
Abstract
The study objective was to explore the experiences of parents of children (6–17 years) with complex mental healthcare needs in accessing healthcare services in Alberta, Canada. Parents were interviewed using a semi-structured guide with open-ended and probing questions. Interviews were audio recorded and transcribed verbatim. Thematic analysis revealed three main themes: (1) Fragmented healthcare services profoundly impacted participants’ experience of mental health care due to (a) a lack of a collaborative approach across disciplines in the healthcare system; (b) unavailability of information related to mental health care and (c) a lack of patient-centred care. (2) Navigating the complex healthcare system was difficult due to fragmented services and was hindered by gaps in accessing and receiving care, lack of continuity of care and lack of resources. (3) Distressed parents discussed the emotional challenges, financial burdens, self-advocacy and stigma they experienced in navigating the system. Parents offered insights into potential solutions to these gaps. Parents recommended the creation of a one-stop shop service with a team approach led by a navigator to facilitate and support navigations across healthcare services that work collaboratively across disciplines among healthcare services and across sectors inclusive of social services, education, policing and community programmes.
Keywords
Introduction
Families of children with complex mental health care needs face significant challenges in the search for timely and appropriate services (Sayal, 2006). Issues include contacting multiple agencies, looking for multiple types of treatments and help for different problems across agencies, resulting in increased burden on the mental healthcare system and the families (Reid et al., 2011; Schraeder and Reid, 2015). Moreover, the process of seeking help by families has been described as ‘circuitous and long’ and the pathway for obtaining a diagnosis for their children is often ‘confusing, distressing and uncertain’ (Clarke, 2012). The help-seeking process can leave families without appropriate access to services and treatment to support their child’s mental health (Clarke, 2012).
About 20% of Canadian youth experience mental disorders (Comeau et al., 2019) with the prevalence steadily increasing (Leung et al., 2019). Children and youth mental healthcare services are provided in the community via clinics, private practice, hospitals and schools (Canadian Institute for Health Information, 2015). Well-recognized gaps in the care delivery system include service availability and integration, timely access and transition of care from youth to adulthood (Canadian Institute for Health Information, 2015). In fact, identifying challenges in service provision to address unmet needs have been identified as a priority for researchers, policymakers and administrators (Duncan et al., 2020).
Experience of families with children living with complex mental health problems remains largely unexplored (Carman and Workman, 2017). Anecdotal discussions with parents reveal a lack of treatment programmes, a lack of information about existing programmes, poor communication between healthcare departments, lack of information about medication safety and efficacy and a lack of adequate treatment monitoring (Clarke, 2012). While we understand the sociodemographic characteristics of those who struggle to find services, such as severity of mental disorder, parental perceptions, child age and gender, and family and social background (Sayal, 2006), and the reliance of current practices on short-term reactive interventions (Reid et al., 2011), less is known about the struggle of families dealing with limited options for treatment and a lack of support for accessing services. Only recently have issues of stigma experienced by families been contemplated; that is, stigma is important as a driver of trauma and emotional burden for the families (Hinshaw, 2005).
Currently, little is known about challenges that families face in their search for resources and navigating the healthcare system to find options for their children. In this patient-oriented research, voices of families are captured to build research evidence to improve access to healthcare services and policies.
Aim
The aim of this study was to explore experiences of parents of children with complex mental healthcare needs in their journey across healthcare services in Alberta, Canada. Specific objectives include identifying gaps in care and proposing recommendations to improve care.
Methods
This patient-oriented qualitative study conducted one-on-one semi-structured interviews with parents of children living with complex mental healthcare needs. According to the Canadian Institutes for Health Research-Strategic for Patient-Oriented Research definition, the term patient refers to individuals with personal experiences of a health issue and/or informal caregivers, including family and friends (Canadian Institutes of Health Research, 2019). An advisory group of three parents from rural and urban areas worked with the research team to advise and support the study to completion. This advisory group co-designed the interview guide with the research team and supported the members’ checking activity as well as the final writing of the manuscript. The interviews were conducted face to face, by video, or by phone, to accommodate the preference of the participants. We conducted thematic analysis using an inductive approach.
Inclusion criteria
Parents met inclusion criteria if they had a child aged 17 or younger at the time of accessing healthcare services in Alberta, diagnosed with depression, mania (hypomania), anxiety or bipolar disorder and were fluent with written and spoken English. Potential participants contacted the research team and were screened by telephone. Those who met criteria were invited to participate. Parents who consented were interviewed by one of the investigators [BL, TP or MS].
Recruitment
Diverse strategies were used to recruit participants. Parents involved in a previous study (Leung et al., 2018) were invited to participate. These parents contacted other parents through their networks, and then snowball sampling continued. In addition, other recruitment strategies included posting information about the study in medical clinics (family doctors, paediatricians and psychiatrists/psychologists), shared with community partners (such as the Family Centre, Addictions and Mental Health Strategic Clinical Network® and Alberta SPOR Support Unit), and through social media such as Facebook posts.
