
Abstract
Coronavirus disease 2019 (COVID-19) created unprecedented challenges for everyone, but especially families of children with medical complexity (MC) who rely on a comprehensive range of health and social services in their daily lives. Yet despite this, there are limited studies exploring caregiver perspectives regarding access to health and social services during the pandemic. To address this gap, we aimed to explore how health and social services can better meet the needs of children with MC and their families. Sixteen parents residing with their children with MC (from birth to 18 years) in British Columbia, Canada participated in semi-structured interviews between July 2021 and April 2022. Findings revealed two different areas to improve services for families of children with MC, those relating to technology and family-centered care. Parents prioritized expanding the use of digital communication tools to support service navigation and scheduling. Virtual platforms were viewed as being valuable for building connections with other families and their community. In terms of family-centered care, parents emphasized the importance of policies recognizing the physical, emotional, and financial needs of the family. Findings have important implications for improving services to enhance the well-being and quality of life of children with MC and their families.
Introduction
Medical complexity (MC) is characterized by chronic conditions, functional limitations, technology dependence, high healthcare utilization, and need for a comprehensive range of medical, psychosocial, educational, and support services (Cohn et al., 2020). Although children with MC comprise of only a small proportion of pediatric patients in Canada, they are a resource intensive group within the healthcare system (Breneol et al., 2017; Cohen et al., 2012). For example, one study found that children with MC account for approximately one third of child healthcare spending and a quarter of hospitalizations in Ontario (Cohen et al., 2012). Costs are attributed to factors such as lengthy hospitalizations, frequent re-admissions, and frequent use of emergency departments (Cohen et al., 2012; Glassgow et al., 2017).
Children with MC also have intensive support needs outside of hospital care (Pordes et al., 2018). Indeed, there is a breadth of research demonstrating the crucial role that caregivers and family members play in providing comprehensive, life-sustaining, and highly skilled support for children with MC (Mooney-Doyle and Lindley, 2020). Thus, it is not surprising that parents of children with MC often report high levels of stress and caregiver burnout (Allshouse et al., 2018; Peckham et al., 2014). It is also not uncommon for parents to report financial burden due to insufficient insurance coverage, employment and income loss, and out-of-pocket costs (Von Schulz et al., 2022). Research has also shown that parents of children with MC have high levels of unmet needs (Kuo et al., 2014; Kuo et al., 2016a; Mooney-Doyle and Lindley, 2020). Parents have reported low satisfaction in areas such as access to subspecialty, dental, and mental healthcare (Kuo et al., 2014; Kuo et al., 2016b; Mooney-Doyle and Lindley, 2020). On the other hand, studies have shown that high levels of care coordination for children with MC is linked to improved access to medical care and lower levels of caregiver burnout (Matsuzawa et al., 2020).
While onset of the Coronavirus disease 2019 (COVID-19) pandemic contributed to unprecedented disruptions for all families, presence of MC in the family posed unique challenges for this population (Diskin et al., 2022; Driansky et al., 2022). Resulting public health measures taken to reduce spreading infection, including lockdowns and cancellation of services, has created elevated stress and anxiety on an already overwhelmed group of caregivers (Von Schulz et al., 2022). In addition to being cut-off from previous formal and informal support networks, social isolation over a prolonged period has further exacerbated mental health concerns in this population (Bayer et al., 2021).
Literature examining caregiver experiences accessing and navigating healthcare services for their children with MC during COVID-19 have been sparse (Diskin et al., 2022; Markham et al., 2022). A handful of cases have primarily relied on quantitative survey methods to examine hospital visits, infection rates, and service utilization during this period. For example, in one study by Brisca et al. (2021), researchers conducted a chart review of hospital stays for children with MC in Italy and found a drop in Emergency Department visits but an increase in overall admission rates and lengths of stay. Another study by Baumbusch et al. (2022) surveyed 188 caregivers of children with MC in British Columbia (BC), Canada found that access to allied health therapies and medical specialists significantly declined during initial months of the pandemic. However, studies to date have not explored caregiver perspectives regarding priorities for improving healthcare services to better meet needs of children with MC and their families. This is a significant gap in research and has important implications for future disaster and health-related emergency planning.
