
Abstract
Objectives: Chronic obstructive pulmonary disease (COPD) is globally a major, but often undiagnosed, cause of morbidity and mortality. The aims of this study were to assess the prevalence of COPD in Helsinki, Finland, with international diagnostic criteria and to analyse risk factors including socioeconomic status, and disease severity. Methods: A general population sample of 628 adults (368 women) completed flow-volume spirometry with bronchodilation test and a structured interview. Post-bronchodilation spirometry was assessed both using the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria and relative to the fifth percentile of the reference value (lower limit of normal, LLN). Results: According to GOLD criteria, 37 (5.9%), and by using the LLN criteria, 43 subjects (6.8%) had airway obstruction consistent with COPD. Using the GOLD criteria, four subjects or 0.6% of the population had severe, 3.0% moderate, and 2.2% mild COPD. Of those with post-bronchodilator obstruction, 49% had no previous diagnosis of obstructive airways disease and did not use medication for any respiratory disease. The prevalence of undiagnosed COPD defined by GOLD was 2.9% (LLN 3.3%). In addition to age, smoking history, and prior history of asthma, socioeconomic status based on occupation was significantly related to COPD in the population. Manual workers in industry (GOLD 10.0%, LLN 11.7%) and non-manual assistant employees (10.2%, 10.2%) had a significantly higher prevalence of COPD than professionals (2.8%, 2.3%).
Introduction
Chronic obstructive pulmonary disease (COPD) is a major source of mortality and morbidity and it has risen to be a major health issue in many countries. The main risk factor for COPD is smoking [1,2]. Other inhalation exposures, e.g. air pollution, occupational inhalation of vapours, dusts, gases and fumes (VDGF), environmental tobacco smoke (ETS) in addition to the role of recurrent or early life lung infections have also been implicated as risk factors for the disease [1 –4].
The World Health Organization Global Burden of Disease project estimates that occupational risk factors account for around 13% of COPD, 11% of asthma, and 9% of lung cancer cases in adults [5]. In Finland, the role of occupational exposures has been increasingly recognized as risk factors for adult-onset asthma [6]. In contrast, there has been limited recognition in Finland of occupational exposures as causative agents of COPD, mainly focused on farming exposures and the role of atopy in potentiating these [7]. Recently, basic educational level has been shown to be an independent risk factor for COPD in Finland [8]. Socioeconomic factors predisposing to adverse COPD outcomes have been increasingly recognized [9].
Various international initiatives have attempted to develop a uniform definition and diagnostic criteria for COPD. The ATS/ERS Taskforce on Standardisation of Lung Function Testing [10] recommended in 2005 the use of the ratio of forced expiratory volume in one second (FEV1) to largest vital capacity (VC or forced vital capacity, FVC) below the lower limit of normal (LLN) as an indicator of airway obstruction [10]. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria use the absolute ratio of FEV1/FVC considering values below 0.7 after bronchodilation as abnormal [11]. Recognizing the potential for over-diagnosis of obstruction in the elderly using this definition, the 2006 update of the GOLD criteria added the use of measures relative to representative reference values [11]. As FEV1/FVC decreases with increasing age, the use of a fixed limit of 0.7 may result in underdiagnosis in young people and over-diagnosis amongst the elderly – a situation in reverse of the treatment objectives [12]. Although the awareness of COPD in the society has increased, underdiagnosis of COPD has still been a marked problem both internationally and in Finland [1,13].
In Finland, a National COPD Programme has been undertaken from 1998–2007 aimed to improve the recognition of COPD in primary care and to promote anti-smoking activities [14]. In the mid 1990s, a population prevalence of 9% was reported from Northern Finland, with age, amount of smoking, and family history of obstructive airways disease significantly increasing the risk for COPD [13]. In a recent Finnish report comparing data between 1978–1980 and 2000–2001 no change in the prevalence of obstruction was found [15]. The prevalence of COPD by GOLD criteria based on pre-bronchodilation tests was 5% in the latter survey [8].
The main aims of the present survey were to study the prevalence of COPD in Helsinki, Finland, using two international guidelines, the ATS/ERS Standards and the GOLD criteria, and to assess the risk factors including socioeconomic status and the extent of underdiagnosis by disease severity in an urban population.
Materials and methods
Study sample
In the FinEsS-Helsinki study, 8000 individuals were randomly sampled from the Finnish Population Register Centre in 1995 to represent the adult population of Helsinki. Randomisation was performed within 10-year age groups and gender with no further exclusion or inclusion criteria applied. Of these, 6062 (76.8%) individuals responded to a postal questionnaire. Later, in 2000, a sample of 1200 individuals was randomly selected from the postal survey responders to a subsequent clinical phase of the study; 1135 subjects were traced and 643 (57%) participated. The non-participants of the clinical part did not differ significantly from the participants when previously reported diagnoses of obstructive airways diseases (OAD), respiratory symptoms, and smoking history were compared from the results of the postal survey [16].
