
Abstract
Osteogenesis imperfecta (OI) is a heritable connective disorder with clinical manifestations including bone fragility and short stature. Previous research identified psychosocial themes related to mental health among children with OI and their caregivers, such as independence, social isolation, depression, and anxiety. Several studies have also examined clinicians of individuals with OI for their perspectives on mental health among their patients. However, no known studies have compared psychosocial themes among all three participant groups concurrently. This qualitative study examined mood and anxiety, along with risk and protective factors, from perspectives of youths, parents, and clinicians. Semi-structured interviews were conducted, which were coded independently by two researchers. Codes were analyzed for extraction of themes. Relevant themes include depressed and anxious mood experienced in individuals with OI, as well as risk factors and protective factors for these symptoms. Participants reported functional limitations and social isolation as key risk factors for symptoms of anxious or depressed mood. In contrast, they discussed positive attitudes, social support, multidisciplinary medical groups, and mental health access as key protective factors. Implications for clinical care and future research are discussed. Convergence and divergence of themes across study samples are discussed in detail.
Introduction
Osteogenesis imperfecta (OI) is a heritable condition with clinical features categorized into skeletal (e.g., short stature, scoliosis, discolored teeth, and bone fragility) and extraskeletal (e.g., blue sclera and hearing loss) symptoms (Forlino and Marini, 2016). There are four main phenotypic types (Sam and Dharmalingam, 2017). Type I is mild; Type II is most severe and lethal; Type III is severe, while Type IV is moderate.
Among children, OI contributes to adverse mental health outcomes, but certain coping strategies may buffer against them (Dogba et al., 2013; Hill et al., 2014; Tsimicalis et al., 2016; Wiggins and Kreikemeier, 2017). Children with OI have endorsed worry about fractures, which may limit engagement in physical activities (Forlino and Marini, 2016; Hill et al., 2014; Santos et al., 2018). Children have also reported isolation and self-consciousness about being perceived as different (Dogba et al., 2013; Hill et al., 2014; Santos et al., 2018; Tsimicalis et al., 2016). Negative judgments made by peers (Dogba et al., 2013; Santos et al., 2018) and desire to be more like non-OI peers may contribute to feelings of depression (Carmoy, 2004). Literature suggests adapting to OI status is associated with resilience and educational achievement (Mc Donald et al., 2023).
Parents of children with OI also face unique psychosocial challenges, although literature is mixed regarding how OI impacts caregivers (Dogba et al., 2013; Hill et al., 2019; Santos et al., 2018; Wiggins and Kreikemeier, 2017). Much like their children, parents of those with OI have reported fear of fracture specific to their child’s OI status (Dogba et al., 2013; Dung et al., 2013; Hill et al., 2019). Also reported are fears of stigmatization and being perceived as different relative to unaffected peers (Dung et al., 2013; Hill et al., 2014). Much like other health conditions, OI is associated with parental anxiety, although acceptance of uncertainty and social support have been proposed as potential coping strategies (Cobham et al., 2020; Dogba et al., 2013; Dung et al., 2013; Hill et al., 2022; Wiggins and Kreikemier, 2017). Functional limitations among children with OI also appear to contribute to caregiver stress (Santos et al., 2018). Children with OI often express desires for independence, yet parental fear, safety concerns, reduced functioning, and pain may limit a child’s ability to engage in activities (Santos et al., 2018). Recent literature suggests child experiences with pain are associated with caregiver stress and quality of life, but not depression (Lazow et al., 2019).
Healthcare providers may offer additional perspectives and insights to complement those of parents and children with OI (Hill et al., 2014, 2022). Consistent with parents and children with OI, providers note fear in both children and parents when children with OI are handled, as well as fatigue and social isolation among children while their peers engage in physical activities (Hill et al., 2014, 2022). Social isolation and body image contribute to perceptions of being different from peers, especially during adolescence (Hill et al., 2022). However, clinicians have also reported these concerns may be mitigated by support from social groups, educators, and clinicians (Hill et al., 2014).
Clinicians also noted challenges faced specifically by caregivers, including feeling overwhelmed by initial diagnosis and inadequate childcare support, often because of anxiety by others, including extended family members, of mishandling their child (Hill et al., 2022). However, literature examining perspectives of providers of children with OI is limited. Since clinicians facilitate mental health treatments, further exploration of their perspective is valuable if future interventions are to be deployed.
Existing literature provides evidence OI contributes to unique psychosocial outcomes for children. However, limited research has examined perspectives of caregivers and healthcare providers of children with OI, two groups that may have insights where children lack awareness. Accordingly, this study relied on a qualitative approach to assess themes reported by children, caregivers, and clinicians, from semi-structured interviews. Perspectives of these three groups were compared to assess converging and diverging perspectives on pediatric OI. This study comparatively explored three participant groups’ perspectives on these topics for children with OI: (1) Associations between OI status and mental health. (2) Risk factors for mental health, including individual, community, and healthcare factors. (3) Protective factors for mental health, including individual, community, and healthcare factors.
