
Abstract
Adolescents with inflammatory bowel disease (IBD) are at an increased risk of anxiety and depression compared to peers, but availability of mental health services in IBD clinics does not meet patients’ needs, and use of primary care services for mental health screening and care is low. This study provides qualitative data regarding adolescent and caregiver perspectives on addressing mental health in IBD. Interviews were conducted with adolescents with IBD and caregivers of adolescents with IBD. Interview transcripts were coded and analyzed for prominent themes. Thirteen adolescents and fourteen caregivers were interviewed. Three primary themes emerged: mental health stigma makes discussing it more difficult, physician–adolescent trust makes conversations about mental health easier, and asking about mental health directly can help adolescents feel comfortable. Adolescents and caregivers highlighted the importance of considering each patient and their family individually when choosing how to discuss mental health. Fostering trust with adolescents with IBD is vital to addressing mental health. While encouraging standardized screening is important, the most patient-centered approach to mental health involves considering families individually to identify and address mental health challenges. Given the increased risk of anxiety and depression in pediatric patients with IBD, all providers encountering these patients should be equipped to discuss mental health non-judgmentally.
Introduction
About 1 in every 1,300 children 2–17 years old in the United States has inflammatory bowel disease (IBD) (CDC, 2022; Ye et al., 2019), a lifelong condition that cycles through periods of flares and remission and causes symptoms such as diarrhea, abdominal pain, and fatigue (CDC, 2022). Although reported rates of psychiatric disease in patients (ages 11–18) with IBD vary (Walter et al., 2016), up to 25% experience symptoms of anxiety and depression (Szigethy et al., 2004). In those aged 16 to 21, this prevalence can be greater with a combined prevalence of anxiety and depression of 55% (Brooks et al., 2019).
Anxiety and depression are associated with persistent physical symptoms (Van Tilburg et al., 2017), lower academic achievement (Singh et al., 2015), hospital readmission, poor medication adherence (LeLeiko et al., 2013), and chronic opioid use (Barnes et al., 2017). Even in periods of remission, patients with IBD may experience functional gastrointestinal symptoms mediated by mental health challenges (Colombel et al., 2019). Worsening IBD symptoms in adolescents are associated with worsening mental health outcomes, in part due to embarrassment and impacts that symptoms can have on interpersonal relationships (Qualter et al., 2021).
Pediatric patients with IBD at average risk should be screened for depression once annually (Mackner et al., 2020), but rates of mental health screening in subspecialty IBD clinics do not match patients’ need (Mackner et al., 2013). While pediatric patients may be screened during well-child checks, patients with IBD receive preventative services at lower rates than peers without IBD (Farraye et al., 2017), and adolescents’ use of primary care is low overall (Tsai et al., 2014). Pediatric patients with IBD from racial and ethnic minority groups are especially at risk of not using primary care (Moran et al., 2021).
Even in subpopulations of pediatric patients with IBD who have higher rates of primary care use (70 to 80%), there are significant gaps in discussions of mental health-related topics, such as mood, relationships, school, and extracurricular activities. Most patients reported that substance use, sexual health, or body image have not been discussed by their care providers (Michel et al., 2020). Primary care providers also have lower rates of use of mental health screening tools and may choose to prescribe medication over other forms of mental health care due to a perceived lack of access (Dempster et al., 2015).
Multiple clinically feasible and validated screening tools exist to assess symptoms of anxiety and depression in adolescents, including the PHQ-9 and GAD-7, the Child Behavior Checklist, the Children’s Depression Inventory, and the RCADS (Walter et al., 2016). Yet, most patients with IBD with anxiety and depression do not receive needed interventions (Bennebroek Evertsz’ et al., 2012), despite evidence suggesting that Cognitive Behavioral Therapy (Bennett and Pfefferkorn, 2019; Yeh et al., 2017) and other modalities can reduce depressive and functional GI symptoms in patients with IBD (Szigethy et al., 2004). When asked in a structured survey, adolescents with chronic illness perceived mental health screening as being easy, comfortable, and important (Iturralde et al., 2017). Our study will fill a gap in the literature by providing qualitative data regarding patient and caregiver perspectives on discussing mental health in IBD.
Aim
The aim was to explore adolescents’ and caregivers’ experiences of mental and emotional health concerns and perceptions of discussing mental health in the context of inflammatory bowel disease.
Methods
Study design and setting
This was a multiple case study in which we conducted individual telephone interviews with adolescents with IBD and their caregivers in North Carolina. Recruitment and interviews were conducted via telephone due to the global Coronavirus disease 2019 pandemic, which began early in this study. Our team had planned to conduct in-person focus groups with adolescent participants, but these were disallowed due to pandemic-related restrictions.
The pediatric IBD program where patients receive care is an academic medical center, safety-net referral center, and cares for over 300 children and adolescents with IBD. Patients can receive care until transition to adult services at ages 18 to 24. This program is housed within a children’s hospital that provides dietitian and psychological services. During the study period, this IBD program was not using a standard process to screen for symptoms of depression and anxiety and did not have embedded mental health personnel. The children’s hospital provided child psychologists for intermittent consultation, but most mental health services were provided through community clinics. This IBD program was chosen because it was proximal to the researchers, and it maintains an active patient registry of individuals with interest in participating in observational research.
Study population and sampling
Inclusion criteria for adolescents included having Crohn’s disease or ulcerative colitis, being between 14 and 19 years of age, and receiving care from the pediatric IBD program at the participating children’s hospital in 2019. We focused on patients in this age group due to their ability to engage independently with interviewers and the increased incidence of mental health concerns in adolescence. Exclusion criteria for adolescents included not being able to participate in an English-language interview and not agreeing to be audio-taped. Inclusion criteria for caregivers included having a child with Crohn’s disease or ulcerative colitis who was between 14 and 19 years of age and received care from the pediatric IBD program at the participating children’s hospital in 2019. We identified potentially eligible adolescents through a registry maintained by the pediatric IBD program. We used criterion sampling to balance waves of recruitment by any history of mental health conditions documented in an adolescent’s electronic medical record system problem list.
In iterative waves of 10–15 subjects, we recruited participants, conducted interviews, and then performed sampling based on a general balance of participants with documented mental health history (for adolescents) versus not. Caregivers were recruited and interviewed first (September 2019–March 2020), followed by adolescents (June 2020–August 2020). A caregiver’s participation or declination did not require or negate that of corresponding adolescents. Iterative sampling and recruitment continued until we were no longer learning substantial new information from participants, defined as thematic saturation.
Our research team mailed an invitation letter and fact sheet to eligible adolescents’ homes addressed to both adolescents and caregivers, and then a research assistant made up to three follow-up phone calls to discuss study procedures, answer questions, and complete enrollment. Caregivers received US$30 and adolescents received a US$50 gift cards for their participation.
Data collection
We developed complementary interview guides for caregivers and adolescents. Participants were asked questions regarding their experiences of mental health screening, as well as barriers and facilitators to discussing and screening for anxiety and depression in IBD-related and general pediatric care. Participants were additionally asked about their experiences with IBD broadly. Interview guides are included as supplemental documents (Supplements 1 and 2). Our study protocol was reviewed and approved by the Institutional Review Board at our university. More detailed ethical approval information is listed elsewhere.
Participants completed informed consent or assent (as appropriate for age) by phone with a trained research assistant; caregivers of adolescents additionally gave verbal permission. Due to the COVID-19 pandemic and low-risk study procedures, the IRB allowed us to document verbal rather than written consent. The research assistant completed a study intake form via phone that included basic demographic and clinical information and then scheduled an interview. Interviews were conducted by an experienced qualitative researcher and digitally recorded with permission. Audio recordings were reviewed for completeness and accuracy and then transcribed verbatim.
Data analysis
Transcripts were imported into ATLAS.ti PC (Version 9.1.7), a qualitative research software program, to facilitate analysis. Transcripts were coded using a codebook based on the content of interview questions and notes taken during data collection. Our initial codebook was used to pilot adolescent and caregiver transcripts, and then initial interviews were reviewed by two team members to fine-tune codebook definitions.
Interviews were coded using a directed content analysis approach (Hsieh and Shannon, 2005). Discrepancies were reconciled through discussion and consensus. Analysis was descriptive and focused on capturing all relevant information, allowing for both emergent and anticipated themes. Anticipated themes were based on review of the available literature describing screening for and care of anxiety and depressive symptoms in children and youth with IBD (Bennebroek Evertsz’ et al., 2012; Loftus et al., 2011; Mackner et al., 2013; Reigada et al., 2018; Szigethy et al., 2014; Van Tilburg et al., 2017). We grouped and condensed codes into themes that captured the richness of participants’ perspectives. Pseudonyms have been used when participant’s quotations are included. Trustworthiness in findings was enhanced by using participants’ quotes and through an audit trail including all versions of study documents, detailed process notes, a recruitment log, and raw data. Data associated with this study can be accessed by contacting the study team with reasonable request.
Findings
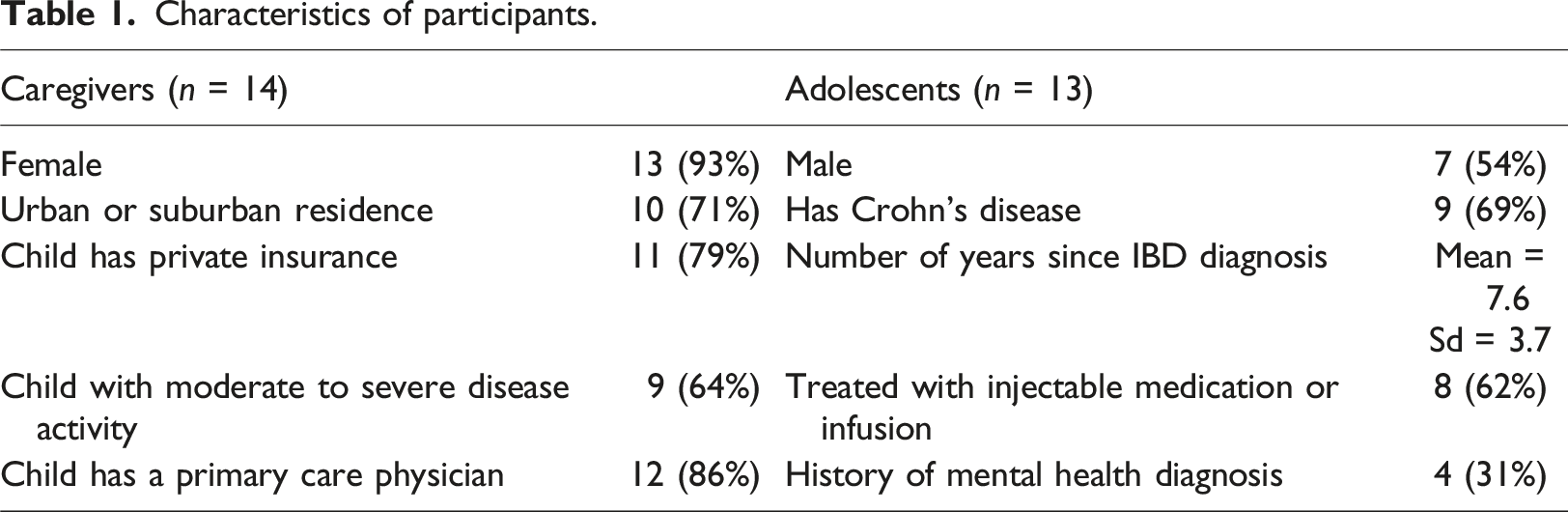
Characteristics of participants.
From interview transcripts, three key themes related to addressing mental health concerns emerged: mental health stigma makes discussing it more difficult, physician–adolescent trust makes conversations about mental health easier, and asking about mental health directly can help adolescents feel more comfortable discussing it. Participants also provided specific recommendations for healthcare providers.
Mental health stigma makes discussing it more difficult
Both caregivers and adolescents with IBD asserted the importance of talking about mental health while discussing stigma as a barrier to open conversations with care physicians. Caregivers described adolescents’ hesitancy to discuss or seek treatment for mental health concerns.
“He’s fifteen and he doesn’t want to talk about that stuff…But he would answer the questions. He would answer them and tell the truth. He would be fairly honest with them as far as how he’s feeling but he wouldn’t agree to continuous mental health care like seeing a therapist or anything” (Emily, Caregiver).
Adolescents perceived that their peers do not want to admit to mental health challenges. One adolescent discussed feeling like they would not seek mental health treatment given the relatively mild nature of their disease.
“Well I feel like there might be a different sort of self-help with this issue because unless you have a severely bad case of Crohn’s, the symptoms are relatively, relatively speaking of course, manageable. So, when you think about it, you think do I really need this, am I really that bad off? I mean there’s people with cancer, diabetes or something horrible that could really need this a lot more than me. Should I really take up this person’s time?” (Adam, Adolescent).
Some adolescents believed that disclosing mental health concerns would only further overwhelm their caregivers. This potential barrier did not emerge from interviews with caregivers.
“Sometimes it’s hard or scary and the people who are close to you, it’s hard to tell them that because then they worry and they worry a lot. I know my mom is a worrier to where some things if I tell her, she wouldn’t be able to focus on her job or function and so to find help, you have to find someone that you know won’t be super, super worried about you or go and tell everybody. You need someone that you can trust but also know that they’ll be okay with what you tell them if that makes sense” (Laura, Adolescent).
Who participates in discussions about mental health was an important aspect of comfort and discomfort for both adolescents and caregivers. Adolescents who believed they should be spoken to alone about mental health felt “conversational freedom” when they were alone with their physician, explaining that they may not want to discuss mental health with their caregivers, or felt they should be responsible for leading conversations about mental health. Caregivers who agreed expressed that adolescents may not feel as comfortable sharing in front of their caregivers.
“I think that the teen should start the conversation because sometimes if adults, like caregivers can sense that something is wrong with their child but the child is not always ready to talk about so personally I would rather bring up the conversation with my GI doctor privately without my caregivers… I definitely wouldn’t feel comfortable talking about my mental health in front of my caregivers now” (Sarah, Adolescent).
Adolescents who expressed that caregivers should be asked separately talked about the possibility that they may be hiding their struggles and noted that caregivers may be aware of changes in their adolescents’ behavior. Caregivers shared that they may be able to provide insights their adolescent is not willing to share with healthcare providers.
“Probably me and my caregivers… Because maybe I told my caregivers something that I’m trying to hide. I don’t know. I don’t know. [but ask at] different times…Because it would be kind of awkward. You’d get different answers and maybe you’d have the folks arguing” (Luke, Adolescent).
“I think both perspectives are important but I don’t think they have to be obtained at the same time. So, I think there’s going to certainly be situations where a kid says ‘everything is fine’ and the caregivers are like ‘what? Everything is not fine. You’re slamming your door and crying yourself to sleep every night. That is not normal’. Then there are going to be other cases where it’s completely the opposite and the kid will say ‘I’m dying inside’ and the family will be like ‘what? I had no idea’” (Marianna, Caregiver).
Other adolescents highlighted the importance of individualizing who is invited to discuss mental health. Some caregivers agreed, noting that some adolescents may be more comfortable with their caregivers present or may have developed more of a trusting and open conversation with their caregivers about mental health.
Physician–adolescent trust makes conversations about mental health easier
Adolescents and caregivers cited trust-related barriers to discussing mental health, including not having a strong relationship with their physicians. This was noted regardless of the specialty of care physician mentioned. Caregivers and adolescents agreed that not speaking directly to adolescents during appointments or only discussing their IBD and not inquiring regarding other aspects of their well-being impeded creating a trusting relationship.
“I don’t think she’d be comfortable talking to the general practitioner at all. I don’t think she’s developed a relationship with her. I don’t think the general practitioner has really tried to develop a relationship with my daughter” (Kasey, Caregiver).
“Well it certainly depends on where you go and what specific doctor you have. Now early on in my treatment, we went to [institution] and the main reason we left it is because the doctor mainly interacted with my caregivers, not me. He didn’t really care as much about what I had to say” (Adam, Adolescent).
Some caregivers also believed that their adolescent’s physician being a different gender than their adolescent impacted how much their adolescent disclosed to their physician. Adolescents did not cite this as a barrier.
The type of physician in question was a consideration for many adolescents who emphasized the importance of trust. Adolescents who would prefer to talk to their gastroenterologists about mental health noted that they see their gastroenterologist more frequently and that adolescents may have a more trusting relationship with them.
“Probably my GI doctor. Well we’ve experienced a lot of stuff together and he is very open about what he thinks and how he feels and so that makes me feel more welcome to share how I feel” (Sarah, Adolescent).
“It’s not like I’m – even though I am seeing a doctor, it’s also like I’m seeing an old friend because of how he interacted with me from such a young age and taught me what was going on” (David, Adolescent).
Some adolescents and caregivers also noted that because much of their care involves specialists, they do not have a designated primary care doctor or see them rarely.
Adolescents who preferred to talk to their primary care physician about mental health noted that their gastroenterologists were focused on IBD, and therefore mental health was not within their realm, and that primary care providers may have more experience with mental health. Other adolescents described a strong relationship over time with their primary care physician.
“I think the main doctor instead of the IBD doctor because I don’t know if the IBD doctor would have as much experience with that or have as much – I definitely get asked about how Crohn’s has impacted my life but I do think that is the job of the primary care” (Luke, Adolescent).
“Okay. I might have to go with [gastroenterologist]. or maybe my psychiatrist, I would say my money might be on [gastroenterologist] and here’s why. I’ve known him the longest. I’ve known him ever since I was a wee baby. I’ve known him for a long, long time, so obviously, I would probably feel more comfortable with him” (Amanda, Adolescent).
Asking about mental health directly can help adolescents feel comfortable discussing it
When recounting experiences discussing mental health, many adolescents recounted providers’ asking about their life during IBD appointments. Some adolescents and caregivers perceived this as the provider inquiring regarding adolescents’ mental well-being, while others disagreed.
“I definitely, like none of my doctors have really brought it up and asked, ‘How are you handling this mentally?’ I don’t recall a time that a doctor has asked me that. The only time is if I brought it up as a concern with the anxiety thing…. Yeah, I mean the pediatrician, whenever you have your normal check-up and you have to fill out that whole sheet on how you’re feeling or whatever. And so you do that, and they look at that. But my GI doctor, it’s never like, --I mean I guess they ask you how are you doing whenever you walk in, but it’s never like, ‘How’s your mental health dealing with Crohn’s?’ It’s never asked like that” (Naomi, Adolescent).
Many adolescents and caregivers noted the importance of physicians asking about mental health directly and non-judgmentally. Some noted that it may be valuable for physicians to ask adolescents verbally because this allows physicians to see adolescents’ emotions and may allow for more in-depth conversations.
“I feel like in person conversation can get a lot more done than a survey…Commonly when I take a multiple choice survey, a lot of times the options don’t quite fit what I want to respond to that question with…Maybe I want to say more than like five words about it” (Adam, Adolescent).
“Just always aim for the verbal because it allows for them to see emotion. It allows for them to see that the provider cares. It allows for validation of like what a lot of patients see is having experienced this and it lets them know they’re not a freak or a weirdo if they are angry or if they are depressed. This is normal. That’s why we’re talking about it and we’ll get a plan to get through it. I don’t know. I think that relationship is very important” (Patricia, Caregiver).
Other participants, especially adolescents, noted the value of providing paper surveys to ask adolescents about their mental health. These participants noted that adolescents may be more honest on paper surveys and that adolescents’ responses on paper surveys can be used as a conduit for more involved conversations.
“I would say writing it down or on a tablet just because of whoever is around. If you ask it verbally, some people may not answer truthfully based on who is around them” (Naomi, Adolescent).
“I had to start filling out a screening every time I went to my primary care provider, my pediatric doctor and so they were like ‘this is totally confidential, the only person who will know is your doctor’. They had us fill out the thing and then they would talk to us based on what it said. So if I checked the oh yeah I’m feeling this or oh no I’m feeling this, like they tell you there’s no need to lie and then they tell you ‘hey, if you don’t want to talk about this, you don’t have to talk about this’. But the doctor based on what the screening says, then they talk to you” (Laura, Adolescent).
Some adolescents and caregivers highlighted that physicians should continue to ask questions about other aspects of an adolescent’s life to understand their emotional well-being.
“Just general asking about her whole well-being, like I said, how are sports, how are you feeling, how’s your eating, how’s applying for colleges, this kind of, --I feel like he’s always been very good at trying to not just talk about her stomach issue, the colitis. Like she wasn’t just colitis, but her as an individual” (Patricia, Caregiver).
Participants who endorsed this strategy discussed that inquiring about an adolescent’s life beyond their disease can help strengthen trust between adolescents and their physicians.
Participants provided strategies that may help build trust between physicians and adolescents to discuss mental health. For example, one adolescent noted that normalizing mental health challenges patients face can be helpful.
“To always say that there are other people who are going through the exact same thing. You’re not alone. Yeah. That’s it… Because some people they feel alone. They feel like they’re the only people going through this. It’s so confusing and what offers clarity is other people, knowing that other people have been through the exact same thing and that yes it’s okay to be scared and all of this stuff but you have, there’s support out there. There are other people out there. You’re not alone” (Laura, Adolescent).
Adolescents and caregivers had suggestions related to confidentiality, building physician–adolescent relationships, and other topics. These suggestions are compiled in Supplement 3.
Discussion
Through gathering qualitative data from interviews with adolescents and caregivers, this study achieved its aim of describing adolescent and caregiver perspectives on addressing mental health concerns with adolescents with IBD. The compilation of these perspectives into themes will facilitate their application to clinical practice. Despite some differences in the focus of caregivers’ and adolescents’ statements, participants noted that stigma can make discussing mental health difficult (Emily, Adam, and Laura). While physician–adolescent trust helps adolescents feel more comfortable, there are barriers to developing strong, trusting relationships (Kasey and Adam). Participants highlighted that asking about mental health directly is important and providing an option to do so on paper can help adolescents feel more comfortable (Naomi, Adam, and Laura). However, participant responses suggest that screening forms are not a replacement for open conversations regarding mental health.
One of this study’s contributions is its systematic approach to eliciting caregivers’ and adolescent’s preferences about approaching screening for mental health concerns in pediatric IBD. Academic literature regarding mental health in pediatric IBD endorses screening for mental health disorders as standard of care for adolescents (Bennett and Pfefferkorn, 2019; Iturralde et al., 2017; Mackner et al., 2020). While some of this work has involved patient and caregiver perspectives (Mackner et al., 2020), our findings suggest that incorporating these perspectives in designing how to identify adolescents at risk for mental health disorders should be prioritized.
Our findings reinforced that stigma could create challenges for open conversations with adolescents about mental health concerns (Luke, Marianna, Laura, and Adam). Adolescents already face a significant degree of mental health-related stigma (Kaushik et al., 2016), which may compound that patients with IBD already feel secondary to their disease (Taft et al., 2017). Increased illness stigma, especially in adolescents with IBD, can compound preexisting mental health-related stigma and worsen or increase the risk of depressive symptoms (Roberts et al., 2019, 2020, 2021). Research regarding interventions to decrease mental health stigma in adolescents is limited and varied, with little consensus on which strategies are most effective (Kaushik et al., 2016).
Adolescents may feel most comfortable discussing mental health with providers with whom they have built trusting relationships (David and Sarah). This could be challenging when considering that some late adolescents may transition to adult care, moving from a provider with which they may have developed a trusting relationship, to an adult provider (Plevinsky et al., 2015). Low primary care use (Tsai et al., 2014) may exacerbate this challenge, as late adolescents may not have a trusted medical professional with whom to discuss sensitive mental health concerns. Pediatric IBD physicians who are transitioning patients to adult care may want to ensure that the patient has a primary care physician and is not transitioning both physicians concurrently.
Caregivers and adolescents may benefit from individualized approaches to screening for and discussing mental health concerns. For example, while adolescents noted that screening forms (such as the PHQ-9) may allow some to feel more comfortable (Naomi and Laura), they also highlighted the importance of face-to-face conversations, regardless of whether an adolescent is currently experiencing symptoms of anxiety and depression (Adam and Patricia). While adolescents with chronic illness may perceive mental health screening through surveys as easy and comfortable (Iturralde et al., 2017), doing so in the absence of conversations about mental health may miss fully capturing an adolescent’s emotional state.
Our work highlights the importance of creating and fostering a trusting relationship with adolescents. Doing so can help them feel more comfortable both discussing and disclosing mental health concerns. Some adolescents may not feel confident sharing how they are feeling even if presented with a screening form. Given that many adolescents with IBD may not have a regular primary care physician—a finding consistent with research both in IBD (Moran et al., 2021) as well as in other pediatric chronic conditions (deJong et al., 2017)—ensuring that gastroenterologists feel comfortable discussing mental health is vital.
Our findings have several implications for screening and discussing mental health in pediatric IBD practices. Despite some common themes in conversations with participants, mental health should be treated as a highly individual part of IBD care. Although pediatric gastroenterologists and primary care physicians may work within a framework that assigns the responsibility of discussing mental health to a particular healthcare physician, participants centered trust as the deciding factor for who should be responsible for mental healthcare. Given the severity and prevalence of mental health disorders in pediatric IBD (Butwicka et al., 2019), all care physicians encountering adolescents with IBD should be well-equipped to identify mental health concerns and offer treatment options. Adolescents may be more willing to discuss mental health with different physicians and asking about mental health regularly may help normalize discussions.
Study limitations
Our participants receive IBD care at a singular institution and geographical area (Study Design and Setting), so their perspectives may not represent those of individuals cared for at other care centers. Practices for discussing and screening for mental health concerns likely vary between different IBD care centers, as well as between primary care offices in different regions. Participants in our study may also be more comfortable discussing mental health issues than an average adolescent with IBD or caregiver, and therefore our findings may be skewed toward those for whom discussing mental health with their IBD physicians feels less daunting. We did not ask how previous psychosocial treatment may have impacted perspectives. We did not ask adolescents to rate their disease severity, and it is possible that patients with more severe disease did not choose to participate. Providing a gift card to adolescents as an incentive may have mitigated this effect somewhat by motivating adolescents who may be more hesitant to discuss mental health to participate.
Implications for practice
Creating partnerships with adolescents and their families is vital to addressing mental health in adolescents with IBD. Although screening for mental health disorders is important, our findings suggest that the most patient-centered approach involves learning from each adolescent and their family regarding variability in approaching mental health.
Gastroenterologists should be trained to discuss mental health, especially given that pediatric patients with IBD may rarely see a primary care physician, if at all (Moran et al., 2021). Given the pervasiveness of mental health concerns in adolescents with IBD, pediatric gastroenterologists should be responsible for ensuring patients’ mental health needs are addressed. Clinics should also consider creating integrated mental health services, a model that has been proposed in IBD (Wong et al., 2018) and other pediatric chronic diseases (Quittner et al., 2020). Embedding a child psychiatrist who is familiar with IBD into pediatric IBD clinics can increase access and reliability of mental health care (Engelmann et al., 2015).
IBD clinics incorporating a yearly health maintenance visit into their workflow should not consider this an adequate alternative to the adolescent’s primary gastroenterologist discussing mental health. Concurrently, this work should engender confidence in adolescents with IBD to communicate their preferences regarding discussing mental health with their physicians.
Future research directions built off this work could include conducting qualitative studies with more geographic variability to assess whether perspectives vary by region. Likewise, a study could be developed that implements standard conversation openers regarding mental health and assesses adolescent comfort immediately after clinic visits. Although further study of mental health in IBD is warranted, addressing mental health with patients should be personalized to their needs.
Conclusion
Three main themes emerge from analyzing qualitative data regarding adolescents’ and caregivers’ perceptions surrounding screening and care for mental health disorders in pediatric patients with IBD. Participants noted that stigma can make discussing mental health more difficult, physician–adolescent trust makes conversations about mental health easier, and asking about mental health directly can help adolescents feel more comfortable discussing it. Our findings support an individualized approach to mental health care for adolescents with IBD that prioritizes multiple modalities for evaluating mental health and the importance of every provider who cares for these patients to discuss their emotional well-being.
Supplemental Material
Supplemental Material - Adolescent and caregiver perceptions of addressing mental health in inflammatory bowel disease
Supplemental Material for Adolescent and caregiver perceptions of addressing mental health in inflammatory bowel disease by Catalina Berenblum Tobi, Maihan Vu, Maria E Diaz-Gonzalez de Ferris, Sherritta Semerzier, Michael D Kappelman and Neal deJong in Journal of Child Health Care
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the grant number KL2-TR00249001 from the National Institutes of Health National Center for Advancing Translational Sciences (NCATS).
Ethical statement
Participant consent statement
All participants in this study provided informed consent.
Data Availability Statement
Data is available from the authors upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.