At the clinical visit undertaken from 2001–2003, subjects completed the Finnish version of the FinEsS structured interview [16] with a physician and underwent flow-volume spirometry with bronchodilation test. All subjects continued their regular medication during the study including any possible asthma medication. The final sample consisted of 628 subjects from whom a complete interview and spirometry results were collected.
The study was conducted according to the Helsinki Declaration and approved by the Ethics Committee of the Department of Medicine of Helsinki University Central Hospital. All participants gave an informed consent.
Flow-volume spirometry and definition of COPD
Spirometry was completed with a flow-volume device (VMax 20c; Sensor Medics, Yorba Linda, CA, USA) with the subject seated. The spirometry method has been described in detail previously [16]. For bronchodilation, the subjects inhaled 0.4 mg of salbutamol aerosol (Ventoline; GlaxoSmithKline, London, UK) through a spacer device (Volumatic; GlaxoSmithKline) using two separate doses. Spirometry was repeated after 15 minutes to determine the bronchodilation response. The spirometry variables analysed were post-bronchodilator FEV1, FVC, and the ratio of FEV1/FVC. The current Finnish reference values were used [17]. Reduced FEV1/FVC ratio was assessed both with the GOLD criteria of absolute FEV1/FVC ratio <0.7 [11] and with respect to lower limit of normal (LLN) defined as below the fifth percentile of the reference value, which has been estimated at 88% of predicted for both men and women [17]. Obstruction was graded from the post-bronchodilator FEV1 using the GOLD criteria. Values of FEV1 <30% of predicted were classified as very severe, between 30–49% as severe, 50–79% as moderate, and at least 80% of predicted as mild COPD [11].
Analyses
Based on data from the postal questionnaire survey and the structured interview, data on possible risk factors for and symptoms suggestive of COPD were collected including current and past smoking status, smoking pack-years, and age of starting smoking for ever-smokers, prior diagnoses of asthma and use of asthma medication, environmental tobacco smoke exposure, socioeconomic group, early life infections, childhood asthma or wheezing, childhood daycare, childhood domicile, and childhood exposure to furry pets. Family history of OAD and socioeconomic status were analysed from the original postal questionnaire data. Socioeconomic classification system suitable for Nordic countries based on occupation developed by Statistics Sweden was used [18]. This classification combines the concurrent effects of level of formal education and the average level of income associated with the occupational category.
Based on the classification, the following categories were used: (1) manual workers in industry: occupations involving production of goods and normally requiring ≤2 years of post-comprehensive school education; (2) manual workers in service: occupations involving service production and normally requiring ≤2 years of post-comprehensive school education; (3) assistant non-manual employees: non-manual occupations normally requiring ≤2 years of post-comprehensive school education; (4) professionals, including executives and civil servants at high and intermediate level: occupations requiring normally ≥3 years of university or college education; and (5) others: housewives, non-professional self-employed, military, and unclear.
The proportion of undiagnosed subjects fulfilling criteria for COPD and the population prevalence of undiagnosed COPD were estimated by using subjects with obstruction (GOLD or LLN criteria) but with no reported prior diagnoses of or use of medication for obstructive airway diseases as the nominator and all subjects with obstruction (GOLD or LLN) and complete sample as the denominator, respectively. The anthropometric variables used for the analysis were gender, age, height, weight, and body mass index (BMI, kg/m2). A person was classified as an ever-smoker, if he/she had ever smoked more than 4 cigarettes per month for 1 year, and as a current smoker if he/she had smoked any cigarettes during the preceding 12 months.
Statistical methods
Statistical analyses were performed with the Statistical Package for Social Sciences (IBM SPSS for Windows version 19.0; IBM SPSS, Chicago, IL, USA). One-way analysis of variance (ANOVA) was used to test for trends. Categorical variables were compared with χ2-test to identify significant determinants. p-values <0.05 were considered significant. Risk factors with p<0.05 in either LLN or GOLD criteria were included in multivariate logistic regression models, and the results are expressed as odds ratios with 95% confidence intervals (CI).
Results
Anthropometric data and smoking habits
Anthropometric, smoking history, and spirometric data are presented in Table I. Of men 37.7% and of women 51.6% (p<0.001) were classified as never-smokers, while 34.2% and 25.3% (p<0.001) of men and women, respectively, were current smokers. Among ever-smokers, the mean smoking pack-years was 19.1 (SD 18.2; range 0.2–95.0). Men had smoked significantly more than women (p<0.001); mean 23.3 (95% CI 20.1–26.4) pack-years compared to 15.4 (13.1–17.6). Considering the socioeconomic background based on occupation, women worked more often in non-manual assistant professions and men more often in manual professions in industry (p<0.001).
Anthropometric data, post-bronchodilation spirometry values, smoking history, and socioeconomic background of the study participants.
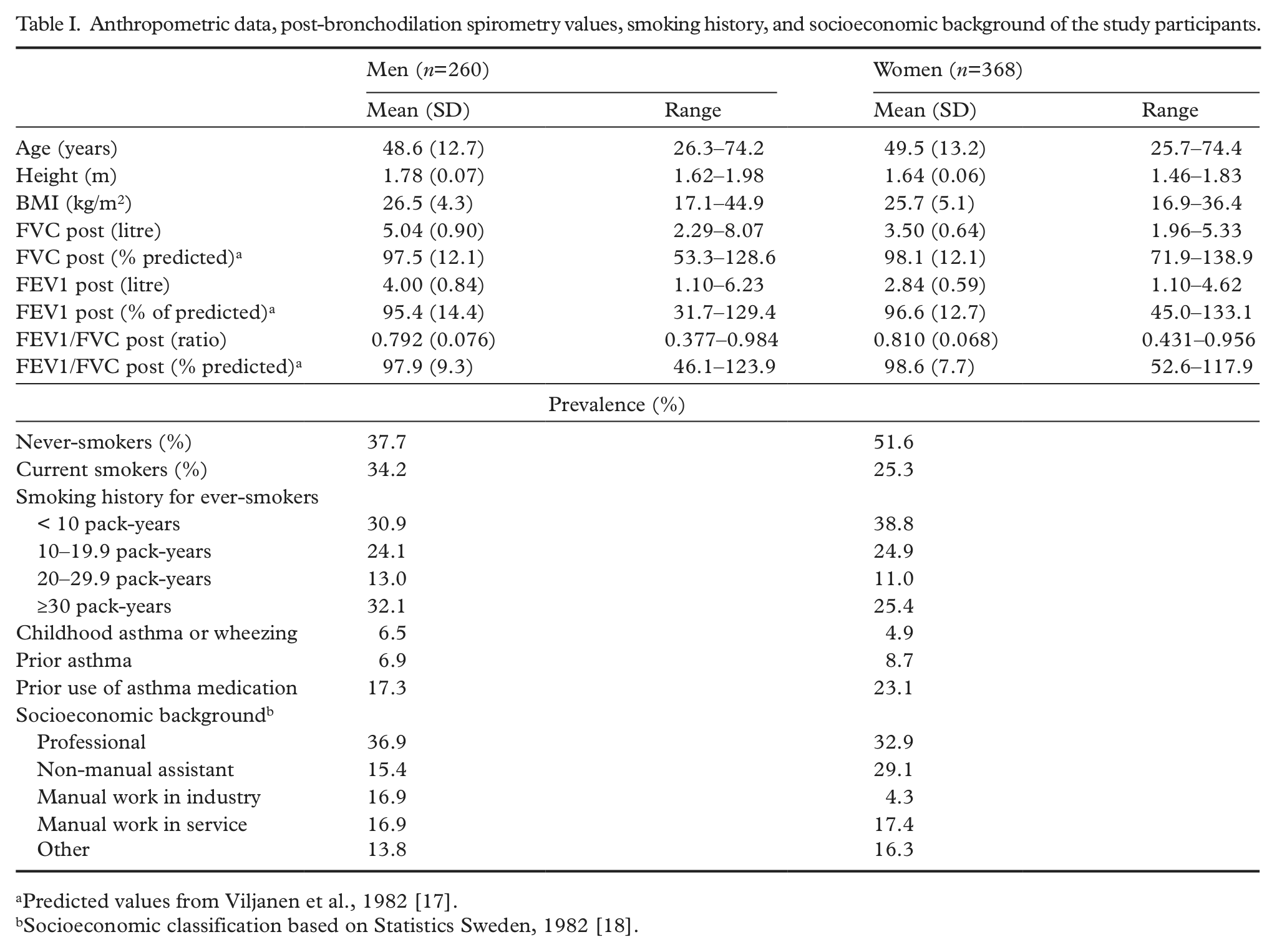
Predicted values from Viljanen et al., 1982 [17].
Socioeconomic classification based on Statistics Sweden, 1982 [18].
Prevalence
The prevalence of COPD in the population using the GOLD and the LLN criteria was 5.9% and 6.8%, respectively. The prevalence of mild COPD was 2.2% using the GOLD and 3.2% using the LLN criteria, moderate 3.0% and severe 0.6% on both criteria. All but one subject fulfilling the criteria of obstruction according to GOLD also fulfilled the LLN criteria of obstruction, while seven subjects out of 43 fulfilling the LLN criteria were not obstructive according to GOLD. Six of the seven discordant cases identified only with LLN criteria were young or middle aged men (mean age 38.3 (SD 13.8) years) that had FEV1/FVC close to borderline values. The distribution of subjects with airflow limitation and the degree of obstruction in terms of FEV1% predicted as a function of age is illustrated in Figure 1.
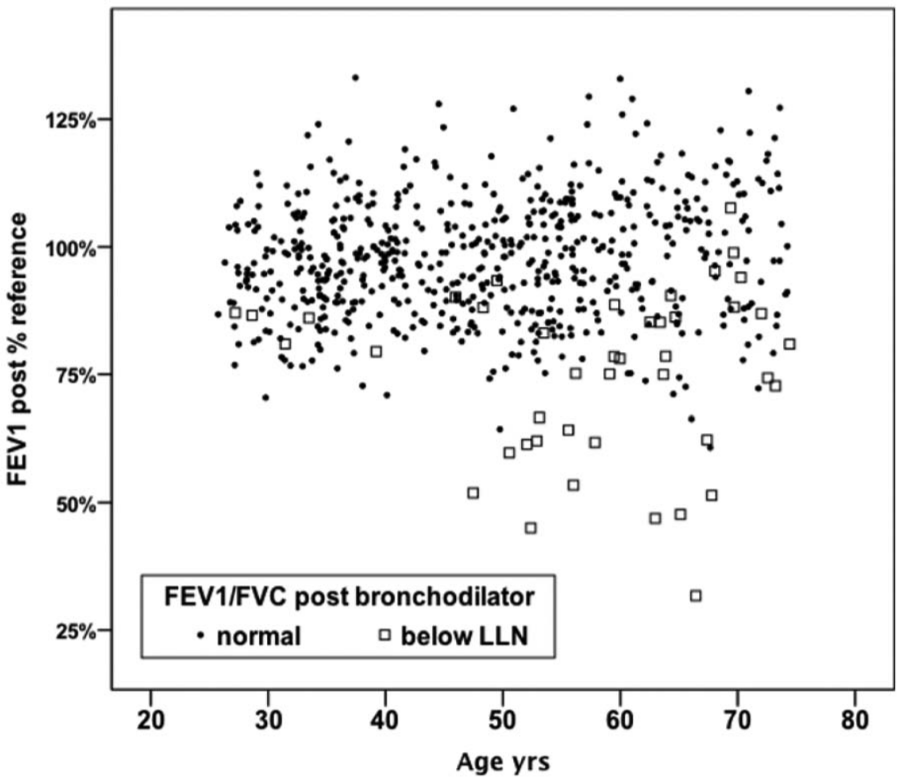
Forced expiratory volume in one second (FEV1) predicted post-bronchodilation in the population sample by age stratified by presence or absence of airflow limitation defined by the ratio of FEV1 to forced vital capacity (FEV1/FVC) post bronchodilation relative to lower limit of normal (LLN).
On the GOLD criteria, 18 individuals (8 women) and on LLN criteria 21 individuals (8 women) with post-bronchodilation obstruction had no previous diagnosis of obstructive airways disease or lung medication representing 49% of subjects with obstruction on both criteria. On LLN criteria, 30.2% (GOLD 32.4%) had a previous diagnosis of asthma. Prior diagnosis of asthma (including asthma in the childhood) or previous use of asthma medication increased the prevalence of airflow limitation consistent with COPD with smoking in a multiplicative way (Figure 2). The population prevalence of undiagnosed COPD was thus 2.9% (GOLD) or 3.3% (LLN) in this sample of general adult urban population. Of the undiagnosed cases with COPD, 50.0% with GOLD or 57.1% with LLN had a mild disease, and 50% with GOLD or 42.9% with LLN had a moderate disease.
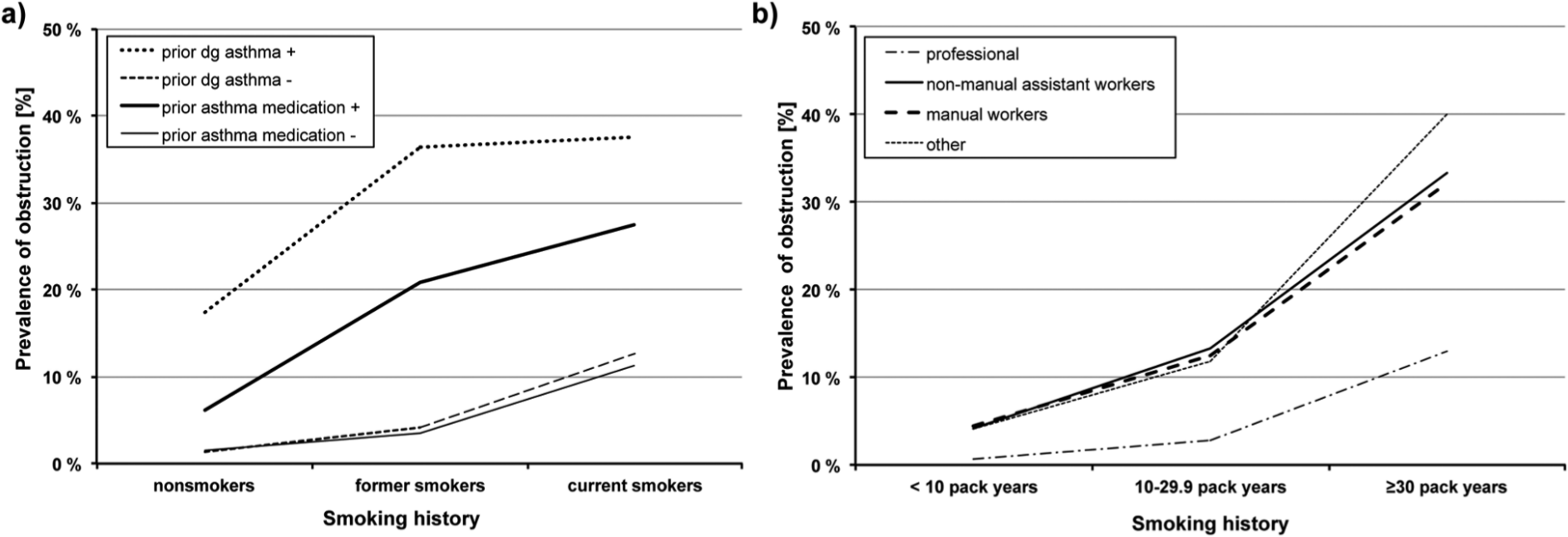
Prevalence of COPD on LLN criteria in post-bronchodilation in the population sample stratified by smoking history and a) prior diagnoses of asthma or use of asthma medication, and b) socioeconomic group based on occupation.
The prevalence of COPD using LLN and GOLD criteria stratified by smoking history and age is shown in Figure 3. The effect of smoking pack-years and age was multiplicative. The highest prevalence of COPD according both GOLD and LLN criteria, 42.9% and 47.6%, respectively, was found in current smokers of the oldest age cohort of 60–75 years. Of those with spirometric obstruction according to the GOLD criteria, longstanding cough was reported by 43.2%, chronic productive cough by 29.7%, dyspnoea (British Medical Research Council grade II) by 13.5%, any wheeze during the preceding 12 months by 48.6%, and any respiratory symptom by 94.6%. Corresponding figures when using the LLN criteria were slightly lower: 39.5%, 23.3%, 11.6%, 46.5%, and 90.7%, respectively.
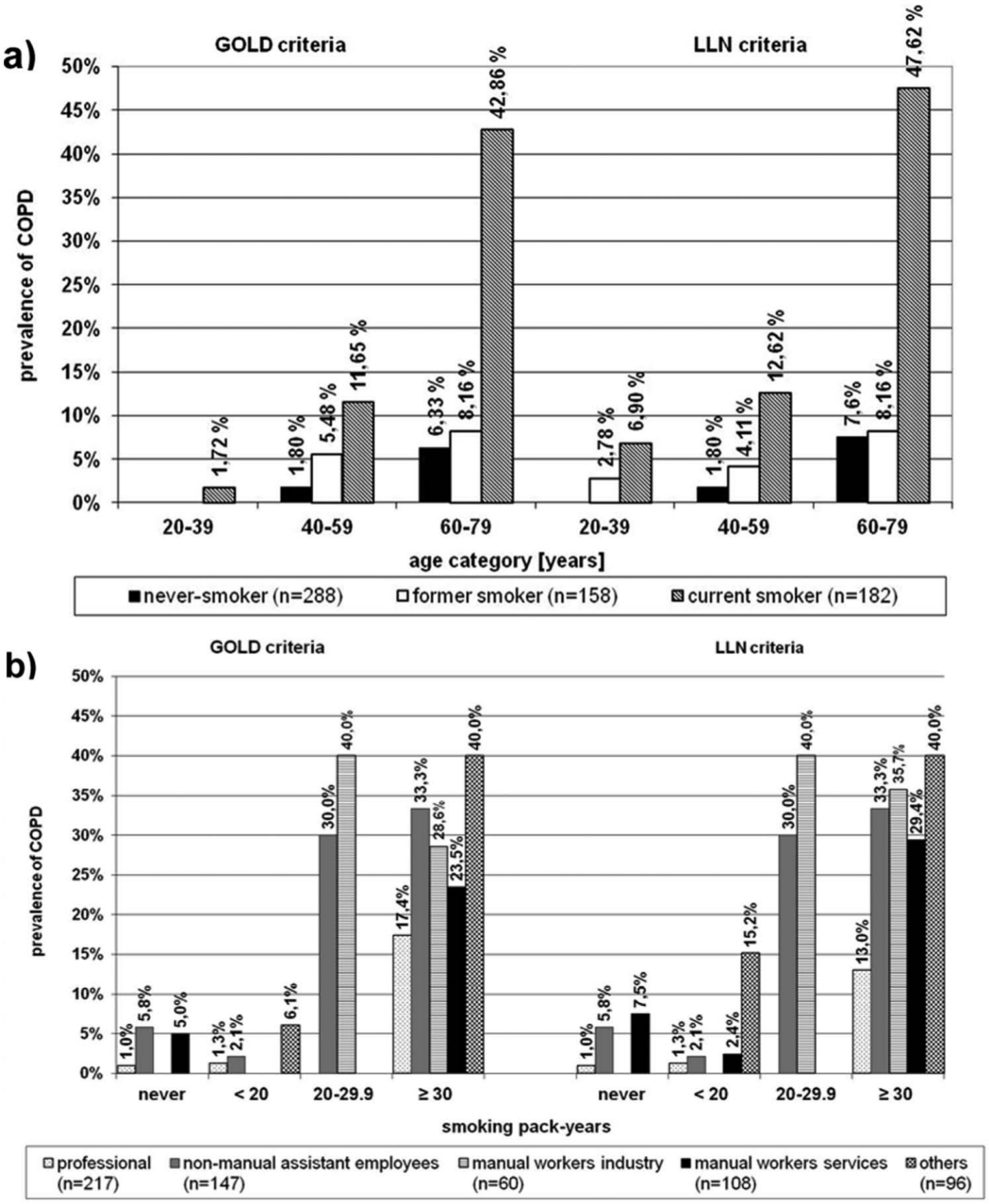
Prevalence of COPD by LLN and GOLD criteria in post-bronchodilation spirometry of a general population sample stratified by a) age groups and smoking history, and b) by smoking history and the socioeconomic group based on occupation.
Risk factors
According to bivariate analysis, age, current smoking status, smoking pack-years, prior asthma or use of asthma medication, socioeconomic status, environmental tobacco smoke exposure, childhood wheezing or asthma, and daycare before the age of 5 years were significantly associated with obstruction (data not shown). Early childhood infections or childhood domicile, number of siblings, or presence of furred pets in early childhood were not significantly related to obstruction (data not shown).
Odds ratios (OR) for the identified risk factors for obstruction calculated using multiple logistic regression are outlined in Table II together with the unadjusted prevalence of obstruction for each risk. The risk associated with smoking increased significantly in smoking history >20 pack-years in the oldest age group (age >60 years) and in manual and non-manual workers compared to professionals. The effect of smoking history on the prevalence of obstruction on LLN criteria stratified by socioeconomic group is illustrated in Figure 2. Professionals (n=217) had a lower prevalence of COPD compared to other socioeconomic groups even after stratifying for smoking history. Daycare before the age of 5 years was a protective factor in the bivariate analysis, but the effect was not significant in the multivariate logistic regression model. That was also the case for family history of OAD, childhood domicile (urban or rural), and early childhood events including lung infections under the age of 5 years.
Risk factor analysis with multiple logistic regression analyses for COPD fulfilling LLN or GOLD criteria.
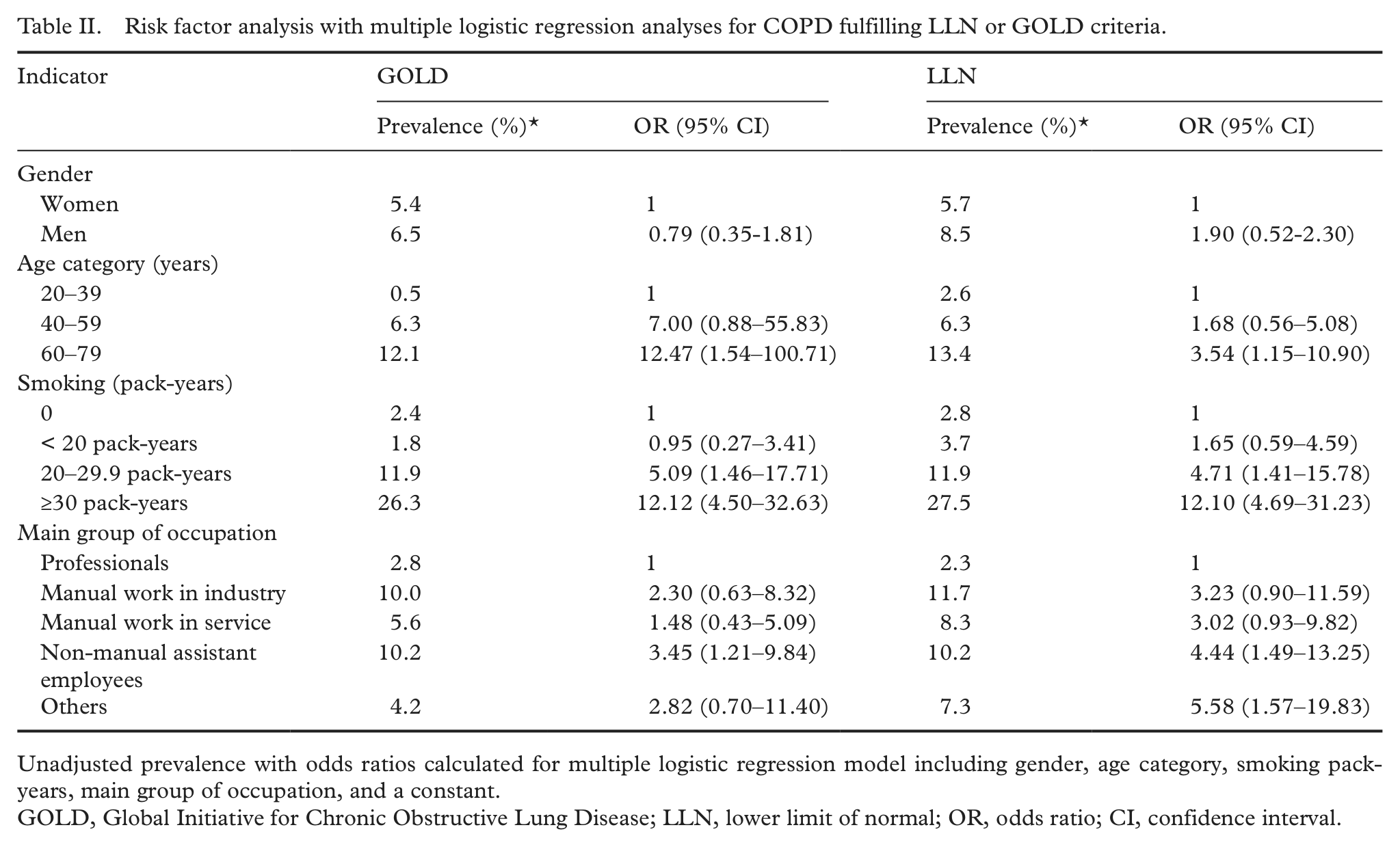
Unadjusted prevalence with odds ratios calculated for multiple logistic regression model including gender, age category, smoking pack-years, main group of occupation, and a constant.
GOLD, Global Initiative for Chronic Obstructive Lung Disease; LLN, lower limit of normal; OR, odds ratio; CI, confidence interval.
The prevalence of LLN and GOLD criteria defined obstruction in different socioeconomic groups based on occupation stratified by smoking history is shown in Figure 3. The prevalence of GOLD criteria defined obstruction in non-manual assistant employees was 10.2% (LLN also 10.2%), which was significantly greater than in professionals 2.8% (p=0.020; LLN 2.3%, p=0.008). Using the LLN criteria, the prevalence of COPD in manual workers (including both industry and services) was 9.5%, which was significantly higher than in professionals (OR 3.10, p=0.039), but with GOLD criteria the difference did not reach significance (OR 1.79, p=ns).
Discussion
The population prevalence of spirometric COPD using the GOLD criteria was 5.9% (LLN 6.8%) in this general urban population sample. Underdiagnosis is common, and 49% of the COPD cases (on both GOLD and LLN) based on post-bronchodilator spirometry had no previous diagnosis of OAD or use of pulmonary medication corresponding to a population prevalence of undiagnosed COPD of 2.9% (LLN 3.3%). In addition to the recognized risk factors of current smoking, smoking pack-years, concurrent or previous asthma, and age, socioeconomic status reflecting occupation was also a significant risk factor for COPD.
The large proportion of symptomatic subjects with spirometric COPD demands action by healthcare services. The National COPD Programme in Finland 1998–2007 was aimed to reduce the prevalence of COPD and the proportion of moderate and severe disease in the population targeting both the identified main risk factor of smoking and the underrecognition of incident cases in the population [14]. However, in our study which falls to the mid of the COPD Programme time schedule, underdiagnosis was of similar magnitude as previously found both in northern Sweden and in northern Finland [13,19].
The use of different criteria in defining COPD is currently under debate internationally. Reduced absolute FEV1/FVC-ratio has been found to correlate with increased mortality in the elderly even when FEV1/FVC relative to reference value (LLN) is in the normal range [20]. The superiority of absolute or relative measures naturally depends strongly on the quality of reference values, i.e. how well they represent the population especially in the elderly [12]. The Finnish reference values [17] differ from many other reference equations in having a logarithmic transformation, hence the predicted values in the elderly for FEV1/FVC ratio do not reduce linearly as in most reference equations, but instead level off in women and even increase slightly in men. In Finland, the reference value for FEV1/FVC diminishes slightly below 0.70 only in elderly women, and thus the GOLD limit will almost invariably result in smaller prevalence estimates in Finland. This explains the slightly higher prevalence of obstruction observed also in some elderly with LLN criteria compared to the use of GOLD criteria in our study (Figure 3, Table II) and the few older discordant cases. In epidemiological studies on the population level, GOLD criteria provide currently internationally comparable measures. On individual level, however, values relative to reference values are needed and even other measures to identify early cases particularly in young and middle-aged subjects should be better evaluated.
In this cross-sectional setting, 8.8% of ever-smokers had GOLD criteria defined obstruction (10.3% LLN), which is slightly less than previously reported from the Finnish Lapland [13] but more than in the national level study [9,15]. The difference with Northern Finland parallels with a somewhat lower smoking exposure in Helsinki. In the study by Vasankari et al. [15] the prevalence was estimated using reference equations from the Swiss SAPALDIA study, which significantly underestimates the prevalence of airflow limitation compared to Finnish reference values. The study by Kotaniemi et al. [13] and several other recent studies including the Third National Health and Nutrition Examination Survey (NHANES III) in the USA have demonstrated that about a half of smokers sooner or later develop COPD [19,21]. Our results are in line with this finding with 43% (GOLD) of current smokers in the oldest age cohort having spirometry-defined COPD.