“Risk factor” in this study refers to factors that trigger, exacerbate, or prolong anxious and/or depressed mood, according to participants. “Protective factor” in this study refers to factors preventing or alleviating anxious and/or depressed mood, according to participants. Neither term is intended to imply quantitative statistical analysis in this qualitative study and cannot be equated with clinical diagnoses or treatment recommendations.
Aim
The aim of the study was to assess characteristics of mental health among children with OI as reported by caregivers of children with OI, children with OI, and clinicians providing care to children with OI, as well as potential risk and protective factors for mental health issues.
Methods
Study design
Participants were interviewed using semi-structured guides covering: (1) Characterization of OI, (2) Pain Challenges, (3) Mental Health, and (4) Priorities for Future Intervention. Interview guides were tailored for each study sample (e.g., children were only asked items specific to their experiences, see Supplemental Materials). Adult participants provided informed written consent before participation, and child participants provided assent while their parents provided written consent. This study was approved by Institutional Review Board at Baylor College of Medicine (IRB # H-49741). Upon completion, participants were compensated US$50.
Recruitment and eligibility
Participants were recruited via email listserv provided by Osteogenesis Imperfecta Foundation (OIF) and social media. Participants contacted researchers via phone or email. Eligible participants include children diagnosed with OI, clinicians who treat children with OI, and caregivers of people with OI. Participants were required to be between 8 and 89 years, speak English, and live in the United States or Canada.
Procedure
Semi-structured interview guides were collaboratively developed by research team members (KMK, EAS, SCS), clinicians specializing in OI, and OIF representatives. Interviews were administered by trained research team members (WCR and ADW) and supervised by a psychologist with extensive clinical interviewing experience (EAS). Self-reported demographic data were collected from all participants.
Data analysis
Pseudonyms were assigned to all participants. Interviews were auto-transcribed. Two research team members reviewed transcripts to confirm transcription accuracy (WSS, HEC) and consulted original video recordings when suspected transcription errors occurred. Researchers analyzed transcriptions in MAXQDA 2020 to develop a standardized codebook for code definitions (WCR, ADW, CNM, and KMK) (Decuir-Gunby et al., 2011). Codes were developed using thematic content analysis by which themes were progressively abstracted, and researchers identified agreed-upon codes and definitions (Boyatzis, 1998; Braun and Clark, 2021). Transcripts were independently coded in three successive rounds using MAXQDA 2020 (VERBI Software GmbH, Berlin, Germany) by two researchers (WSS, HEC).
Coding entailed subjectively determining an interview segment’s relevance to a particular code. Throughout codebook familiarization, code attributions become more consistent across coders. However, they are unlikely to become perfectly uniform, and differences between coders provide valuable divergence—one coder will see what another missed. Interrater reliability requires a balance of coding similarly but not identically, leaving room for diversity of perspective. To establish reliability, coders compared each other’s code attribution frequencies across three transcripts. They identified significant discrepancies in coding styles by examining each coder’s “top 10 most attributed” versus “bottom 10 least attributed” codes. For example, if a code appeared in one coder’s top 10 most attributed codes but bottom 10 of another’s, team discussions were used to address discrepancies. These discussions resulted in new consensus understandings for future coding. This process was repeated twice, producing greater consensus across coders, until further discussions offered diminishing returns. Although there is an arbitrary threshold for “sufficient reliability,” this procedure guided formation of a greater consensus among coders.
Once achieved, both researchers coded remaining transcripts independently and discussed discrepancies. Codes for mental health consisted of topics: depression, anxiety, and risk/protective factors for depression and anxiety. Depression and anxiety referred to depressed and anxious mood, rather than clinically diagnosable conditions (e.g., mood or anxiety disorders). Themes were extracted using thematic analysis from coded interview material (JHQ, CG) (Braun and Clarke, 2021). Thematic analysis identified themes related to depression, anxiety, and risk and protective factors for anxious or depressed mood in children with OI. Illustrative quotes are included in Results with pseudonyms.
Quantitative data were analyzed and reported to help contextualize qualitative findings. Median interview time (Mdn) and interquartile range (IQR) were reported to account for data skew and outliers. Thematic frequencies and percentages were reported for themes and subthemes. Demographics were also reported, including frequencies for categorical descriptives, and Mdn and IQR for age to account for data skew.
Results
Sample characteristics
All interviews were conducted from February 2021 through March 2022, recorded over a secure teleconference application (Mdn = 50.5 min; IQR = 23.5 min), with caregivers (Mdn = 63.0 min; IQR = 18.00 min), children (Mdn = 42.5 min; IQR = 16 min), and clinicians (Mdn = 44.5; IQR = 15.25 min).
Participant demographic data.
