
Abstract
Aims: The impact of indoor mould on employees’ long-term absence from sickness (more than 10 days of absence) is poorly understood. This paper examines whether self-reported mould was related to long-term absences from work between 1 and 3 years later. Methods: By using negative binomial modelling, we analysed a representative sample of the working-age population in Finland (N = 16,084) from the Finnish Quality of Work Life Surveys in 1997, 2003, 2008 and 2013 combined with the register-based follow-up data of participants’ long-term sickness absences covering a period of 1 to 3 years after the Finnish Quality of Work Life Surveys was collected. Results: After all necessary background, work- and health-related factors were included in the model, employees who reported mould in their work had 1.20 higher rates of long-term sickness absence than those who did not report mould (mould: estimated marginal mean = 13.45 days; no mould: estimated marginal mean = 11.23). If employees perceived that mould caused strain, they had 1.30 higher rates of long-term absence than those who did not report such strain (mould caused strain: estimated marginal mean = 14.64 days; mould did not cause strain: estimated marginal mean = 11.25). In total, 10% (N=1628) of employees reported mould in their workplace and 6% (N=987) reported that mould caused strain.
Keywords
Introduction
An increasing amount of the world population works indoors. It is well known that exposure to chemical and biological factors in indoor environments can adversely affect employees’ health. For example, there is cumulative evidence that dampness and mould are associated with asthma and other respiratory illnesses and symptoms [1, 2]. It is estimated that over 2 million healthy life years are lost annually in European Union countries due to exposure to chemical and biological factors germane to indoor environments [3].
In addition to health, the extant literature shows that poor indoor environmental quality is linked to increased sickness absences from work, which has a further negative impact on productivity [4–8]. The primary focus of the literature has been attentive to the relationship between poor ventilation and absence [5, 8]. For example, Fisk et al. (2011) estimated that increasing ventilation rates to 15 L/s per person would avoid 10 million days of short-term absence in the USA [9]. In addition, the association between building-related symptoms (i.e. sick building syndrome) and sickness absence has also received considerable attention [4, 6]. These mainly cross-sectional studies have suggested that self-reported building-related symptoms and absences are significantly related. The impact of dampness and mould in the workplace on sickness absences is, however, seldom analysed despite the effects it has on health [1–2]. To our knowledge, there has been only one published study in the English language that has reported an association between self-reported mould and absences [7]. Based on this research, Fisk et al. (2011) have estimated that reducing just 30% of the damp and mould in US office buildings would result in an annual reduction of 1.5 million absence days [9].
Aims
Hitherto, the scholarship considering indoor environmental quality has rarely focused directly on long-term sickness absences. This study fills the gap in the extant research by analysing the relationship between Finnish employees’ reports about mould in their work environment and long-term sickness absences (more than 10 days) occurring 1 to 3 years later. A particular emphasis on long-term absence is important because lengthy instances of sickness can increase the risk of work disability, create financial problems, increase social isolation, reduce self-esteem and decrease career opportunities [10–13]. To test this relationship, we measured self-reported mould with a questionnaire and long-term sickness absences by register-based data.
Methods
Data and participants
The data consist of two linked datasets. The first is the Finnish Quality of Work Life Survey (FQWLS) conducted by Statistics Finland since 1977 [14] and reflects views about working conditions from employees covering all sectors and occupations in Finland. Our study uses the surveys collected in 1997, 2003, 2008 and 2013. The total original sample size of these 4 years was 22,600 wage and salary earners. From this, a sample of 16,351 individuals were interviewed face-to-face with a response rate of 72% [14]. All the information we use in the analysis except that relating to employees’ long-term sickness absences is derived from FQWLS.
The second data source is a register-based follow-up data of the entire Finnish population maintained by the Finnish Social Insurance Institution (KELA). KELA keeps records on sickness allowances paid for medically certified absences longer than 10 days. This allowance can be granted for a maximum period of 300 working days per year. According to the statistics provided by KELA, the most common cause for sickness allowance periods in 2018 were: musculoskeletal diseases (28%), mental and behavioural disorders (22%), external causes (e.g. fractures, 14%) and respiratory diseases (6%) [15]. Maternity leave and absence from work to care for sick children were not included in the absence register.
