
Abstract
Aims: The article examines whether preventive measures and work adjustments at the establishment level affects sickness absence among workers aged 50 years and older. Methods: We combine survey data from a representative sample of 713 Norwegian companies, mapping the prevalence of preventive health measures in the work place in 2005, with register data on sickness absence and demographic variables for workers aged 50 years or older in 2001 and 2007. By means of a difference-in-differences approach, we compare changes and differences in the likelihood of sickness absence among the sample group, with and without the various measures/ instruments in 2005 respectively. Results: In general, work-place preventive measures at the establishment level have not contributed to reducing the probability for sickness absence among workers aged 50 years and older. However, analyses comparing differences between industries find that the work-place measures have had a positive effect on public administration employees.
Background
In Norway, the employment rate among older workers is one of the highest in Europe. Almost 70% in the age group between 55 and 66 years are employed [1]. At the same time, sick leave rates in this age group are also among the highest in Europe [1]. Over the past decade, it has been a high priority for politicians to reduce sickness absence in Norway. An Inclusive Working (IW) life agreement (IA-avtalen) has been signed by the government and the social partners, committing them to reduce sickness absence rates by 20% from the 2001 rates [2]. Many enterprises have also signed up for this agreement, and the number is growing [3], committing employers to work to reduce sickness absence in their establishments. Different measures have been implemented by the government, such as earlier and more continuous attention to workers on sick leave and increased use of graded sick leave [4,5]. In addition, employers’ and employees’ organizations have been campaigning to get more establishments to join the IW-agreement and to continue employing measures to prevent health problems among older workers and to facilitate work for employees with poor health and reduced work ability.
Sick-leave rates vary between sectors and industries and between different groups of workers [6,7]. Rates are high in health and care services compared to other industries. Rates are also higher in manual industries such as construction, transportation and hotels than in information, communication, finance, insurance and public administration. In addition, women have higher sick-leave rates than men, and sick-leave rates increase with age and decrease with increasing levels of education [6,7].
Knowledge on individual’s sick-leave risks is well established [8–11]. However, to what extent sick leave is work-related remains unclear. Estimates for this vary, depending on whether physicians or workers are being asked, and estimates also vary according to diagnoses [12–16]. However, it is generally assumed that work conditions cause about half of all sick leave [7], implying that there may be a large potential for reducing sickness absence by means of applying preventive work-place measures.
A meta-analysis comprising 84 different studies of sick leave found that the relationship between physical work environment and sick leave was well documented, pointing especially to ergonomics [17]. High levels of work autonomy have also been found to reduce sick-leave rates. The relationship between high work demands and sick leave is unclear, as is the role of in-work social support. Although there is a relationship between work-environment and sick leave, part of this correlation can be attributed to socio-economic differences, as workers experiencing poor working environments often are less educated, which again is correlated with bad smoking, drinking, nutrition and exercising habits. These are all are factors known to increase the risk of sick leave. Low socio-economic status is therefore in itself correlated to sick leave and other health risks [18]. In addition, several studies have found that establishment down-sizing increases self-reported bad health, which increase the sick-leave risk, particularly among older workers and among workers with previously-known health problems [18 –24].
Knowledge on how to prevent work-related sick leave is scarce [7]. Some studies have found the IW-agreement to influence sick leave levels, others that it does not [6]. However, these studies have applied designs and methods that are less suited to identify the causes behind observed outcomes as they are either based on a very limited sample of enterprises, on aggregated data, or on limited time periods.
The aim of this study is to investigate whether the introduction of work-place preventive measures, initiated and financed by the establishments influence the individual probability of sickness absence among elderly workers. Such measures are of particular interest since absence reduction is one of the main goals of the IW-agreement.