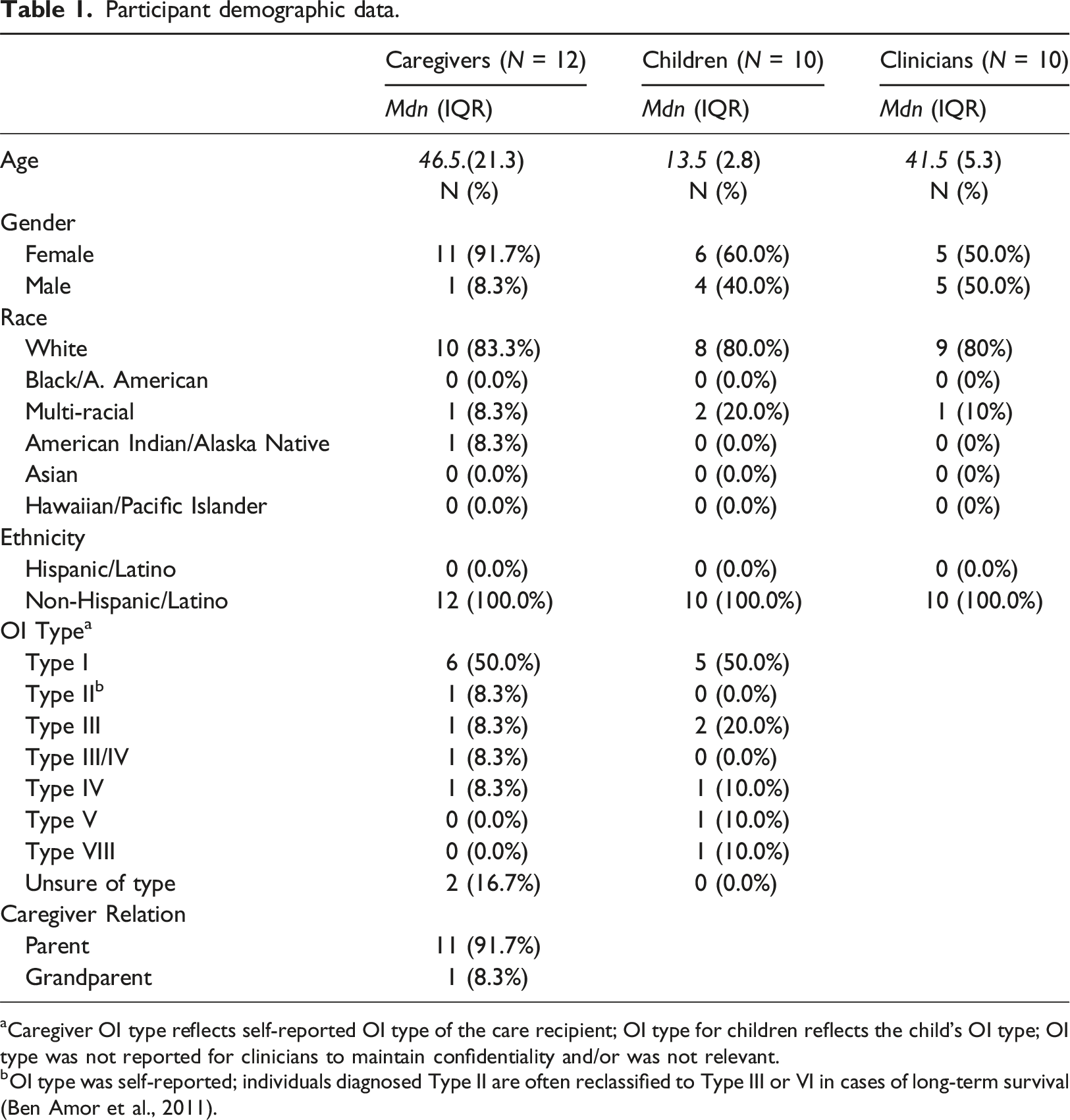
aCaregiver OI type reflects self-reported OI type of the care recipient; OI type for children reflects the child’s OI type; OI type was not reported for clinicians to maintain confidentiality and/or was not relevant.
bOI type was self-reported; individuals diagnosed Type II are often reclassified to Type III or VI in cases of long-term survival (Ben Amor et al., 2011).
