
Abstract
Nurses and midwives can be instrumental to global efforts to address child abuse and neglect through a public health approach of prevention and early intervention. However, there is limited understanding of nurses’ and midwives’ roles, and no international or local guidelines to inform and evaluate their safeguarding practices. The aim of this modified Delphi study was to build consensus on the nature and scope of nursing and midwifery practice in safeguarding children in Australia. Sixty-four statements located within seven clusters were developed from a literature review and nursing and midwifery practice standards. Participants (N = 102) were nurses and midwives working with children in diverse contexts. They were asked to indicate the importance of each statement to their practice setting. Consensus (80%) was achieved on all statements in Round Two. Findings highlight that participating nurses and midwives agreed safeguarding children is a core component of their practice in diverse child-focussed settings. Findings can inform ongoing discussions about development of nursing and midwifery practice standards and guide effective workforce preparation, education, support and resourcing. Further research about ongoing development of nursing and midwifery roles in safeguarding children is essential to explore how to most effectively mobilise these professions to prevent child abuse and neglect.
Introduction
Nurses and midwives are the largest group of health professionals and have unique capacity to promote children’s health, safety, development and wellbeing (World Health Organization, 2020c). Internationally, nurses and midwives can contribute to better outcomes for children by advancing the Sustainable Development Goals and the United Nations Children’s Fund (UNICEF)(2022) goal that ‘every child, including adolescents, is protected from violence, exploitation, abuse, neglect and harmful practices’. Protecting children from violence and abuse requires investment in a public health workforce that can identify and intervene early when children and families experience adversities (Lonne et al., 2020; UNICEF, 2019). In doing so, services must be accessible and equitable for all, so children experiencing the greatest adversities can be supported to reach their full potential (UNICEF, 2016). A public health response to inequities in childhood that contribute to violence, abuse and neglect can prevent many problems before children are seriously harmed (Higgins et al., 2019; World Health Organization, 2016).
Nurses and midwives can be core to supporting children to thrive, but the scope of their complex roles in prevention and early intervention for child abuse and neglect is poorly understood (Lines et al., 2018; Peckover and Appleton, 2019). Nurses and/or midwives are explicitly named in some policies for addressing child abuse, but clear and comprehensive explanations of their roles are absent (Clark et al., 2017; Peckover and Appleton, 2019). For example, in the United Kingdom, responsibilities of nurses who have designated safeguarding roles are clearly outlined, but responsibilities of all other nurses working with children or families are not (Her Majesty’s Government, 2018). Similarly, in Australian policies for children’s protection, health, welfare and development, nurses’ and midwives’ roles are either missing or mentioned in scant detail (Lines et al., 2022). This lack of policy recognition is incongruent with international evidence demonstrating nurses’ essential roles in promoting health and wellbeing across the lifespan, including through violence prevention (World Health Organization, 2020c). Without clear understanding of nurses’ and midwives’ roles, there will be insufficient infrastructure for workforce education, resourcing and evidence-based practice development to support children to thrive.
In the Australian context, the Safe and supported: national framework for protecting Australia’s Children emphasises it is ‘everyone’s business’ to ensure children thrive in families and communities that are free from abuse. Although ‘strengthening the child and family sector and workforce capability’ is a priority of Safe and supported, nurses and midwives are not mentioned (Commonwealth of Australia, 2021). The lack of guidance for nurses and midwives from Safe and Supported and other Australian policies is a barrier to effectively mobilising this large existing, highly educated workforce to prevent and respond to child abuse. More broadly, Australian registered nurses and midwives are regulated by the Registered nurses standards for practice (Nursing and Midwifery Board of Australia (NMBA), 2016) and Midwife standards for practice (NMBA, 2018), respectively. Furthermore, nurses or midwives working in certain specialist areas have additional standards outlining the unique expectations for nursing/midwifery practice in these settings (Wightman et al., 2021). However, despite the array of local standards and guidelines, there is no consensus about what nurses and midwives do in a public health response to child abuse and neglect. In the absence of a single source of guidance, this study aims to build consensus around the nature and scope of Australian nursing and midwifery practice in keeping children safe.