Aim
To explore parents’ perspectives on improving healthcare services and supports to better meet the needs of children with MC and their families.
Materials and methods
Study design
Methodology guiding this study was interpretive description (ID). This is a pragmatic methodology that aims to provide guidance and useful direction for policy and practice (Thorne, 2016). In small scale qualitative investigation of clinical issues, ID is particularly useful as it captures patterns and themes in subjective responses that helps in addressing complex experiential questions while ensuring practical outcomes that inform clinical understanding (Thorne et al., 2004). Studies using ID often draw on multiple data collection strategies to bring forward a meaningful account of experiential knowledge shared by its participants and to offer useful directives for policy and practice (Thompson Burdine et al., 2021). This approach was particularly suitable as it allowed for exploration of participants’ views on ways to address their families’ needs during COVID-19 (Thorne, 2016). Research ethics approval was obtained from University of British Columbia’s Behavioural Research Ethics Board (certificate H20-02158).
Setting
The setting of this study was in British Columbia (BC), Canada. In BC, a recent report found that in 2015–2016 there were approximately 802 children with MC per 100,000 children (Canadian Institute for Health Information, 2020). On January 28, 2020, this province was second in Canada to identify a case of COVID-19 and less than 2 months later a global pandemic was declared by the World Health Organization (CBC, 2020; World Health Organization, 2020). Healthcare services underwent significant changes including shifts to virtual appointments, cancellation of elective surgeries, and restrictions on family members accompanying patients into hospitals (Canadian Institute for Health Information, 2020; Provincial Government's Guidance for Family Presence and Visitor Policies, 2021). In BC, there is only one tertiary pediatric hospital, which is located in Vancouver. Most outpatient medical specialties are also based out of this hospital. Therefore, families that live at a distance from this location often need to travel there to access highly specialized services their child requires.
Participants and recruitment
Purposive sampling was used to select participants from a large cross-sectional survey Baumbusch et al. (2022). Survey recruitment involved posting on public social media, posting in a private Facebook group for families of children with MC, and a traditional media report (i.e. newspaper article). Surveys were completed on the host institution’s survey platform. Respondents indicated whether they were interested in participating in a semi-structured interview. Using sociodemographic responses on the survey, we identified respondent characteristics that previous authors have suggested are limited or lacking in samples with this population (e.g. men, residing in rural/remote areas, and non-White). Priority was given to respondents from those groups to participate in interviews.
Interview inclusion criteria were as follows: (i) parent/caregiver of at least one child (from birth to 18 years) with MC, (ii) co-residence in the same household, (iii) living in BC, Canada, and (iv) fluent in English. It is important to note that although the age of the children with MC needed to be birth to 18 years (inclusive) at recruitment, by the time the interviews were conducted one participant’s child had turned 19. Parents were offered their childcare expenses to be covered to facilitate their active participation in the interview process. To ensure confidentiality of all participants, which is especially critical when dealing with small sample sizes, pseudonyms were assigned when reporting findings.
Data collection
Interviews with participants took place virtually via Zoom between July 2021 and April 2022. All participants provided their consent to have their interviews videorecorded. Researchers and community partners collaborated in developing and adapting an interview guide. Topics covered included caregiver experiences accessing services and supports (e.g., medical services and allied health therapies) for their child during COVID-19 and access to government financial supports for families (Supplementary Material 1). To describe the study cohort, sociodemographic data (e.g., family income, and race) were also collected.
