Byczek et al. 13 reported a prevalence of hypercholesterolemia in 24% of US firefighters, and Martin et al. 6 reported that 29.7% of volunteer firefighters had dyslipidaemia. Leary et al. 31 reported a higher prevalence, where 46.7% of firefighters had high triglycerides, and 31.1% had low high density lipoprotein cholesterol levels. Gendron et al.4,15 reported that male firefighters had a higher prevalence of dyslipidaemia compared to females (17.4% vs 5%, respectively). Similarly, Santora et al. 23 reported that hypercholesterolemia was present in 46% of male firefighters and 11% of female firefighters. Cohen et al. 37 reported a prevalence of dyslipidaemia in 56.5% of firefighters and that is was significantly associated with age. Burgess et al. 38 reported that 26.97% of firefighters had high low density lipoprotein cholesterol (LDL-C) levels, and in the 45-year and older age-group, increased LDL-C was significantly associated with hypertension. Glueck et al. 24 reported that White and Black US firefighters had a similar prevalence of hypercholesterolemia. Poston et al. 39 reported that firefighters of color had a higher prevalence of hypercholesterolemia compared to White firefighters (32.7% vs 28.1%, respectively). Fast foods, which are firefighters first choice options are also high in saturated and trans-fatty acids, and are directly related to increased TC.4,18,40 Environmental and wildland fire smoke has been reported to cause an increase in oxidative stress and to increase certain serum haematological parameters, specifically TC, LDL-C, lactate dehydrogenase, creatine kinase and urea nitrogen. 40 These factors in combination may contribute to the high prevalence of dyslipidaemia in firefighters in the City of Cape Town.4,18,40
Strengths and limitations
This study provides valuable research data on firefighters according to gender, age and ethnicity in a scarcely studied area, especially in South Africa. This was the first study in South Africa to look at CAD risk factors in firefighters according to gender, age and ethnicity. The study is limited by convenient sampling and a small sample size, as prescribed by the municipal authority of the City of Cape Town, that negatively impacted the external validity. The study was also under-represented by female participants, and with only one firefighter of Indian ethnicity.
Recommendations
It is recommended that future studies use random sampling that would be sufficiently powered in order to ensure external validity. A more representative sample of female firefighters in the CoCT is recommended. In addition, a larger sample size is recommended to ensure greater statistical power and generalizability of the results.
Conclusion
Hypertension, obesity, cigarette smoking and dyslipidaemia were the most prevalent CAD risk factors among firefighters, with older males having the highest prevalence of multiple CAD risk factors, especially in firefighters who were White and of mixed ethnicity. Male firefighters were more likely to be smokers, hypertensive and diabetic. Female firefighters had a higher prevalence of obesity, especially central obesity. As firefighters aged the prevalence of the CAD risk factors increased, apart from blood glucose, similar to previous literature. Compared to other regions of the world, the City of Cape Town firefighters had a higher prevalence of dyslipidaemia and cigarette smoking, with most other CAD risk factors having similar prevalence's. The high prevalence of dyslipidaemia, cigarette smoking and obesity can be attributed to firefighters opting for high caloric fast foods due to their erratic work schedules. This study highlights the high prevalence of CAD risk factors in firefighters in the City of Cape Town and the need to promote regular CAD risk factor screening and to adopt behavioural strategies to ameliorate CAD risk prevalence in firefighters.
Footnotes
Acknowledgments
We thank the City of Cape Town for granting permission to conduct the study, and to Mr Ian Bell for supporting the study from the start to the end. To each District Head and Station Commander that allowed testing and to every firefighter that voluntarily participated in the study.