Data and methods
We analysed data from two separate sources; a survey on a random sample of Norwegian establishments, and register data on all employees aged 50 years or above in these establishments. The survey was carried out among 713 establishments which had at least 10 employees and at least one employee aged 60 years or above in 2005. The sample was stratified according to industry and establishment size [25]. The survey, with a response rate of 73%, comprises information on different work-place measures employed to facilitate work for employees with poor health and/or reduced work ability, as well as other establishment characteristics. Data on individual characteristics, work and sickness absence was drawn from Statistics Norway’s (SSB) registries. The data analysed comprised all employees who were 50 years or older in 2001 and in 2007, respectively.
The dependent variable was sickness absence certified by a physician and lasting for more than 16 days. Shorter periods of sickness absence were not registered in our data. The wage costs related to absences lasting for between 16 consecutive days and up to 52 weeks is reimbursed by the Norwegian Labour and Welfare Administration (NAV). The data were recoded into a binary variable indicating whether individuals had at least one sickness spell in either 2001 or 2007 lasting for more than 16 days.
Our principal independent variable was whether establishments have initiated arrangements to facilitate work among employees with health problems or reduced work capacity. Information on the presence of such measures in the work-place was included in the 2005 establishment survey. However, we do not know exactly when these different measures were introduced. Other studies however have shown that most establishments have increased their efforts to lower sickness absence following the start of the IW-agreement in 2001 [9]. We therefore assume that there has been a similar increase in use of measures in the participating establishments since 2001, i.e., that a large share of establishments which stated that they had measures in place in 2005 did not have them in 2001. In 2007, a total of 41% of employees worked in establishments with arrangements to facilitate work among employees with health problems or reduced work capacity. The work-place measures include for instance work adjustments by e.g. use of technical aids or change of occupation or working tasks.
The trends in sick leave rates in establishments with and without preventive measures in 2005 were similar in the period 2001–2005 (data not shown). To investigate whether work-place measures have an effect we therefore used a quasi-experimental design, where we compared changes in the likelihood of sickness absence over time between individuals with and without access to preventive work-place measures. This approach, called difference-in-differences, is considered one of the best available methods for measuring actual effects of interventions and regulatory changes [26,27].
In our analysis, we compared individual sickness absence probability in 2001 with sickness absence probability in 2007, among individuals in enterprises with and without work-place measures. One feasible approach could have been to follow all employees from 2001 onwards and study their sickness absence levels. However, this would have increased the risk of a “healthy worker” selection bias where attrition in terms of work-exits among employees with a bad health, leaving the healthiest employees in the 2007 sample. To avoid this bias, we analysed two pooled cross-sections comprising all employees aged 50 years and older in the 713 surveyed establishments in both 2001 and 2007, comprising 14,261 and 18,960 individuals, respectively, in sum 33,221 individual records.
We included controls for the following individual characteristics: gender (reference = male) and age (ref = 50 years) including a second order polynomial to allow for non-linearity. In addition we adjusted for education, categorized as compulsory school (= reference), upper secondary school, lower level university or college education, and higher-level university or college education. Income, after tax, was measured in percentiles, thus measuring the effect of relative placement in the income distribution. For partly disabled individuals we included degree of disability, which was a factor that could affect sickness absence probability.
All information pertaining to the different establishments originated in the survey conducted in November and December 2005. All establishment variables were categorical. We included the major industries: manufacturing (= reference), construction, retail, hotels and restaurants, public administration, education, health and social services, and “other” industries. The establishment size dummy indicated whether there were more than 230 employees or not (= reference). In addition, we adjusted for dummies on whether the establishments had a human resources (HR) professional or not (= reference), whether they were exposed to competition or not (= reference, e.g. public sector) and whether they had experienced downsizing through 2001 to 2005 or not (= reference).
In addition, adjusting for participation in the IW-agreement was important since such establishments have access to services and benefits which are not available to other establishments. IW-establishments have a designated contact at the Norwegian Labour and Welfare Administration (NAV), and could utilize e.g. graded sick leave without preliminary approval [4]. Finally, we adjusted for whether the establishment became an IW-establishment in 2001, 2002–2005, or did not join the agreement (= reference).