The two datasets were merged by using the personal security numbers of employees, a process approved and performed by Statistics Finland. The matching of the survey data and register-based follow-up data was approved by the Ethical Committee of Statistics Finland. The final data do not include any information that compromises the anonymity of the participants and all ethical standards of Statistics Finland were followed throughout the study. In the final analysis, we included only those participants aged between 18 and 62 years. The final sample size was 16,084 employees. The missing values varied between 0% and 0.4%.
Measures
Outcome variable: Long-term sickness absences
We drew long-term absence from sickness information from the register data maintained by KELA (i.e. long-term absence). This measure corresponds to the total number of days an employee has been absent from a work because of a long-term illness (i.e. absences that exceed 10 days) over a period of 3 years. We used this number as our outcome variable, limiting the follow-up to a period that started 1 calendar year after FQWLS was collected and ended 3 years later (e.g. if FQWLS was collected in 2013, the follow-up years were 2014, 2015 and 2016). These accumulated long-term absences may result from one or several sickness periods that exceed 10 days and were not necessarily consecutive. The register data do not include information about the number of absence periods or short-term absence days. We used long-term absences in the previous year the FQWLS data were collected as the baseline absenteeism measure in the analysis.
Predictor: Perceived mould (that caused strain) in a work environment
Given that people may experience mould in their workplace very differently, we tested two models. In the first model as a predictor we used the degree to which the participants perceived there was mould in their work environment (i.e. perceived mould). It was measured by one item: 0 = no mould, 1 = mould. In the second model as a predictor we used the degree to which the participants perceived there was mould in their work environment, which put a strain on them (i.e. perceived mould that caused strain). It was measured by two items. The first item asked whether there was mould in the work environment as explained above and the second asked about the degree to which mould was perceived to affect participants at work: five response options varied between very much and not at all. We combined these two items and recategorized the new variable so that the value ‘0’ means that there was no mould in the work environment, participants did not consider mould to be a strain, or only a minor strain. The value ‘1’ means that mould caused quite a lot to very large strain on participants.
The background and work-related factors were selected on the basis of the extant literature [9]. The background variables included gender, age, marital status, at least one child under 18 years at home and level of education. In addition, we controlled for the employee’s perceived control over their job tasks, physical and mental demands of the job task and perceived social support offered by the supervisor.
Statistical analyses
The relationship of the control variables with our perceived mould predictors were examined using cross-tabulations and analyses of variance (see Table I). The relationships of the control variables and perceived mould predictors with subsequent absences due to sickness were examined using analyses of variance (see Table I). The relationships between perceived mould predictors and long-term absence were analysed using a negative binomial model (see Tables II and III). One predictor was used in one model. The days of long-term absence were clearly over-dispersed: the variance was higher than the mean and there was an excess of zeroes, therefore indicating that a simple Poisson model was unsuitable for the analysis [16]. In the case of days of sickness absence, the negative binomial model was more appropriate than Poisson, because the events of interest were not independent [17]. The results are represented as incidence rate ratios (IRR) with 95% confidence intervals. We adjusted all the analyses for background factors (gender, age, marital status, dependent children, level of education), work-related factors (perceived control over the job, physical and mental demands, supervisor’s social support) and health-related factors (earlier absence days). The survey year was also added to the model.
