
Abstract
Child healthcare (CHC) nurses play a crucial role in supporting children and families from early life. This study describes CHC nurses’ experiences of health promotion in Child health service (CHS), focussing on how they develop and apply their competence. Fourteen nurses from five CHC centres were interviewed, and the data were analysed using qualitative content analysis. One overarching theme emerged: tuning in and adapting support for the family in the child’s best interests – supported by three categories: finding opportunities to promote health, growing in one’s work, and organisational support. The findings emphasise CHC nurses recognising their own competence and using learning processes, such as work-integrated learning, to achieve healthier outcomes for children. Continuous professional learning also enables nurses to cope with the challenges of an evolving healthcare environment.
Keywords
Introduction
Understanding health promotion in Swedish Child Health Services (CHSs) requires insight into Child healthcare (CHC) nurses’ clinical experiences (Swedish National Board of Health and Welfare, 2014). Recognition of health promotion as a process and resource enables individuals to increase control over and improve their own health as outlined in the Ottawa Charter (World Health Organization, 1986). Occupational stress among healthcare professionals is a well-known global issue, which affects wellbeing (Brand et al., 2017). Nevertheless, Swedish CHSs form a key health promotion arena reaching nearly all young children, from birth to 6 years of age (Wettergren et al., 2016). The need to promote equal and optimal health and development for children, in accordance with Swedish legislation and guidelines (SFS 2017:30; SFS 2018:1197; Swedish National Board of Health and Welfare, 2014), underscores the importance of CHS work delivered through a child- and family-centred perspective.
The Swedish national CHS programme is structured across three levels: universal interventions for all children, which include standard health visits and assessments; selective interventions for children with specific needs, such as additional visits or consultations with other professionals; and targeted interventions for vulnerable children requiring extra support, including assistance from social services (Reuter, 2018). A prerequisite for meeting children’s unique needs is to identify them by adhering to the national programme through standard visits and providing additional support when needed (Reuter, 2018; Swedish National Board of Health and Welfare, 2014).
Background
Child healthcare nurses’ health promotion competence
Multiple factors can influence CHC nurses’ work in CHSs. According to Ekström-Bergström et al. (2022) and Langeland et al. (2022), CHC nurses need to have specific competence to identify both risk factors and health-promoting factors, encompassing all aspects of child and family health as well as the practice of health promotion itself. A qualitative study from India found that healthcare professionals’ performance in maternal and child health services depends on contextual and health system-related factors, such as supportive colleagues and personal job satisfaction (Gouroumourty, 2025).
Antonovsky (1979, 1987) describes generalised resistance resources (GRRs) – such as resilience and supportive relationships-as determinants of health that help individuals develop a sense of coherence (SOC). SOC enables people to perceive the world as understandable, manageable, and meaningful, thereby enhancing health and decision-making (Lindström and Eriksson, 2011).
Healthcare is in a constant state of transformation, presenting complex challenges that require ongoing adaptation. A key to addressing these changes, as emphasised by Tynjälä (2008), is that workplace learning is essential for fostering lifelong learning. Today, the need for continuous professional development is more pressing than ever, as it facilitates work-integrated learning (WIL), which bridges practical experience with theoretical understanding (Billett and Choy, 2011).
CHC settings function as ‘communities of practice’, where shared participation and interaction foster professional identity and health promotion competence. It works especially when supported by organisational learning (Säljö, 2014; Wenger, 1998). Learning in situated activities occurs through interaction with others (Wenger, 1998; Wenger-Trayner, 2006) and facilitates the development of health promotion competence, particularly when the organisation supports knowledge sharing, skill development, and adaptation to new challenges (Säljö, 2005, 2014). Workplace learning in CHS can, therefore, be understood as WIL, integrating theoretical knowledge with practical experience (Sunnemark et al., 2023). To strengthen individual learning and professional competence, workplaces should provide effective and sustainable WIL opportunities that support continuous learning and the development of expertise in nursing (Andersson et al., 2022). Moreover, reflective practice is essential to enable deeper understanding and professional growth (Schön, 1983).