The dependent variable in our analyses was a binary categorical variable, thus we used logistic regression. We report odds ratios (OR) with 95% confidence intervals. As an additional control, we have also used linear probability models, which substantiate our reported estimates. Stata, version 10.1, was used for the statistical analysis.
We started out investigating the overall effect of work-place measures by only including the measure and a year-dummy, as well as an interaction between work-place measure and year (i.e., the measure effect). This gave a “gross” effect of the measure. However, it is unlikely that establishments with and without measures are similar in all manners. It is also unlikely that their respective employees are similar. Thus, we have a model were we adjusted for individual (employee) characteristics, and a model were we adjusted for establishments characteristics, and finally a model with both employee and establishment characteristics.
Results
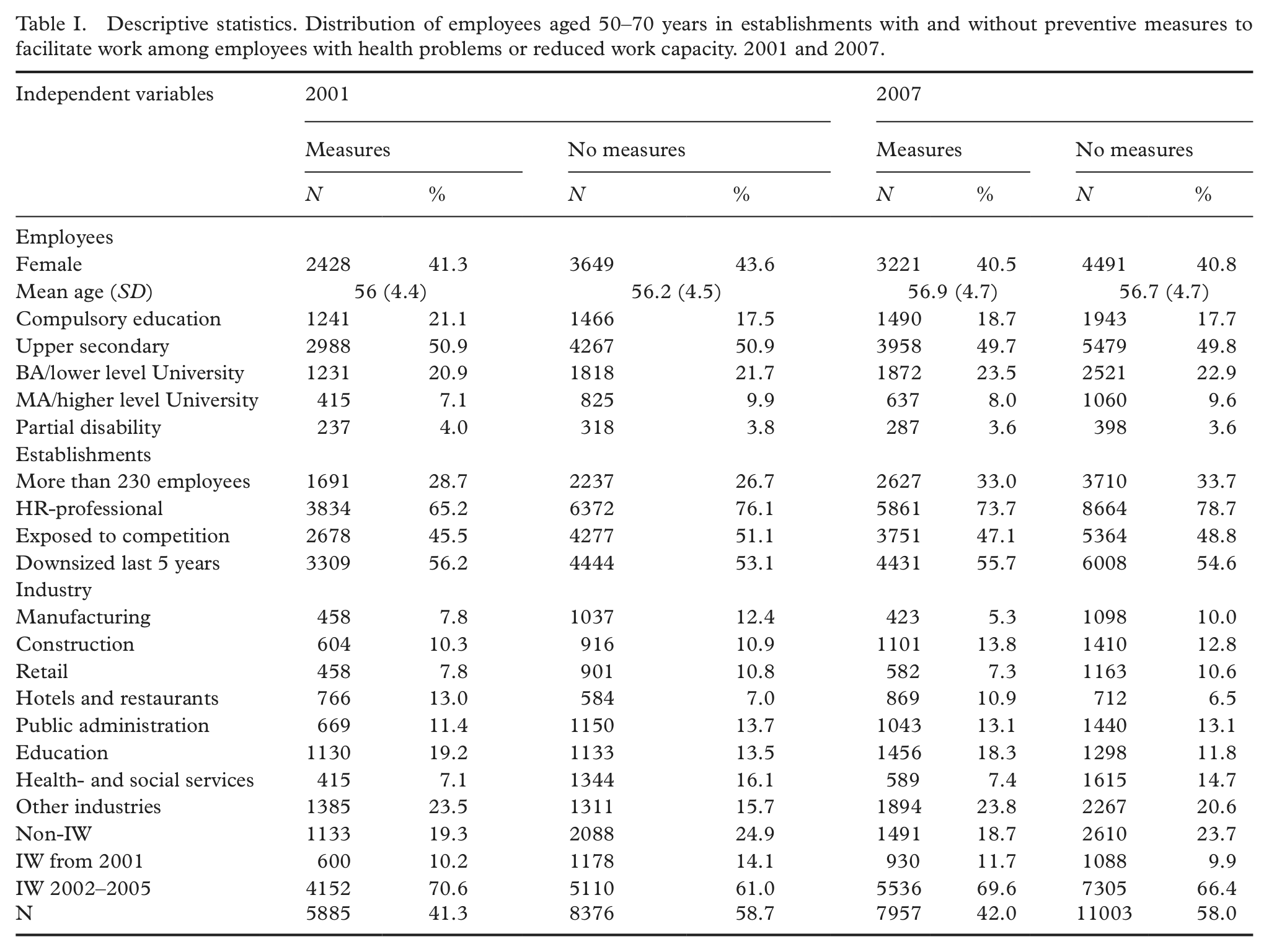
In both 2001 and 2007, establishment with and without preventive measures were similar regarding the distribution of gender, employees’ mean age (and SD), educational level and percentage being partly disabled (cf. Table I). The share of large establishments was about the same in both groups, as was the share of private sector, competition exposure and downsizing experience. However, the share of establishments with an HR-professional was somewhat higher among establishments with preventive measures in place. The largest differences between the two groups concern industry and the share of IW-establishments. Previous