Data collection
A semi-structured guide with open-ended questions and probing questions was used (see Supplementary information Appendix A – Interview Questions for semi-structured interview). Interview questions were piloted to assess for language (understandability), relevance (i.e. makes sense to patients) and comprehension (i.e. content validity). Pilot testing of the interview questions was performed by three parents not in the study, who reviewed the questions and provided feedback on language, relevance and comprehension. Feedback from parents was incorporated to revise the interview guide. Data were collected to saturation where no new themes were derived from the data. Interviews were conducted from October 2017 to April 2018.
Demographic and health-related characteristics of parents and their children.
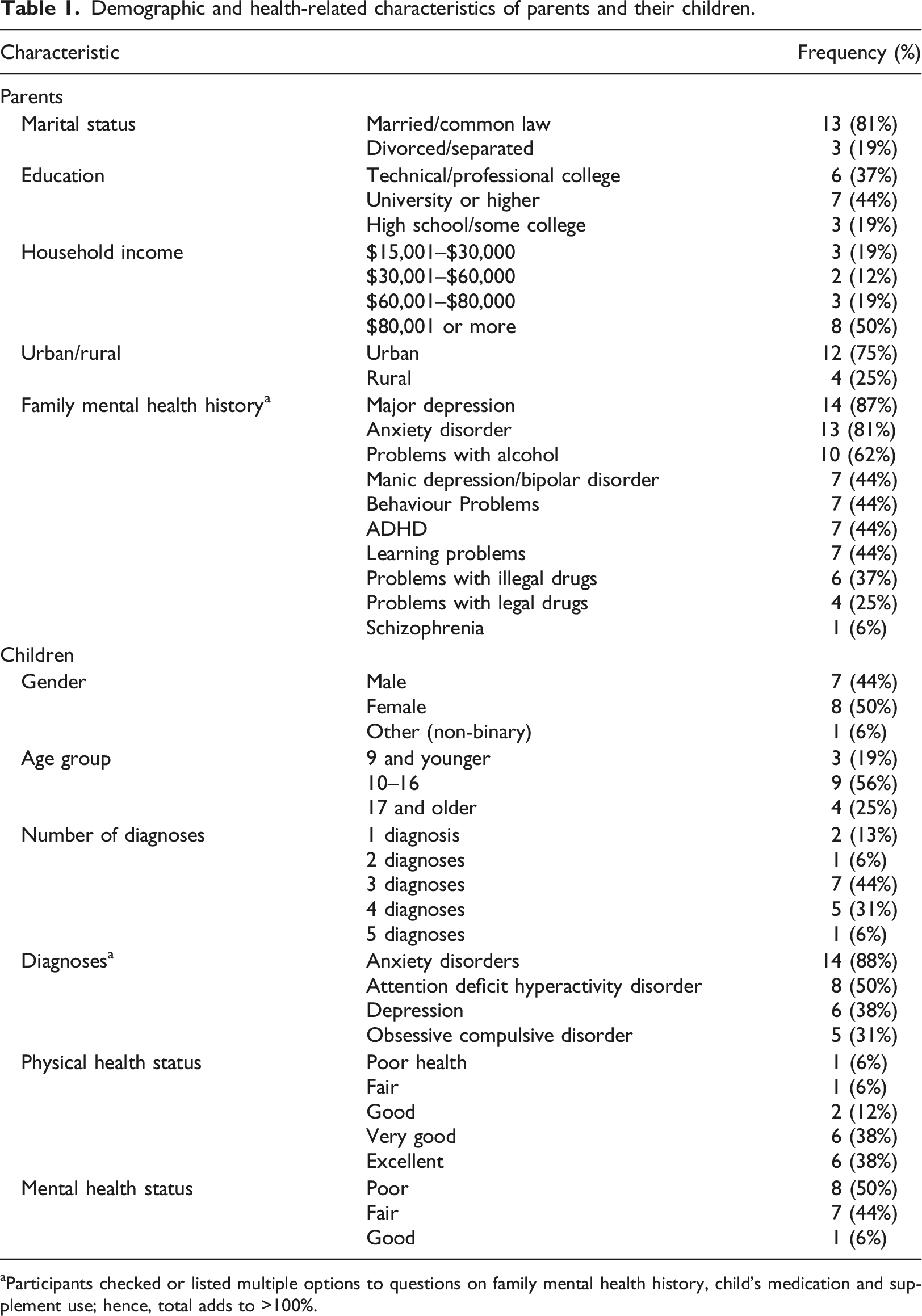
aParticipants checked or listed multiple options to questions on family mental health history, child’s medication and supplement use; hence, total adds to >100%.
Data analysis
Qualitative data collected via interviews were audio recorded and transcribed verbatim, with anonymized names and locations. Thematic analysis of text data was undertaken by two researchers independently. A total of four team members coded the data, and two researchers developed the themes in an iterative process with constant check-ins and comparisons to arrive at consensus.
The researcher read each transcript several times to become familiar with the data. Then we followed the inductive approach of thematic analysis (Braun and Clarke, 2014; Maguire and Delahunt, 2017) to identify the initial codes from the data, using a line-by-line coding. The coding was data driven, meaning the themes were extracted as the data unfolded, using open coding (i.e. not relying on pre-set codes). Each segment of relevant data was coded to produce as many patterns as possible. Each transcript was coded separately by at least two analysts and codes were reviewed, compared and refined to arrive at a consensus. Once the coding was completed, the codes were organized to identify themes.
