
Abstract
The motoric cognitive risk syndrome (MCR) is a novel and clinically relevant pre-dementia syndrome indicating a higher dementia risk (e.g., for Alzheimer's disease). Given that MCR prevalence is unknown in Germany, we conducted a cross-sectional study, in which 208 participants from Germany aged 50 and 82 years answered an online survey including questions to assess subjective MCR (sMCR). The adjusted sMCR prevalence was 25.3%. Adults with sMCR reported more diseases and showed negative associations with physical activity, sedentary behavior, and sleep, suggesting that lifestyle modifications can play a significant role in MCR prevention. Further research is required to complement our preliminary findings on sMCR prevalence in Germany.
Introduction
The motoric cognitive risk syndrome (MCR) was established in 2013 by Verghese and colleagues as a pre-dementia stage that is defined by slowed gait speed and subjective cognitive complaints. 1 Several studies have identified cardiometabolic (i.e., high blood pressure, diabetes, obesity) 2 and lifestyle factors (e.g., physical inactivity and sedentary behavior) as crucial contributors to the development of MCR. 3 Furthermore, MCR is well-suited for a broader application in different public health contexts, based on (i) a strong body of evidence indicating that individuals with MCR have an increased risk for negative health events such as falls, dementia, and mortality4,5 and (ii) the time-efficient assessment of MCR allowing for easy implementation in various settings. The assessment of the (objective) MCR is based on the measurement of gait speed (e.g., 4m-walk test) and a question about the cognitive status of the participant (e.g., “Do you feel you have more problems with memory than most others?”) (see for more details 6 ). However, to the present date, the prevalence of MCR in older adults ranging between 2.4%–33.3% has only been established in individual countries (e.g., China, USA, France) 7 and is lacking in Germany. Recently, a subjective assessment via a questionnaire of MCR has been proposed (i.e., subjective motoric and cognitive complaints 8 ) allowing for its application in different survey types (e.g., online or telephone surveys). However, as no data on subjective MCR (sMCR) prevalence exists in Germany, this study aimed to address this gap in the literature.
Methods
Population and study design
Data were collected as part of a larger cross-sectional online survey on digital health literacy between June 2023 and March 2024. The total sample consisted of 208 participants (104 female) aged between 50 and 82 years (mean age: 59.9 ± 7.7 years); see Table 1 for more details. Recruitment was conducted via advertising in various political and social organizations, as well as via the recruitment tool Prolific (www.prolific.com) (2023–2024). Individuals living across Germany who (i) were aged 50 years and above, (ii) with proficient German language skills, and (iii) without a diagnosis of dementia or mental disabilities were eligible to participate. The study was approved by the local ethics committee of the University of Potsdam (No. 7/2023).
Overview of the general characteristics of the participants (N = 208). The number of data sets for the specific variables varies because of missing values.
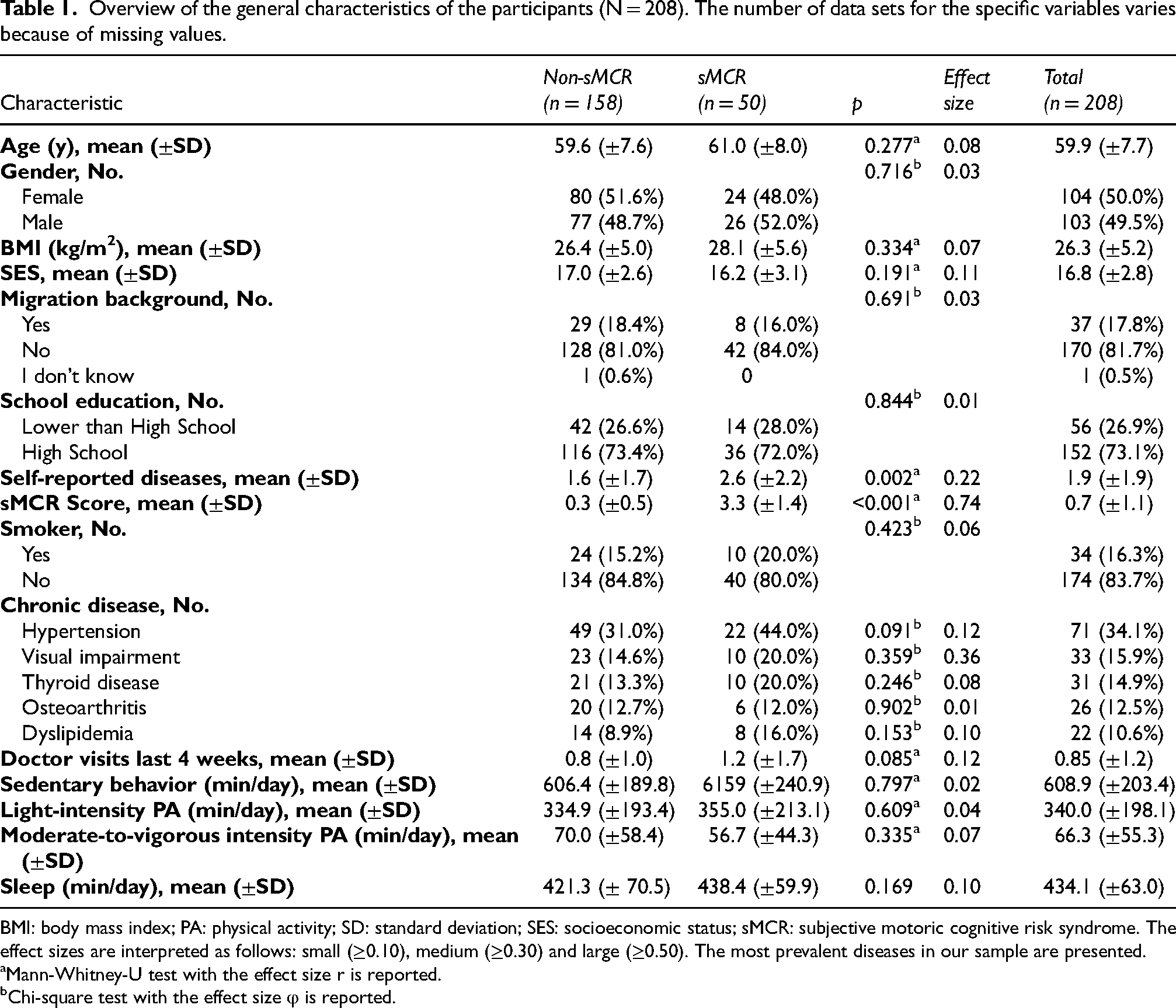
BMI: body mass index; PA: physical activity; SD: standard deviation; SES: socioeconomic status; sMCR: subjective motoric cognitive risk syndrome. The effect sizes are interpreted as follows: small (≥0.10), medium (≥0.30) and large (≥0.50). The most prevalent diseases in our sample are presented.
Mann-Whitney-U test with the effect size r is reported.
Chi-square test with the effect size φ is reported.
Subjective motoric cognitive risk syndrome
In this study, a German translation of the sMCR screening tool, originally developed by Ayers and colleagues, was used to assess sMCR. 8 The questionnaire allows for a remote screening (e.g., online questionnaire or videoconference), requiring only minimal financial or personal resources. 8 Based on the high sensitivity (84%) and specificity (82%) reported previously, 8 five questions regarding the domains “subjective cognitive complaint” (SCC) and “subjective motor complaint” (SMC) were used in our online survey (see Supplemental Material). All questions need to be answered by a dichotomous response (e.g., yes or no) and one point was awarded for each affirmative answer. In the current study, the regression coefficients reported by Ayers and colleagues were utilized as weights for each subjective complaint item, with the resulting points summed up to obtain the final MCR score. 8 A score of greater than two was defined as the cut-off for the presence of sMCR. 8
Risk factors
In the online survey, additional information such as age and gender were collected as covariates. Body height and body weight were used to determine the body mass index (BMI). Information about education, employment and income was used to determine the participants’ socioeconomic status (SES), based on the operationalization of the SES index by the Robert Koch Institute 9 (3–21 points). Additionally, self-reported information on the presence of specific diseases was obtained, and the German version of the Daily Activity Behaviors Questionnaire (DABQ), which has satisfactory psychometric properties, 10 was used to quantify the 24-h movement behaviors of the participants’ including sedentary behavior (SB; minutes per day), sleep (minutes per day) and physical activity (PA; minutes per day).
Statistical analyses
After an initial data control (i.e., checking for missing values and plausibility), descriptive analyses of frequencies, means, standard deviations, and prevalence, adjusted for age and gender were determined. Group differences between non-sMCR and sMCR were investigated using a chi-square test (χ2) for categorical variables and a Mann-Whitney U test for continuous variables. The risk factors for sMCR were examined using binary logistic regression analysis. For both regression models, an adjustment was made to account for age, gender, and SES. Odds ratio (OR) and 95% confidence interval (95% CI) are reported. Data analysis was performed using SPSS Statistics software (IBM SPSS Statistics for Windows, version 28.0.1.1. Armonk, NY: IBM Corp), with a significance level of α ≤ 0.05.
Results
Demographics and characteristics
The sample of 208 participants from diverse regions in Germany can be described as educated, with a comparatively high SES (16.82 ± 2.75 points), an average burden of diseases (1.9 ± 1.9 diseases), 11 and with a low proportion of participants with a migrant background (n = 37, 17.8%) (for more details, see Table 1). Statistically significant group differences between non-sMCR and sMCR are displayed in Table 1.
Prevalence
Of the 208 participants, 50 exhibited a score of more than two on the sMCR questionnaire. Following adjustment for age and gender, the prevalence of sMCR in our non-representative German sample was 25.3%.
Binary logistic regression of risk factors
Two binary logistic regressions were conducted to determine the association of the covariates and risk factors with the sMCR. Model 1, adjusted for age, gender, and SES, included the following risk factors: high blood pressure, type II diabetes, depression, heart disease, and dyslipidemia. The overall binary logistic regression model was not statistically significant (χ²(8) = 11.10, p = 0.196), resulting in a small amount of explained variance (Nagelkerke's R² = 0.110). The overall classification accuracy in Model 1 was 73.9%. The regression model suggests that none of the eight variables exhibited a statistically significant effect: age (p = 0.288), gender (p = 0.556), SES (p = 0.200), high blood pressure (p = 0.81), type II diabetes (p = 0.055), depression (p = 0.753), heart disease (p = 0.556) and dyslipidemia (p = 0.442). In a second logistic regression (Model 2), adjusting for the aforementioned covariates (i.e., age, gender, SES), the parameters of 24-h movement behaviors (i.e., SB, sleep, light-intensity PA, and moderate-to-vigorous-intensity PA) were entered. Model 2 was statistically significant (χ²(7) = 14.52, p = 0.043), and explained 16.3% of the overall variance (Nagelkerke's R² = 0.163). The classification accuracy of Model 2 was 74.8%. Of the seven variables, four were identified as predicting sMCR namely SB (p = 0.032), sleep (p = 0.031), light-intensity PA (p = 0.032), and moderate-to-vigorous-intensity PA (p = 0.031). A longer sleep duration (OR = 0.38, 95%-CI [0.16, 0.92]), and more time spent in light-intensity PA (OR = 0.38, 95%-CI [0.16, 0.92]), moderate-to-vigorous-intensity PA (OR = 0.38, 95%-CI [0.16, 0.92]) or SB (OR = 0.36, 95%-CI [0.16, 0.92]) was observed to have a protective effect by reducing the likelihood of sMCR. The model coefficients of Model 1 and Model 2 as well as corresponding odds ratios can be found in Table 2 and Table 3 in the Supplemental Material.