Previous research
CHC nurses are the first point of contact for families with young children, and a trusting nurse–parent relationship is essential for a healthy outcome (Bohlin et al., 2022). However, nurses sometimes feel that their knowledge of promoting responsive parent–child interactions is inadequate (Eklund et al., 2022). CHC nurses’ experiences of health promotion are shaped by various challenges, including barriers and the need for tailored strategies to enhance understanding and maintain a child-centred perspective (Hallgren et al., 2022; Lind et al., 2024). Bohlin et al. (2025) highlighted health promotion in CHSs as a process of interaction for; sharing, caring and mutual learning, where WIL supports understanding of the dynamic integration of theory and practice, as described by Pennbrant and Svensson (2018). Previous research highlights gaps in CHC nurses ‘supportive abilities and the need to enhance their capacity for accessibility and inclusiveness (Engström et al., 2021).
To explore how CHC nurses apply their experience, skills, and competence in health promotion, it is necessary to examine their work practices (Harder et al., 2017).
Considering previous research and the role of reflection on experience in developing competence (Schön, 1991), there remains a gap in knowledge regarding how CHC nurses develop and apply their competence in health promotion.
Aim
To describe nurses’ experiences of health promotion in child healthcare.
Methods
Design
This study employed a qualitative method with an inductive approach, aiming to identify patterns from individual interviews (Polit and Beck, 2021). The interviews with CHC nurses were conducted in their workplace.
Ethical considerations
Ethical approval was obtained from The Swedish Ethical Review Authority, registration number 2022-03858-01. The study was conducted in accordance with the Declaration of Helsinki (WMA, 2024). Participants received both written and verbal information about the study’s aims and provided their written informed consent. Participation was voluntary, and participants were informed that they could withdraw from the study at any time.
Data collection and participants
Data were collected at five CHC centres with CHC nurses working with families from diverse backgrounds. Purposive sampling ensured participation. All CHC nurses were specialised in working within the national CHS programme, including growth monitoring, health counselling, vaccinations, and home visits for infants.
The study was conducted from 5th October 2022 to 9th February 2023 at five CHCs in western Sweden. Eight CHCs were invited to participate; three managers could not be reached, while five agreed to take part and granted the researchers permission to invite CHC nurses. All participating centres are part of the Swedish primary healthcare system, either publicly or privately managed, and publicly funded.