Themes were derived from the coded data. Emerging themes were obtained with descriptive categories and subthemes (Morse, 2008). Thematic analysis commenced at the beginning of data collection, where researchers familiarized themselves with the data and generated initial ideas of themes to explore in subsequent interviews. Due to this iterative and reflective process, researchers were able to identify the point at which data saturation was reached. Differences with respect to emerged categories or themes were resolved by discussion and consensus by the research team. Overarching themes were formulated to provide insight into the research questions.
The advisory group reviewed transcripts and the themes derived from the data for validity check. Additionally, we used the Consolidated Criteria for Reporting Qualitative Research checklist (Tong et al., 2007) to report all aspects of the study including analysis of the data and interpretation of the results.
Quantitative data from the demographic questionnaire were used to describe the sample characteristics using frequency, proportion, mean and standard deviation (where appropriate).
Results
A total of 36 parents expressed interest in participating and were invited to participate in the study. Of the 36 parents, 16 (15 mothers and one father) were interviewed. Interviews lasted 60–90 min. The reasons for individuals not interviewed included not returning calls/emails, n = 8 (22%), incomplete screening, n = 5 (14%), loss of interest, n = 3 (8%), and not providing consent, n = 3 (8%).
Characteristics of participants
Characteristics of the parents and children are presented in Table 1. Majority of parents were married, n = 13 (81%), had college/professional or university education, n = 13 (81%), and had household incomes over $80,000 Canadian, n = 8 (50%).
Children were equally distributed by gender, with one child self-reported as non-binary. The largest age group was 10–16, n = 9 (56%). For the child’s physical health status, a majority, n = 14 (87%), reported being in ‘good’, ‘very good’ or ‘excellent’ physical health. For mental health status, n = 8 (50%) reported having ‘poor’ status and n = 7 (44%) experienced ‘fair’ mental health. Of the 16 diagnoses reported by parents, the majority of children, n = 14 (88%), had two or more diagnoses. The most common diagnoses among the children were anxiety disorders, n = 14 (88%), followed by attention deficit hyperactivity disorder (ADHD), n = 8 (50%), depression, n = 6 (38%), and obsessive compulsive disorder, n = 5 (31%).