Aim
To build consensus about the nature and scope of Australian nursing and midwifery practices in safeguarding children to inform how they contribute to a public health response to keeping children safe from abuse and neglect. The two specific objectives were: (1) to investigate nurses’ and midwives’ perceptions of their role in keeping children safe and (2) identify the nature and scope of nurses and midwives safeguarding roles in diverse child-focussed settings in Australia.
Methods
A modified Delphi technique (Keeney et al., 2011) was used to identify the nature and scope of nursing and midwifery practices in safeguarding children in Australian settings. A Delphi study is a multi-stage, iterative process facilitated by a research team whereby a group of experts work towards consensus on a topic (Keeney et al., 2011). In doing so, a Delphi study synthesises and co-constructs knowledge from lived-experiences of experts to negotiate shared understandings on the research topic (Jünger et al., 2017). This study used a modified Delphi technique, whereby the authorship team developed statements for Round One based on literature reviews and nursing/midwifery practice standards. A Delphi technique was an appropriate methodology because there are no existing Australian standards for nurses’ and midwives’ roles in keeping children safe. Delphi techniques have previously informed consensus and development of nursing practice standards (Grant et al., 2017; Mannix, 2011). A Delphi study has up to four rounds, depending upon response stability and achievement of a predetermined level of consensus (Grime and Wright, 2016; Keeney et al., 2011). For this study, the agreement level was set at 80% with a maximum of three rounds (Keeney et al., 2011).
Development of statements for Round One of the Delphi process
Statements for Round One were developed through content analysis (Elo and Kyngas, 2008; Graneheim et al., 2017) of sources, including professional frameworks for nurses and midwives in Australia. These were standards of practice for all nurses or midwives published by the NMBA (2016, 2018) and specialist practice standards that further guide nurses or midwives working with children (Australian College of Children & Young People’s Nurses, 2016; Australian Nursing and Midwifery Federation, 2019; Grant et al., 2017; Australian College of Neonatal Nurses, 2019). Other sources informing Round One were key findings from existing literature reviews (Lines et al., 2017; Lines et al., 2018; Lines et al., 2023 and authors’ previous work (Lines et al., 2020a; Lines et al., 2020b; Lines et al., 2019; Lines et al., 2021). These nursing and midwifery practice frameworks and key themes from existing literature were independently inductively coded in NVivo (version 12, QSR International) by two researchers (LL & TK) and discrepancies resolved through discussion. Next, authors deductively organised these codes into clusters that aligned with headings and structure of the Registered nurse standards for practice (NMBA, 2016). Final statements were reviewed by the research team for content and clarity before exporting into Qualtrics (2021) survey platform.
Registered nurse standards do not guide midwifery practice, but the Midwife standards for practice (NMBA, 2018) uses a similar structure. These clusters (standards) are: 1) ‘Thinks critically and analyses nursing practice’, 2) ‘engages in therapeutic and professional relationships’, 3) ‘maintains the capability for practice’, 4) ‘comprehensively conducts assessments’, 5) ‘develops a plan for nursing practice’, ‘provides safe, appropriate and responsive quality nursing practice’ and 7) ‘evaluates outcomes to inform nursing practice’ (NMBA, 2016).
Delphi survey
Round One of the Delphi survey was piloted with ten nurses and midwives prior to distribution. Minor changes to question flow and wording were made in accordance with their feedback. See Supplementary Online File One for final version of the online Delphi survey.
Experts were invited to complete the online Delphi survey in Round One. Experts were defined as nurses and midwives working with children in Australia. Recruitment of experts involved advertisements through professional nursing and midwifery organisations, social media promotion both unpaid (LinkedIn, Twitter) and paid (Facebook) and snowball sampling. Participants were provided with study information before opening the survey, and completion of the survey was an indicator of consent. The survey firstly requested demographic data about participants’ professional characteristics and then asked participants to rank each statement on a five-point (1–5) Likert scale. Specifically, participants were asked to ‘rank how important you believe each item is for nurses and/or midwives working to safeguard children your practice setting’. A score of five meant that statement was considered ‘extremely important’ and score of one meant the statement was considered ‘not at all important’.
Participants were asked to provide feedback on depth, breadth and relevance of the statements for their context of practice after each of the seven question clusters. Participants were then invited to supply an email address so they could be invited to participate in subsequent rounds. Round One opened in April 2021 and remained active for 3 months; Round Two commenced in August 2021 and remained active for 5 weeks. Participants were notified about Round Two through their nominated email address, and weekly reminders were sent to non-respondents for a period of 4 weeks.