The interviews were conducted in the nurses’ consulting rooms or in other rooms where privacy could be ensured. The first author (VB) approached the study with preunderstanding based on experience as a former CHC nurse. The initial questions were ‘What does health mean to you?’ and ‘What does it mean to you as a CHC nurse to work with children and families to promote health?’
Data analysis
Examples of the coding process.
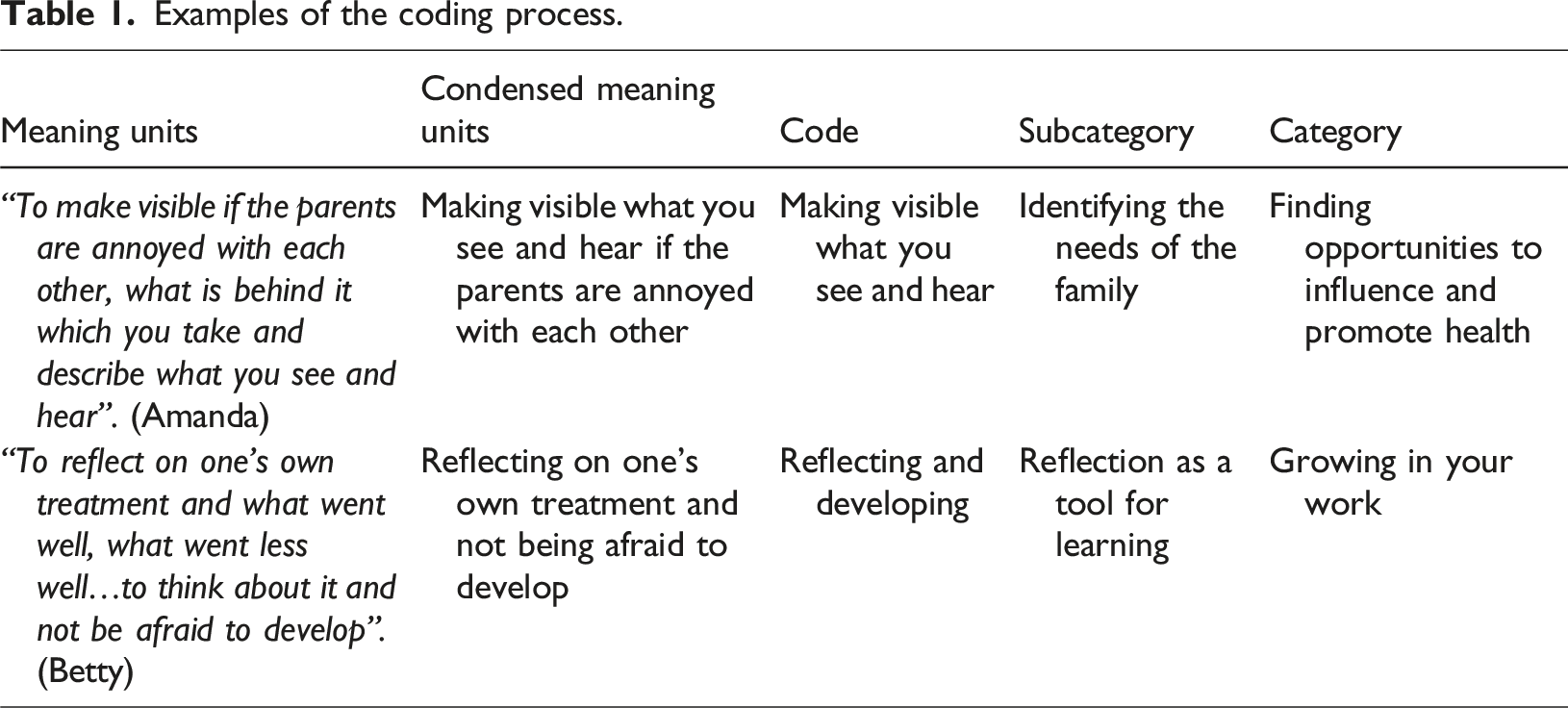
The authors discussed the codes collaboratively to minimise subjective interpretation, drawing on their nursing experience. The codes were organised into subcategories and overarching categories, leading to an overarching theme. The analysis involved an iterative review to identify a common thread and relate the content to the study’s aim to increase trustworthiness (Graneheim et al., 2017; Guba and Lincoln, 1994).
Findings
Description of the participants.
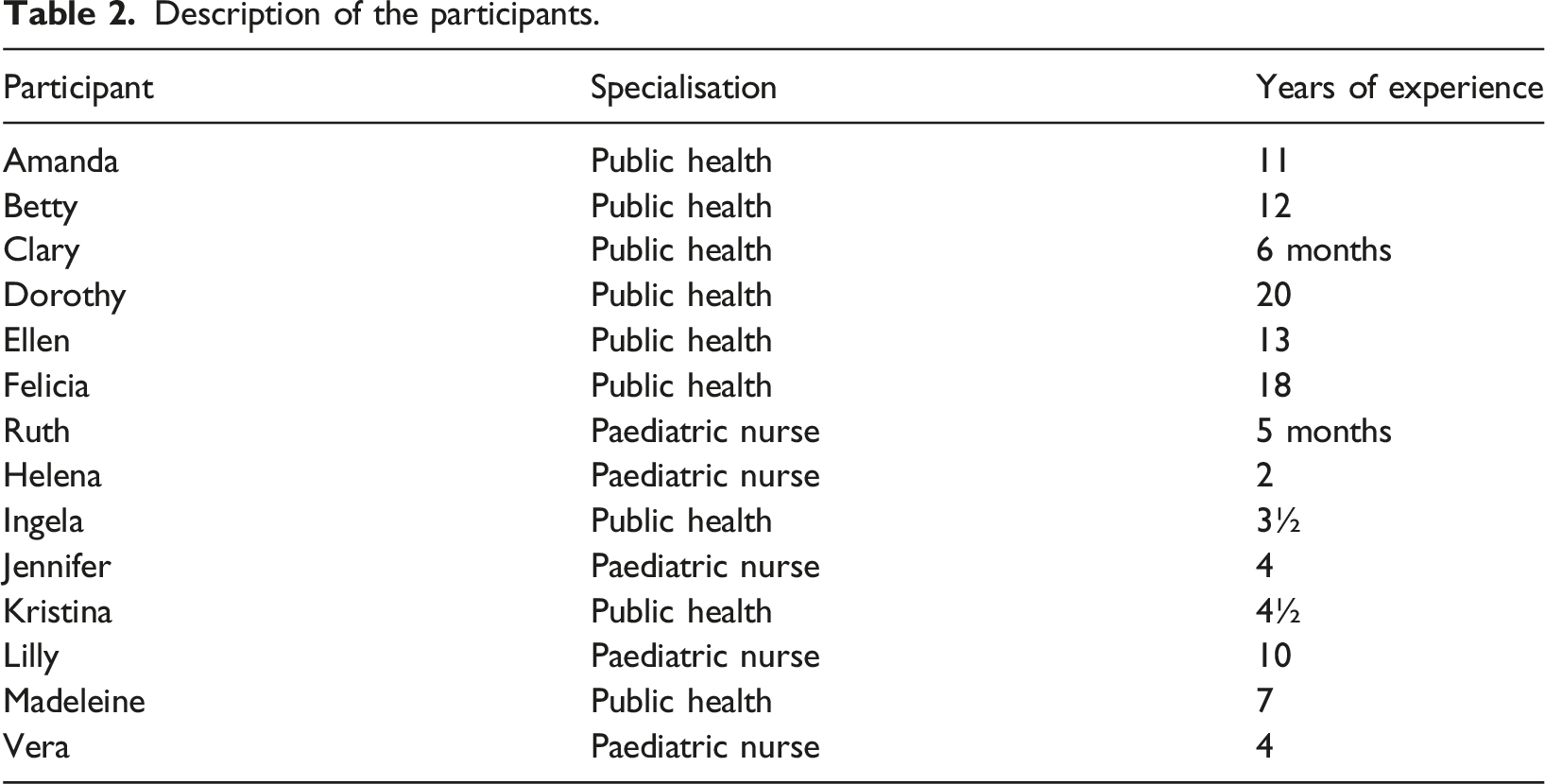
Participants had 5 months to 20 years (mean 7 years 10 months) of CHC experience and were aged 36–60 years (mean 49 years 10 months). Interviews lasted between 24 min and 1 h 8 min, totalling 8 h and 47 min (mean 37 min).
Overview of the overarching theme, categories, and subcategories.
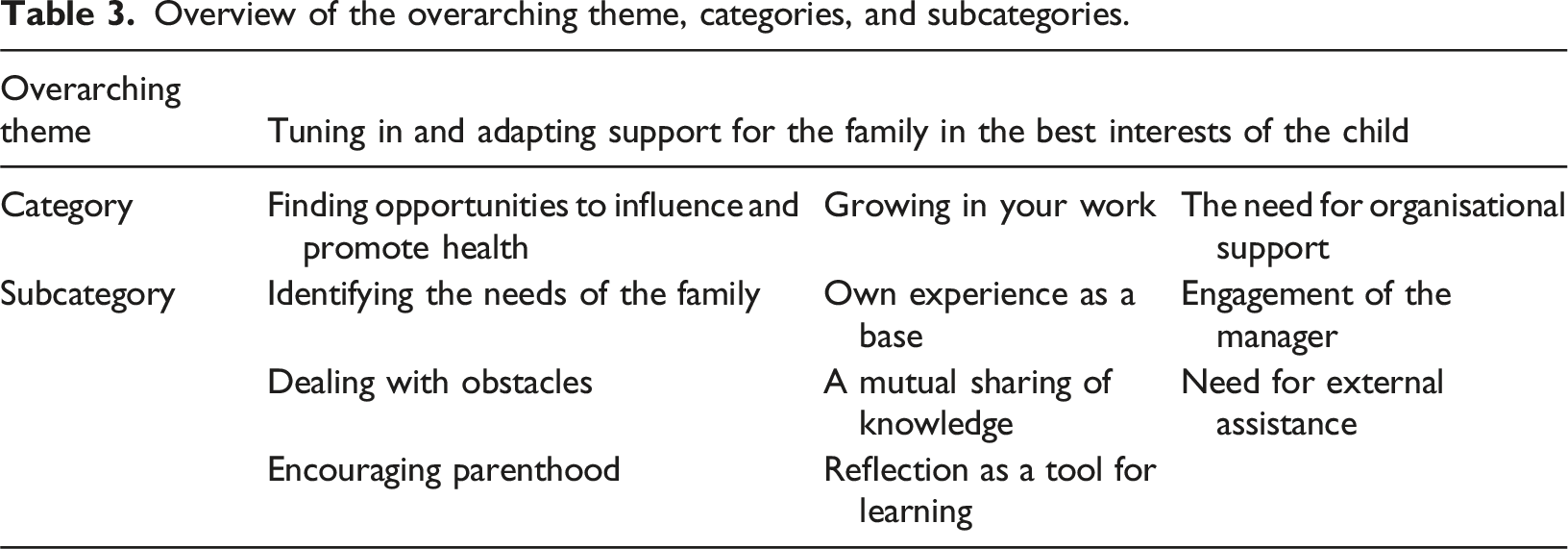
Finding opportunities to influence and promote health
Opportunities to influence and promote health allowed the nurses to make a meaningful difference for the children. Health promotion was central to their work, reflecting their impact on children’s development. Inclusivity and trustworthiness were prerequisites for identifying families’ needs, supporting parenthood, and addressing challenges.