Mental health manifestations include depression and anxiety symptoms
Thematic frequencies are reported in Table 2. A majority of all three stakeholder groups reported anxiety and depressed mood among children with OI (12/12 caregivers (100%), 8/10 children (80%), and 10/10 clinicians (100%)). Depressed mood was most often attributed to sadness resulting from functional limitations (2/12 caregivers (17%), 3/10 children (30%), and 3/10 clinicians (30%). A subset of participants reported that inability to participate in sports and other physical activities contributes to low mood. One child stated: “something I get angry about is that taking steps in a walker was always a huge goal of mine until it kept getting like, you have this surgery and then have to restart”—Lauren (Child, Multi-Racial Non-Hispanic, Female, Age 16, OI Type III). Frequencies of mental health themes among three stakeholder groups. Note. Themes and subthemes are noted in the first column. Remaining columns represent stakeholder groups, frequencies, and percentages at which themes and subthemes were reported.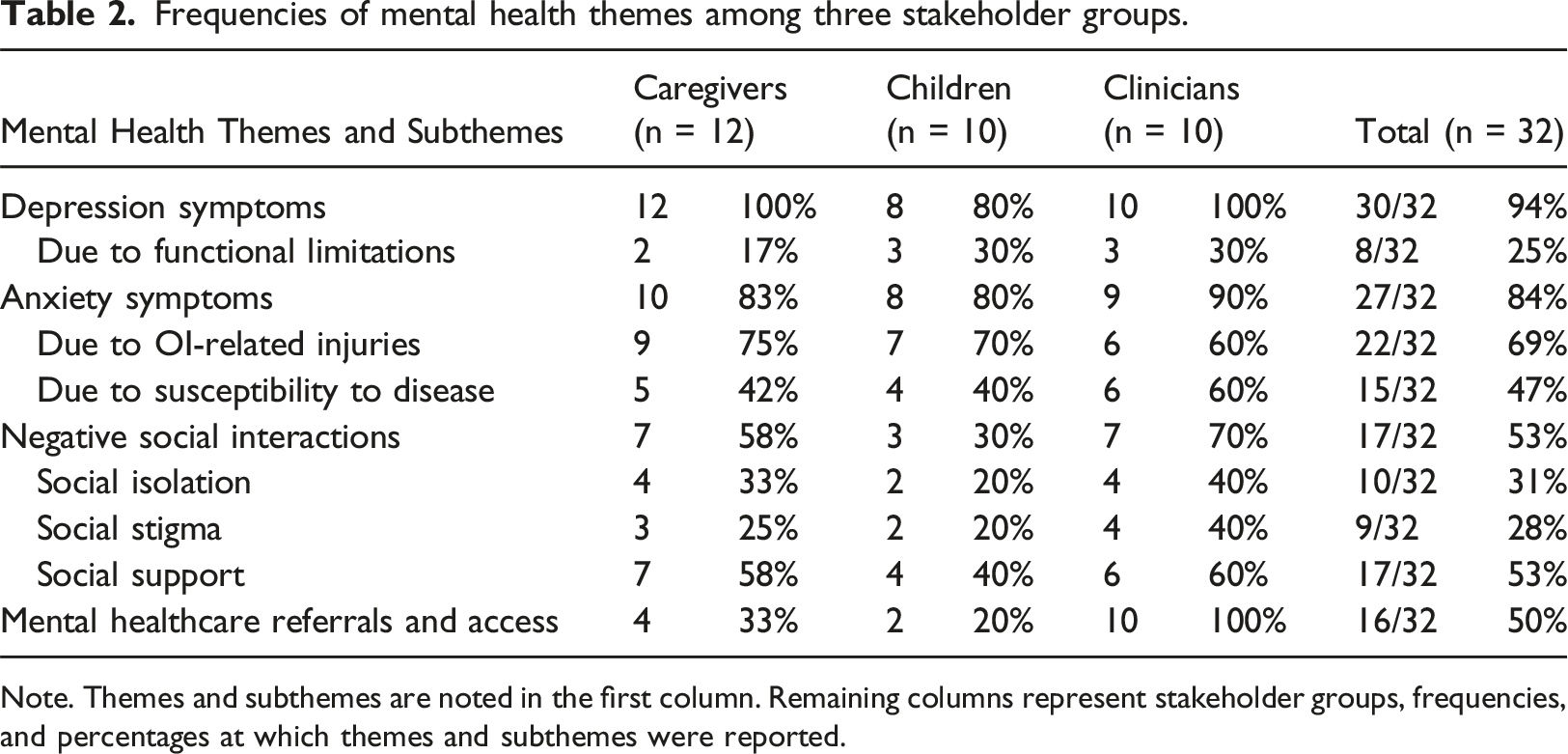
Anxiety was commonly reported by participants (10/12 caregivers (83%), 8/10 children (80%), and 9/10 clinicians (90%)). OI-related risk factors for anxiety in children included OI-related injuries (9/12 caregivers (75%), 7/10 children (70%), and 6/10 clinicians (60%)) and increased susceptibility to disease and associated comorbidities, including during the coronavirus disease 2019 (COVID-19) pandemic (5/12 caregivers (42%), 4/10 children (40%), and 6/10 clinicians (60%)). One caregiver described their child’s anxiety regarding the COVID-19 pandemic and their vulnerability, stating: “if [their child] got COVID and they had to intubate, she would be broken and cracked and she’d be dead ... fatality of COVID meant [their child’s] anxiety was off the charts”—Sally (Caregiver, White Non-Hispanic, Female, Age 64).
Most interviewees who discussed anxiety about injuries described children’s increased caution about daily and extracurricular activities (2/12 caregivers (17%), 2/10 clinicians (20%), and 6/10 children (60%)). One child described a time when they broke a bone after falling off a bike and expressed feeling apprehension about riding again, stating: “well it’s simple, just don’t get on that bike”—Andrew (Child, White Non-Hispanic, Male, Age 9, OI Type I).
In addition, another child reflected: “I probably analyze where I’m stepping and stuff like that… and I overthink especially when I fall… I overthink like, ‘is it numb to the pain or did I break it [bone]?’”—Michelle (Child, Multi-racial Non-Hispanic, Female, Age 14, OI Type III).
