
Abstract
When pediatric services are not coordinated, children, youth, and their caregivers cannot always access the right services at the right time. Guidance is needed for how pediatric services should be planned and organized to improve integrated care. The objective of this rapid scoping review was to map and characterize current evidence on standards of care for integrated pediatric levels of service. This rapid scoping review was conducted in accordance with Cochrane Rapid Reviews Interim Guidance. We searched academic databases and gray literature in 2022, published in English from Canada, United States, United Kingdom, Australia, New Zealand, with no date parameter. Fifty-three sources met inclusion criteria and were included in this review. Levels of service frameworks categorized services into three, four, or six distinct levels. Eight sources described integrated levels of service. Most pediatric standards of care frameworks defined levels of service by roles and responsibilities. Differences were defined by transitions between levels of care, planning for services across urban and rural communities, and coordinating integrated levels of service. Future research is required to build evidence base of how levels of service frameworks can be used in practice, adapted to local contexts, and evaluated.
Introduction
Access to comprehensive and coordinated care is critical for delivering quality pediatric care (American Academy of Pediatrics et al., 2012). Children and youth (younger than 18 years of age) and their caregivers are often challenged with managing and coordinating care within health systems that silo pediatric clinical services by subspecialty and function independently of one another with varying levels of care (Meehan et al., 2019). When pediatric health services are not integrated across care settings, children and their caregivers cannot access the right services at the right time and experience worse health outcomes (Allen et al., 2009). A lack of integrated care also presents challenges for decision-makers to allocate resources efficiently and effectively with equitable standards of care that meet health needs of pediatric patients across urban and rural settings (Canadian Institutes of Health Research, 2020; Leatt et al., 2000; Wolfe et al., 2020).
When health services are integrated through co-location of services and sharing of information, they have the potential to generate significant health benefits, including improved quality patient-centered services, reduced health system costs, and meeting continuum of care needs (Armitage et al., 2009; Kelly et al., 2020; Shortell et al., 1994; Suter et al., 2009; World Health Organization, 2016). Integrated care has been defined through functional integration (coordination of financial and information management and human resources), care provider integration (collaborative relationships between care providers and extent that care providers are economically linked to a system and actively participate in its planning and management within leadership positions), and clinical integration (continuity and coordination of care, disease management, and sharing of information) (Conrad and Shortell, 1996; Devers et al., 1994; Leatt et al., 2000). Health systems commonly achieve integrated care through horizontal and vertical integration of services (World Health Organization, 2016). Horizontal integration occurs when health organizations delivering the same level of service come together (Heeringa et al., 2020; World Health Organization, 2016). For example, a single specialty group practice would merge into a team of multidisciplinary healthcare professionals delivering similar services at one collaborative care clinic (Mezzalira et al., 2024). Vertical integration occurs when health organizations or programs delivering different levels of care come together (e.g., primary care, acute care, post-acute care) (Heeringa et al., 2020; World Health Organization, 2016). For example, different levels of care merge within one acute care hospital setting to provide a range of general and subspecialty care including pharmacy services, diagnostic imaging and laboratory services, and post-acute rehabilitation (Amado et al., 2022).
When pediatric health services are integrated, children and their caregivers have improved access to healthcare services and quality of care as close to home as possible. Pediatric-specific integrated models of care improve quality of life, reduce health care use and system costs, lower family expenses by minimizing travel, enhance communication between providers and caregivers, and strengthen family-centered plans that address medical and social needs of children and caregivers (Adams et al., 2013; Allen et al., 2009; Satherley et al., 2021; Wolfe et al., 2020). For example, when pediatric mental health care services are integrated within collaborative care teams, children and their caregivers have increased access to behavioral health treatment and experience improved mental health outcomes (Burkhart et al., 2020). Achieving integrated pediatric care remains challenging due to fragmented funding models, disconnected administrative, organizational, and service structures (Cumming, 2011), and the complexity of coordinating services for children with diverse health conditions across different developmental stages (Cohen and Coller, 2020; O’Shea et al., 2018). Improving integrated care is particularly important for children and youth with medical complexity that require subspecialty care and more frequent use of primary health care services, hospital care, and emergency department care for chronic conditions such as malignant neoplasms, cardiovascular diseases, and gastrointestinal diseases (Adams et al., 2013; Canadian Institutes of Health Research, 2020).
Coordinating integrated care from multidisciplinary teams is challenging for children at different developmental stages and across different community settings. Multidisciplinary care teams commonly experience time constraints for interprofessional collaboration, inadequate training in collaborative care settings, frequent turnover of professionals, and meeting specialized needs of children while addressing family-centered needs of multiple caregivers (Nooteboom et al., 2021). Further, planning and coordinating integrated pediatric care across different community settings is challenging for communities with different levels of service available to meet pediatric population health needs. Countries with large geographical territories spanning urban and rural communities must coordinate levels of service across rural or remote communities with low population density and fewer resources to deliver more specialized care (Waibel et al., 2021).
Levels of service definition and terminology.