research has indicated that there is a correlation between having preventive measures and being an IW-establishment [28,29]. The somewhat larger differences between establishments with and without measures between industries may indicate that there is some self-selection among establishments regarding which industries employ measures. However, the variation is not very substantial, and we control for industry in the initial analyses and perform separate analyses by industry in later analyses. In addition, there is, in our view, no reason to expect individual employees to self-select into establishments with measures.
Descriptive statistics. Distribution of employees aged 50–70 years in establishments with and without preventive measures to facilitate work among employees with health problems or reduced work capacity. 2001 and 2007.
In the unadjusted model, the odds for sickness absence is about 20% higher for employees in establishments with measures compared to establishments without such measures (cf. Model 1 in Table II). This may indicate that such measures were initiated in establishments where they were most needed. However, the trends in sick-leave rates in establishments with and without preventive measures were similar in the period 2001–2005.
Logistic regression models (ORs with 95% CI) on the risk of sick leave. Adjusted for individual and establishment characteristics.
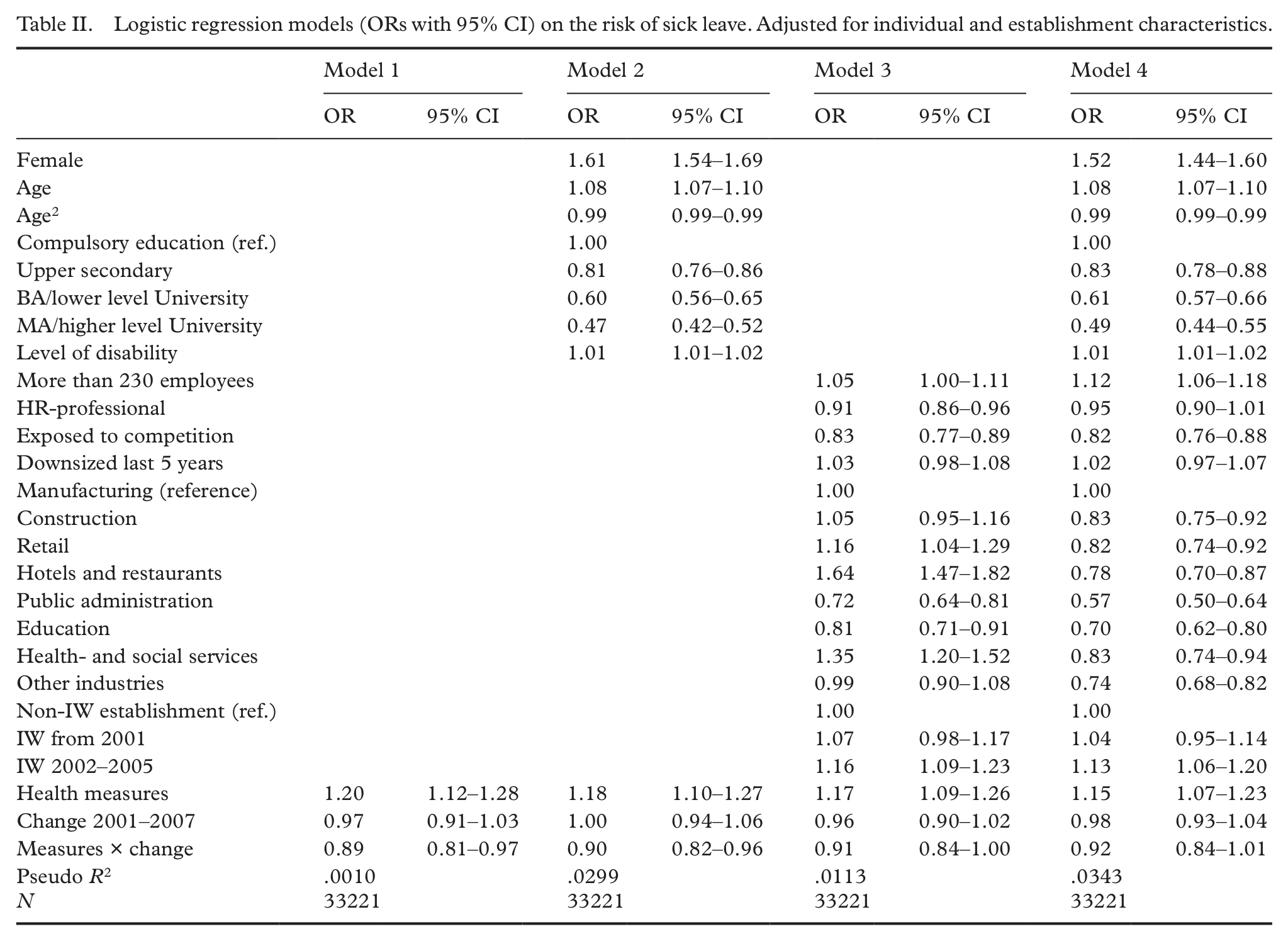
Whereas individuals in establishments without measures experienced no change in sickness absence levels, employees in establishments which initiated such measures experienced a 10% drop in the odds for sickness absence in the period from 2001 to 2007. This suggests that such measures can be efficient means to reduce sickness absence levels.
Adjusting for individual characteristics (Model 2) does not alter this finding, however adjusting for establishment characteristics (Model 3), or establishment and individual characteristics (Model 4), we find that the unadjusted effects of the measures can be accounted for by establishment characteristics, and not by the work-place measures themselves.
Although work-place measures targeting elderly workers do not influence sickness absence among the oldest workers, we find that both individual and establishment characteristics matter. The probability for experiencing a spell of sickness absence lasting for more than 16 days is high for women and low for the highly educated. The risk increase with age, but the second-order term implies that the effect diminishes with increasing age. Employees with some disability are more prone to experience sick leave, which is to be expected. Sick-leave levels are the highest among employees in manufacturing, construction and in health- and social services. Levels are high in large establishments and low in establishment exposed to competition. The presence of an HR-professional, having experienced a down-sizing within the last 5 years and being an IW-establishment, however do not have a significant impact on individual sick leave probability.
We have seen that sickness absence varies by industry. We therefore ran the analysis in Table II separately by industry (cf. Table III).
Logistic regression models (ORs with 95% CI) on the risk of sick leave. By industry.