Although perceived severity was not formally assessed, few participants mentioned OI severity as a risk factor for depression and anxiety symptoms (1/12 caregivers (8%), 0/10 children (0%), and 2/10 clinicians (20%)).
Participants infrequently mentioned other factors, including mobility limitations and fatigue. However, these were not frequently reported, and data presented here highlight thematic consistencies and notable inconsistencies across study samples.
Positive attitudes appear to buffer against mental health concerns
Several participants identified personal characteristics among children with OI that may buffer against poor mental health (4/12 caregivers (33%), 1/10 children (10%), and 7/10 clinicians (70%)). In contrast to children with OI, a few caregivers and clinicians identified a positive attitude as a protective trait (1/12 caregivers (8%), 0/10 children (0%), and 4/10 clinicians (40%)). According to one clinician, patients who stay positive have better mental health, which in turn contributes to better overall health. However, another clinician cautioned against overemphasis on positivity, stating: “The message that we're taught is … positive attitude overcomes everything … But then it leaves people who don’t feel connected to that consistently kind of additionally feeling like, ‘Gosh, like I'm not even good at being a person with OI’”—Dr. Smith (Clinician, White Non-Hispanic, Female, Age 41).
Social isolation and stigma add mental stress, while social support was linked to reduced stress
In addition to disease characteristics and individual traits, social isolation (4/12 caregivers (33%), 2/10 children (20%), and 4/10 clinicians (40%)) and social support (7/12 caregivers (58%), 4/10 children (40%), and 6/10 clinicians (60%)) were frequently discussed as factors associated with mental health. When asked about how OI has impacted their life, a child noted: “[It impacts my] social life, mostly. And mental [health], probably because ... it takes a toll”—Michelle (Child, Multi-racial Non-Hispanic, Female, Age 14, OI Type III).
One clinician explained: “if you're not able to do the same things your peers do, even if it's going to school or playing outside, being involved in recess, that can be isolating for children and stigmatizing … [other kids] pick on differences”—Dr. Johnson (Clinician, White Non-Hispanic, Female, Age 35).
Furthermore, social isolation through bullying was highlighted by multiple participants (3/12 caregivers (25%), 0/10 children (0%), and 3/10 clinicians (30%)).
In addition to isolation, stigmas of both mental health and OI status were reported as mental health stressors (3/12 caregivers (25%), 2/10 children (20%), and 4/10 clinicians (40%)). Regarding mental health stigma, one caregiver described: “Mental health is still stigmatized. It's not sexy”—Sally (Caregiver, White Non-Hispanic, Female, Age 64).
This stigma may then deter individuals accessing mental health resources: “Society stigmatizes getting help for mental health”—Dr. Johnson (Clinician, White Non-Hispanic, Female, Age 35).
In addition, OI status is stigmatized, leading children with OI to attempt to conceal their disease: “I think in the chronic health issue community a lot of times people downplay their pain, downplay their experiences, downplay their chronic health condition”—Dr. Johnson (Clinician, White Non-Hispanic, Female, Age 35).
However, supportive family, friends, community, and disability support groups were associated with improved mental health (7/12 caregivers (58%), 4/10 children (40%), and 6/10 clinicians (60%)). Sources of support included family, friends, partners, community, and other individuals with OI. A child mentioned it can be helpful for OI kids to talk to other OI kids who relate to similar issues (Child, White Non-Hispanic, Female, Age 12, OI Type V).
Poor mental health among children with OI can be addressed with mental health referrals from providers and improved healthcare access
Half of all participants (4/12 caregivers (33%), 2/10 children (20%), and 10/10 clinicians (100%)) identified referrals for mental health care and access to mental health services as protective factors for psychosocial well-being among children with OI. According to clinician reports, primary care physicians and specialists treating OI may often be first to help facilitate access to mental health treatment for people with OI. When a mental health screening question elicits a concern, one simple follow-up step is making a referral. Five clinicians (5/10, 50%) discussed how non-mental health providers can address patients’ mental health needs with referrals. To make referrals easier, some clinicians work in a multidisciplinary team, including social workers, psychologists, or psychiatrists, making referrals easier (5/10 clinicians, 50%). However, not all clinicians make mental healthcare referrals. As one caregiver (1/12, 8%) mentioned: “The palliative care team was incredibly helpful … setting up Medicaid and all those other, you know, medical resources, but they did not hook us up with mental health stuff”—Rachel (Caregiver, White Non-Hispanic, Female, Age 36).
Participants also discussed how mental health resources are not always available. Limited healthcare access (8/12 caregivers (67%) and 5/10 clinicians (50%)) was a commonly reported issue, especially for mental healthcare (7/12 caregivers (58%) and 5/10 clinicians (50%)). Financial barriers (2/12 caregivers (17%) and 2/10 clinicians (20%)) and location (4/12 caregivers (33%) and 2/10 clinicians (20%)) were barriers to mental healthcare access. According to one clinician, “finding a specialist is ideal, but you don't want to not get treatment because you can't find a specialist”—Dr. Smith (Clinician, White Non-Hispanic, Female, Age 41).