Ethical approval
The study was approved by Flinders University Human Research Low Risk Panel (Project ID: 2939).
Data management and analysis
Data were exported from Qualtrics (2021) to other software for processing and analysis. Quantitative data were exported to SPSS (ver. 25.0, SPSS Inc, USA) while qualitative data from participant comments were copied and pasted in a table next to the corresponding statement. Descriptive statistics of frequencies, percentage agreement (agree or strongly agree), mean and median were used to analyse and present data on participant demographics and level of agreement (refer to Supplementary Online File Two). Participant feedbacks about each statement were reviewed by the research team and proposed changes to statements were agreed by discussion. A summary of changes made in Rounds One and Two are provided in Supplementary Online File Two.
Results
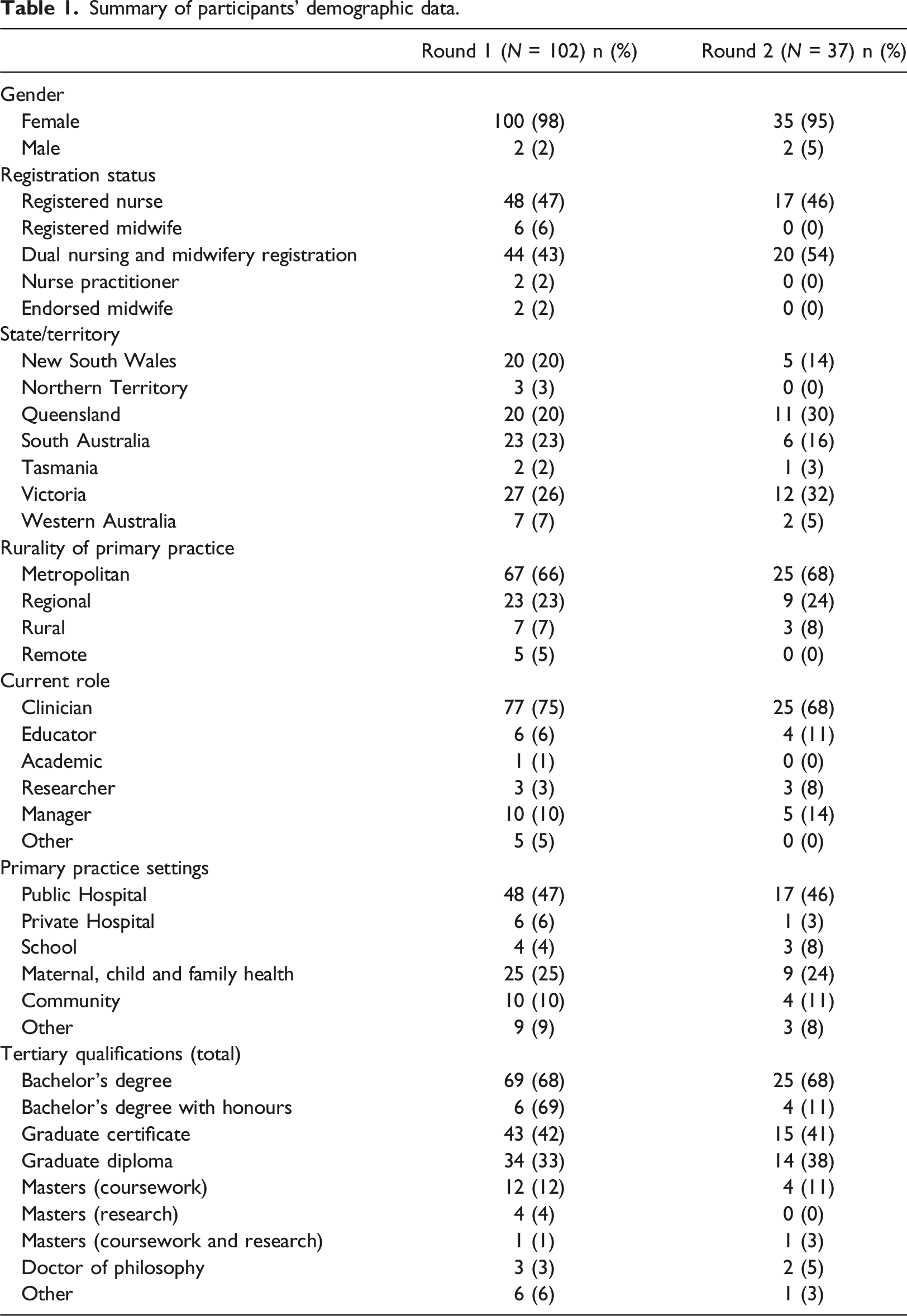
Summary of participants’ demographic data.
