
Abstract
Keywords
Introduction
Elevated blood pressure (BP) is an important epidemiological concern because of its rising prevalence in many adult populations around the world.1,2 Hypertension (HT) is a well-known risk factor for cardiovascular disease and has been associated with increased mortality and morbidity.1-4 Past studies have established clear associations between anthropometric measurements and elevated blood pressure.5-10 These associations have been linked to the presence of obesity and metabolic syndrome, entities also relevant to cardiovascular morbidity and mortality.11-16
The Guatemalan region of Sololá consists of the territory surrounding Lake Atitlán, located in the western part of the country. Most of this area is rural tropical mountainous country with difficult vehicular access. The remoteness of the area has promoted cultural uniformity in its populations. However, there seems to be a slow but increasing rate of societal interchange with other ethnic groups in the country. According to government data, 17 approximately 94% of the inhabitants of these regions are indigenous and form part of 1 of 4 Mayan ethnic subgroups: Cakchiquel, Tzutujil, Quiche, or Mam. Little is known about the genetic background and epidemiological data of HT and cardiovascular disease in these populations.
Previous studies in Guatemala describe a low prevalence of HT in the rural (3.93%) and urban (9.39%) areas of Guatemala, although this study included a majority of women (61% of 1517, of whom 825 were categorized as “rural”) and only subjects 19 years or older. 18 The CAMDI study reported a hypertension prevalence of 17.1% using a sample of 1397 subjects, age 20 years or older, from the urban region of Villa Nueva. 19 However, cumulative evidence suggests that there is a trend of increased prevalence of HT and cardiovascular disease in developing countries.19-21 It is important to understand the magnitude and characteristics of this epidemiological transition in the indigenous population of Guatemala to consider possible public health interventions.
Objectives
In this study, we measured the blood pressure, body mass index (BMI), and waist circumference (WC) in the adult indigenous population of Sololá. In addition, we determined the prevalence of HT in the region and the associations between HT, place of residence, and increases in BMI and WC.
Methods
Medical research in rural Guatemala is difficult to perform because communities are geographically isolated and medical services are scarce and uncoordinated. Even official population and health data are often imprecise and useless to plan research. We obtained a sample size of 1104 subjects (552 men and 552 women) for the entire population of Sololá, estimated at 170 588 adults by the National Statistics Institute in 2006. 17 Subjects were randomly chosen via a combined geographical cluster and quota sampling methods. The total sample size was distributed in quotas corresponding to the 19 official municipalities in Sololá, subsequently substratified into the largest 50 communities within those municipalities, according to population data obtained from municipal and state officials. Criteria for inclusion involved both men and women, 18 years or older, who were born and resided in the municipal region in which they were to be sampled by the data collection team. This sampling was done by the data collection team visiting the rural community and the subjects in their homes. Subjects were asked to participate if they fulfilled inclusion criteria and were willing to give informed consent. Only 2 female subjects refused participation and were excluded from the sample. All subjects were included without regard to past medical history or current treatment for HT. It is important to note that in this part of Guatemala a very low proportion of the adult population has formal contact with medical services. A digital photograph archive was kept and revised during analysis for all 1104 subjects in order to verify consistency of the data and the measurement methodology. Subjects found to be hypertensive had referrals to national health posts, but not all accepted such referrals.
Measurements
Seventeen trained general practitioners in supervised rural practice collected the data. They lived among the rural communities of Sololá for three weeks in order to complete the sample size. BP was measured in the subject’s home by a designated team member, once on each arm following standardized methods 22 using calibrated mercury sphygmomanometers. The subjects had at least a 5-minute rest period before BP measurements and were told to refrain from smoking and caffeine for 30 minutes. The higher of the 2 measurements was recorded and confirmed by a second data collection team member. Korotkoff phase V was used for diastolic blood pressure recording and measurements where rounded to the nearest 2 mm Hg. Standing height was measured in centimeters rounded to the nearest centimeter, with shoulders and buttocks against a vertical surface, the subject looking straight ahead, with joined feet, and arms hanging on both sides. Body weight was measured in kilograms with calibrated portable scales placed on an even surface. Waist circumference was obtained with a graduated flexible nonelastic tape with subjects in standing position and the measurement made at the horizontal iliac crest level. BMI was calculated for each subject as kg/m2.
Diagnostic Criteria
Hypertension was defined as a systolic blood pressure (SBP) level ≥140 mm Hg and/or a diastolic blood pressure (DBP) level ≥90 mm Hg. Subjects were also classified as hypertensive if current pharmacological treatment for HT was reported. An elevated WC was defined as ≥80 cm for women and ≥94 cm for men, as per the International Diabetes Federation 2006 definition. 16 Subjects with BMI ≥25 kg/m2 were classified as having elevated BMI and subclassified as overweight if BMI was ≥25 but <30 kg/m2 and obese if BMI was ≥30 kg/m2.