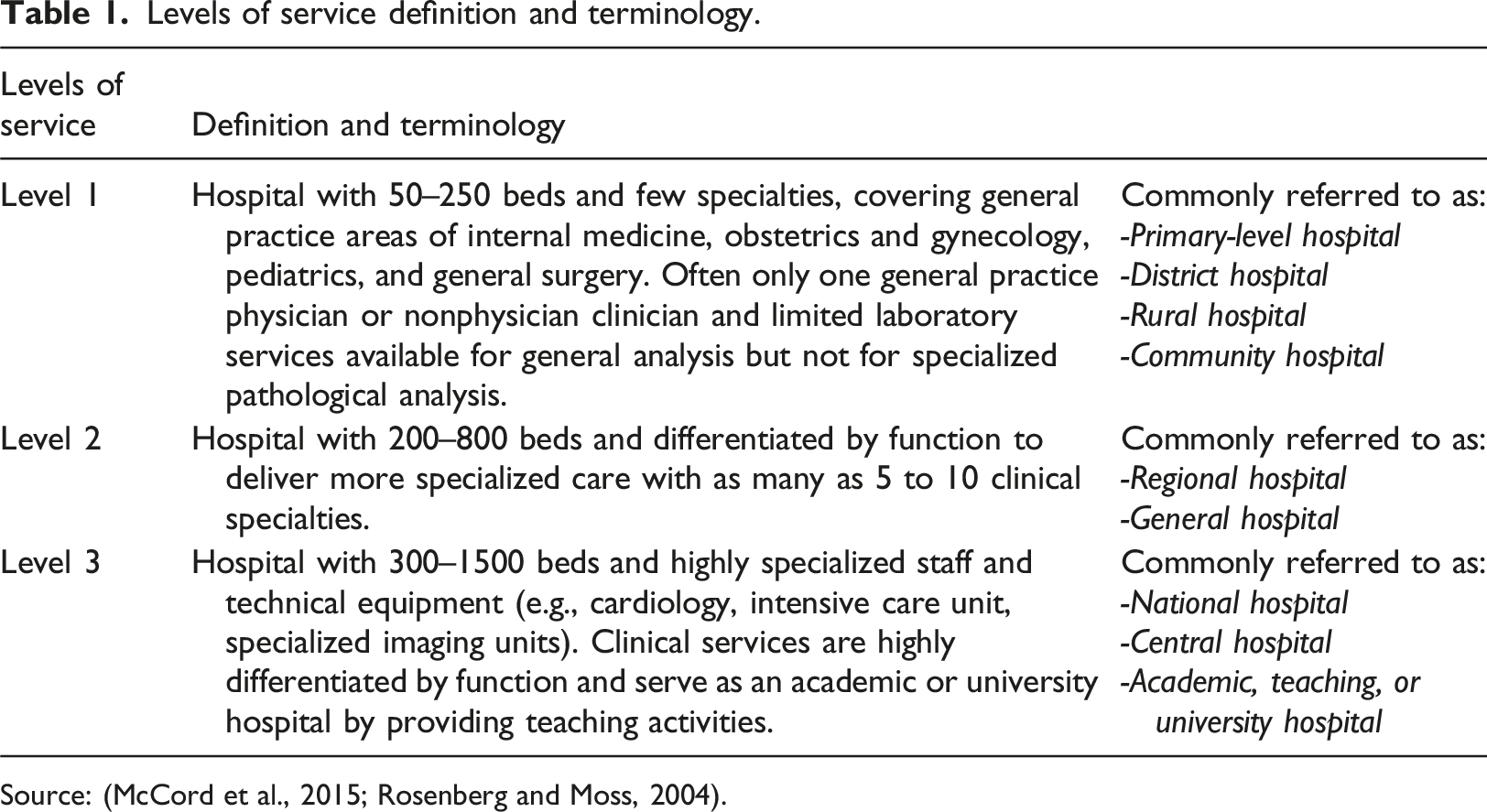
Source: (McCord et al., 2015; Rosenberg and Moss, 2004).
An overview of evidence defining standards of care and integrated levels of service is critical for decision-makers. Integrated levels of service frameworks are needed to provide a guide for systems planning across organizations and geographical boundaries. For example, it could allow decision-makers to promote active health service planning such as allocating appropriate resources, staffing, roles, equipment, supports, etc., needed to provide timely and equitable access to care based on available financial and health human resources at local, regional, and provincial levels. Integrated and coordinated levels of service also promote quality and patient safety while reducing redundancies and inconsistencies in care. For example, integrated care could enhance delivery of person and family-centered services by matching the appropriate level of care with pediatric needs and coordinating commonly accessed services like primary care as close to home as possible.
Aim
To map and characterize current evidence on standards of care for integrated pediatric levels of service. Our objectives were to: 1. Identify standards of care for pediatric clinical service delivery 2. Describe how pediatric levels of service are defined and integrated
Methods
This rapid scoping review was conducted in accordance with Cochrane Rapid Reviews Interim Guidance from Cochrane Rapid Reviews Methods Group (Garritty et al., 2020).
Inclusion criteria
The most recent literature and jurisdictional review (Waibel et al., 2021) was conducted to develop a framework for defining and planning pediatric services across British Columbia, Canada. This review focused on a limited search of academic peer-reviewed literature published within MEDLINE since 2008. Our rapid scoping review expands a search to include multiple academic and gray literature sources of pediatric clinical services without a date parameter.