Parents identified a total of 13 medications prescribed to or used by children for their psychiatric condition. The most common drugs used were antipsychotics (risperidone and aripiprazole), antidepressants (fluoxetine and sertraline) and ADHD medications (methylphenidate and guanfacine). Of the drugs used, six children were on antipsychotics, five children used ADHD medications and nine children were on antidepressants. One child used medical marijuana, and one child did not use any medication.
Parents reported the most common supplements given to children were vitamins, n = 11 (69%), followed by fish oils, n = 4 (25%), probiotics, n = 3 (19%), and melatonin, n = 3 (19%). Many children took more than one category of supplements. Four participants, n = 4 (25%), reported no supplementation use. Parents reported multiple psychiatric conditions in their family history, with the most common being anxiety and depression, n = 13 (81%) and n = 14 (87%), respectively, and alcohol use, n = 10 (62%), with one family reported a family history of schizophrenia.
Themes derived from the data
Analysis of the data generated 96 different labels that were then assigned to three main themes: (1) fragmented healthcare services, (2) navigating the complex healthcare system and (3) parents distressed by the system. The following section presents the themes and subthemes (i.e. the gaps identified) and the solutions proposed by the parents.
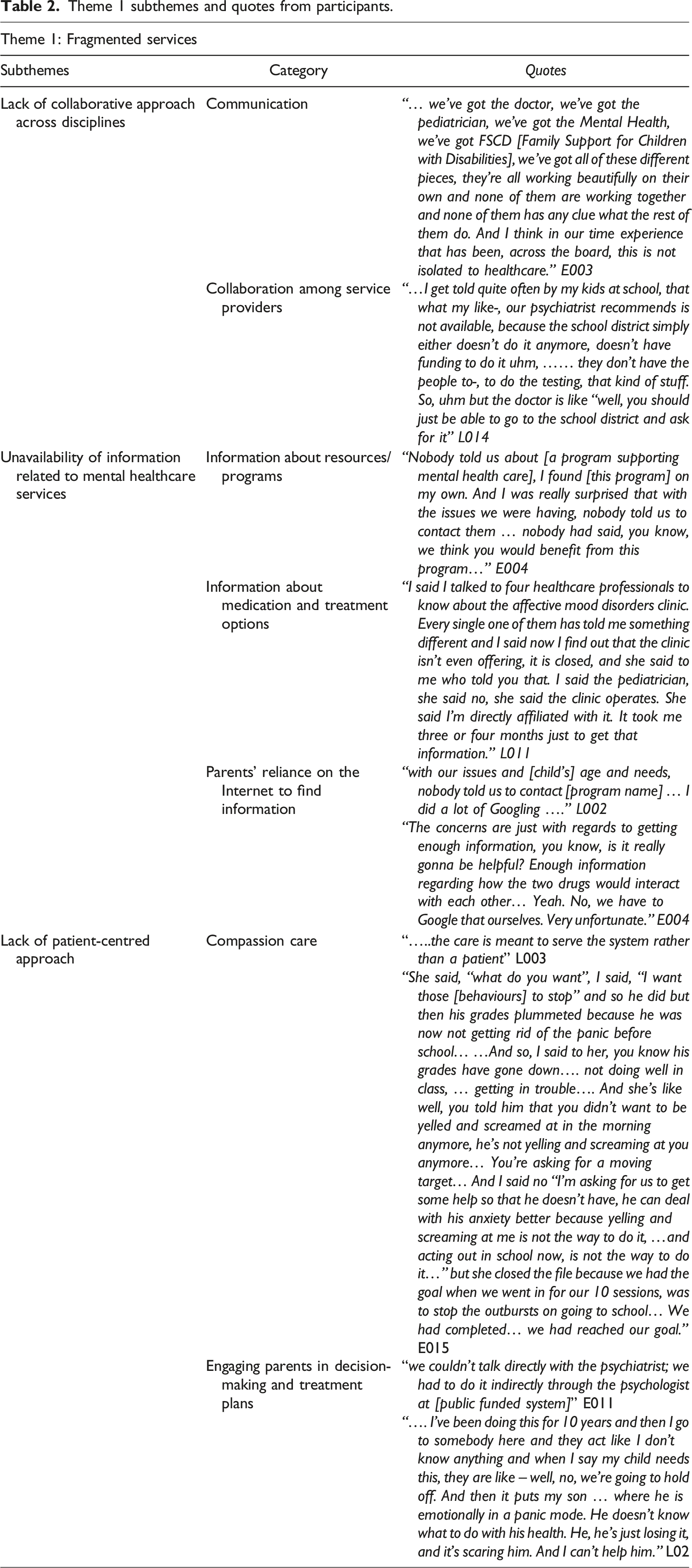
Theme 1: Fragmented healthcare services
Fragmented healthcare services profoundly impacted participants’ experience of mental health care. The first theme is further supported by three subthemes:
Subtheme: Lack of collaborative approach across disciplines including school and community services
Parents reported a lack of collaboration and communication among healthcare professionals in different departments, schools and the community. The services provided by different professionals such as school teachers and counsellors, or sectors such as community services and clinics, are fragmented and disjointed without clear communication among them.
Subtheme: Unavailability of information related to mental healthcare services
Information about resources and treatments was hard to find. Parents were occasionally provided with misinformation. Parents highlighted the lack of resources specifically related to the lack of knowledge by educational and healthcare professionals about available resources and programmes for supporting mental health and education.
Subtheme: Lack of patient-centred care approach