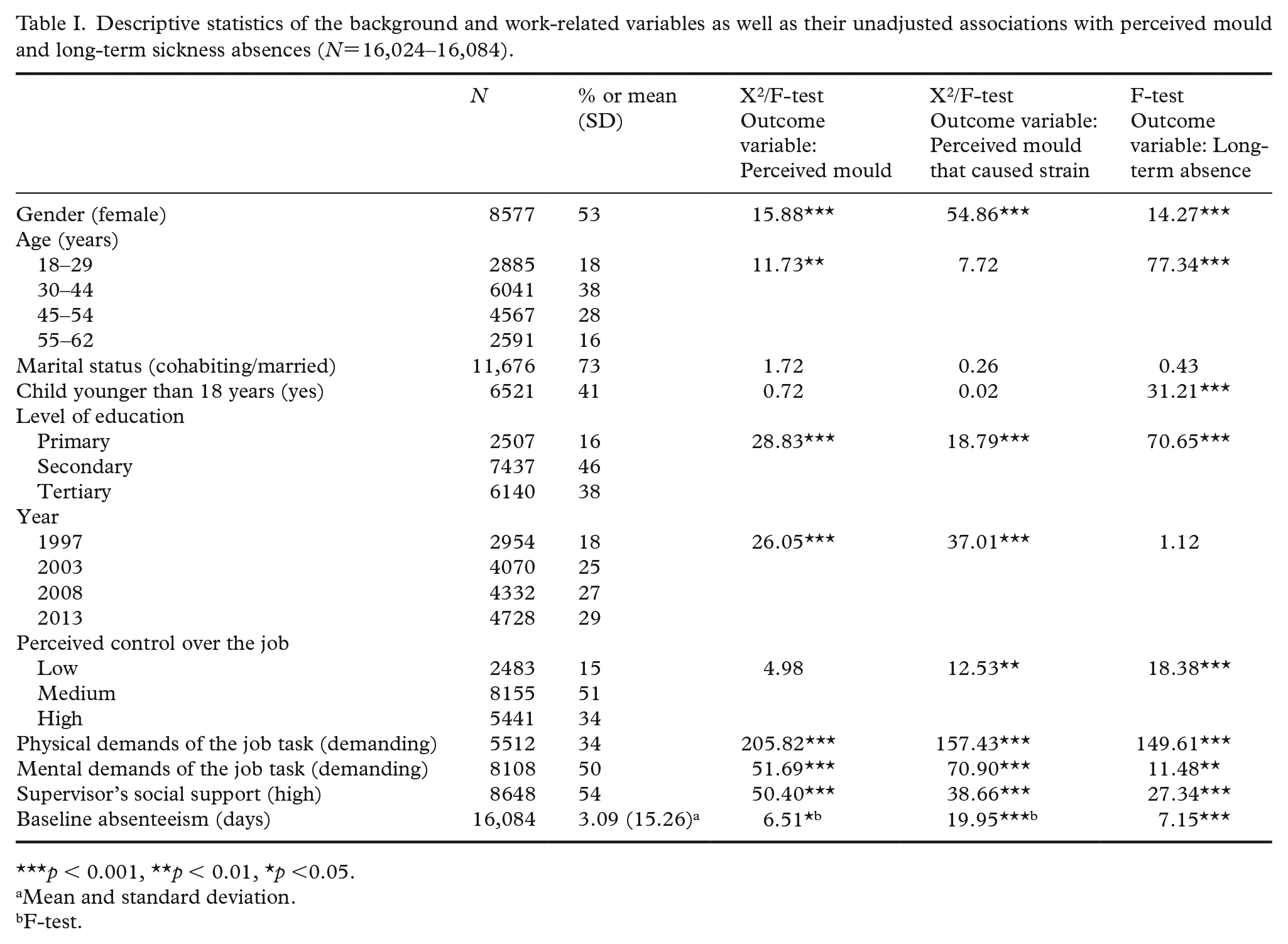
Descriptive statistics of the background and work-related variables as well as their unadjusted associations with perceived mould and long-term sickness absences (N=16,024–16,084).
p < 0.001, **p < 0.01, *p <0.05.
Mean and standard deviation.
F-test.