In response to access issues, one caregiver and one clinician proposed telehealth expansion as a solution. Caregiver appreciated that telehealth enabled access to behavioral and OI specialists (Caregiver, White Non-Hispanic, Female, Age 36). However, they still had poor access to necessary in-person services, such as ER visits.
Discussion
We conducted semi-structured interviews with children with OI, caregivers of children with OI, and OI clinicians to assess mental health among children with OI. Thematic analysis was used to identify salient themes. Depression among children with OI was consistent with existing OI literature indicating that post-fracture depressive symptoms are common among adults with OI (Rork et al., 2023) and associations between illness-induced functional impairment and depressive symptoms (Hill et al., 2019; Williams and Murray, 2015). Functional impairment may contribute to depressive symptoms (Hill et al., 2014, 2019). Like adults, children with OI may experience depressive symptoms like those with other chronic illnesses (Barker et al., 2023). However, while other chronic illnesses result in higher rates of clinical depression compared to those without chronic illness (Uhlenbusch et al., 2019, 2021), more research is needed on whether this pattern extends to pediatric OI. Qualitative reports of depression symptoms cannot be equated with clinical diagnoses of mood disorders by a mental health professional. If rates of clinical depression are indeed greater in children with OI than in unaffected children, further work may be needed to tailor psychotherapy and pharmacotherapy for this specific population. Additionally, it may be beneficial for providers to use their platform to advocate for integrated care between OI medical care and pediatric psychology.
Study participants also noted children with OI have anxiety about future injuries, similar to findings in adults (Rork et al., 2023) and other children, who were cautious even with minor physical activities (Dung et al., 2013). Associations between COVID-19 and anxiety due to high risk of complications with comorbid OI have not been examined previously. This pattern is consistent with COVID-related anxiety among other disease populations, including diabetes and hypertension (Salah et al., 2023). While COVID concerns are likely context dependent, future pandemics and world events may contribute to similar concerns. It is also important to note anxiety can be adaptive in certain circumstances (e.g. COVID-19), as those with OI exhibit greater risk of morbidity and mortality compared to those without OI (Smyth et al., 2023). Physical limitations attributable to OI exacerbate mental health concerns and overall well-being. Prior research suggests that long-term physical disability is associated with increased risk for psychological problems in children (DeMaso et al., 2009) and increased duration of poor mental health among those with chronic conditions (Froehlich-Grobe et al., 2016). Therefore, an important therapeutic target for OI patients may be healthy coping with disease-specific limitations.
Healthy problem-focused coping in chronic illness consists of two seemingly contradictory coping mechanisms: a belief in overcoming limitations and acceptance of limitations (Bombardier et al., 1990). Acceptance-Commitment Therapy may show promise for addressing mental health problems among children and families of children with OI. This psychotherapeutic modality is focused on principles of acceptance, or welcoming psychological experiences without trying to change them (Hayes et al., 2006), and has shown promise among other disease populations, including cancer (Jiang et al., 2024), epilepsy (Lundgren et al., 2006), pediatric neurologic injury (Brown et al., 2014), and pediatric chronic pain (Pielech et al., 2017). Mindful Self-Compassion (MSC) programs, consisting of self-kindness, management of negative thoughts, and acceptance of negative experiences, may be explored in pediatric OI populations (Edwards et al., 2019). MSC has resulted in decreased anxiety and increased illness acceptance in adults with chronic pain (Torrijos-Zarcero et al., 2021), and similar approaches may benefit children with OI.
Children reported functional limitations as a cause of depression much less frequently (1/10 children) than caregivers (7/12) and clinicians (4/10). Specific to chronic illnesses such as OI, children may have lower insight regarding their physical limitations relative to caregivers and clinicians. It is possible these children do not perceive their experiences as different or informed by OI, as they do not know a life without OI (Dogba et al., 2013). In contrast, their healthcare providers and caregivers may not necessarily have OI themselves and are more likely to identify differences. Functional limitations are related to desire for independence (Hill et al., 2014). However, more research is needed to determine an optimal compromise concerning independence. While parents overprotect to prevent injuries, learning through experience may help children develop more realistic estimations of their physical abilities (Plumert, 1995).
Infrequent mention of OI type is consistent with previous research, in which OI Type III was not associated with worse mental health than less severe types (Wehrli et al., 2023). This pattern may be due to patients with severe, long-term illnesses developing resilience in response to their illness (McDonald et al., 2023). Notably, 5 out of 10 children identified as having OI Type I, presenting limitations in sample sizes for severe types. Positive attitude was cited as a protective personal quality by caregivers and clinicians but not children. These children may have more limited insight into their disease state and their reaction to their condition. In contrast, clinicians see multiple children with OI and can compare children with more positive attitudes versus those with more negative attitudes.