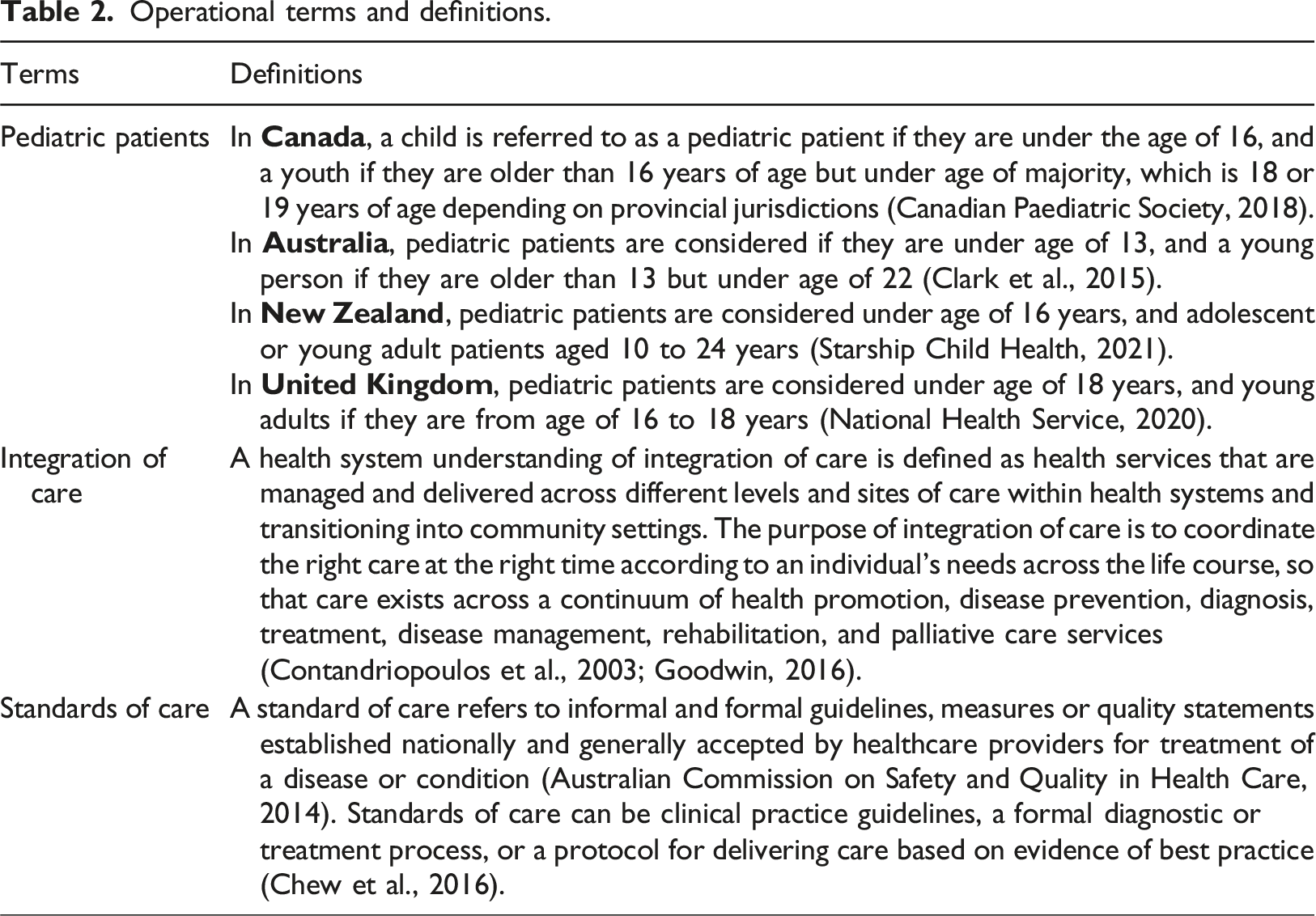
Operational terms and definitions.
Population
This review is focused on pediatric clinical services designed and delivered for children and youth younger than 18 years, age of majority for many countries including Canada, Australia, and United Kingdom (UK).
Concept
This review includes literature exploring pediatric standards of care and levels of service coordinated across regions with varying resources. Coordination of care is particularly a challenge for countries with large geographical territories spanning urban and rural communities, as rural or remote communities with low population density have fewer resources delivering level or tier one services in comparison to densely populated cities with greater resources to deliver higher and more complex levels of service.
Context
This review includes literature focusing on delivery of pediatric services across different clinical areas including oncology, palliative care, general, emergency, maternal and newborn health, and other subspecialty care areas. During data extraction and data presentation phases, we documented what pediatric clinical service areas are included in the evidence.
Search strategy
Our search strategy aimed to locate published peer-reviewed literature and gray literature. A list of academic and gray literature sources, keywords, and index terms were developed by all team members in conjunction with a health sciences librarian. A search of databases was executed by a health sciences librarian on our research team.
First, a limited search of MEDLINE (Ovid) was conducted to identify academic sources on this topic. Text words contained in titles and abstracts of relevant articles (Ogle et al., 2018; Rosenberg and Moss, 2004; Waibel et al., 2021) and index terms describing articles were used to develop a full search strategy for MEDLINE including variations of (child OR adolesc OR pediat OR paediat); (standard? OR level? OR tier OR framework); (care OR service? OR health); (standard of care); (integrat OR coordinat OR comprehensive); (care OR service? OR health); (delivery of health care) (see Supplemental Table I).
Our search was developed using three main concepts: pediatrics, standards of care, levels of care, and integration or coordination of care. A pediatric search filter (Tjosvold et al., 2020) was modified for our needs and used to define pediatrics. A MEDLINE search was translated to Embase (Elsevier), Cumulative Index of Nursing and Allied Health (CINAHL) Full Text (EBSCO), and Scopus (Elsevier) and run on June 30, 2022 from inception (see Supplemental Table I for all database searches). Due to time constraints and in line with Cochrane’s rapid review guidance, our database searches were not peer-reviewed by a second health sciences librarian. Reference lists of included academic articles included were manually screened and a forward search of article titles that met inclusion criteria was conducted by one reviewer.