Smoking is the most important causative factor for COPD [1,2], a result also confirmed by our study. Unfortunately, the strong association of COPD with smoking has resulted in a weaker understanding of the other risk factors for COPD, factors that occur also in never-smokers. Inhalation of other noxious substances can also potentiate the effects of smoking. Early life events have been proposed as factors explaining host susceptibility for COPD [3]. Our sample size was too small to detect early life events reaching significance. Bias caused by forgetfulness may contribute, as it is possible that subjects do not accurately remember early childhood events, and hence to elucidate their role larger samples and optimally prospective studies are needed. Childhood wheezing or asthma and previous asthma are recognized risk factors for COPD, a finding reinforced by our study. We found a multiplicative relationship between prior asthma or asthma medication and irreversible airflow limitation consistent with COPD. It is important to note that all subjects continued their eventual medication during the study. Prior diagnosis of asthma or use of asthma medication were excluded from the undiagnosed COPD cases.
Despite our not very large sample size, we found statistically significant associations between socioeconomic status based on occupation and COPD. Especially manual workers particularly in industry and non-manual assistant employees had an increased prevalence of COPD not attributable to differences in smoking habits according to stratified analyses (Figures 2 and 3). There are no previous comparable population studies on the influence of occupation on COPD in Finland, but the result conforms with findings in northern Sweden [19]. In a Finnish rural population cohort of elderly people (>64 years), COPD was more frequent in low socioeconomic groups with smoking exposure and concurrent exposure to dusts during their working life [7]. Farming exposures related to grains, organic dusts, or animal endotoxins have been implicated to potentiate the risk of atopy and increase the prevalence of chronic bronchitis [2,7,22].
The impact of occupational factors on adult-onset persistent asthma in Finland has been shown to be much larger and widely spread than it previously was assumed [6]. The classification of socioeconomic groups we used has been widely used in epidemiological studies in Sweden and other Northern European countries. Low socioeconomic status has been shown to be a risk factor for the development of asthma [23,24]. The socioeconomic group based on occupation reflects not only possible occupational exposures but also various life-style factors, e.g. associated with differences in exposures to environmental tobacco smoke and other irritants, and educational level. Occupational exposure to chemical agents, inorganic and organic dusts increase the risk of COPD according to industry-based epidemiological studies e.g. in mining, construction, and agriculture, occupations that are considered “dusty” [2,25]. On a population level, several studies have mainly documented the role of similar occupational exposures to construction, mining, chemicals, and textile dust [26], but also transportation, health care, office work (e.g. records processing clerks, sales), and waitresses [21]. Combination of smoking and occupational exposure to vapours, gas, dust, or fumes (VGDF) carries an additive deleterious effect on lung function promoting development of COPD. In a recent matched case–referent study that evaluated occupational exposures in COPD patients both with a job exposure matrix and subjects self-report, VGDF exposure was associated with an increased risk of COPD (OR 2.1) and a population attributable fraction of 31% of COPD cases, whereas joint exposure with VGDF and smoking increased the risk to OR 14.1 [27].
Many of these population studies have relied on patient reports of previously diagnosed COPD or on flow-volume spirometry without bronchodilation test [21, 27]. These definitions are prone to cause biases both from underdiagnosis and even overreporting; further asthmatic obstruction cannot be ruled out. The population attributable risk of COPD from occupational exposures in non-smokers has been estimated between 11–53% [2, 21, 28], compared to around 51% reported for smoking [29]. Occupational exposures have earlier been shown to increase morbidity [30] and mortality in COPD [25]. As reviewed above, internationally there is much evidence that occupational exposures can increase the risk of airway obstruction, but less so regarding non-manual work. Recent studies have shown an additional effect of social components to occupational exposures [9], which is also reflected in the SEI classification used in this study.
We have shown that, independently from smoking habits, significant differences exist between different occupational groups in development of pulmonary function abnormality consistent with COPD also in Finland. This offers clear potential for prevention of occupational exposures predisposing to development of COPD and should be further studied. The sample size is too small to allow more detailed analysis of effects from socioeconomic status and occupational exposures on development of COPD, and larger studies with more detailed socioeconomic and occupational history are clearly needed. Identification and targeting prevention activities to less well-known risk factors will be necessary to further reduce the burden of COPD both in smokers and in never-smokers alike to continue the efforts set forth with the National COPD Programme [14].
In conclusion, the found prevalence of COPD in Helsinki was 5.9% (LLN 6.8%), which conforms to other results from studies in the Nordic countries. Underdiagnosis of COPD is common also in Helsinki affecting about 3% of adult population, however, most moderate and severe cases were identified by the healthcare system. In addition to smoking, increasing age, and previous asthma, the socioeconomic groups manual workers and non-manual assistant employees were significantly associated with obstruction consistent with COPD in this urban population sample. The potential role of current and previous occupation should be considered more systematically to identify potential future avenues of prevention of COPD.
Footnotes
Acknowledgements
The authors would like to thank the Research Unit for Respiratory Medicine at the Helsinki University Central Hospital for their excellent assistance.
Funding
This study was supported by a special governmental subsidy for health sciences research (Helsinki University Central Hospital project grant numbers TYH 1235, TYH 2303, and TYH 4251) and the Foundation of the Finnish Anti-Tuberculosis Association and the Research Foundation for Pulmonary Diseases (Heli) (AK).