Parents described gaps in patient-centred care, specifically highlighting the need for compassionate care and engagement in decision-making. Parents’ input was not considered when deciding on a treatment plan. Thus, parents felt sidelined in deciding how best to address child’s needs.
Theme 1 subthemes and quotes from participants.
Theme 2: Navigating the complex healthcare system
Navigating the complex healthcare system was hindered by gaps in accessing and receiving care, lack of continuity of care and lack of resources. The inability of parents to find and access appropriate services led to increased visits to the emergency department. These gaps were systemic, such as a bureaucratic structure making referrals a complex process or inappropriate information (including referrals) provided by clinical staff.
Theme 2 subthemes and quotes from participants.
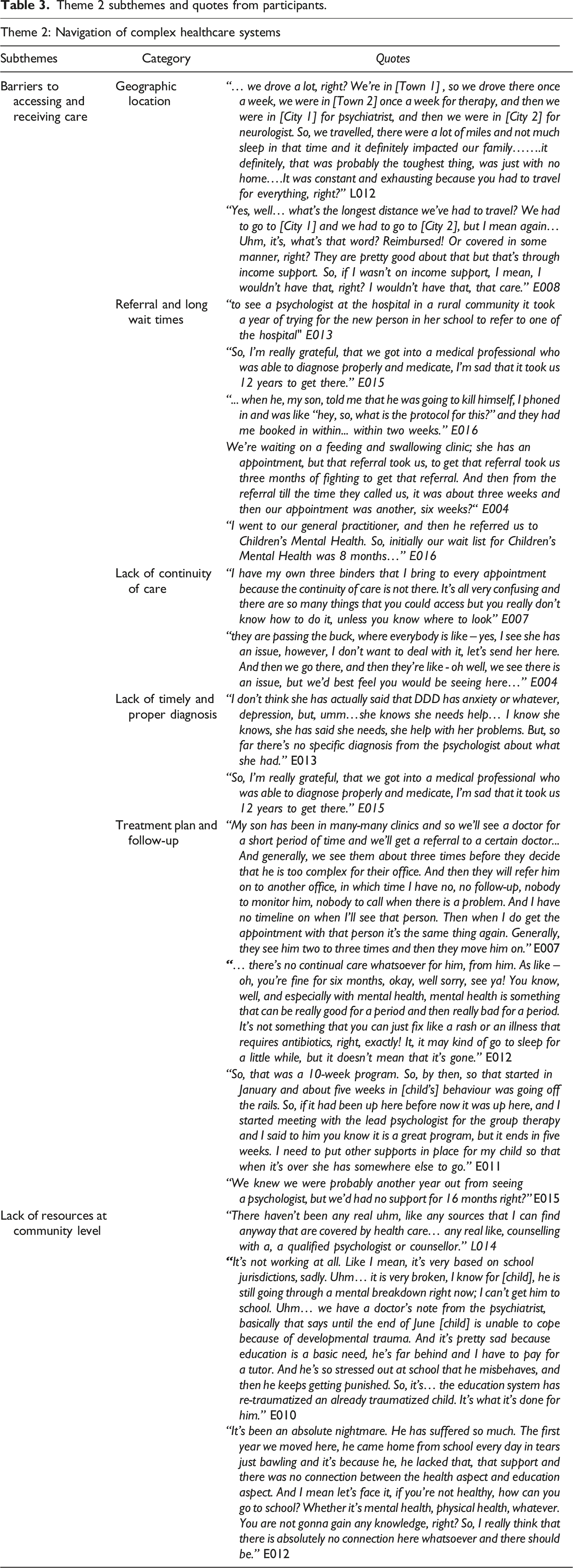
Subtheme: Barriers to navigating and accessing care
Barriers disclosed by the participants included difficulties in accessing care due to: i. Geographic location: Parents living in rural areas had a hard time accessing services as most services were located in urban centres. Driving time as well as indirect and direct expenses attached to driving to urban areas or to bigger rural areas presented a barrier to accessing and receiving care. ii. Lack of continuity of care: Parents described the gaps related to care that is not well-organized as being affected by slow referrals to specialist care and long wait times, lack of proper and timely diagnoses and lack of treatment plans. iii. Referrals and long wait times: Parents waited for referrals to specialists, ranging from school to counsellor, from family doctor to paediatrician, psychiatrist and also to psychologists. iv. Lack of timely and proper diagnosis: Families often required a diagnosis for their child to receive treatment or referrals to programmes. However, obtaining a diagnosis was often fraught with delays and inadequate assessments. v. Treatment plan and follow-up were insufficient as services were often provided within time frames that did not meet the needs of the child.
Theme 3: Distressed parents
Theme 3 subthemes and quotes from participants.
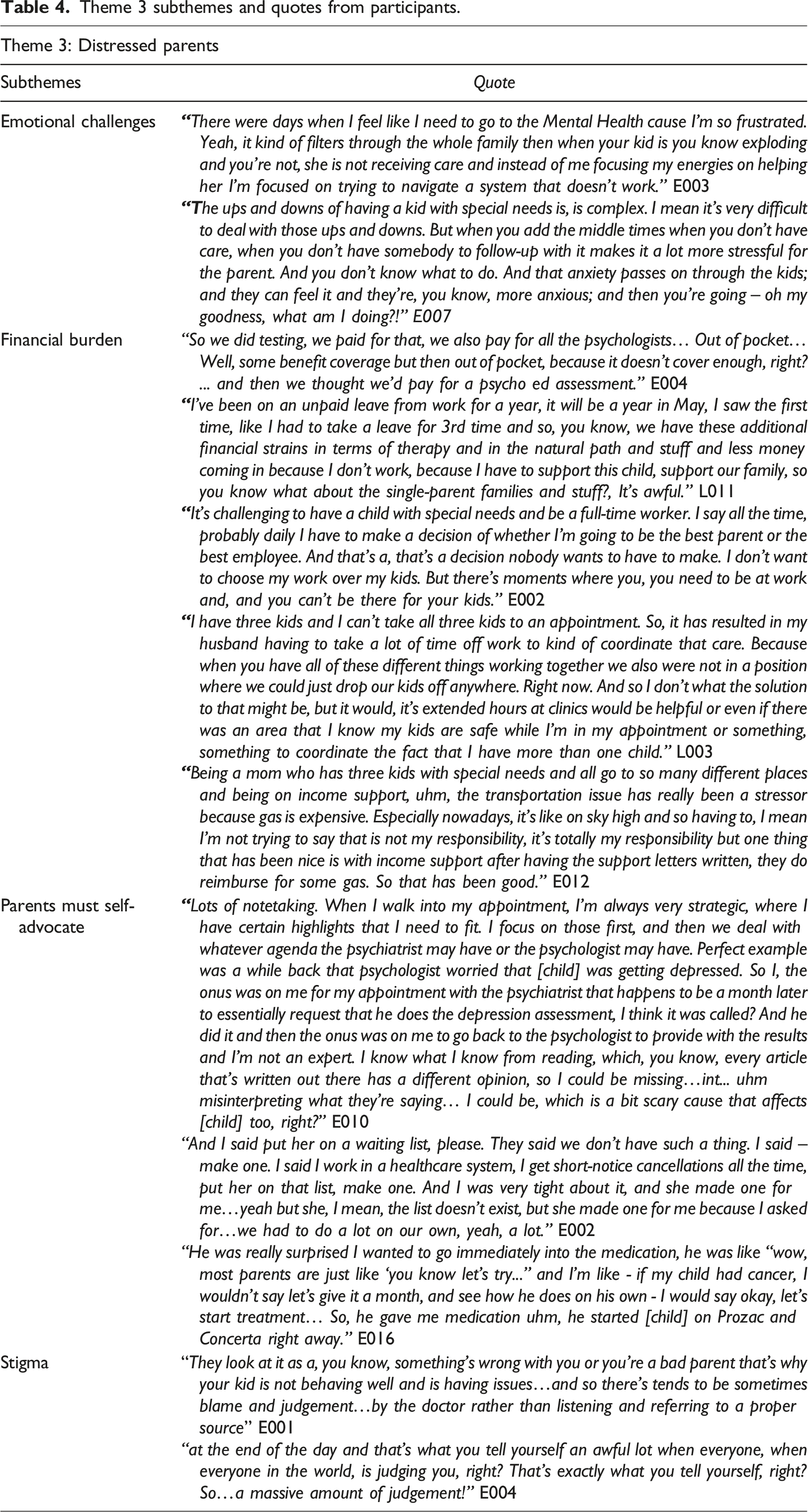
Emotional challenges
Parents described their struggles and trauma related to a fragmented system that is difficult to navigate. Their struggles affect not only their children, many of whom are dealing with suicidal ideations and violent behaviours, but also the family at large, specifically stressors on marriages, single parents and other siblings, in addition to the time commitment involved around the parents’ other daily responsibilities.
Financial burden
Parents faced a considerable financial burden when paying out-of-pocket for services that are not funded to avoid long waits, when treatment did not work, and when their child’s needs were not addressed. Financial burden adds stress to parents that are already struggling to care for their child with the mental health disorder, as well as their other children.
Parents must self-advocate
Navigation within the fragmented healthcare system is impeded by poor continuity of care, and parents need to become advocates for their children needs. Some parents took notes during their visits and others informed themselves using Google to discuss their children care plans, including medications.
Stigma
Stigma came from healthcare providers, friends and family and educators at school. Parents felt blamed, judged and socially isolated because of their child’s behaviour. Parents felt they were judged as ‘bad parents’ for their child’s behaviour instead of receiving the compassion and understanding they needed.
Proposing solutions
Parents proposed solutions when they answered the open-ended question about their vision of ‘an ideal world of a healthcare system that works to meet the needs of both you and your child’. Parents highlighted a need for well-coordinated care across the continuum based on a team approach, that includes navigators and enhance continuity of care to address the existing gaps and promote the integration of healthcare services.
A team approach is described by the parents as healthcare teams where providers work collaboratively to share information, communicate directly with each other and parents and co-design treatment plans for their child’s care. Parents suggested a central location, a one-stop shop including a multi-disciplinary team with the active involvement of a physician trained in mental health, would more effectively address the disintegration of existing services already in place.
“to have a team of people that work together in a central location would be valuable or even to take it a step further to have a psychiatrist in that role might be really valuable as well…and I think that when you have a three-year-old on psychiatric medication, the next natural step would be have a psychiatrist to oversee that” [L003]
Parents suggested centralized coordination with a navigator to oversee the team and its functions in the child’s overall care. This would mitigate many deficiencies in the system, including frontline staff/professionals (including doctors) who lack knowledge of the resources available and are unable to direct families to those resources efficiently.
The navigator could be a case manager or resource worker to assist children with complex medical and mental healthcare needs to follow through with all the different specialities and be the one contact for all aspect of care needed by the child.
“that worker would know ….. [the] issue, then [recommend] this will be the route to go and I’ll make that initial phone call for you and I’ll initiate the referral or – here’s the phone number for you”. Instead, currently, a parent stated “I have my own 3 binders that I bring to every appointment” because the continuity of care is not there. “It’s all very confusing and there are so many things that you could access but you really don't know how to do it, unless you know where to look”. [C007]
“Mental health counsellor – like at Key Connections, e.g. monitor disability (claim) for the insurance company – be the liaison between all of those people to make sure that everybody has the same information (parents, doctor, school)” [C007]
Establishing a team approach with centralized coordination of care would enable streamlining and the continuity of care. In addition, this streamlined approach would also allow for early interventions before the child’s condition deteriorates, requiring more intensive and extensive care.
“Don’t wait until things are dire, which is a level of service that’s incredibly expensive; behaviours get so bad to the point that’s ... hugely stressful and potentially very dangerous for the, for kids and families to be, to be in positions where they are having to kind of navigate this on their own”; “need to catch it earlier, need to recognize the complexity (of what these children need)”. [C006]
Parents also cited the need to have cross-sectoral cooperation of services and professionals in the areas of health, social services, policing and education, at minimum having a line of communication between sectors/professionals:
“parents [are] willing to sign a waiver so that communication between services, departments, professionals, etc. can take place”. [L003]
Another parent proposed a triangle of home–school–community working together:
“they [can] hand you a package and be like this is what’s available to you, like this is what Child’s and Family Services does, this is what Child’s Intervention does, this is what Mental Health does”. [L003]
Parents living in rural areas suggested the use of videoconferencing, so therapists, practitioners and other professionals working with the child could be ‘on the same page’, having an open-line of communication and shared knowledge of various aspects to the child’s care.
Discussion
This qualitative study heard from parents of children with complex mental healthcare needs and learned about their experiences in searching for and accessing mental healthcare services in Alberta, Canada. Parents in our study came from diverse sociodemographic backgrounds, yet their shared experience of accessing care for their child was similar. That is, accessing and navigating the system was difficult regardless of education, income or urban/rural residency. For example, a parent clearly described their struggles to access care living in a rural area, despite having higher education and socioeconomic background that was similar to another parent living in an urban centre but had lower income. Parents highlighted a number of gaps and areas needing improvement. Parents offered insights into potential solutions to these gaps.
In many ways, our results are neither new nor startling but confirm the experiences of families and their concerns and frustrations with regard to the functionality of the healthcare system and its treatment of patients with mental health problems (Boulter and Rickwood, 2013; Crouch et al., 2019; Reardon et al., 2017). Our findings are echoed in a report to The United Way–Calgary and Area which also indicated the inability to access mental health services and supports (i.e. ‘Getting In’ to the system), lack of assessments and support for the whole family, the lack of supports while waiting for and beyond ‘treatment’ and transitioning from adolescent mental services to adult services (German et al., 2018). Their findings also suggested a lack of integration across government, non-government and private organizations at the provincial level. The experiences are similar in both Alberta and British Columbia whereby families had difficulties in accessing screening, diagnostic and interventional services because of geographic isolation, transportation limitations, costs due to limited numbers of healthcare providers responsible for widespread service delivery to a broad geographic catchment area and barriers to services when transitioning from one age group to the next (Young et al., 2019).
The shared experience of families
The challenges experienced by parents in our study are not unique to the Canadian context. The literature highlights parents from a number of Western countries also facing challenges in navigating complex systems, through an often arduous process, to obtain appropriate mental health care for their children (Bone et al., 2015; Boulter and Rickwood, 2013). Parents found it difficult to understand the process to obtain help and encountered numerous obstacles.
Similar to our findings, studies also highlighted parents having to deal with stigma, the lack of integrated healthcare services and a shortage of providers with the expertise in early childhood mental healthcare (Walter et al., 2019). The literature on stigma and mental illness is large; often, stigma experienced by children and their families lead to shame and low expectations, which cause further distress (Heflinger and Hinshaw, 2010). Stigma is a barrier to parents’ help-seeking behaviour, in particular where parents felt ‘blamed’ by professionals (Reardon et al., 2017). Strategies to address stigma need to be done with community, public and social policies as well as health care to shift it (Hinshaw, 2005). The barriers to accessing services can occur in various stages of the help-seeking process, from parental attitudes that influence help-seeking behaviour to accessibility that influences ability to contact services (Reardon et al., 2017; Reid et al., 2011). Conversely, access to services is more likely facilitated by factors such as having affordable and flexible support, enabling trust to be developed with practitioners and reducing stigma for parents and providing clear information on how to access services (Reardon et al., 2017).
Parents expressed a lack of confidence in their healthcare provider’s expertise; they were also unsatisfied with the monitoring of their children’s medication use (Lake et al., 2015). Similar to parents in our study who had to ‘self-advocate’ for care, parents often play a navigator role in accessing mental health treatment and the use of specialist mental health services, thus putting the burden on parents to recognize their child’s mental health needs and having to figure out a pathway for obtaining appropriate care (Crouch et al., 2019). Thus, from Canada to the United States to Australia, families are emphasizing the need for supporting parents in their critical role of identifying mental health problems in their children and gaining early access to appropriate mental health care (Boulter and Rickwood, 2013).
Parents’ vision for ideal care
Parents recommended the creation of a one-stop shop for services with a team approach led by a navigator to facilitate and support coordinated care across disciplines and sectors, from health care to schools, social service, among other community services. Care coordination has a positive effect on timeliness of care (Miller, 2014), including rapid access and early interventions (Settipani et al., 2019), and promotes favourable attitudes by the care team for the children in their care (Young et al., 2020). Coordinated care has been reported to be desired by parents and beneficial for children with mental healthcare needs (Miller, 2014; Settipani et al., 2019); however, it remains an unmet need with a number of barriers to its implementation (Brown et al., 2014). These include lack of service knowledge, limited time and communications (Young et al., 2020), as well as lack of coordination across sectors leading to discontinuity of care and reliance of parents to act in a liaison capacity between practitioners and sectors (Tobon et al., 2015).
Coordination of care across sectors is especially challenging for children with complex mental healthcare needs (Tobon et al., 2015). Barriers to cross-sector collaborations are often due to ideological and structural differences (Wiart et al., 2010), as well as ineffective coordination of services between systems and lack of mutual understanding (Mikkelsen et al., 2013). A number of facilitators have been proposed to overcome these barriers. For example, leadership in the respective organizations can promote a shared culture of care, long-term trusting relationships and key players as ‘bridge builders’ to build knowledge, attitudes and skills for sharing a common vision and language with all partners (Martsolf et al., 2018). Thus, a multi-faceted approach is required to streamline procedural differences and increase interaction, understanding and respect between sectors (Mikkelsen et al., 2013; van Vooren et al., 2020). Resolutions to procedural differences include shared personnel or resources, written agreements and holding regularly scheduled meetings made possible by policies, programmes and fundings that enable cross-sector partnerships (Ladekjær Larsen et al., 2020).