Identifying the needs of the family
The CHC nurses described encounters as opportunities for active listening and patience, aiming to convey a sense of security and build trust. Gaining the trust of both children and families was essential for identifying their unique needs and establishing positive relationships. Consequently, it was important to include all family members and recognise each of them as individuals.
Once trust was established, parents opened up, allowing the nurses to address each family’s concerns effectively. Open communication was crucial, even on challenging topics, helping both nurses and parents feel comfortable asking questions. A CHC nurse illustrated how to achieve a successful encounter in the following quotation. I think the most important thing in the encounter itself is that we work from a health perspective, to succeed in making the parent feel safe about being able to ask and be unsure and dare to mention things that they feel in their parenting (Lilly).
The CHC nurses described various family situations, such as when a single mother required special attention, highlighting the importance of identifying the child’s and mother’s social network and support system. By observing parents’ cues, nurses recognised family resources, understood unique needs, and provided support through universal or additional CHS interventions.
To understand families’ needs during encounters, CHC nurses adapted their approach to each family unit, making the family’s perspective central to promoting the children’s best interests.
Family participation and needs could vary between visits. This meant that adjusting support was an ongoing process that sometimes required multiple encounters. CHC nurse Ruth emphasised mutual understanding as a key step in gaining a comprehensive view of the family. and because we meet so often, you usually get small things each time that you can try to put together to form a picture (Ruth).
The CHC nurses emphasised that actively listening and empathy provided valuable insights into the families’ situations hence accurately identifying families’ needs also required parents to be receptive and engaged. Some participants noted that responsive parents often asked questions and showed interest in learning more.
The CHC nurses shared examples of openly framed questions that allowed families to express their needs. By listening to parents’ responses, nurses identified potential risk factors. Occasionally, when parents did not respond, the nurses adapted by asking more focused questions. One participant noted her principle of treating others as she would like to be treated.
Dealing with obstacles
All CHC nurses reported obstacles during parent interactions. Some parents resisted advice, interpreted by the nurses as signs of insecurity in their parenting. This resistance made it difficult to identify certain risk factors, as parents often refrained from answering questions. To address this, CHC nurses employed various strategies to understand parents’ needs and encourage them to engage. This approach was vital in sensitive situations, such as childhood obesity or parental vaccine hesitancy, with the nurses’ focussing on the child’s best interests. When parents remained unreceptive – for example, refusing vaccination – nurses provided information on its importance. At a vaccination age I will ask parents again, so they don´t have to come every time and feel that we are going to argue again (Amanda).
CHC nurses sometimes worked with parents’ receptivity over an extended period. With time, initially non-receptive parents became more responsive. Some nurses emphasised skills such as patience and sensitivity in tuning their support to meet parents’ needs, helping them become more attentive to their child’s wellbeing.
Time pressure was another obstacle. Tight schedules required prioritising visits for younger children, delaying older children and regular home visits for eight-months-old infants. CHC nurses sometimes had to forgo breaks to manage their workload.
Encouraging parenthood
All CHC nurses appeared confident in their role of supporting and encouraging parenthood. Their aim was to help parents feel secure by providing tailored health promotion advice. Some described how they encouraged parents to find solutions using their own resources. Supporting parents in building trust in their parenting involved fostering self-esteem through affirmation and encouragement, enabling them to feel confident in asking questions. Several nurses noted that parents developed and gained confidence when they could formulate their own questions. Strengthen their confidence in their own ability (parents) to do the right thing for their children and to think correctly themselves about the decisions they make (Betty).
Parent groups served as a forum for meeting other parents and creating support networks. These networks provided opportunities to discuss everyday challenges related to their children and to offer mutual support.
Growing in your work
CHC nurses emphasised that their professional experience was essential for their growth in practice. The mutual sharing of knowledge between nurses and parents depended on their previous professional experiences, which they drew upon during encounters with families. The nurses also recognised the value of reflecting both during and after interactions to learn from their experiences with children and parents.