Google was used to source gray literature from Canada, UK, New Zealand, Australia, and United States (US). Focusing on selected high-income countries allows for an in-depth search of sources and comparison between countries with similar tiered health systems and resources for delivering services across large geographical areas (Canadian Institutes for Health Information, 2019). Two different Google searches (Supplemental Table II) were run five times (10 searches total), using country search filter on Google’s advanced search page. Sources from first five pages of results were screened, and relevant websites uploaded to an Excel document. Gray literature sources included websites, organizational reports, policy literature, and government documents.
Study selection
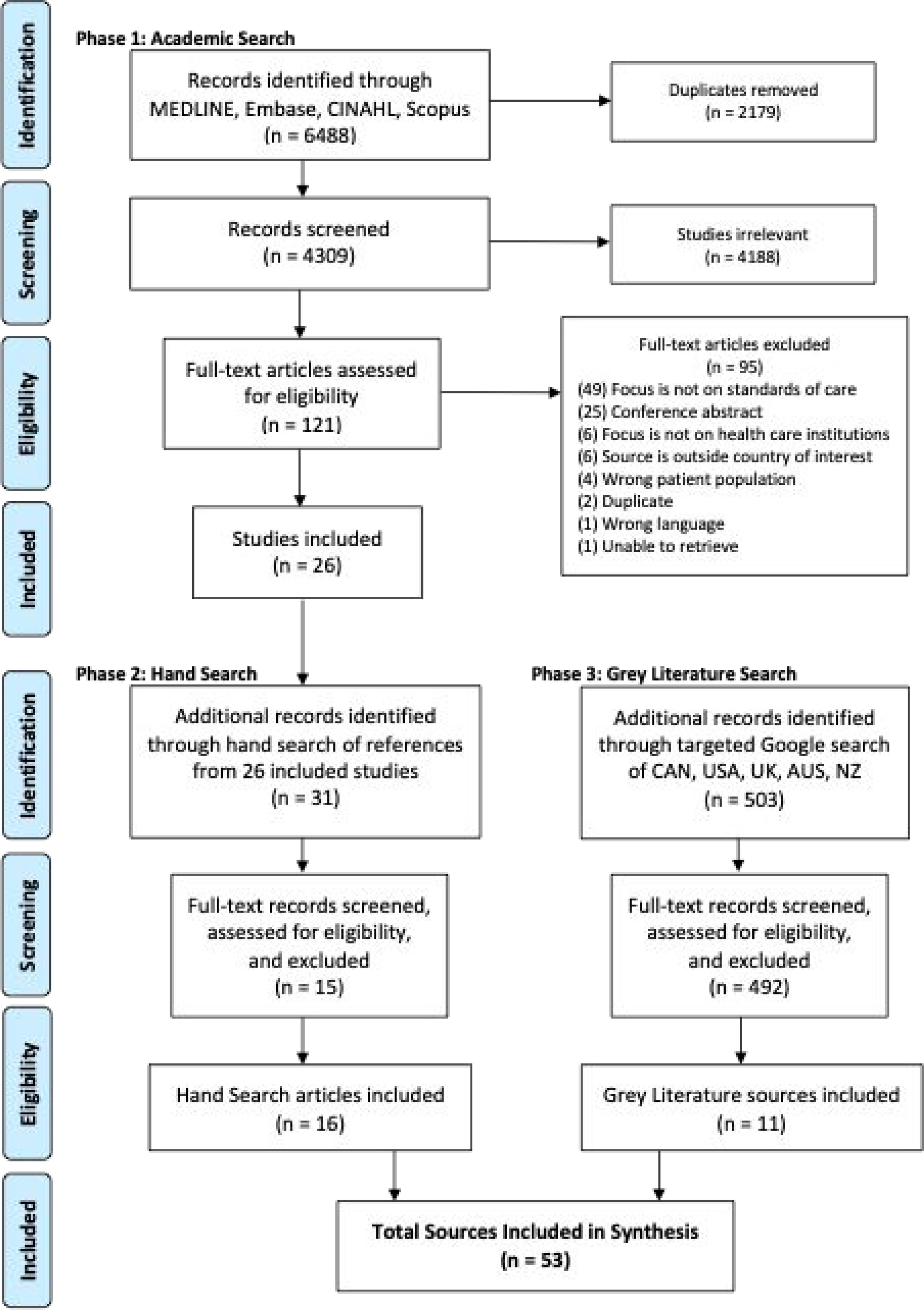
Phase 1: All records identified through database searches were uploaded into Covidence (Covidence Veritas Health Innovation Ltd, 2023), a screening management system, and duplicate records removed. Title and abstracts were screened independently by two reviewers for assessment against the eligibility criteria. Full texts of potentially relevant articles were uploaded into Covidence and assessed in detail against inclusion criteria by one reviewer (Garritty et al., 2020). Results are reported using the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) checklist (Tricco et al., 2018) and presented within Figure 1 PRISMA flow diagram (Page et al., 2021). Reason for exclusion of full text articles that did not meet inclusion criteria are reported in Figure 1. Phase 2: Reference lists of included academic sources were hand searched by one reviewer to identify additional sources with titles that included key terms such as pediatrics, standards or guidelines of care, levels of service, and integration or coordination of care. The citation information for potentially relevant sources was recorded within an Excel document for full text review. Full text articles were assessed against eligibility criteria by one reviewer. Phase 3: Google searches were split between two different reviewers. Each reviewer ran their searches and screened first five pages of results directly in Google. Citation information of potentially relevant sources was added to an Excel document and duplicates manually removed. Full text sources were assessed against inclusion and exclusion criteria by one reviewer. All sources with sufficient information on pediatric standards of care and levels of service were included. Gray literature sources included websites, organizational reports, policy literature, and government documents. Sources that did not focus on pediatric standards of care or did not provide enough information for data extraction were excluded. Prisma flow diagram.