Parents in our study advocated for a ‘navigator’ (i.e. a facilitator or case manager or resource worker) to be the one contact for all aspects of care needed by the child. Research evidence supports collaborative care with a care manager to provide continuous support with the patients including initiating contact with services, follow-up and feedback, as well as facilitating patients to engage in self-management. Benefits to patients, the healthcare system and societal costs were reported to be higher for those with a case manager compared to usual care, for patients with depression (Holst et al., 2018). Navigator programmes have been used in care of chronic diseases such as cancer, diabetes, HIV, cardiovascular disease and dementia (McBrien et al., 2018). While navigator programmes appeared to improve processes of care, less is known about their impact with patient experience, clinical outcomes or costs.
A care ‘navigator’ would facilitate the continuum of care with a team approach and cross-sectoral collaboration as recommended by our study participants. A team approach encourages therapeutic engagement where children and their parents are listened to by building relationship with professionals and taking into account patients’ tolerance of treatment plan and proactive strategies (Bone et al., 2015). A multi-disciplinary team approach has been recommended in mental health services (Chafe and Audas, 2014); however, cross-sectoral collaboration amongst medical providers, social service workers, law enforcement and educators has yet to be explored in Canada. Children with complex mental healthcare needs often require services at the intersection of different sectors. Thus, future research is needed to determine how cross-sectoral corroboration would be managed to protect the privacy and confidentiality of the child and their families while also enabling information sharing to enhance care coordination.
Strengths and limitations of study
A strength of this study is we had participation from across Alberta, including families from different socioeconomic levels and living in both rural and urban communities. Another strength is the insights provided by parents to the issues that have challenged them and the recommendations for strategies to address the gaps in the system which may be tested within the Alberta context and serve as a model for other jurisdictions.
The main limitation of this study is that despite our attempt to find families with both positive and negative experiences, the parents in our study mainly focused on the challenges and negative experiences. These families are more likely to participate in the study as they may be more inclined or invested to voice their concerns. Thus, our findings may be biased towards this singular experience, and less is known about families who have had a mostly positive experience with their services and the processes that worked well for them.
While we did not have enough data to develop into themes, a few parents did voice some of the positive aspects of their interactions within the healthcare system. For example, (1) one parent felt their doctor took time and listened to the parent’s concerns; thus, feeling heard and understood was important to the parent and the care they received; (2) another parent felt they had a voice in the decision-making process; (3) a third parent felt the practitioner acknowledged the parent as a person, was interested in their own mental health needs and self-care and inquired about the parent’s well-being; and (4) another parent said they appreciated the ability to provide input into aspects of treatment, such as duration choice to continue [the treatment] if effective or discontinue if not effective, and integrating different services and therapies, for example, medication, counselling, behavioural therapy and exercise. While some aspects of the patient–practitioner relationship were positive, navigating through the healthcare system seamlessly was the major challenge.
Implications for practice
The findings of this study strengthen the current understanding of patient (i.e. children, parents and families) centred care for children with complex mental healthcare needs. Implications for practice inferred from the results of this study are multifarious. Firstly, an implication for research is the involvement of parents/families (as patient partners or consultants) in the discourse to address barriers and gaps in the healthcare system to find practical solutions in a timely and effective manner. As indicated in our study, the trauma experienced by parents navigating the system has not been well researched to inform changes to services and policy; thus, more research is needed to address this issue. Secondly, the implications for practice include creating a more centralized approach to assist parents/families to better navigate the system and enable parents/families co-design educational material to ensure better access of resources at community level. Thus, programme administrators and managers need to be given the ability (i.e. supported by policy) to create navigator positions and train frontline staff in making appropriate referrals in the pathway of services. Thirdly, the implications for policy are to impart multi-systems guidance for improving access to care, continuum of care across sectors of health, social services, education, among others providing services to children with complex mental healthcare needs to enable cross-sector collaboration. Thus, policies include (1) establishing model of integration of services by enabling coordination of the right service at the right time using a transdisciplinary approach, (2) creating effective lines of communication amongst healthcare providers and across-sectors to enable a continuum of care and (3) developing policies to support families and communities specifically addressing stigma by enabling cross-sector collaboration.
Conclusion
This study identified the gaps and solutions to improve mental healthcare services in a Canadian context. For patients, it means their experience of care is connected and well-organized through their entire care journey, from care provider to care provider, from education to social services to health care and back again. To have an effective and supportive continuum of care, the healthcare system must communicate clearly to families. That is, patients would like to know (1) who is involved in providing and at times directing their care; (2) what is the plan of care and (3) what will happen next.
Supplemental Material
sj-pdf-1-chc-10.1177_13674935211028694 – Supplemental Material for Working with parents of children with complex mental health issues to improve care: A qualitative inquiry
Supplemental Material, sj-pdf-1-chc-10.1177_13674935211028694 for Working with parents of children with complex mental health issues to improve care: A qualitative inquiry by Brenda MY Leung, Cynthia Wandler, Tamara Pringsheim and Maria J Santana in Journal of Child Health Care
Footnotes
Acknowledgements
We thank the parents for sharing their experiences and insights. We also thank members of our advisory group for their valuable input on the process of designing questions for the interview guide, recruitment and checking of the analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Maternal, Newborn, Child & Youth Strategic Clinical Network Health Outcomes Improvement Fund.
Ethics board approval
Ethics approval was granted by the Health Research Ethics Board (University of Alberta), REB# Pro00072489.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.