Own experience as a base
The nurses adapted their knowledge based on experience and the needs of each child and family. They also described their professional experience as a source of strength and security, providing confidence even when specific knowledge was lacking. The CHC nurses were self-assured in their role, recognised gaps in their knowledge, and actively sought to acquire the necessary skills and information.
The nurses were also aware that their experiential knowledge expanded as they encountered different family constellations. They described their growing experience as ‘baggage’ – a valuable knowledge base.
Despite their experience, maintaining professionalism could be challenging, as encounters with complex family issues sometimes triggered lingering emotions.
While maintaining a professional stance during these interactions, the emotional impact of challenging encounters could persist afterwards. The nurses described relying on their intuition and tacit knowledge, often sensing that something might be wrong based on a ‘gut feeling’.
They also emphasised using their accumulated experience appropriately to meet the needs of each child and family. We all have our baggage with all our different points of view, so that as a CHC nurse you always get to see what kind of person you have in front of you in every encounter (Ingela).
A mutual sharing of knowledge
The CHC nurses described knowledge sharing as a natural and valuable process. They highlighted mutual exchange and the importance of active listening. Parents were regarded as active participants in this exchange.
The nurses consistently adapted the information they provided based on what they learnt during the encounters. Sometimes, they recognised that the parents could not absorb all the information at once, so they shared it in smaller portions over multiple interactions. One CHC nurse referred to this approach as ‘knowledge injections’.
Knowledge sharing between CHC nurses and parents extended beyond spoken words to include body language. Some CHC nurses sensed emotional cues, remaining receptive to parents’ words and body language. It feels as if you relieve someone sometimes by taking it (emotions) (Kristina).
Through active listening during mutual knowledge sharing, CHC nurses could acknowledge and ease parents’ emotions, recognising that parents possessed valuable insights about their children that the nurses needed to understand.
Reflection as a tool for learning
CHC nurses’ need for reflection arose in different situations but carried a consistent purpose: to understand why they reacted as they did in interactions with children and parents. One reason reflection was necessary was that nurses often absorbed and processed parents’ emotions during active listening. As time for formal reflection was limited, they frequently had to carry these emotions and experiences with them throughout the day, which could resurface after work, such as in the car or at home, highlighting the importance of organised reflection time. Another key reason for reflection was to facilitate knowledge sharing and mutual learning. When nurses had the opportunity to reflect on a family prior to an encounter, it allowed them to retain insights and enhance their understanding for future interactions.
Letting go of certain emotions and situations could be difficult, prompting CHC nurses to seek opportunities to debrief and reflect with colleagues. This highlighted the importance of collective reflection for learning and professional growth. Some nurses described reflection as valuable and developmental for the nursing profession. Although there was no designated time for reflection, it was common practice to seek out a colleague when needed.
Additionally, the nurses maintained ongoing contact with the child psychologist regarding challenges with children and families, providing further opportunities to reflect with others and to understand their own reactions in various situations. Then sometimes there can be things that you find out that might be good for your colleagues to know too, some cultural difference or something (Madeleine).
They also believed that reflecting and learning collaboratively with colleagues could lead to meaningful and necessary changes in the workplace.
The need for organisational support
CHC nurses highlighted the need for organisational support in their health promotion work with families, emphasising both managerial engagement and access to external assistance.
Engagement of the manager
The CHC nurses described the manager’s commitment as an important source of professional support. Having a manager who advocated for them and spoke on their behalf in various situations was particularly meaningful. Another way a committed manager could provide support was by allocating regular, structured reflection time. Although nurses reflected individually, having designated reflection sessions was valuable, as it ensured that all CHC nurses had the opportunity to engage in the process. Organised reflection time became easier to implement when it was established as a routine known to everyone. …we brought up a case and reflected so it was very good (Felicia).
A set time for reflection was considered support from a committed manager.
Need for external assistance
Social Services was an important source of external support when a child required additional assistance. Occasionally, CHC nurses needed to alert Social Service about a child of concern; however, they did not always receive the expected support, which could be frustrating. Lack of assistance sometimes arose unexpectedly in situations where help was needed for a child.
Another source of external support was the Central Child Health Service Unit, which provided training and regular meetings for all CHC nurses in western Sweden. Nurses valued this support, as it allowed them to feel acknowledged and to receive training on various topics, such as postpartum depression screening and breastfeeding.