Data analysis
All interviews were transcribed verbatim, with all identifying information removed and uploaded to NVivo 12 (QSR International), a data analysis software that enables researchers to manage, organize, code, and analyze qualitative data. Three team members took part in developing the codebook using an iterative process. One team member first reviewed a subset of three transcripts and identified initial codes. Two different authors reviewed these transcripts and confirmed initial coding. During this phase, codes were added and revised based on consensus among team members. Once it was determined that no new codes were arising and that codes were being applied accurately and consistently among team members, the codebook was finalized. As analysis progressed, codes were further collated to capture emerging themes and patterns that provided a meaningful account of parents’ experiences and perspectives. For instance, while our codebook, to cover breadth of data, included codes such as “Access to educational services,” “Changes in provision of healthcare,” “Changes in other healthcare supports,” and “Gaps in services,” among others, an in-depth analysis of these codes revealed recurring themes around importance of technology, virtual care, and family-centered care in families’ lives. We focus on these recurring themes, in this article, to generate an interpretive description of how healthcare systems can best support needs of this population. Throughout analysis, criteria developed by Lincoln and Guba (1985) were used to ensure trustworthiness or quality and degree of confidence and trust in data and interpretation of findings. See Supplementary Material 2 which summarizes techniques and strategies used to address each criterion (e.g., credibility, dependability, and transferability).
Findings
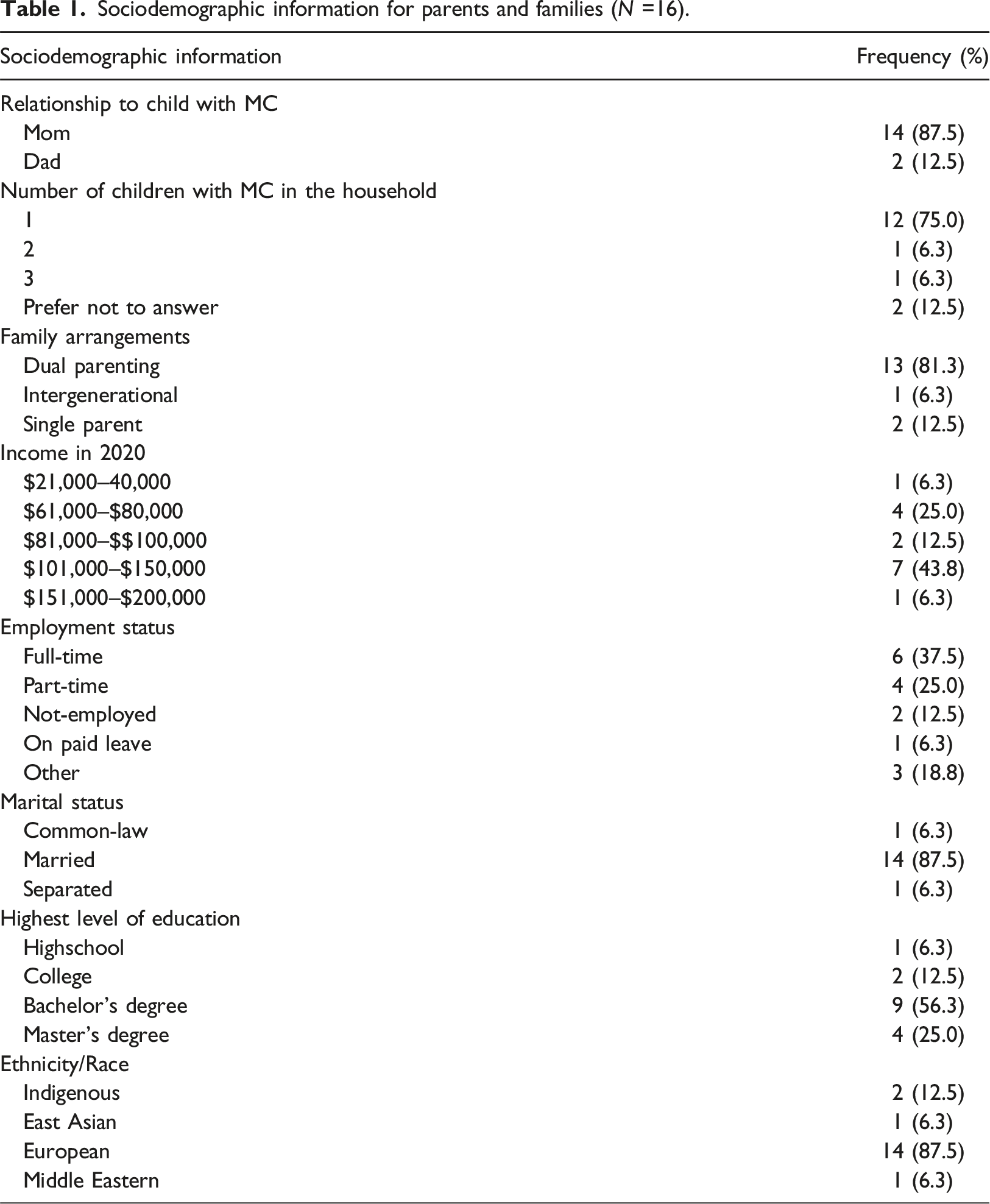
Sociodemographic information for parents and families (N =16).