Perspectives on positive attitude were consistent with literature connecting optimism with improved mood and quality of life in chronic illness (Hurt et al., 2014). Illness cognition referring to how an individual processes their disease experience to emphasize negative aspects, diminish aspects, or add positive meaning (Evers et al., 2001) appears to be relevant among those with OI. Positive cognition (e.g., high acceptance and low helplessness) among other chronic disease populations has been associated with better physical and mental health, including reduced anxiety and depression (Verhoof et al., 2015). Positive attitude may also be related to resilience, which has been associated with lower depression and anxiety symptoms in adolescents with orthopedic conditions (Miyamoto et al., 2023). Further research is needed to better understand how illness cognition can buffer negative psychosocial outcomes among those with OI. Social isolation concerns are consistent with a previous systematic review that identified social challenges as mental health domains most significantly impacted by OI (McDonald et al., 2023). Social isolation is associated with anxiety, depression, increased cortisol levels, and worse cognitive development in children and adolescents (Almeida et al., 2021). Therefore, social isolation may serve as a psychosocial treatment target for pediatric OI populations. Stigma of OI status was also reported as a factor contributing to adverse psychosocial outcomes. Among individuals with chronic illness, perceived discrimination and stereotypes have previously been associated with greater levels of depression and anxiety (Grover et al., 2021).
Close relationships have been identified as protective against depressive symptoms in chronic illness populations, while having many diffuse relationships and receiving emotional support buffer against depressive symptoms (Penninx et al., 1998). Social support is linked to improved mental health, self-efficacy, and positive health behaviors in those with chronic disease (Reblin and Uchino, 2008). Interventions targeting social support also have benefits. Support groups increase illness acceptance, and CBT teaching psychosocial skills improves utilization of existing social ties, improving quality of life and reducing loneliness (Reblin and Uchino, 2008). Social support has an inverse relationship with perceived social stigma (Grover et al., 2021).
Clinicians were much more likely to mention referrals as a protective factor, compared to caregivers and children. This discrepancy may be explained by clinician involvement in making referrals, while caregivers and especially children may have less understanding of differences between healthcare specialists. Although mental health referrals are beneficial, physicians may struggle to provide them due to inadequate insurance coverage and low supply of mental health providers (Trude and Stoddard, 2003). This shortage is worsened by uneven distribution; non-urban areas have a particularly poor ratio of psychiatrists to inhabitants (Ku et al., 2021). Underserved counties designated as Health Professional Shortage Areas (HPSAs) do significantly worse in mental health metrics, such as suicide rate (Ku et al., 2021). This shortage is compounded by children with OI and their caregivers often having trouble finding professionals familiar with OI (Hill et al., 2019).
Telehealth, mentioned by several respondents, has evidence in treating various mental health conditions, including anxiety and depression (Bulkes et al., 2022), which may benefit underserved areas. Services, including Psychology Interjurisdictional Compact allowing license reciprocity across State lines for psychologists, may expand telehealth access; similar efforts to increase access to care may be considered in other jurisdictions or countries (Webb and Orwig, 2015).
Group model health maintenance organizations (HMOs) allowed greater ease in making mental health referrals (Falkson and Srinivasan, 2023). HMOs facilitated multispecialty coordination efforts since different providers often worked together in one entity and location. Similarly, in our study sample, clinicians commonly explained how mental healthcare is enhanced by multidisciplinary clinics, where mental health providers work alongside OI clinicians.
Limited research on psychiatric treatment among those with OI further exacerbates issues related to care. Unlike conditions such as cancer, OI does not fall under jurisdiction of professional organizations such as the American Psychosocial Oncology Society, which connects mental health professionals for networking and sharing research. Individuals with OI are supported by a robust patient advocacy system (i.e., OIF); partnering with these groups may facilitate development of personalized training protocols.
Study limitations
This study has limitations. First, although themes related to mental health were reported, future quantitative research is needed to verify findings associated with OI. Second, while this study examined symptoms resembling depression and anxiety, this approach is not a replacement for diagnosis by a clinician. Future studies should seek to replicate and expand findings here through use of formal diagnostic measures for mood and anxiety disorders. Third, study samples were homogenous, with limited diversity across racial identity and OI types, and no assessment of perceived severity. Future studies ought to assess self-reported or subjective OI severity in addition to OI type (e.g., Westerheim et al., 2024). A more diverse sample would also help elucidate themes of intersectionality with racial and ethnic identity with OI status to more fully understand psychosocial needs. Additionally, greater representation of OI types may yield specific healthcare needs related to those subtypes. Fourth, further research can explore mental health themes beyond limited codes of depression, anxiety, and risk/protective factors.
Implications for practice
Results suggest assessment of anxiety and depression may be warranted in OI treatment settings. Functional limitations and social isolation may contribute to these concerns, and assessment may be appropriate following injury and/or medical interventions. Convergence across all groups suggests parents, who may first notice anxiety and depression in their child, should voice concerns with treating providers. Providers should be vigilant in monitoring symptoms and providing appropriate referrals. Finally, pediatric OI specialty clinics should consider incorporating pediatric health psychologists and psychiatrists to improve access to mental healthcare. Further large-scale studies, including intervention research, are warranted before system level changes can be implemented.