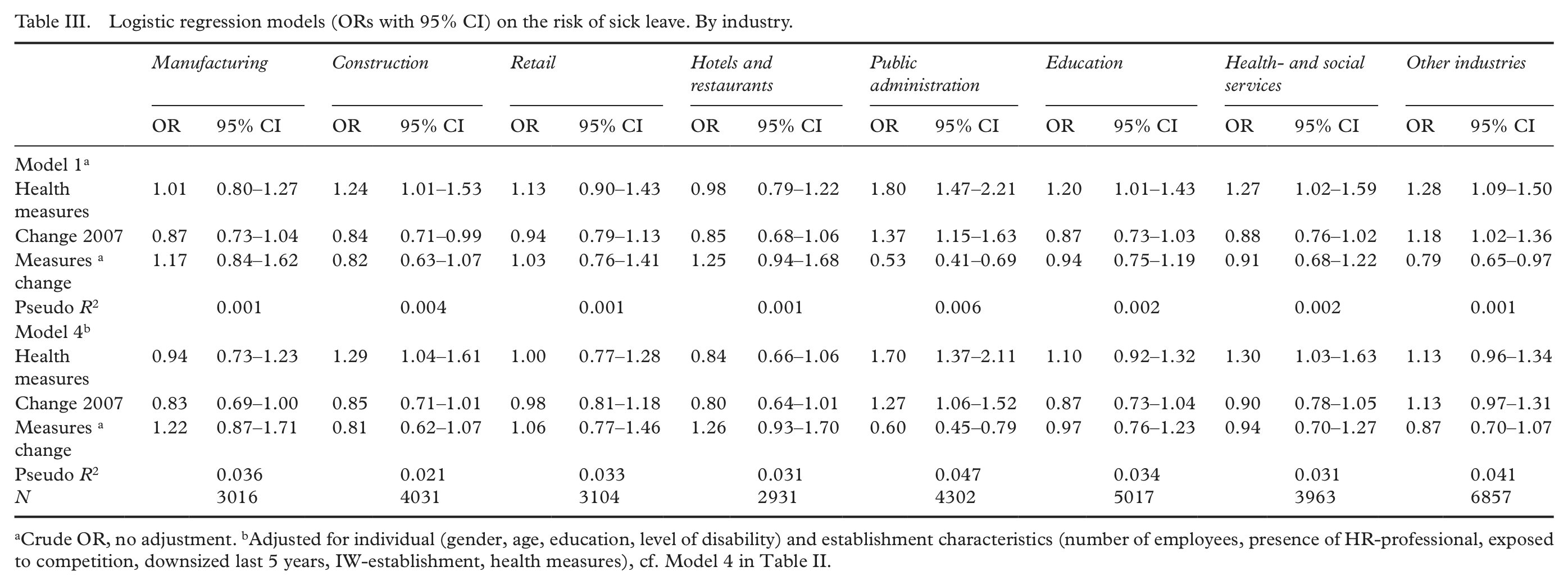
Crude OR, no adjustment. bAdjusted for individual (gender, age, education, level of disability) and establishment characteristics (number of employees, presence of HR-professional, exposed to competition, downsized last 5 years, IW-establishment, health measures), cf. Model 4 in Table II.
Our results suggest that in public sector establishments with available measures, the measures themselves have contributed to reducing sickness absence among employees aged 50 years or older. This effect is not found in any other industry.
Discussion
Work-measures have an effect on sick leave among employees aged 50 years or older in public administration establishments, not in other industries. Our analysis do not answer why measures’ efficiency vary by industry. In light of previous case studies [3], it is, however, reasonable to attribute this variation to difference in work conditions between industries. Office and executive work is more easily carried out when feeling ill, than in manually and physically demanding work. In addition, office work is more adaptable to individual illness by means of reducing work load, moving deadlines, and even the place where the work is carried out can be flexible. For work in other sectors, you often have to be present at a set location at a certain time in order to carry out the job. This pertains to for instance teaching and health professions and to retail work. These professions often have to relate to customers and users, which may give less scope to adjust work content. Also, office employees are (normally) not part of a larger production chain, where e.g. machines determine work speed.