Data extraction
Data were extracted from each source by two independent reviewers using our data extraction tool developed by the research team (Supplemental Table III: Data Extraction Instrument). Extracted data included specific details about author(s); year of publication; title of source; country of origin; study aim/purpose; study population (children age, diagnoses); pediatric clinical service area; study setting (healthcare/ clinical setting); study design; guidelines of care; reported health systems outcomes; integration with other services; and implementation strategy (barriers or facilitators).
Analysis
A narrative synthesis of data extraction results was conducted, integrating key characteristics of included sources to develop a comprehensive overview of the evidence base. Findings were categorized by pediatric clinical service areas and healthcare settings, enabling identification of trends in care guidelines, levels or tiers of service, integration approaches with other services, and associated health system outcomes.
Results
Pediatric standards of care
Academic and gray literature results describing pediatric levels of service.

Number of service levels are defined within three, four, and six levels. Services at level one provides primary and generalized health care in community and ambulatory settings, whereas services at levels three and six provide advanced and comprehensive critical care in regional/quaternary settings. For example, a framework of six tiers of service from Waibel et al. (2021) delineates minimum services each tier should be able to provide with higher tiers providing more complex and subspecialty services to larger regions and provincial populations. Tier one provides a wide breadth of general services accessible in most communities and tier six provides more comprehensive, sub-specialized services targeting complex pediatric health needs (Waibel et al., 2021). In contrast, specialty clinical services for Pediatric Intensive Care Unit (PICU) (Rosenberg and Moss, 2004) are defined by two levels of care, where level one manages most severely ill pediatric patients with subspecialty multidisciplinary care teams and level two stabilizes critically ill pediatric patients before transferring to a level one center. Differences between service levels and delineation of role and responsibilities of each level are specific to clinical service areas.
Most levels of service were reported by US (n = 8), Canada (n = 7) and UK (n = 6), with general pediatrics the most advanced (n = 6) reporting tiers of service (Table 3). Within US, standards of care for Women and Newborn Health are defined by four levels of care including a classification system of consistent definitions for neonatal care and organization of levels of maternal care by institution, state health department, regional and national organizations. Services are delineated within four levels of care by roles and responsibilities of healthcare providers delivering general, specialty, subspecialty care for complex conditions, and most complex and critically ill women and newborns (American Academy of Pediatrics et al., 2012; Barnea et al., 2021; Kilpatrick et al., 2019). Within Canada (British Columbia), standards of care for general pediatrics are defined by six tiers of service that define roles and responsibilities for delivering care according to patient level of acuity, medical complexity, and health centers with varying resources for inpatient, hospital-based, outpatient, and community-based services (Child Health BC, 2018c; Waibel et al., 2021). British Columbia’s six tiers of service framework was developed by synthesizing standards of pediatric service delivery and consulting provincial stakeholders to enhance definitions of community- and hospital-based service areas, health promotion strategies and prevention, and determinants of health contributing to children’s health (Waibel et al., 2021). Within UK, standards of care for pediatric and adolescent mental health are defined by four tiers of service, where a range of services are coordinated through referral for service between care settings and each tier of service (Sutton Council, 2004). Four tiers of service include early intervention in community sites and settings, targeted services through community counseling, specialized mental health services, and inpatient provision and specialized units for more severe mental health challenges to be assessed and treated.
Integrated levels of service
Results of academic gray literature findings reporting pediatric integrated levels of service.
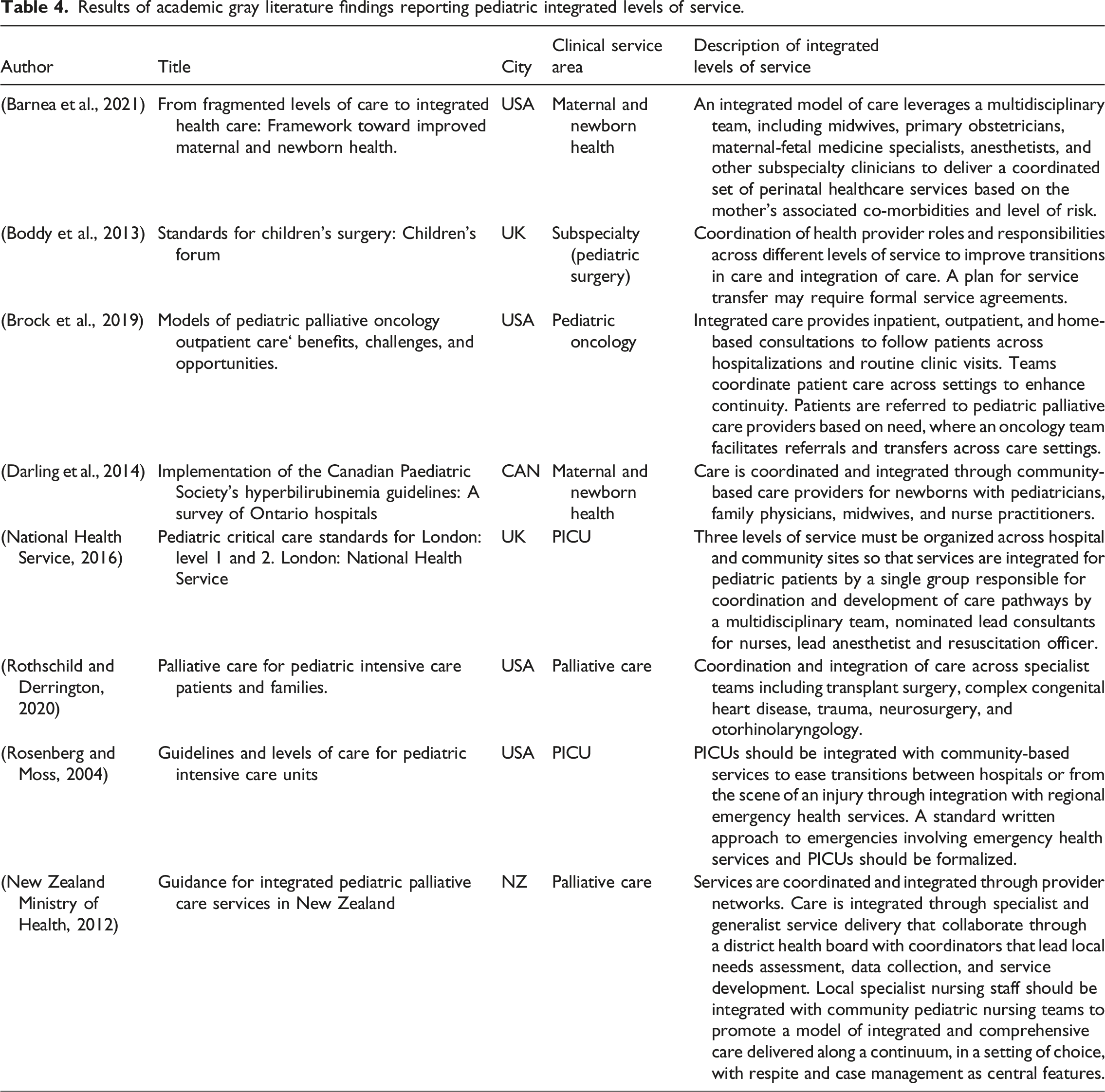
All eight sources described integrated levels of care through integration of specialist and generalist services, including coordination of roles and responsibilities for health professionals across different levels of service, agreements for transferring patients between units or sites, and use of one electronic health record system across different levels of service. New Zealand’s framework for integrated pediatric palliative care was most advanced describing a comprehensive approach for organizing and planning integrated levels of service (New Zealand Ministry of Health, 2012). New Zealand’s framework (Figure 2) describes how national specialist services are coordinated by district health boards, responsible for organizing local generalist services within hospital, community, and primary care to provide palliative care as part of general scope of practice. Both national specialist and local generalist services are linked to district health boards where a nurse coordinator and lead pediatrician coordinate local services and service development. New Zealand pediatric palliative care system relationships. Source: New Zealand Ministry of Health. Guidance for integrated pediatric palliative care services in New Zealand [Internet]. 2012. Available from: https://www.health.govt.nz/system/files/documents/publications/guidance-integrated-paeiatric-palliative-care-services-nz.pdf.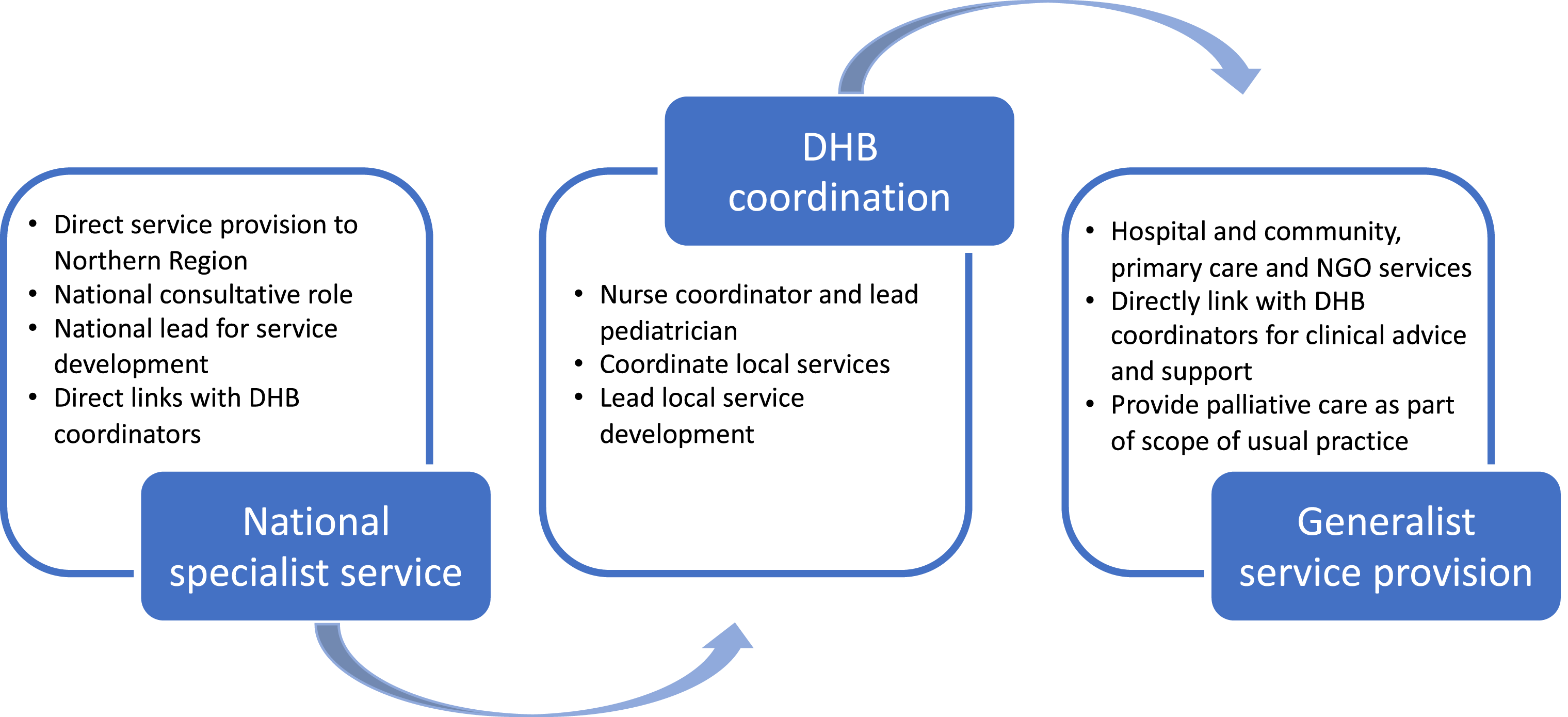
Discussion
This scoping review provides a comprehensive overview of current evidence on pediatric standards of care and levels of service, revealing critical themes that shape how care is structured and delivered across diverse settings. Thematic analysis highlighted consistent patterns in how service levels and standards of care are defined and linked to pediatric health outcomes. Importantly, the review uncovered significant geographical and contextual variations, reflecting how different countries approach pediatric service delivery based on their unique healthcare priorities. Of 53 sources identified, 27 sources reported on levels or tiers of service and eight described integrated levels or tiers of service. The US (n = 8), Canada (n = 7) and UK (n = 6) are most advanced with defining levels of service and New Zealand most advanced with describing integrated levels of pediatric palliative care. Almost all frameworks defined levels or tiers of service by increasing complexity, where higher levels or tiers provide more specialized services across larger regions and populations.
Pediatric levels of service frameworks provide important information for defining common language, practice guidelines, and planning and organizing services across jurisdictions, health care organizations, and levels of care. Levels of service frameworks we identified used a similar approach to defining levels of patient acuity and medical complexity, where each level is differentiated by roles and responsibilities of healthcare providers across care settings (e.g., community-based services, outpatient, hospital, and inpatient). Differences between country specific levels of service frameworks were defined by health system priorities such as, operationalizing roles and responsibilities of providers (Kilpatrick et al., 2019; Rosenberg and Moss, 2004), improving transitions between levels of care (Tasmanian Government, 2018), organizing and planning for services across urban and rural communities within local, regional, and state or provincial service areas (Waibel et al., 2021), and coordinating integrated services (New Zealand Ministry of Health, 2012). For example, Australia’s (Queensland and Tasmania) six tiers of service framework emphasize minimum service requirements to improve pediatric transitions across levels of care and health care settings (Tasmanian Government, 2018). Australia’s framework operationalizes roles and responsibilities of providers within each tier of clinical service to coordinate safe and continuous care management for patients moving to public or private health facilities (Queensland Health, 2014). Whereas New Zealand’s framework of three levels of service emphasizes a need for improving integrated standards of palliative care across different regions and health centers (New Zealand Ministry of Health, 2012). New Zealand operationalizes the role and responsibility of district health boards to coordinate and lead service development between nationalist specialist and generalist services by integrating palliative care services as usual scope of practice across all care settings (New Zealand Ministry of Health, 2012).
Few sources (n = 8) described integrated standards of care (Table 4), focusing on horizontal integration (coordinating care within same service levels) to reduce fragmentation and utilize multidisciplinary teams, as seen in perinatal services (Barnea et al., 2021). Vertical integration (coordinating different care levels) was described for PICU and community pathways (National Health Service, 2016), while clinical integration (continuity and coordination of care, disease management, and sharing of information) emphasized improving continuity and transitions between various care settings (Boddy et al., 2013; Brock et al., 2019; Darling et al., 2014; Rosenberg and Moss, 2004; Rothschild and Derrington, 2020). New Zealand’s integrated palliative care model exemplifies clinical and functional integration through district health boards, coordinating assessments, service development, and comprehensive care delivery (New Zealand Ministry of Health, 2012).
Integrated care frameworks are vital for coordinating pediatric services across fragmented systems, especially for pediatric patients and their families navigating specialist services and regions where urban hospitals manage rural hospitals (Cohen and Coller, 2020; Cumming, 2011; O’Shea et al., 2018). In Canada, proportions of Canadians living in rural areas vary greatly by province or territory. For example, in Atlantic provinces, most residents live in rural areas (Government of Canada, 2022), yet specialized pediatric services are centralized in Halifax, Nova Scotia. Defining roles, scopes, and responsibilities within an integrated framework could improve care navigation, reduce redundancies, and minimize delays (Splane et al., 2023). This review highlights gaps in describing and operationalizing integrated care standards, emphasizing a need for future research to refine these frameworks and clarify levels of service.
Levels of service frameworks clarify roles, responsibilities, and care standards across service levels, enabling consistent care delivery and alignment with patient needs (Rosenberg and Moss, 2004). Their practical implementation and adaptation to local contexts remains unclear (Shaw et al., 2014). We identified two case studies, from Canada and New Zealand, detailing health service planning approaches. In Canada, Waibel’s (2021) six-tier framework uses educational modules and self-assessments to enhance planning and coordination across care levels, fostering urban-rural partnerships and quality improvement. Utilizing this framework could enable stronger partnership between urban and rural sites, facilitate opportunities to learn from each other and increase understanding of rural versus urban health care contexts. These processes are particularly vital in developing countries (Carmone et al., 2020; Goma et al., 2017) where resource limitations and fragmented healthcare systems often hinder equitable service delivery. With this, improvements, innovation, and lessons learned can be shared beyond local contexts.