Final version of statements developed in this Delphi study.
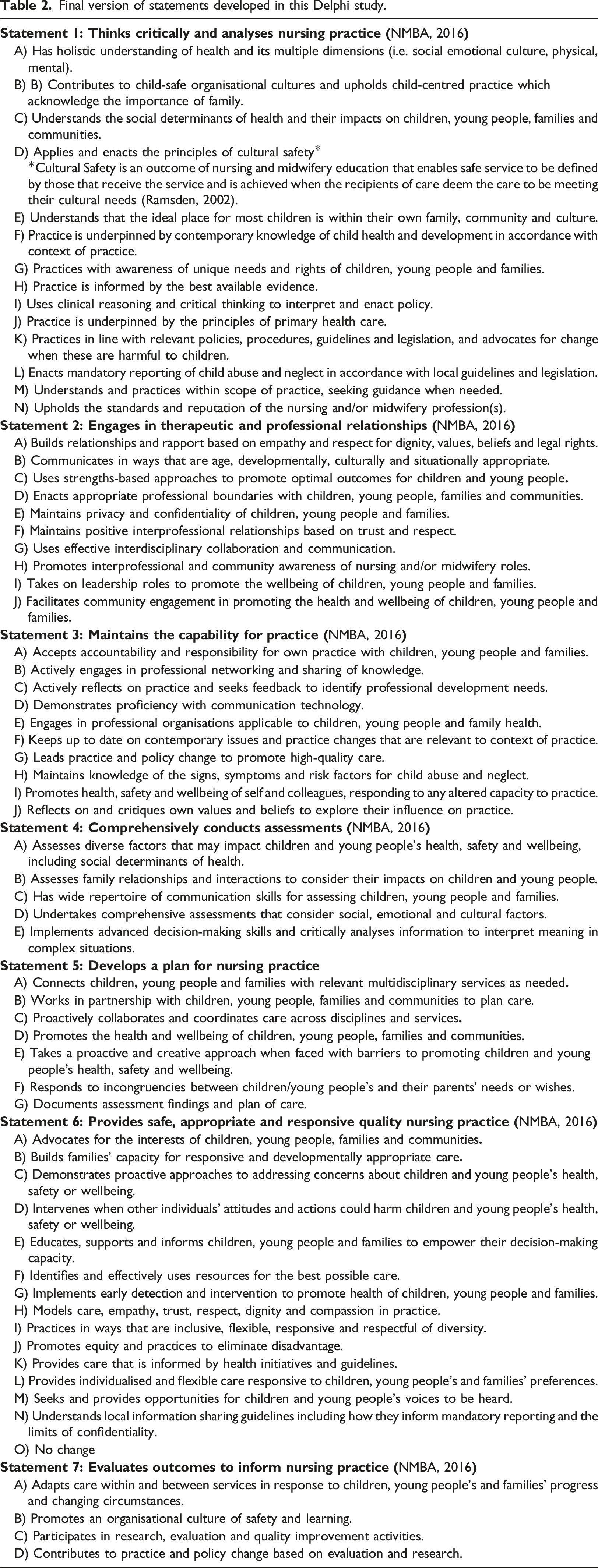
Thirteen statements were changed after Round One, but only an additional three were amended following Round Two. Supplementary Online File Two presents a summary of changes made in each round to the statements within the seven clusters. Changes were made to statements within five of the seven clusters, and clusters four and five were not amended in either round due to absence of participant feedback indicating need for change. Participants provided feedback about 45 of the 64 statements in Round One, and the research team subsequently amended 13 statements. Not all statements were amended in response to feedback because some feedback was general or supportive rather than advocating for change. An example of change arising from participant feedback was statement 1E ‘Understands that the ideal place for children is within their own family, community and culture’. Statement 1E generated feedback (n = 4) that families and communities can at times cause harm to children. This statement was subsequently amended for Round Two to include the qualifier of ‘most’ children. A full summary of changes made after each round can be found in Supplementary Online File Three.