Thus, we find that what primarily drives sickness absence rates are differences in gender, age, education levels and level of (partial) disability, which corroborates previous research. In addition, industry, establishment size, and exposure to competition are important factors. Also, establishments which joined the IW-agreement at a later stage (2002–2005) have higher sick leave levels compared to both establishments participating from 2001 and establishments outside the IW-agreement. This suggests that high sick-leave rates among employees may motivate an enterprise to join the IW-agreement.
Lower levels of sickness absence prevalence in small establishments may be attributed to factors such as social control, i.e., that each employee is relatively more important in smaller establishments where (at least perceived) production/output will suffer more compared to larger establishments, making the threshold for staying away from work higher. When employees in competitive establishments have lower sick-leave rates, this might be caused by raised awareness about the economic consequences sick leave may have on the economic sustainability of the establishment. Although the wage costs related to sick leave is reimbursed, there may be other costs to the employer when someone is absent, such as reduced productivity. Considering previous research, it is somewhat surprising then that experiencing downsizing and the presence of an HR professional in the establishment has no bearing on sickness absence rates. The former might be explained by the age groups included in our study, and that seniority will, at least in a Norwegian setting, legally “protect” older employees from layoffs. In addition, when downsizing, establishments may offer severance pay to elderly workers with bad health, thus remaining employees are healthier.
Methodological considerations
This study investigates whether preventive work-place measures targeting elderly workers with poor health and/or reduced work ability have an effect on reducing sickness absence levels. This study does not explore whether such measures have an effect on the length of the absence, or the number of sickness absences during a year. Future research may want to investigate this. In addition, future surveys may target the employees, rather than the establishment, to investigate whether eligible employees actually have been offered measures aiming to reduce sickness absence.
In the analyses, we had no access to data that allowed us to control for differences related to individuals’ health status, working environments and working conditions. These are factors which previous studies have demonstrated influence sickness absence [17]. It is possible that working conditions and working environment in enterprises that offer facilitation and/or special initiatives for seniors are on the whole less favourable than in enterprises that do not provide such initiatives, thus providing an explanation for the absence of any effects. This means that the initiatives may have an effect, but this is not sufficient to counterbalance the negative effect of working environment. We control for level of education and industry in our analyses. However, this may not capture all the differences in working conditions between individuals working in the same types of industries, who may be working in a variety of occupations.
Conclusion
By means of a difference-in-differences estimator, we have investigated whether establishments’ measures targeting elderly workers with poor health and/or reduced work ability have reduced individual sickness absence levels from 2001 to 2007. In our models, this estimator is adjusted for individual characteristics (gender, age, education, and disability level) and establishment characteristics (sector, industry, size, IW-agreement participation, HR-professional, downsizing experience and exposure to competition).
Overall, sickness absence levels has decreased more in establishments with preventive measures, but our analysis show that this decrease is not due to the measures themselves, but rather to other establishment characteristics. However, analyses by industry show that the measures have been effective among public administration employees, suggesting that measures’ efficiency may be related to the amount of physical labour, and that in manual occupations work adjustments for employees with poor health and/or reduced work ability may be more difficult to introduce.
Future research should investigate whether such measures have an impact on the number of sick days, and it might be of special interest to focus on long term absence. Most reimbursed sick leave lapses are relatively short. However, about half of all sick days are due to less than 10% of lapses [30]. In addition, it may be important that future research carry out more differentiated analyses of the specific measures since some of the measures may be more efficient than others in reducing sickness absence.
Footnotes
Acknowledgements
The authors would like to thank Åsmund Hermansen, Anne Hege Strand and the anonymous referee for comments and suggestions.
Conflicts of interest
None declared.
Funding
The project was financed by FARVE – forsøksmidler arbeid og velferd (The Norwegian Labour and Welfare Administration).