Statistical Analysis
Data were collected in paper format and organized in a Microsoft Excel database where BMI, mean arterial systolic, diastolic, and pulse pressures were calculated for all subjects. All analyses were performed using Stat Soft 2009 software. To evaluate differences in parameters between genders, Student’s unpaired t test was used. Percentages were compared using the χ2 test. Logistic regression was used to obtain odds ratios (ORs) and 95% confidence intervals (CIs). The statistical models used included the entire population and subgroup analysis for gender, controlling for sex, age, BMI, and WC accordingly to obtain an OR for hypertension for each risk factor. A P value ≤.05 was considered statistically significant.
Results
Blood Pressure Measurements
The mean arterial blood pressures (MAPs) found in this study are reported in Table 1. The average SBP and DBP levels were 115.05 and 73.97 mm Hg, respectively. Men had statistically significant higher average SBP, DBP, and MAP levels (116.24 vs 113.8 mm Hg, 75.24 vs 72.69 mm Hg, and 88.91 vs 86.39 mm Hg, respectively). Blood pressure levels <120/80 mm Hg were found in 716 subjects (384 women, 332 men). This corresponds to 69.1% of women and 60.1% of men with optimal blood pressure as per the seventh report of the Joint National Committee (JNC-7) categorization of BP. 23
Blood Pressure and Anthropometrics in the Adult Indigenous Population of Sololá, Guatemala.
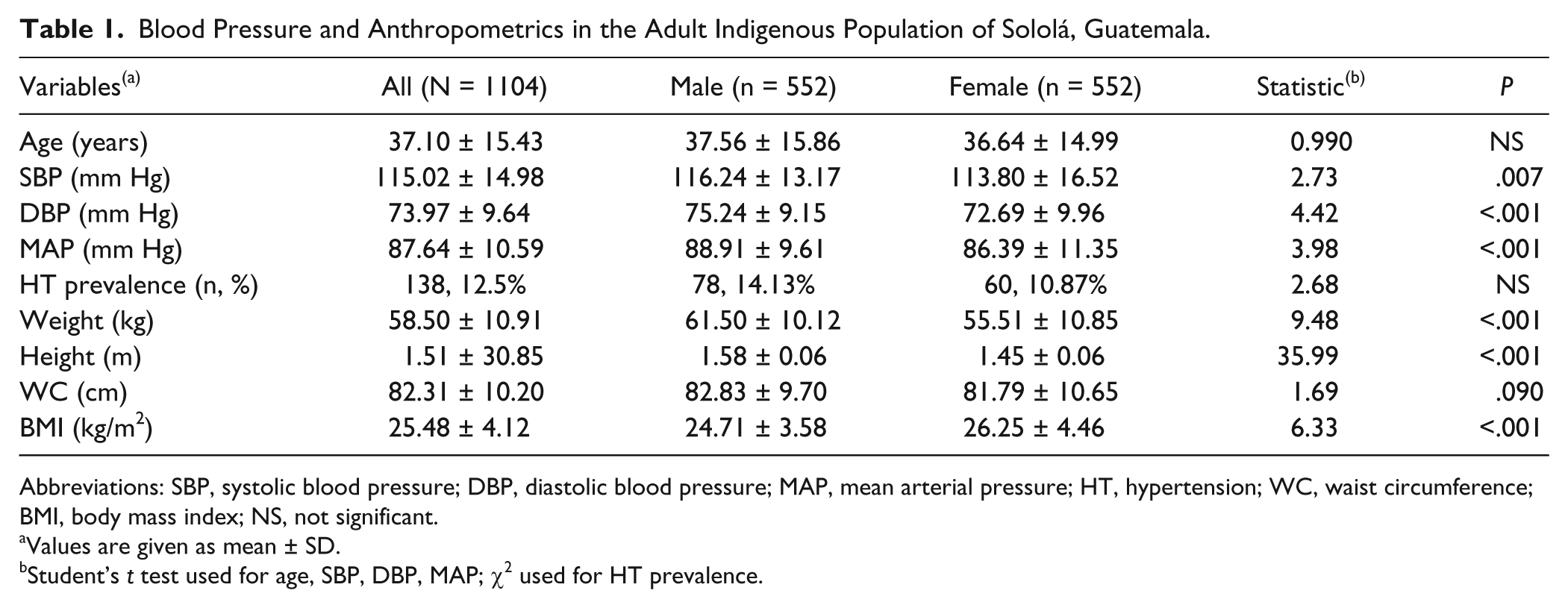
Abbreviations: SBP, systolic blood pressure; DBP, diastolic blood pressure; MAP, mean arterial pressure; HT, hypertension; WC, waist circumference; BMI, body mass index; NS, not significant.
Values are given as mean ± SD.
Student’s t test used for age, SBP, DBP, MAP; χ2 used for HT prevalence.
Anthropometric Measurements
The mean (±SD) BMI for the entire population was 25.48 (±4.12) kg/m2. Women had a significantly higher mean BMI than men (26.25 vs 24.71 kg/m2, P < .001). Weight, height, and WC measurements were higher in men when compared with women (see Table 1). The mean WC for men was 82.83 ± 9.7 cm and for women it was 81.79 ± 10.65 cm. An increased WC was found in 70 men and 279 women, with a prevalence of 12.7% and 50.5%, respectively (Table 2).
Age, BMI, and WC in the Adult Indigenous Population of Sololá, Guatemala.

Abbreviations: BMI, body mass index; WC, waist circumference; NS, not significant.
Elevated WC was defined as ≥80 cm for women and ≥94 cm for men, as per the International Diabetes Federation 2006 definition.
Hypertension Prevalence
The crude prevalence of HT was 12.5% (see Table 1). When comparing genders, HT was more prevalent in men than women (14.13% vs 10.87%), but this was not statistically significant (χ2 = 2.68, P = .101). JNC-7 classification stage 1 hypertension was found in 37 women and 64 men. Hypertension stage 2 was found in 23 women and 14 men. Overall, 73.2% (101 of 138) of hypertensive subjects can be classified as JCN-7 stage 1.
Association Between Blood Pressure and Anthropometrics
The results obtained show significant associations between increments in age and WC and the presence of HT, but not for increments in BMI. Logistic regression was used to calculate ORs for HT, controlling for sex, BMI, elevated WC, and age ≥55 years. These ORs show the possible risk associations regarding each variable in an unadjusted (see supplementary material, available at http://jpc.sagepub.com/content/by/supplemental-data) and adjusted model (see Table 3).
Adjusted Odds Ratios for Hypertension and Associated Risk Factors.

Abbreviations: OR, odds ratio; CI, confidence interval; BMI, body mass index; WC, waist circumference; NA, not applicable.
aC resident refers to subjects residing in Sololá’s capital city.
Discussion
Prior studies have demonstrated an association between anthropometrics and blood pressure levels, but the details of this association are not well defined.24,25 The data presented here show that these associations are also present in the rural indigenous population of Guatemala, where the prevalence of raised BP, BMI, and WC was highly underestimated in the past. This study shows that HT is present and poses risks in rural indigenous Guatemala, an underserved population in whom HT and associated risk factors are scarcely recognized. Men, as in other regions around the globe, 1 had a higher prevalence of HT and had an increased risk of HT (OR 2.19, 95% CI 1.44-3.40).
The prevalence of HT is higher than that of both Official Epidemiology Reports and other investigators that have reported for rural and urban Guatemalan populations. 18 Although the arbitrary definitions of “urban” and “rural” segments of the population are difficult to define in developing countries, analysis of place of residence (capital region of Sololá vs rest of the department) demonstrated here an inverse relationship with associated HT (OR 0.56, 95% CI 0.34-0.94) so that noncapital subjects were at higher risk. This relationship was also statistically significant in the female subgroup (OR 0.34, 95% CI 0.13-0.84). A better estimate of the true burden of cardiovascular risk factors is imperative to efficiently allocate public health resources in Guatemala.
The single most important isolated risk factor was age for women (OR 6.76, 95% CI 3.59-12.72) and WC for men (OR 3.23, 95% CI 1.52-6.87). Increased BMIs alone (BMI ≥25-30 or ≥30 kg/m2), when controlled for other confounders, are not significantly associated with HT in any group. BMI and WC measurements are easily obtained “low-tech” clinical evaluation tools. Their use as a screening tool for indigenous populations at risk for HT and cardiovascular disease still needs to be evaluated. These methods might aid in the detection and treatment of HT in regions where medical access, not to mention CVD risk assessment, is very difficult. We believe these types of interventions are important, especially in underdeveloped regions where full-blown and uncontrolled incidence of cardiovascular disease would be disastrous to the economic livelihood of these populations.
Footnotes
Acknowledgements
The authors wish to thank the invaluable collaboration of the members of the Hipertensión Arterial en Adultos de Sololá (HAAS) study group. Also, we would like to thank Shengping Yang for his statistical assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.