Collaborative networking involved working with others to focus on the child and strengthen support for children and families. This included partnering with libraries to organise visits for parent groups, teaching the importance of language and introducing books. Networking could also mean involved coordinating with midwives to hold joint parent group sessions arranging schedules in collaboration with yoga studios sometimes, which many mothers attended for exercise. In addition, collaboration with preschools was important when multiple perspectives were needed to assess a child’s situation. Through such partnerships, organisations such as CHC centres and preschools could advocate more effectively for the best interests of the child, as they could consider the child’s needs from different angles.
Discussion
The findings highlight CHC nurses’ professional experiences in health promotion work and the continuous process of applying both theoretical knowledge and practical experience to provide tailored support. Awareness of the interaction process when encountering children and families, combined with WIL, integrating theoretical knowledge with practical experience (Sunnemark et al., 2023), and the process of sharing and mutual learning as a form of healthy learning (Bohlin et al., 2025; Lindström and Eriksson, 2011), can serve as a foundation for preparing and guiding health promotion in clinical practice.
By actively listening and adapting their work to meet each child’s and family’s individual needs, CHC nurses strive to create a safe and trusting relationship where the child’s health and wellbeing are the focus. Their flexible interactions contribute to ongoing professional learning and the development of health promotion competence. However, the findings highlight several obstacles to fully utilising professional competence and reflection time, particularly due to tight schedules, which can increase the risk of suboptimal outcomes for children. The subcategory Dealing with Obstacles illustrates how limited time can make it difficult to prioritise breaks or follow-ups, leading to potential ethical stress when nurses cannot provide tailored support. Tight schedules are particularly critical because neglecting or delaying health visits under the universal measures of the national CHS programme prevents nurses from assessing children’s needs and supporting optimal health and development, as outlined in Swedish legislation and guidelines (SFS 2017:30; SFS 2018:1197; Swedish National Board of Health and Welfare, 2014).
The category of Growing in your work addresses the requirement for CHC nurses to grow in their profession and professional role in order to promote health in the child´s best interest. The subcategories Own experience as a base is about being able to handle health promotion from one´s own experience. The mutual sharing of knowledge depended on previous experiences and is needed in the encounter between a nurse and families, as well as acting as a tool for a healthy outcome. According to CHC nurses, The need for organisational support is crucial both internally and externally. The manager´s engagement was obvious when there were opportunities for a specific reflection time in the workplace. These reflection sessions ensured that the CHC nurses remained engaged with the ongoing processes.
The need for external assistance was important so that health promotion work could continue uninterrupted when the child required such assistance. When Social Services failed to respond adequately, the CHC nurses felt neglected and there was a risk of ethical stress, which could be detrimental to children´s health outcomes. According to Article 3 of the United Nations Convention on the Rights of the Child (SFS 2018:1197), all children have the right to have their best interests treated as the primary concern.
When nurses cannot tune in to children’s unique needs, their professional competence is underutilised, health promotion work is compromised, and children’s chances of achieving a healthy outcome are reduced. If parents feel disempowered, collaboration with a CHC nurse may become more hierarchical and less partnership-oriented (Reeder and Morris, 2021), limiting SOC development for both nurse, child and family, potentially affecting children’s future experiences with healthcare (Sahlberg et al., 2020). Therefore, the wellbeing of CHC nurses is crucial for effective health promotion (Brand et al., 2017).
Despite the challenges, CHC nurses’ descriptions of opportunities to influence health promotion demonstrate that they experienced SOC, as their work was meaningful. This aligns with research showing that SOC provides health benefits and supports professional engagement in health promotion (Antonovsky, 1987; Lindström and Eriksson, 2006; Vinje and Mittelmark, 2006). This may help explain why CHC nurses choose to remain in CHS despite the risks of ethical stress, highlighting the importance for healthcare organisations globally to prioritise nurses’ wellbeing (Brand et al., 2017). Antonovsky (1979, 1987) emphasised that GRRs are important for managing stress and promoting health. CHC nurses apply their skills – such as patience, tact, and professional knowledge – as GRRs to strengthen children’s and families’ own resources, thereby enhancing the potential for positive development and healthy outcomes.
Sometimes, good intentions did not lead to the desired outcomes. For example, within the category Identifying the Needs of the Family, one CHC nurse explained that her intention was to treat parents as she herself would like to be treated. This reflects a normative approach to encounters. Instead of tuning in to the unique needs of the family, the nurse relied on her own norms, which meant that the family’s specific needs could be overlooked. This finding highlights the importance of nurses being aware of their own values and assumptions, as prescribed norms may inadvertently exclude rather than include families, consistent with findings from a study on CHC parenting groups and reasons for non-attendance (Forslund Frykedal et al., 2019).
The participating CHC nurses appeared aware of the importance of reflection for their professional growth. During the encounters, theoretical knowledge was integrated into practice through a dynamic process of WIL, with nurses reflecting on their actions to plan future support for families. They also navigated the lack of dedicated reflection time by spontaneously seeking out colleagues when needed. The crucial skill of tuning in and recovering from emotional strain may be difficult without opportunities to process emotions. Reflection is essential for professional development, both in and on action (Schön, 1983). Rather than relying solely on structured reflection sessions, nurses initiated discussions with colleagues using shared dialogue to process experiences and insights in real time. This demonstrates their flexibility and awareness within the constraints of demanding schedules, while also highlighting the need for allocated time in CHC nurses’ schedules to safeguard children’s rights as active participants in encounters (Sahlberg et al., 2020).
Research emphasises that learning occurs through experiences in interactions, which is a fundamental process for developing expert competence (Hutchings and Jarvis, 2012; Tynjälää, 2008). CHC nurses rely on collaboration with other professionals to complement and strengthen their own competence. By working together and sharing experiences, they create a community of practice where knowledge can be deepened and professional practice further developed (Lave and Wenger, 1991).
Limitation
One limitation of the study is that another data collection had been conducted prior to the interviews with twelve of the participants, which may have influenced their responses. Another limitation could be the amount of participating CHC nurses, though a strength of the study is the broad sample of them, drawn from five centres located in both well-functioning urban areas and rural areas with fewer amenities. Another strength is that all authors are nurses with specialisations within healthcare, neonatal intensive care and pedagogy, each bringing diverse experiences, providing valuable preunderstanding of nursing competence. To strengthen credibility and facilitate transferability, the analysis process was presented in tabular form. The findings were also discussed by all authors to ensure trustworthiness and reflecting against the literature (Graneheim et al., 2017; Guba and Lincoln, 1994).
Implications for practice
CHC nurses awareness of their professional skills and competence is crucial for promoting the best interests of the child, thereby increasing the likelihood of positive health outcomes. It is important to have a pedagogical theme as a basis for discussion so that the CHC nurses can have conversations in workplace, about how to handle practical experiences with theoretical knowledge. In this way, opportunity to enhance lifelong learning is created. WIL can serve as a pedagogical approach to prepare nurses for effective health promotion in CHS’s.
Further research is needed to explore how healthcare settings can best provide wellbeing and support for CHC nurses, enabling them to deliver high-quality health promotion.
Conclusion
The findings highlight the importance of CHC nurses becoming aware of their own competence and using learning process, such as WIL, to promote the best possible health outcomes for children. Findings also highlight the fact that workplace conditions can strengthen or weaken an individual’s SOC. The CHC nurses needs to have the ability to tune in to the unique needs of the child and family. Therefore, managers need to give them opportunities to reflect with each other for developing SOC and a lifelong learning in the child´s best interests. Continuous professional learning also supports nurses in coping with challenging healthcare changes.
Footnotes
Acknowledgements
We wish to thank all participating CHC nurses for valuable knowledge sharing in taking time to share your experiences.
Ethical considerations
Ethical approval was obtained from the The Swedish Ethical Review Authority, registration number 2022-03858-01.
Consent to participate
Informed consent to participate in written and verbally.
Consent for publication
Informed consent in written and verbally.
Author contributions
All authors contributed to the conception and design of the study and methodology. Acquisition and compilation of data; first author. Data curation, all authors. Analysis and interpretation of data, ethical permission application, all authors. Project administration, first author. All authors have been involved in drafting and critically revising the manuscript, validation of the results, and approval of the final version for publication. The authors are responsible for all aspects of the work and have ensured that questions related to the accuracy of any part of the work were appropriately investigated and resolved.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Department of Health Sciences, University West, Trollhättan, Sweden and The Red Cross Home Foundation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are kept in a locked, safe server for research use at University West. The participants in this interview study did not consent to having their data publicly available as they contained personal information that could be used to identify them.