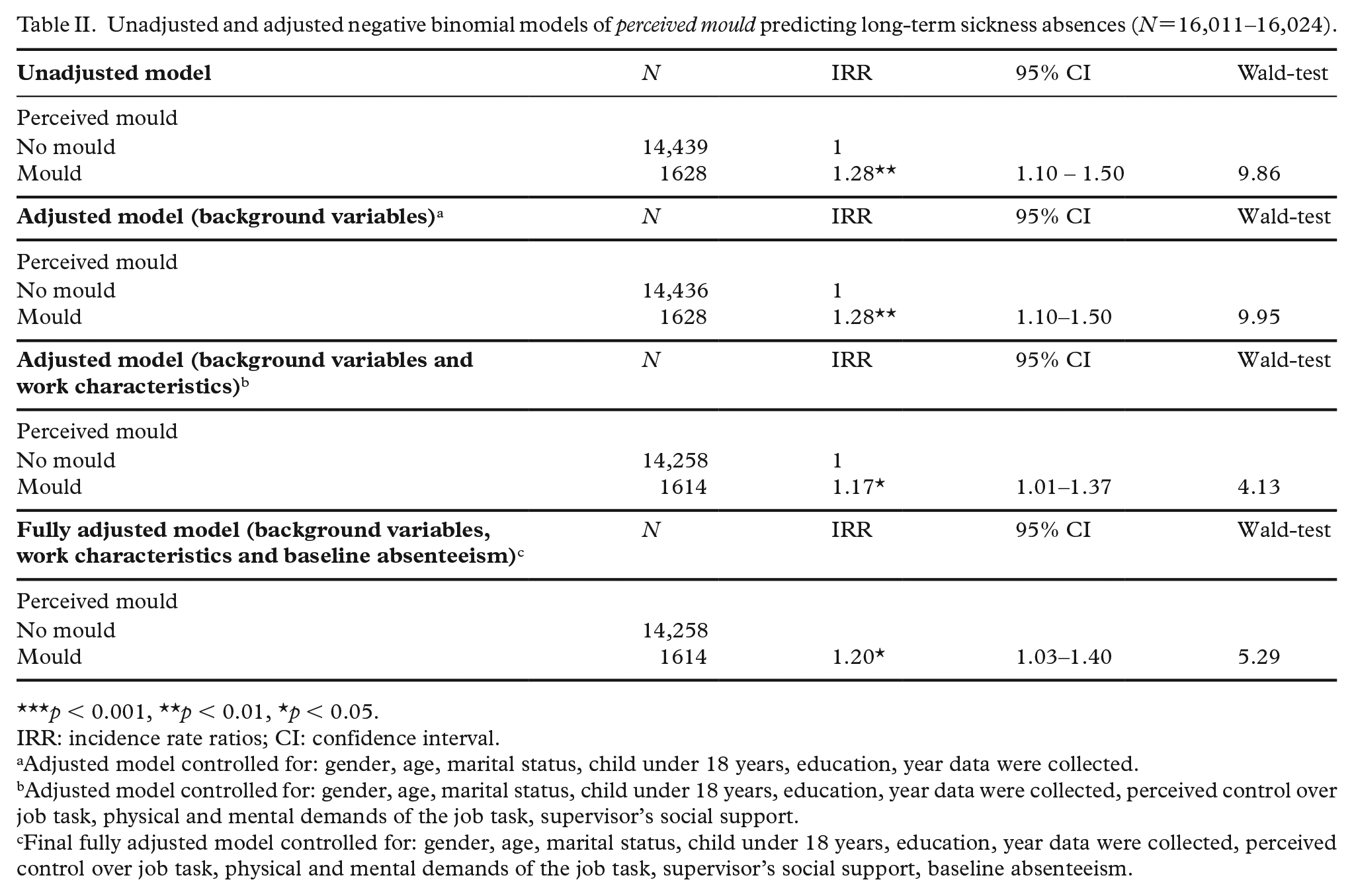
Unadjusted and adjusted negative binomial models of perceived mould predicting long-term sickness absences (N=16,011–16,024).
p < 0.001, **p < 0.01, *p < 0.05.
IRR: incidence rate ratios; CI: confidence interval.