Sociodemographic information for children with medical complexity (N =16).
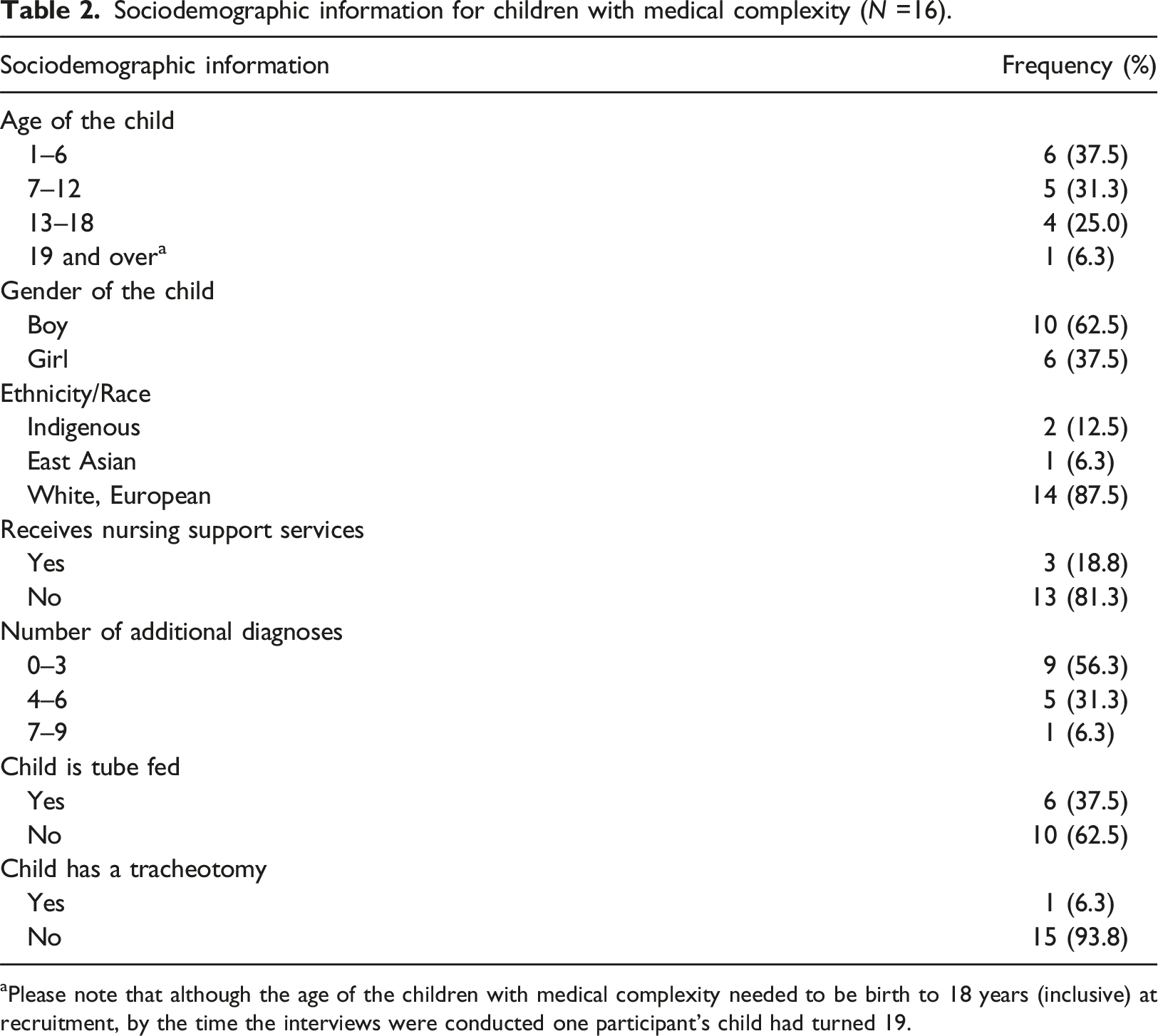
aPlease note that although the age of the children with medical complexity needed to be birth to 18 years (inclusive) at recruitment, by the time the interviews were conducted one participant’s child had turned 19.