Discussion
In summary, we observed an adjusted prevalence of 25.3% of sMCR in our non-representative German sample which is higher than the European (10.6%) and in the range of the worldwide prevalence (9.0%; ranging from 2.4% to 33.3%) being reported for objective MCR in older adults. 7 The relatively high MCR prevalence in our sample is perhaps related to the use of subjective measures to establish MCR prevalence (i.e., online survey via questionnaire) instead of objective ones (i.e., gait analysis). The non-significant associations between gender, age, and SES with sMCR differ from the findings of previous studies,12–14 although it has to be acknowledged that the link between MCR and gender remains a topic of discourse.7,12,13
Moreover, the associations between sMCR and a range of diseases, including hypertension, type II diabetes, heart disease, depression, and dyslipidemia did not reach statistical significance, which is perhaps related to the small sample size in the present study. However, the assumption that specific diseases are associated with a higher MCR prevalence, as evinced in the literature,15,16 is also supported by our findings showing a statistically significant group difference between non-sMCR and sMCR concerning the number of diseases. Consistent with previous work, we observed that sleep, light-intensity, and moderate-to-vigorous-intensity PA are significantly negatively associated with sMCR, potential reasons for such associations are discussed elsewhere.3,14,16 Furthermore, we noticed that higher levels of SB are associated with lower odds of sMCR, which is contrary to the findings of previous studies providing evidence for the opposite relationship.3,16 Hypothetically, such an observation is related to the lack of differentiation between different types of SB, namely mentally active (e.g., reading, playing an instrument, computer use, or paperwork) or mentally passive SB (e.g., TV viewing). 17 Given that the educational level of our sample can be rated as relatively high, it seems reasonable to hypothesize that in our sample SB might primarily involve mentally active SB. This assumption is supported by the findings of a study showing that older European adults, who have a relatively high level of education, spent more time in mentally active SB compared to peers with a lower educational level, who spent more time in mentally passive SB. 18 A higher engagement in mentally active SB may exert a protective effect on cognitive performance, 17 and, in turn, lowers (s)MCR prevalence. However, further studies are required to elucidate whether the type of SB moderates the association with (s)MCR status.
Taken together, our observations imply that promoting a physically and mentally active lifestyle, as well as sufficient sleep can be a promising approach to prevent (s)MCR and associated negative health events. Although previous feasibility studies employing lifestyle interventions (e.g., home-based PA interventions) among older adults with MCR showed promising initial results,19,20 future studies investigating the influence of cost-effective intervention approaches (e.g., home-based and digitally-delivered PA interventions21,22) on (s)MCR-related markers are required to provide more robust empirical evidence to support the application of lifestyle interventions as routine intervention approach for MCR prevention.
Our preliminary findings obtained from a relatively small sample should be interpreted with some caution because the data collection via an online survey is prone to selection bias since only individuals with a certain level of digital literacy and digital infrastructure (e.g., own smartphone, PC) could participate. It is also relevant to note that our study sample exhibited a relatively high SES, which might limit the generalizability of our findings to samples with a lower SES. In addition, although a high concordance of sMCR with objective MCR has been confirmed, 8 the precise overlap between sMCR and objective MCR is not fully understood, which makes, in turn, an extrapolation of the present findings to objective MCR challenging.
Nonetheless, this study provides the first quantitative evidence of the prevalence of sMCR in Germany (25.3%). However, to better inform future actions of public health promotion, further research on (s)MCR including but not limited to generating more robust prevalence estimates (e.g., for Germany) and evidence on protective factors (e.g., lifestyle behaviors) is required.
Supplemental Material
sj-docx-1-alz-10.1177_13872877241307407 - Supplemental material for Subjective motoric cognitive risk syndrome: Preliminary prevalence from an online survey of a German cohort aged 50+
Supplemental material, sj-docx-1-alz-10.1177_13872877241307407 for Subjective motoric cognitive risk syndrome: Preliminary prevalence from an online survey of a German cohort aged 50+ by Paula Theobald, Fabian Herold, Thomas Gronwald and Notger G Müller in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
The authors thank all persons who conducted the online survey.
Author contributions
Paula Theobald (Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Project administration; Writing – original draft); Fabian Herold (Conceptualization; Methodology; Writing – review & editing); Thomas Gronwald (Methodology; Supervision; Writing – review & editing); Notger G. Müller (Methodology; Resources; Supervision; Writing – review & editing).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The articles were funded by the Open Access Fund of the University of Potsdam provided by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) – Projektnummer 491466077.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The raw data will be made available by the authors, upon written and reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.