New Zealand is recognized for actively developing integrated approaches to pediatric services (Dempers and Gott, 2017; Garrett et al., 2020; Wodchis et al., 2015). Their 3-year phased approach for implementing pediatric palliative care provides guidance on which organizations are responsible for leading operationalization of integrated care and service development (New Zealand Ministry of Health, 2012). In year one, New Zealand established and resourced care networks, appointed and trained regional health board coordinators, developed guidelines, conducted needs assessments, and implemented after-hours support. Year two focused on disseminating guidelines, developing care coordination mechanisms, and establishing quality and research data systems. By year three, evaluation frameworks were created, and services were aligned with local Māori developments and evolving policies.
New Zealand’s approach to coordinating and implementing pediatric care exemplifies effective health system practice and sustainable change (Davies, 2006; Mackenzie et al., 2011). It integrates community networks, comprehensive provider training, and prioritizes quality improvement through needs assessments and service mapping. By using evaluation frameworks and aligning services with Māori developments, it delivers culturally responsive and evidence-based care. This strategy ensures equitable access, adaptability to policy changes, and resilience in service delivery (Wodchis et al., 2015), showcasing forward-thinking planning and collaboration to maintain high standards of care and address evolving health needs.
While these studies provide valuable insights into implementation, health system decision-makers and practitioners may benefit from using a systematic approach to guide adapting and implementing standards of care to their cultural and organizational context (Harrison et al., 2013). Drawing from implementation science literature, the three phase ADAPTE process (set-up, adaptation, and finalization) provides a systematic way for health organizations and jurisdictions to identify, critically appraise, and adapt standards of care guidelines for local use (ADAPTE Collaboration, 2009). The ADAPTE toolkit supports identifying, appraising, and adapting guidelines through three phases: preparation, adaptation, and finalization, ensuring relevance to local needs and policies (ADAPTE Collaboration, 2009). Frameworks like ADAPTE promote evidence-based decision-making, equitable resource allocation, and knowledge sharing across service levels (Bashiri et al., 2021; Fervers et al., 2011). In some cases, tertiary centers may have more resources dedicated to knowledge translation of best evidence. A levels model may accelerate knowledge translation to other sites with fewer pediatric admissions or high acuity low occurrence health conditions (Darzi et al., 2017). Standardized approaches similar to those outlined above can set the stage for comprehensive and fiscally responsible allocation of resources, services, and supports (Amer et al., 2015). From a health systems approach, this creates opportunity to share resources and knowledge, increasing capacity and quality of care provided at various levels.
Further research using similar implementation frameworks is needed to build the evidence base on how to operationalize and evaluate integrated pediatric levels of service frameworks in health systems. Researchers and health system partners should identify barriers and facilitators to implementing standards of care frameworks and develop tailored strategies to support their implementation. Further, evaluation efforts, including both process and outcome evaluations, are needed to examine impacts of these standards of care frameworks on achieving the quintuple aim of including improved patient, provider, health system, population, and health equity outcomes (Gerlach and Varcoe, 2021).
Strengths and limitations
This rapid scoping review has several notable strengths. Rigor and quality were upheld by following established scoping review methodologies from PRISMA-ScR guidelines. A clearly defined protocol guided the review process, incorporating comprehensive search strategies across academic and gray literature, independent screening and data extraction by multiple reviewers, and thorough documentation to ensure transparency and consistency. There are also important limitations to consider. First, the review was limited to English-language publications, which may have excluded relevant evidence published in other languages. Second, the focus on high-income countries (Canada, US, UK, Australia, and New Zealand) limits the generalizability of findings to low- and middle-income contexts, where health system structures and resource constraints differ significantly. Finally, the search was restricted to publicly available sources, omitting internal or unpublished documents such as health organization policies and procedures, which may offer valuable insights into how pediatric service delivery frameworks are implemented in practice.
Implications for practice
This review highlights the importance of adopting standardized pediatric levels of service frameworks to support consistent, equitable, and coordinated care delivery across diverse healthcare settings. Defining clear roles and responsibilities within these frameworks enables improved care planning, reduces fragmentation, and supports transitions between care levels, particularly vital for children with complex needs and for regions with urban-rural disparities in service access. Health system leaders and practitioners can look to models from countries like New Zealand, Australia, and Canada for practical strategies on operationalizing standards of care. Implementing evidence-based frameworks, such as the ADAPTE process, can guide local adaptation and foster collaboration across service levels, while also supporting culturally responsive care. As pediatric health systems face increasing demands, integrating these frameworks into practice offers a pathway toward more efficient, patient-centered, and sustainable service delivery.
Conclusion
Pediatric standards of care and integrated levels of service frameworks provide important information for defining common language, practice guidelines, and planning and organizing services across jurisdictions, health care organizations, and levels of care. This review identified pediatric standards of care and integrated levels of service frameworks; however, health organizations would benefit from learning how other jurisdictions implement and adapt models of service delivery to local population needs and resources available. There is a need to strengthen processes for adapting pediatric standards of care to local contexts by engaging health system decision-makers, patients, and families as stakeholders impacted by guidelines. Further research is needed to build an evidence base of processes for operationalizing and implementing integrated services to advance ultimate goals of improving pediatric care that is comprehensive and coordinated across different service regions and levels of care.
Supplemental Material
Supplemental Material - Standards of care for pediatric clinical service delivery: A rapid scoping review
Supplemental Material for Standards of care for pediatric clinical service delivery: A rapid scoping review by Brittany Barber, Annette Elliott-Rose, Amanda Higgins, Kristy Hancock, Amy Mireault, Katie McDonald, Stacy Burgess, LeeAnn Larocque and Cassidy Christine in Journal of Child Health Care
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the IWK Health Centre (1025462).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.