Two different areas to better meet needs of children with MC and their families were identified in interviews, those relating to technology and family-centered care (FCC). Parents prioritized expanding technology use and digital communication tools to support service navigation, scheduling, and building connections and relationships with their communities. Parents also discussed ways to improve FCC through policy, service delivery, and interactions with professionals. Main findings from interviews are summarized in Supplementary Material 3.
Technology
Expanding the use of digital communication tools in healthcare
Parents expressed various advantages and disadvantages of transitioning to virtual appointments and therapies for their child during COVID-19. Many families living in rural and remote areas articulated their preference for virtual over in-person appointments. For these parents, virtual appointments were more convenient and saved them travel time and money for gas:
The opportunity to do things by Zoom instead of in-person [was preferred] because there’s a lot of things we don’t need to do in-person. We don’t need to travel two hours on a ferry and take an entire day off work when it could take thirty minutes which is what has happened in this [pandemic] and its great, yeah. You don’t have to commute to the hospital. That’s one of my not favorite nightmares. (Angela, 38-year old mother)
In-person appointments tended to be preferred when it was necessary to have a physical exam that wasn’t possible with a virtual platform:
I mean for certain things we brought him in-person where that care was needed like looking at some weird tissue around his medical device. But as far as the rest of his care, which doesn’t really require a physical examination, it’s totally fine to do that virtually. Most of those appointments are punctual than the in-person ones, and then even if you wait, you’re waiting in your home rather than in a hospital which is a lot better. (Noah, 36-year old father)
However, some parents expressed less favorable views towards virtual care, particularly when it came to allied health therapies for their child. These parents pointed out that certain types of virtual therapies were unable to engage their young child or were incompatible with their child’s accessibility needs. For example, one parent shared:
We did some of it online for a while but speech and language especially was very difficult because she’s deaf/blind and so she’s absolutely not interested in screens of any kind. So I couldn’t get her to engage at all with the SLP and he wasn’t very comfortable with in-person visits and so as a result we just had to stop therapy. I think when I look back over the years that was the most significant therapy for her. She was completely orally averted for most of her life, fully dependent on a G tube but with work the SLP was able to get her to eat orally a little bit and to enjoy taste and senses. (Stephanie, 60-year old mother)
Regardless of preference, there appeared to be some consensus across different families that they should be asked and given the option to choose between virtual or in-person therapies and appointments:
I love the idea of virtual appointments if people are going to stick with that but to make it optional, to be asking families what you need because sometimes I really just need to see humans [laughs]. (Kristen, 42-year old mother)
Parents frequently discussed challenges scheduling appointments and coordinating multiple therapists and services for their child which often led to missed or postponed appointments. These parents expressed needing greater follow-up and assistance in this area:
You find that they would schedule the appointment and then not call you so you’re waiting around for them and then it just doesn’t happen. And so we went eighteen months without any dietary support whatsoever for a G-tube fed child and we got cut off our formula supply because of it so we couldn’t order. We should be able to have regular follow-ups to like track how we’re doing and increase his oral intake and like meet goals but we’re not. We’re seeing them once a year if that sometimes almost two years in-between. (Kristen)
Miscommunication and errors ordering supplies or running out of supplies created elevated stress and worry in parents often leaving them feeling overwhelmed:
It’s tough and it’s a lot of scheduling all the appointments, scheduling all the meds to be refilled like all the supplies and when they don’t get it right you’re on the phone for hours. During the pandemic I didn’t think we would get supplies. What are we going to do if we can’t get diapers? What are we going to do if we can’t get his supplies for his medical device? It was all that stress too right? It’s like regular parenting times a thousand. (Isla, 36-year old mother)
Building connections with other families
Similar to pre-pandemic, parents appreciated and valued peer support (Baumbusch et al., 2018). During COVID-19, previously held in-person supports shifted to virtual platforms. One parent spoke about various benefits of online meet-ups, starting with having to adjust to using virtual platforms:
I think we found these Zoom calls to be really helpful. It took a long time because I’m old and I don’t know how to work these computers very well and it was technology so it created anxiety. But once I got used to it I’m very happy with the ability to connect by Zoom. (Stephanie)
This parent went on to speak about how virtual platforms facilitate connecting families:
The family hangouts that were created got very popular and people started to connect and some of these calls were twenty people strong. I worried that it was going to be people beefing about the restrictions but it really didn’t turn out that way, it was about what they needed and how they could cope with what they were feeling. It would never have occurred to me before the pandemic that I would be talking to anybody on a computer like this, that I would engage with people, with peers or friends. (Stephanie)
They also reflected on how virtual meet-ups eliminated labor involved in going to in-person events:
Going anywhere is a chore and a half, you have to empty catheters, fill feed pumps, load wheelchairs into the bus, stabilize everybody, and anchor them all down. There’s all this work that has to be done to get to a place for a half hour and then you have to do it all in reverse to get them back home again. I hope that this will continue these ways of connecting and that they will make life easier for some of us to stay connected with each other. (Stephanie)
Family-centered care
Considering physical, emotional, and financial needs of families
The need for healthcare professionals and policies to recognize emotional, financial, and physical impacts on caregivers of children with MC was emphasized. Hospital policies of having only one parent accompany a child was particularly challenging for parents of older children who needed not only the emotional but physical support of their partner to help carry and transport their child. For example, a 42-year old mother of a teenage girl who was admitted to the emergency described her frustration with the one-parent policy:
Under no circumstances were they letting two parents in. [My child] is over seventy pounds, she doesn’t really wake up that well from anesthetics. And they would not let [my husband] come in at all so I had to do that by myself. My child was actually unfortunately hospitalized for twenty-one days in March with a terrible condition. So to be alone with her, like afraid that she was going to die and not have my husband there was terrible. My child’s care was so appalling that I had to be her nurse, I couldn’t be her mother so I never could sleep. I was awake for like twenty-one days and nights straight. I needed help with her and I was losing my mind and there were no exceptions. (Elvira)
For some parents, addressing physical and emotional needs of families could be met through better access to respite. Parents perceived respite to be valuable yet highly inaccessible both before and during the pandemic due to various reasons, including a lack of respite providers, funding for this service, and concerns about exposure to viral infection. One parent shared their struggles obtaining respite:
In the best of times, like last year before the pandemic hit, I was frustrated trying to get respite, like I was fighting with staff because we’d been on the respite list like since forever and we just weren’t getting it. I was just like ‘I need help’ and that was even before when I had more help than I do now. I don’t know it all sucked before and now it just sucks even more. (Isla)
It was not uncommon for families who expressed needing respite to report feeling overwhelmed, scared, and burnt out:
I’m not sure that everybody understands the longevity of it. I think a lot of people think everything is going to be fine and I know that’s not the case. There’s a massive shortage of nurses, there’s a backlog of surgeries and procedures that haven’t been done and people who aren’t getting what they need. It’s very scary to think of. I see the world as being a very different place than when the pandemic started. And of course, it came as a shock to me. I wasn’t prepared, I didn’t anticipate that this was going to happen. (Stephanie)
Pre-pandemic, families experienced additional financial strain related to caregiving. Out-of-pocket costs spent on therapies, services, equipment, and supplies that were not covered by their insurance or government funding put a significant strain on families:
I have to fight for every one of those medical supplies. Like he’s five, he needs diapers, he doesn’t walk so he needs a medical device, and he also needs alternate positioning feeding. To explain to people like that all comes from the same budget like where do I come up with $10,000 of my own money? I don’t think people realize how expensive it is to have a kid that doesn’t fall into like the “typical” category. Even having a kid with mobility issues is even more expensive because we have to have the special enclosed bed which isn’t covered, the special chair to fit in, all the therapy appointments he’s supposed to go to. And that’s just to keep him healthy just so that he doesn’t need super expensive medical surgery. People don’t understand what that looks like. (Isla)
Considering financial burden experienced by almost all participants, many parents expressed their enthusiasm when hospital parking fees were canceled during COVID-19 and parking was free. A number of parents appreciated this gesture which helped alleviate a small but accumulating cost especially with multiple hospital visits:
One thing I think that they did do well is making hospital parking free, I think that was huge. I wish they could keep that forever because even when we did go to some of his specialist appointments it was like one less thing to worry about. (Maya, mother, age not provided)
Flexibility in government funding
During the pandemic, changes were made to government-administered funding for respite which included greater flexibility in how families could use the money. This allowed some families to use respite funding to purchase meals for their families, iPads to support their child’s learning, or exercise equipment for their child. Many parents were very satisfied with this change:
[I used the respite funding] for housekeeping or to get take-out or different things that could alleviate some of the burden. I put it into the housekeeping, to the ordering food to make our lives easier, I also put it towards like sports stuff for my child. I’m super thankful for it. (Connie, 47-year old mother)
Participants were also relieved that paperwork involved in accounting for respite funding was eliminated, as this was additional unpaid labor for them:
What was nice during the pandemic is you could use that funding for a broad range of things not just respite and you didn’t have to fill out 5,000 forms to justify it during the pandemic. (Melissa, 50-year old mother)
Strengthening professional-family relationships
Parents also appreciated when service providers made efforts to check-in with families to see how they were doing and if certain accommodations could be made so that their child could safely continue with therapy:
We were able to continue with speech therapy because we have a therapist who went the extra mile to install a plexiglass screen and she wore a mask with a clear face visor and then our child didn’t have to because he was on the other side of the plexiglass. I appreciate their attempts to keep it going. (Patrick, 46-year old father)
During COVID-19, greater attempts were made by medical specialists to set up mobile sites and provide outreach services to families in remote and rural areas. One parent shared:
Before the pandemic we would have to go to the city to see our medical specialist. That’s one of the big challenges is coming to the city all the time for seeing the doctors and stuff. Since the pandemic, there’s been a respiratory outreach come here and they’re coming again next month. This is the first time ever that they’ve come too. (Lin, 32-year old mother)
Discussion
Drawing on qualitative data obtained through semi-structured interviews, we have revealed ways that healthcare services can better meet needs of children with MC and their families based on learnings from COVID-19. Consistent with previous studies (Notario et al., 2019; Rosenbaum et al., 2021; Ross et al., 2020), our findings confirmed advantages of and preference for virtual care for families of children with MC. However, our research has expanded these findings by identifying specific contexts where virtual care is preferred as well as considerations for delivering virtual care to this population. Although expansion of virtual care has increased rapidly, especially during the pandemic (Whaley et al., 2020; Van Cleave et al., 2022), moving forward it is crucial for parents and caregivers to be given options to choose what their preference is (virtual vs in-person) for therapies and appointments. Indeed, families have diverse needs in terms of their distance to healthcare services, access to technology and high bandwidth internet, childcare, child’s accessibility requirements, and mobility.
While previous research has broadly identified care coordination as a significant barrier to accessing services (Kuo et al., 2016a; Matsuzawa et al., 2020; Mooney-Doyle and Lindley, 2020), this study found that scheduling appointments and filling out forms is highly stressful and demanding for parents. These specific aspects of care coordination are often overlooked yet are important and time-consuming activities which take away from childcare, work, and self-care opportunities. Expanding technology use to assist caregivers with scheduling and navigating services may help reduce caregiver burden. Alternatively, being sent reminders about future appointments and medication or supply refills may help reduce stress, avoid missed appointments, and consequently future hospitalizations (Glassgow et al., 2017).