Conclusion
Qualitative interviews of children with OI, caregivers, and clinicians yielded four major themes about mental health. First, depressive and anxious symptoms were commonly reported among participants. Second, functional limitations were a common risk factor for depressed mood and anxiety, while a positive attitude was protective for individuals with OI. Third, social isolation and social support were frequently cited as risk and protective factors, respectively. Fourth, access to mental healthcare and multidisciplinary clinics with mental health providers are key healthcare needs for children with OI. Discrepancies with thematic frequencies and content were observed across study samples. These findings add to existing literature on mental health in children with OI, by assessing themes and comparing across three participant groups. Findings here suggest future research would benefit children with OI by increasing mental health awareness and treatment options.
Members of the BBDC
The “Members of the BBDC” include Brendan Lee, V. Reid Sutton, Sandesh CS Nagamani, Frank Rauch, Francis Glorieux, Jean-Marc Retrouvey, Janice Lee, Paul Esposito, Maegen Wallace, Michael Bober, David Eyre, Danielle Gomez, Gerald Harris, Tracy Hart, Mahim Jain, Deborah Krakow, Jeffrey Krischer, Eric Orwoll, Lindsey Nicol, Cathleen Raggio, Peter Smith, and Laura Tosi.
Footnotes
Acknowledgements
We extend our gratitude to all who participated in this study. We would also like to acknowledge the Osteogenesis Imperfecta Foundation, their members, and all individuals and their families living with OI. We would also like to acknowledge the contributions of Mr. W. Conor Rork.
Author Contributions
Justin H. Qian: formal analysis, writing—original draft and writing, and writing—review and editing; Andrew D. Wiese: participant recruitment, data acquisition, formal analysis, writing—original draft and writing, and writing—review and editing; Clarissa Gonzalez: formal analysis, writing—original draft and writing, and writing—review and editing; Whitney S. Shepherd: formal analysis and writing—review and editing; Hannah Cho: formal analysis and writing—review and editing; Gianna M. Colombo: writing—review and editing; Julia Morales: writing—review and editing; Kristin M. Kostick-Quenet: formal analysis; writing—review and editing; Diane Nguyen: project administration; Sophie C. Schneider: conceptualization and writing—review and editing; Members of the BBDC: conceptualization and writing—review and editing; Marie-Eve Robinson: writing—revising and editing; Chaya N. Murali: data acquisition, writing—original draft, and writing—revising and editing; Brendan Lee: conceptualization, funding acquisition, project oversight, and writing—review and editing; V. Reid Sutton: conceptualization, funding acquisition, project oversight, and writing—review and editing; Eric A. Storch: conceptualization, funding acquisition, project oversight, and writing—review and editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Mr. Qian, Dr. Wiese, Ms. Gonzalez, Ms. Shepherd, Ms. Cho, Ms. Colombo, Ms. Morales, Ms. Guo, Dr. Kostick-Quenet, Ms. Ngueyn, and Dr. Schneider report no completing interests to declare. *Dr. Ayers declares the following relationship: Osteogenesis Imperfecta Foundation Board of Directors member. *Dr. Robinson discloses the following relationships: research support from Ascendis Biopharma and Ipsen Biopharmaceuticals and consultant for Ultragenyx and Ipsen Biopharmaceuticals. *Dr. Murali discloses the following relationships: past research support in the last 12 months from BioMarin Pharmaceuticals. *Dr. Lee discloses the following relationships: research support from Sanofi and Kyowa-Kirin. *Dr. Sutton discloses the following relationships: research funding from Ultragenyx; Osteogenesis Imperfecta Foundation Board of Directors member. *Dr. Storch discloses the following relationships: consultant in the past 12 months for Biohaven Pharmaceuticals and BrainsWay; book royalties from Elsevier, Springer, American Psychological Association, Wiley, Oxford, Kingsley, and Guilford; stock valued at less than $5000 from NView for distribution of OCD scales; and research support from NIH, International OCD Foundation, Ream Foundation, and Texas Higher Education Coordinating Board.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS) and National Institute of Mental Health under Award Number U54AR068069-S1, and by the Eunice Kennedy Shriver National Institute of Child Health and Human Development of the National Institutes of Health under Award Number P50HD103555 for use of the Clinical and Translational Core facilities. The Brittle Bone Disease Consortium (1U54AR068069-0) is a part of the National Center for Advancing Translational Sciences (NCATS) Rare Diseases Clinical Research Network (RDCRN) and is funded through a collaboration between the Office of Rare Diseases Research (ORDR), NCATS, the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), the National Institute of Dental and Craniofacial Research (NIDCR), the Eunice Kennedy Shriver National Institutes of Child Health and Development (NICHD), and the National Institute of Mental Health (NIMH). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Data Availability Statement
The data that support the findings of this study may be available upon request to the corresponding author. Data are not publicly available due to privacy and ethical restrictions.