Clarity and wording of each statement were discussed after each round. In doing so, some statements (n = 1 Round One, n = 2 Round Two) were modified for clarity. For example, ‘Implements early detection and intervention to promote health of children, young people and families’ was amended to ‘
Discussion
This study used a Delphi methodology to develop consensus about the nature and scope of Australian nursing and midwifery practices in keeping children safe from abuse and neglect. Overall, this study identified that participating Australian nurses and midwives working with children agreed safeguarding is an important component of their practice. It is possible findings do not reflect perspectives of non-participating nurses and midwives because individuals with a special interest in safeguarding children may have been more likely to participate. However, participants were from diverse professional backgrounds and contexts, meaning findings are likely to be generalisable to other nurses and midwives in Australian child-focussed settings. These findings build our understanding of the comprehensive nature of nurses’ and midwives’ existing practices in keeping children safe. Furthermore, findings can inform ongoing discussions about strategic planning for effective education, support and evaluation of nursing and midwifery practice into the future.
This study provides strong evidence for core roles of nurses and midwives in a public health response to child abuse and neglect as outlined by the National Framework for Protecting Australia’s Children (Commonwealth of Australia, 2021). Final statements incorporated nurses’ and midwives’ practices across the spectrum of public health responses for child abuse and neglect, including universal services, targeted intervention through to intervention for suspected cases of abuse. High levels of consensus were demonstrated across both rounds, indicating that experts agree that nurses and midwives have a core role in preventing and responding to child abuse and neglect. In comparison to other similar Delphi studies seeking consensus on an area of nursing practice, this study had more participants. We received 102 responses in Round One, and 37 in Round Two, compared with significantly fewer participants in similar Delphi studies (Round One n = 11–21, Round Two n = 11–22) (see, for example, Al-Motlaq et al., 2019; Benito et al., 2017; Mannix, 2011). Furthermore, participants were from a range of geographical, professional and practice contexts meaning findings are likely to reflect broad views of Australian nurses and midwives working with children and families.
There is currently no single set of standards in Australia representing nurses’ and midwives’ work in keeping children safe to inform their roles in a public health response to child abuse and neglect (Lines et al., 2022). Without existing guidelines, these findings represent consensus of nurses’ and midwives’ perspectives and can inform ongoing discussions about formal standards for nurses’ and midwives’ public health approach to keeping children safe. Formalised standards would firstly increase multidisciplinary awareness of nursing and midwifery roles to underpin high-quality, coordinated multidisciplinary care for children and families (Grant et al., 2018; Russ et al., 2022). Furthermore, standards for practice can inform education and professional development to enhance nursing and midwifery expertise in keeping children safe in all practice contexts. Standards for practice also facilitate benchmarking of existing practice to support development of evidence-based ways to engage this highly educated and skilled existing workforce to improve outcomes for all children.
Consideration needs to be given to philosophical orientations to care when developing standards for nurses’ and midwives’ public health response to child abuse. For example, there are variations between nursing and midwifery approaches to care, and further differences between generalist nurses and nurses who specialise in care for children or families. Most notably, there is varied language across nursing and midwifery guidelines about the individual or group who is the nurse or midwife’s focus of care. For example, the International Council of Nurses’ Code of ethics (2021) expects all nurses to enact a ‘person-centred’ approach, while the International Council of Midwives’ (2014) Code of ethics emphasises women-centred partnerships. Yet although both nurses and midwives work with children and families, neither code explicitly acknowledges potential conflicts between adults’ and children’s interests.
Australian specialist practice standards for nurses working with children and young people emphasise keeping children and young people at the centre of care (Australian Nursing and Midwifery Federation, 2019; Australian College of Children & Young People’s Nurses, 2016). A focus on children and young people as the centre of care can raise tensions for nurses and midwives when their clients are both the child and the parent. These tensions are acknowledged in the specialist National standards of practice for maternal, child & family health nurses which outline the need for both ‘person-centred’ and ‘family-centred’ approaches (Grant et al., 2017). These specialist standards go on to highlight that families’ attitudes and behaviours may be harmful to children and require the nurse/midwife to advocate for the child. Tensions arise when nurses and midwives work with families to advance the interests of children (Uniacke et al., 2018), and this must be acknowledged when developing shared visions for a public health response to keeping children safe. Developing effective ways of working together should focus on similarities and synthesise strengths of different viewpoints towards ‘pragmatic, purposeful ends’ (Grant et al., 2018). This means drawing upon nursing and midwifery expertise to explore and unite different philosophies to negotiate complexities of keeping children safe.
This study developed consensus on a set of statements that could form the basis for standards of practice for nurses’ and midwives’ roles in a public health response to keeping children safe. However, these statements reflect current practice, and do not necessarily represent a final set of standards to be uncritically used to guide future nursing and midwifery practice. Despite existing international efforts, child abuse, neglect and social inequities remain for children, especially for First Nations children (UNICEF, 2016; United Nations, 2018). Instead of existing approaches that respond to individual cases of abuse and neglect, a public health approach addressing social and economic inequities at the population level is needed (Higgins et al., 2019; World Health Organization, 2020a, 2020b). Adopting such an approach requires widespread philosophical, political and economic change to restructure and reframe the ways nurses and midwives work (Klevens and Metzler, 2019).
There is urgent need to critically discuss and develop nurses’ and midwives’ roles in keeping children safe within the context of broader health, social and economic changes. Although nurses’ and midwives’ capacity to enact a public health approach is inextricably linked to the systems in which they work, there are also implications for ongoing development of nursing and midwifery practice. For example, a successful public health response requires sound professional knowledge of social determinants of health, strength-based approaches and reasons why child abuse occurs (Lonne et al., 2020). Furthermore, ongoing experiences of racism and social inequities by First Nations Peoples means nurses’ and midwives’ capacity to enact cultural safety will be core to engaging with these populations (Lonne et al., 2021). Specialist nursing and midwifery expertise is needed to enact a public health approach, and will require appropriately tailored preservice preparation and ongoing education and development (Jones et al., 2021).
Limitations
We aimed for broad participation in this study, but it is possible that perspectives are not broadly representative because individuals interested in working with children are more likely to self-select for participation. Furthermore, results may not be generalisable outside the Australian context of a high-income country with past and ongoing colonising practices that oppress First Nations Peoples. Another limitation was an absence of engagement with stakeholders including children, young people, families and Australian First Nations Peoples. However, these findings are just the start of ongoing conversations about the best ways to mobilise nurses and midwives to make a difference for Australian children. Future development and planning for nursing and midwifery practice in a public health approach to keeping children safe will require engagement with these key groups. Consultation and partnership with Australian First Nations peoples will be especially important to decolonise practices and promote cultural safety in all aspects of nurses’ and midwives’ work with children (Mackean et al., 2019).
Implications for practice
Greater understanding of nurses’ and midwives’ complex roles a public health approach to preventing and responding to child abuse and neglect is needed in Australia and internationally. The implication for nurses and midwives is how to support evidence-informed professional practice development as systems pivot towards prevention and early intervention for child abuse and neglect.
Conclusion
The aim of this modified Delphi study was to build consensus on the nature and scope of Australian nursing and midwifery practice in safeguarding children. Findings build our knowledge of the poorly understood but crucial role of nurses and midwives in preventing and addressing child abuse and neglect. Furthermore, findings support that nurses’ and midwives’ practice demonstrates a public health response to child abuse by incorporating prevention, early intervention and responses to abuse and neglect. Findings provide a starting point for ongoing research and debate about nursing and midwifery practice standards for safeguarding children, which can inform preparation, education, support and resourcing for nurses’ and midwives’ work. Further research about future development of nurses’ and midwives’ roles in a public health response to child abuse is essential because existing systems have not reduced the social inequities contributing to abuse. In addition, discussions about future directions for nursing and midwifery professions in safeguarding children must partner with key stakeholders, including children and First Nations peoples.
Supplemental Material
Supplemental material - Nurses’ and midwives’ contributions to a public health response to keeping children safe from abuse and neglect – a Delphi study
Supplemental material for Nurses’ and midwives’ contributions to a public health response to keeping children safe from abuse and neglect – a Delphi study by Lauren E Lines, Tracy Alexis Kakyo, Alison Hutton and Julian Maree Grant in Journal of Child Health Care
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by a Flinders Foundation Health Seed Grant 2020
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.