Another significant finding in our study was that parents often valued virtual platforms for building connections with their community and other families of children with MC. Similar findings were reported by Baumbusch et al. (2018) which observed that parents of children with rare diseases found peer support to be an effective and valuable resource which virtual platforms helped to facilitate. Additionally, online peer support was also shown to create opportunities for families that may have been more isolated due to geography or other structural vulnerabilities. Similar to previous studies conducted during COVID-19, connecting virtually during this time helped lessen feelings of isolation and improve their mental health and well-being (Lightfoot and Moone, 2021; Milberger et al., 2021).
Our findings also shed light on ways to improve FCC for children with MC and their families. Similar to previous research, parents expressed needing healthcare professionals and formal policies to recognize physical, emotional, and financial impacts of raising a child with MC (Mooney-Doyle and Lindley, 2020; Von Schulz et al., 2022). Extending these findings, interviews revealed specific strategies and solutions for addressing these. For parents this meant having exceptions to one-parent policies implemented in hospitals during the pandemic. This policy is particularly detrimental to families of children with MC for a number of reasons. For example, parents in this study reported not being able to sleep during hospitalizations where having their partner present would have enabled them to do so. Additionally, recognizing the significant financial impact of raising a child with MC (Kuo et al., 2011; Rose-Jacobs et al., 2016), hospitals can help alleviate some of this strain and improve families’ experience by providing free parking to parents of children with MC who spend a significant amount of time there. On a larger scale, policy changes that address disparities in financial and employment outcomes for caregivers of children with MC are urgently needed. Indeed, current findings add to existing literature demonstrating the importance caregiver benefits and government financial supports have on supporting caregivers in their role (Lum et al., 2014).
Consistent with previous research (Cleveland et al., 2022; Mooney-Doyle and Lindley, 2020), parents interviewed frequently required needing respite. However, parents varied in their views regarding what respite meant to their families. For some, respite meant having a person outside their home watch their child with MC for a few hours, whereas for others, respite meant being able to purchase meals so parents could use meal preparation time to spend with their children and families. Parents also preferred service models that allow for flexibility in funding. Policies which support diverse and constantly evolving needs of children with MC and their families are critical. Ultimately, parents are experts in their child’s care and are able to make decisions regarding where to allocate funding to meet their child’s needs. Current service models with strict eligibility criteria for therapies, excessive paperwork, poor care coordination and follow-up are all barriers to FCC.
Study limitations
There were a number of limitations that warrant caution when interpreting findings of our study. Mostly all participants were white woman and all spoke English fluently. Although this is common in this area of research, greater efforts are needed to recruit men, gender diverse, and minority language speaking participants in future studies. Another limitation relates to the cross-sectional nature of this research. Future studies using longitudinal designs are needed to better understand service and support needs of families of children with MC which fluctuate and change over time.
Implications for practice
Barriers that families experience often relate to challenges navigating services and scheduling appointments. To address this, greater investments and resources are needed to develop user-friendly platforms to support service navigation. Policies are also needed which promote equitable access to virtual care services and ensure a comprehensive coverage of a broad range of services. The findings also highlight FCC and policies which address physical, emotional, and financial needs of families. Examples may include providing respite, child care, and financial supports to families based on their unique circumstances and needs.
Conclusion
Two different areas to better meet needs of children with MC and their families were identified, those relating to technology and FCC. Parents prioritized expanding digital communication tools to support service navigation and scheduling. Virtual platforms were viewed as being valuable for building connections with their community as well as with other families of children with MC, and for delivering therapies and appointments especially for families living in remote and rural areas. In terms of FCC, parents prioritized policies recognizing the physical, emotional, and financial needs of families, having flexibility in funding, and strengthening family-professional relationships. Findings have important implications for improving service delivery and quality to enhance well-being and quality of life of children with MC and their families.
Supplemental Material
Supplemental Material - “A very different place from when the pandemic started”: Lessons learned for improving systems of care for families of children with medical complexity
Supplemental Material for “A very different place from when the pandemic started”: Lessons learned for improving systems of care for families of children with medical complexity by Vanessa C Fong, Jennifer Baumbusch, and Koushambhi Khan in Journal of Child Health Care
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Canadian Institutes of Health Research.
Supplemental Material
Supplemental material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.