Adjusted model controlled for: gender, age, marital status, child under 18 years, education, year data were collected.
Adjusted model controlled for: gender, age, marital status, child under 18 years, education, year data were collected, perceived control over job task, physical and mental demands of the job task, supervisor’s social support.
Final fully adjusted model controlled for: gender, age, marital status, child under 18 years, education, year data were collected, perceived control over job task, physical and mental demands of the job task, supervisor’s social support, baseline absenteeism.
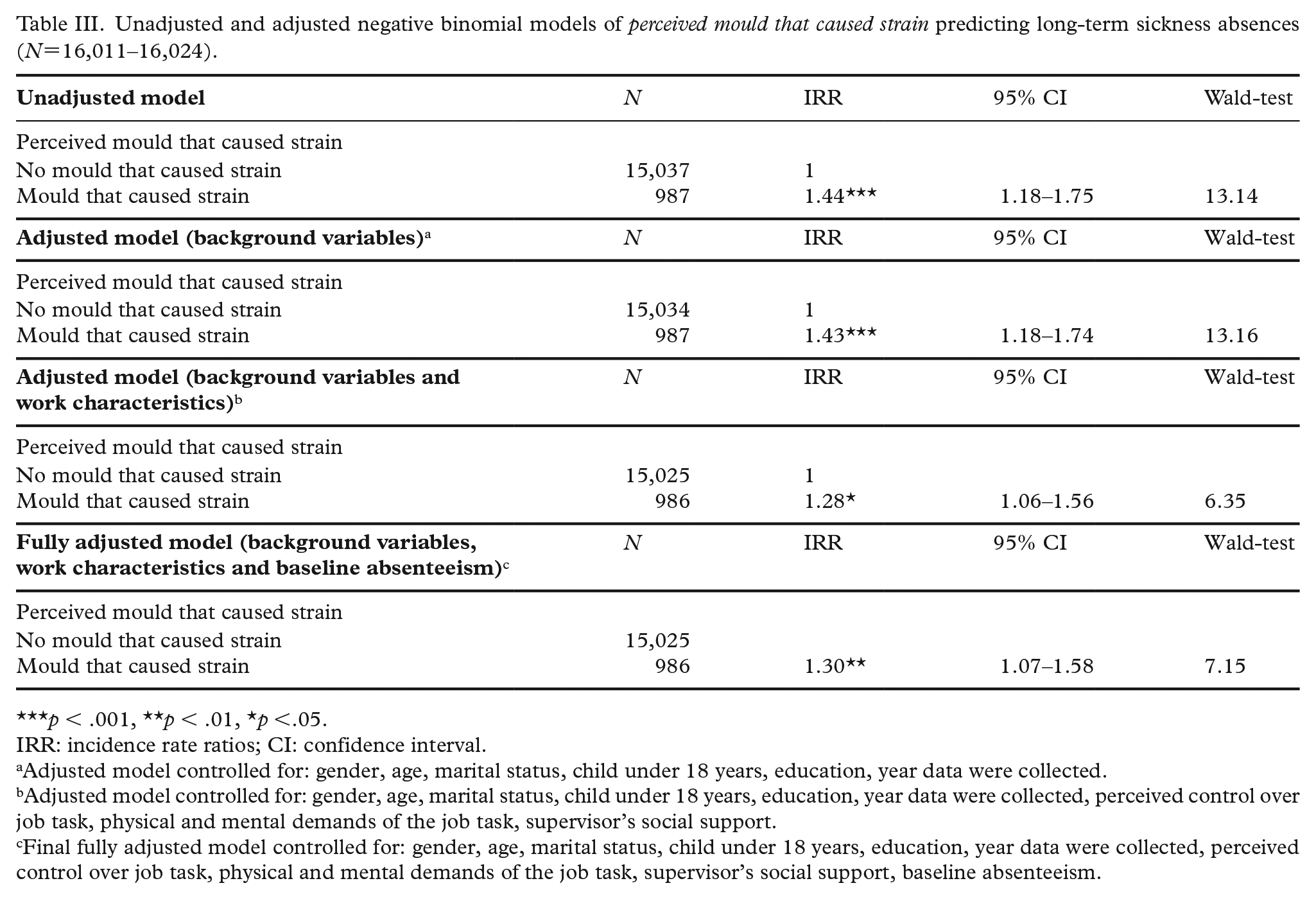
Unadjusted and adjusted negative binomial models of perceived mould that caused strain predicting long-term sickness absences (N=16,011–16,024).
p < .001, **p < .01, *p <.05.
IRR: incidence rate ratios; CI: confidence interval.
Adjusted model controlled for: gender, age, marital status, child under 18 years, education, year data were collected.
Adjusted model controlled for: gender, age, marital status, child under 18 years, education, year data were collected, perceived control over job task, physical and mental demands of the job task, supervisor’s social support.
Final fully adjusted model controlled for: gender, age, marital status, child under 18 years, education, year data were collected, perceived control over job task, physical and mental demands of the job task, supervisor’s social support, baseline absenteeism.
Results
In total, 10% (N=1628) of employees reported mould in their workplace and 6% (N=987) reported that mould caused at least some strain to them. These reports increased significantly over the years surveyed. The proportion of mould was 9% in 1997, 10% in both 2003 and 2008 and 12% in 2013. The proportion of mould that caused at least some strain was 4% in 1997, 6% in both 2003 and 2008 and 8% in 2013. The mean of long-term absence during the 3-year follow-up period was 14.06 days (SD = 44.28; min = 0, max = 507). This value excludes the period prior to the start of long-term absence period. There were no significant changes between the survey years.
Table I presents the frequencies and the mean of the background and work-related variables, as well as their associations with perceived mould and long-term absence. The majority of the participants (that caused strain) were women, aged between 30–44 years and had secondary education.
There were significant associations between perceived mould that caused strain and gender and education. In addition, work-related variables were associated with perceived mould that caused strain. Those participants who had low levels of control over their work, those whose work was physically and mentally demanding and those who received low levels of social support from their supervisors made the highest incidence of reports that mould caused them strain at work.
Long-term absences were significantly associated with all the other variables except marital status and survey year. Women had more long-term absence days (mean = 15.29, SD = 44.71) than men (mean = 12.65, SD = 43.74). Most long-term absences were among the oldest participants, participants with the least education, who had no children under 18 years at home, who had the least control over their work, worked in physically and mentally demanding jobs and who had low social support from their supervisors.
Table II illustrates the results of both unadjusted and adjusted negative binomial models of perceived mould on long-term absences. The univariate association between perceived mould and long-term absences was significant (p = 0.002). Participants who reported mould had 1.28 higher rates of long-term absences than those who did not report such exposure (mould: estimated marginal mean = 17.52 days, standard error = 1.32; no mould: estimated marginal mean = 13.65, standard error = 0.35). After all the background variables were included in the final adjusted model, perceived mould still predicted significant long-term absences between 1 and 3 years later (IRR = 1.20, p = 0.021; mould: estimated marginal mean = 13.45 days, standard error = 1.00; no mould: estimated marginal mean = 11.23, standard error = 0.28).
Table III illustrates the results of both unadjusted and adjusted negative binomial models of perceived mould that caused strain on long-term absences. The univariate association between perceived mould that caused strain and long-term absences was significant (p < 0.001). Participants who reported that mould caused at least some strain had 1.44 higher rates of long-term absences than those who did not report such strain (mould caused strain: estimated marginal mean = 19.66 days, standard error = 1.90; mould did not cause strain: estimated marginal mean = 13.69, standard error = 0.34). After all the background variables were included in the final adjusted model, perceived mould that caused strain still predicted significant long-term absences between 1 and 3 years later (IRR = 1.30, p = 0.008; mould caused strain: estimated marginal mean =14.64 days, standard error = 1.39; mould did not cause strain: estimated marginal mean = 11.25, standard error = 0.27).
Discussion
We found that employees who reported mould in their workplace had higher rates of long-term sickness absences (more than 10 days) than those who did not. In addition, we found that employees who reported that mould caused them to suffer from strain in the workplace had higher rates of long-term sickness absences than those who did not. Both relationships remained significant even after all the background, work and health-related factors were included in the model. To our knowledge, the association between self-reported mould in the workplace, and sickness absence from work has only been considered in one other study [7] and our findings are broadly consistent with this study. However, unlike the study of Sahakian et al. [7], we focused on long-term sickness absences in particular. This was important because, as noted above, long-term absences can have long-lasting effects on an employee’s wellbeing and financial position [9–13]. In addition, we had the advantage of accessing register-based data, meaning we were not reliant on self-reported absence rates, which are nonetheless common in this research field. Finally, our design had a temporal component, which allowed us to test for the first time whether self-reported mould was related to employees’ long-term absences 1 to 3 years later.
Interpretations, limitations and future research
Unfortunately, the diagnoses of those participants who had long-term sickness absences remain unknown to us. In Finland in 2018, respiratory diseases were the fourth common cause for sickness allowance [15]. The report of Finnish Institute of Occupational Health (FIOH) states that between 2005 and 2014, asthma was the sixth most common diagnosis among recognized occupational diseases; from 1146 recognized occupational asthma cases 333 were caused by dampness and mould (323 related to dampness-related agents and 10 to farm work) [18].
Nevertheless, despite its well-known health effects [1, 2], the impact of the indoor environment on people’s health, especially on non-specific symptoms, is partly contested in Finland. For example, the Current Care Guidelines of Duodecim do not recognize the causal relationship between mould or dampness and health [19]. Current Care Guidelines are independent, evidence-based clinical practice guidelines that have an important role in the Finnish healthcare system. Thus, employees who attribute their health problems to their workplaces’ indoor environments may face delegitimation by not being believed or by being ignored by their supervisors or occupational health care professionals [20]. Processes of delegitimation and experiences of injustice can be stressful for employees [21], which may increase the risk of long-term absences [22]. In addition, it is typical in context of contested illnesses that patients’ symptoms are regarded as psychosomatic, or they have been offered a psychiatric diagnosis [23]. Sometimes this can be the case also with people who attribute their health problems to indoor environments [20]. Mental and behavioural disorders are the second common causes for periods of sickness allowances in Finland [15]. Indeed, it is the task of future research to analyse how these people are diagnosed. In addition, the kinds of mechanism that influence the relationship between building-related health problems and long-term sickness absences are worthy of more systematic analysis. We suggest there exists both somatic and psychosocial mechanisms.
Arguably, the second limitation to our study was that we had no physical measurements. Nevertheless, a cumulative amount of research has shown that people can relatively accurately evaluate indoor environmental quality [24, 25], observed dampness and mould associates with measurements of microbial agents [26] and the associations between mould and respiratory symptoms reported by laypeople have been demonstrated in the literature [27]. However, psychosocial factors can also influence how indoor environments are perceived [28] and therefore questionnaires cannot be the only tool to evaluate their quality. Finally, there was no information on tobacco smoking in FQWLS and our model did not include information from different occupational sectors. Thus, future research is needed to replicate our findings using additional tools of measurement, information on tobacco smoking and comparing differences between occupational sectors.
The practical implication of this study is that supervisors, occupational health practitioners and other authorities need to take seriously their employees’ complaints about indoor environmental quality in the workplace and avoid conflicts between authorities and employees. In addition to practical solutions, as FIOH recommends, special attention should be given to organizational communication, which ought to be open, respectful and regular [29].
Conclusions
Our results show that self-reported mould in a workplace is related to long-term sickness absences from work. Additional research is needed to replicate our findings using other measurement tools and to map potential mechanisms. We suggest these underlining mechanisms include both somatic and psychosocial components.
Footnotes
Acknowledgements
This paper is dedicated to the memory of Professor Jouko Nätti.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: