
Abstract
Objective:
The objective of this study was to identify factors associated with nurses’ and midwives’ skills in performing neonatal resuscitation.
Method:
Health facility-based analytical cross-sectional study design was employed from January 2021 to April 2021 among 340 nurses and midwives selected by multistage random sampling technique. An observation checklist was used to collect data. Data were coded and entered into SPSS version 20 for analysis. Bivariate and multivariate logistic regression was used to assess factors associated with nurse/midwives’ skills in neonatal resuscitation.
Results:
Among 340 nurses and midwives, 141 (41%) had adequate skills in neonatal resuscitation. After adjusting for confounders, factors associated with adequate skills were; age of the midwives (20–34 (adjusted odds ratio = 0.082, p < 0.008) and 35–49 (adjusted odds ratio = 0.087, p < 0.010)); work experience (worked 4–6 (adjusted odds ratio = 2.905, p < 0.003) and > 10 years and above (adjusted odds ratio = 12.825, p < 0.000)); district hospitals (adjusted odds ratio = 1.544, p = 0.032); distance from place of residence (6–10 km (adjusted odds ratio = 0.090, p < 0.001) and > 16 km (adjusted odds ratio = 0.049, p < 0.001)); number of midwives per shift, ⩾ 4 (adjusted odds ratio = 2.396, p = 0.012) and number of deliveries per day (6–10 (adjusted odds ratio = 1.385, p < 0.031), 11–20 (adjusted odds ratio = 2.693, p < 0.016) and > 20 delivery per day (adjusted odds ratio = 6.007, p < 0.001).
Conclusion:
Less than half of the observed nurses and midwives had adequate skills in neonatal resuscitation. Nurses and midwives who were younger, less experienced (<4 years of work experience), and work in small, lower volume settings with fewer colleagues and limited births (dispensaries, fewer than four nurses and midwives per shift, less than six deliveries per day) were less likely to have adequate skills in neonatal resuscitation. Knowledge gained from this study may provide future research related to a cost-effective strategy to empower nurses and midwives in neonatal resuscitation.
Introduction
Neonatal resuscitation includes a set of interventions at the time of birth to support the establishment of breathing and circulation. 1 Positive pressure ventilation is the most critical intervention to initiate and sustain respiration among neonates needing resuscitation at the time of birth. The Golden Minute® is a key concept used in the Helping Babies Breath® (HBB) program, which highlights the importance of the first minute after birth, by which time a neonate should be breathing or receiving positive pressure ventilation with an appropriately sized bag and mask. 2 The inability of the neonate to initiate and sustain respiration within the first minute after birth may result in the condition known as birth asphyxia. Birth asphyxia is defined by the World Health Organization (WHO) as the failure of a neonate to initiate and sustain breathing at birth. 3 Delays in assisting the non-breathing neonate to initiate breathing may increase the risk of hypoxia, increase the need for assisted ventilation, and contribute to neonatal morbidity and mortality. 4
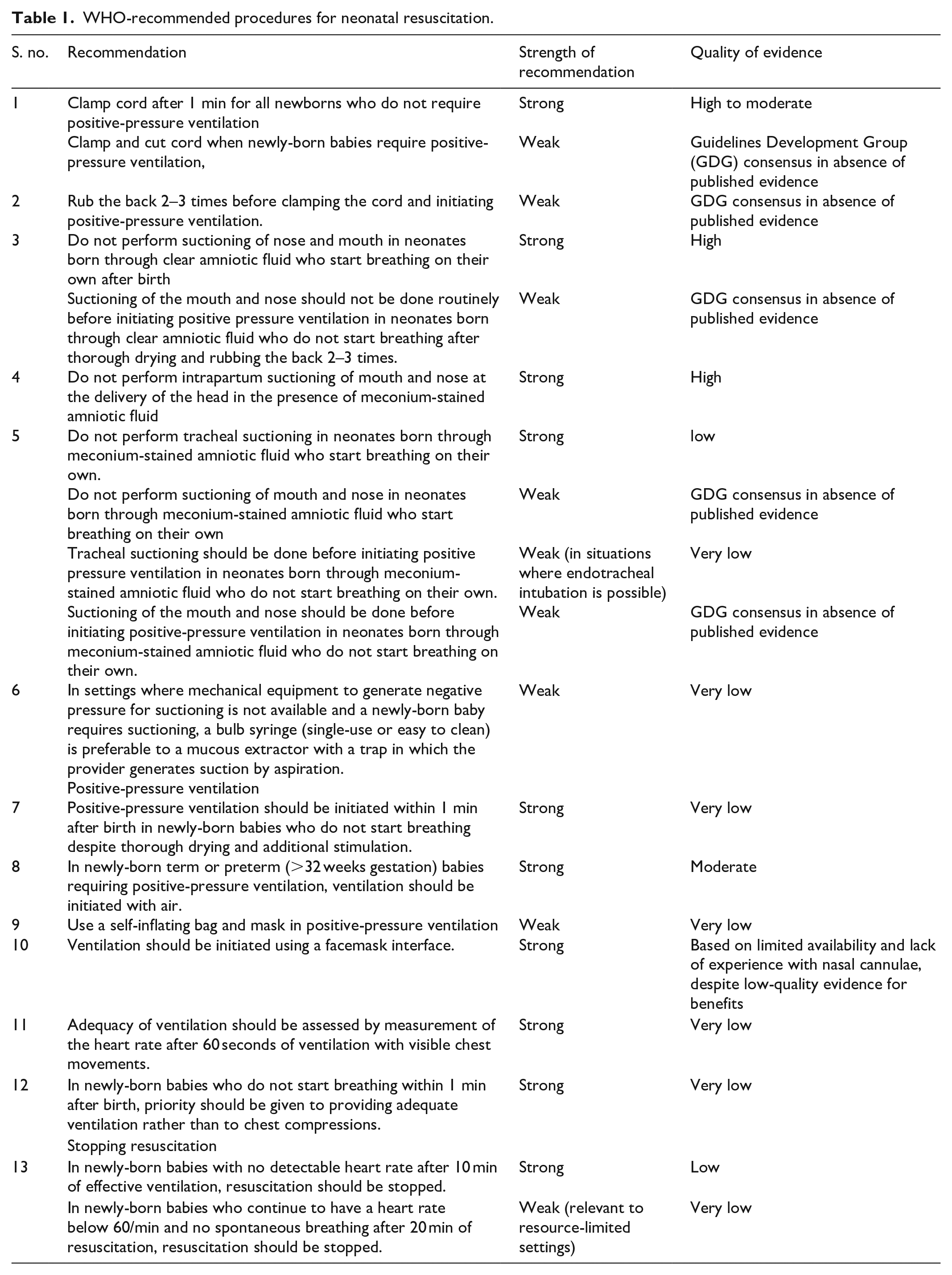
Evidence from previous studies demonstrates that facility-based basic neonatal resuscitation can prevent up to 30% of intrapartum-related neonatal deaths. 4 The WHO has recommended the neonatal resuscitation process as shown in Table 1. 5
WHO-recommended procedures for neonatal resuscitation.
Performing effective and timely neonatal resuscitation has been demonstrated to prevent neonatal morbidity and mortality. In Tanzania, most births are attended by nurses and midwives who are providing care for both the birthing woman and her neonate. In some higher-level health facilities, the team may include additional support such as a pediatrician may arrive to assist. More commonly, such specialized support is not readily available. In more developed nations, frontline nurses, midwives, physicians, and respiratory therapists are all trained and certified in neonatal resuscitation. In settings with more resources, a neonatal resuscitation team is summoned urgently to the bedside and may include a neonatologist or pediatrician and a specialized Neonatal Intensive Care Unit (NICU) registered nurse (RN). In Tanzania, nurses and midwives attend the majority of the deliveries and provide subsequent neonatal resuscitation at delivery if required. Adequate competence among nurses and midwives and the ability to follow the basic standard steps in neonatal resuscitation could lead to a decrease in neonatal morbidity and mortality rates. 6
Research has shown that approximately 75% of neonatal deaths arise in the Southeast-Asian and sub-Saharan African (SSA) countries.6,7 According to WHO, Sub-Saharan countries had the highest neonatal mortality rate in 2018 with 28 deaths per thousand live births. 8 Tanzania is among the sub-Saharan countries with high neonatal mortality. The neonatal mortality rate in Tanzania has declined from 40 deaths per 1,000 live births in 1995 to 28.97 deaths per 1000 live-birth in 2020. 9
Literature reviews have shown that, in SSA, neonatal mortality is due to complex factors, including neonatal, maternal, and healthcare-related factors as well as the long distances and delays in seeking care. 10 Neonatal factors including neonatal infection, congenital malformation, and preterm birth are cited as the leading causes of neonatal mortality. 10 Maternal factors such as obstructed labor, eclampsia, placental abruption, infection (malaria, HIV), and anemia all affect the health of pregnant women and neonates and contribute to the high neonatal mortality in SSA.11,12 The delay in deciding to seek health care, delay in accessing mode of transport, the long distances to facilities, and a lack of knowledge and training of frontline health workers also contribute to the increased number of neonatal mortalities in SSA. The leading causes of early neonatal deaths (within the first week) are severe infections, preterm births, and asphyxia. 13
In many parts of SSA, studies have shown health care providers have poor competence in performing neonatal resuscitation even if they do attempt to perform resuscitation.13–15 Furthermore, studies have shown that a lack of skills in neonatal resuscitation is common among low and middle-income countries with the uppermost percentage in sub-Saharan countries. 6 Research in Nigeria and Zambia has demonstrated that asphyxia contributed to a larger percentage of neonatal mortality. 14 Despite the severity of asphyxia on neonatal death and morbidities, the capability to manage neonatal resuscitation has continued to be a substantial challenge in developing countries where neonates’ death arise due to poor resuscitation techniques. 14
The HBB pilot program was launched in Tanzania in 2009 and subsequently demonstrated a 47% reduction in neonatal deaths. 15 Despite deliberate efforts to increase nurses’ competence in neonatal resuscitation through on-the-job training such as HBB training, the number of neonates losing their lives due to birth asphyxia remains unacceptably high.14,16 This signifies that the skills of nurses midwives in neonatal resuscitation likely remain an ongoing challenge. Therefore, this study aimed to assess the factors associated with nurses’ and midwives’ skills in neonatal resuscitation.
Operational definitions
These are three main educational training levels of the professional nurses and midwives included in this study; certificate level, diploma level, bachelor’s degree level, and master’s degree level. They were all trained using the English language as a medium of instruction. In this study, health facilities referred to a range of health settings where health care is provided. These settings included: The Regional Hospital, District Hospital, Health Centers, and Dispensaries. Dispensaries and Health Centers are the primary levels of health facilities in Dodoma Region, Tanzania. Neonatal resuscitation education models (NeoNatalies®) are mannequins that are used globally in the training of neonatal resuscitation HBB program.
Method
Study setting and design
A health facility-based analytical cross-section study was performed in Dodoma Region, Tanzania from January 2021 to April 2021. According to the 2012 National Census, the region had a population of 2,083,588. 17 The Dodoma Region has an annual growth rate of 2.1% which was recognized as the highest one in the country. The region has seven districts which are Dodoma Urban, Bahi, Chamwino, Kondoa, Mpwapwa, Chemba, and Kongwa Districts (Figure 1). The Region has a total of 7 hospitals (5 public; 2 private), 32 Health Centers (26 public; 6 private), and 269 dispensaries. This study was conducted in 32 health facilities that were recruited using probability sampling. The final sample was comprised of 4 hospitals, 12 health centers, and 16 dispensaries (Figure 1).
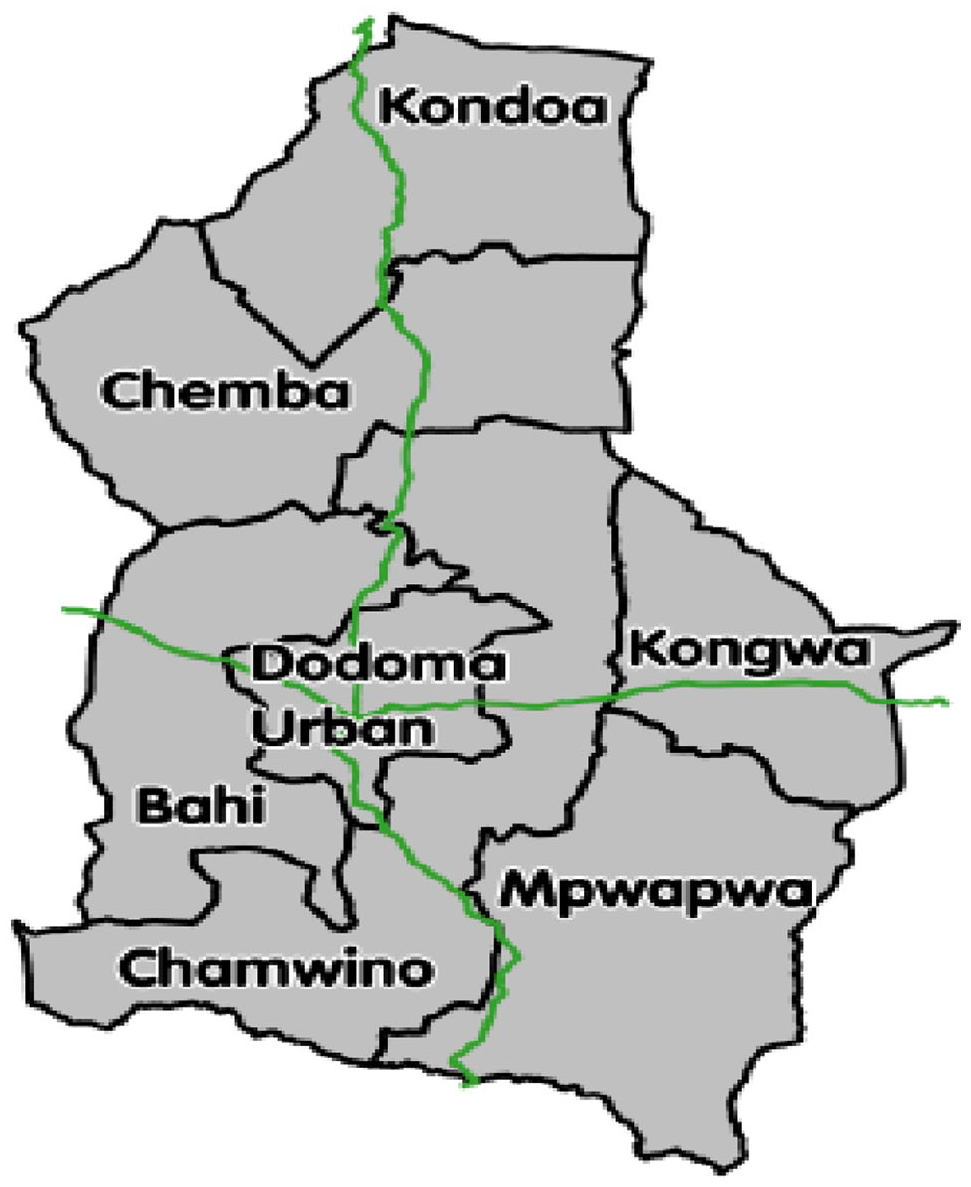
Dodoma region map.
Study population
The target population in this study was nurses and midwives working in the neonatal units and labor wards at the time of data collection.
Inclusion criteria
The study included all nurses and midwives who were working in the labor ward and neonatal units.
Exclusion criteria
The study excluded nurses and midwives who were sick and unable to participate in the study.
Sample size estimation and sampling procedure
Sample size estimation
The sample was obtained by using the single population proportion formula with the assumption of proportion (p) for nurses and midwives who were working in the labor ward and neonatal units and had performed resuscitation p = 67%. 18
where, z = standard deviation at 95% level of confidence, ɛ = margin of error (5%), p = proportion (0%) (p = 0.67), and q = 1 − p, that is (q = 0.5).
Thus, n = 1.962 × 0.67(1–0.67)/0.052 = 340.
Therefore, the minimum sample size of 340 nurses and midwives was recruited to participate in this study.
Sampling procedure
A multi-stage sampling method was applied to randomly select the district and its hospitals having a labor ward and neonatal unit. In the first stage, the Regional Hospital was purposively included in the study because it is a referral center of the region. The second stage was the selection of 4 district hospitals, 16 health centers, and 8 dispensaries. District hospitals were selected conveniently because each district has only one district hospital, but health centers and dispensaries were selected using simple random sampling from each district. The third stage was the selection of nurses and midwives. The Regional Hospital nurses and midwives contributed 30% to the total sample, 30% were from district hospitals, 20% of the total sample were from health centers, and 20% were from dispensaries. A systematic sampling technique was used to select the midwives from each visited health facility.
Data collection tools, methods, and procedures
Data collection tools
An observation checklist with 13 steps of basic neonatal resuscitation was used to assess nurse/midwives’ skills in neonatal resuscitation. The observational checklist was prepared in English. It was adopted from the WHO guideline for neonatal resuscitation skills. 19 The adopted checklist was piloted among 10% of the study population. Study respondents were recruited from unselected health facilities. The study was conducted by two research assistants trained in both the use of the checklist and standard HBB neonatal resuscitation skills. A simulated neonatal resuscitation scenario environment was prepared to utilize HBB® mannikins and participants were required to perform neonatal resuscitation. An observation checklist was used to assess nurses’ and midwives’ skills in neonatal resuscitation.
Research variables
Dependent variable
The dependent variable was nurses’ and midwives’ adequate skills in neonatal resuscitation. This was measured by using an observation checklist with 13 questions that were adopted from previous researchers. 5 The total score a respondent could get was 13 points which was equivalent to 100%. Those who scored less than 50% were termed as having inadequate skills in neonatal resuscitation and were given 0 and those who scored correctly more than 50% were regarded as having adequate skills in neonatal resuscitation and were given 1.
Independent variables
The independent variables were the nurses’ and midwives’ social demographic characteristics and facility characteristics. Socio-demographic characteristics were individual characteristics such as age, sex, level of professional training, and economic status. Facility characteristics were factors such as distance to the health facility, number of nurses per shift, working shift, birth volume, and level of health facility. All these variables were measured using a nominal scale.
Statistical analysis
The collected data were coded and entered into SPSS Software Version 20 for statistical analysis. Social demographic characteristics, knowledge, attitude, and practice were analyzed by descriptive analysis and presented by frequency and percentages. Chi-square was used to measure the relationship between independent and dependent variables. The level of significance was considered at the p-value < 0.05. Inferential analysis that includes binary logistic regression analysis was employed, and 95% confidence interval was used to measure the strength of the association.
Ethical consideration
Ethical clearance was obtained from the University of Dodoma. Permission to conduct the study was sought from the Regional Administrative Secretary of the Dodoma Region and all District Executive Directors of the four districts which were selected. Informed oral and written consent was obtained from nurses and midwives who were eligible for the study. Nurses and midwives were ensured of confidentiality and privacy. Nurses and midwives were informed of their freedom for giving their responses and the opportunity to withdraw from participation at any time. Unique identification numbers instead of names were used to identify study participants. Also, data from the field were secured for authorized personnel only.
Results
Socio-demographic characteristics
This study comprised 340 participants with a response rate of 100%. Findings showed that most of the participants 241 (70.9%) were between 20 and 34 years with an average mean age of 31.20 ± 8.568. The majority 224 (65.9%), were female, half of the 184 (54.1%), were single, less than half 143 (42.1%) had working experience less than 4 years, more than half 207 (60.9%) were nurses and midwives with diploma level, about 195 (57.4%) had 5 years working experience (Table 2).
Proportion distributional of nurses/midwife in Dodoma region (N = 340).

Nurses’ and midwives’ skills in neonatal resuscitation
Only 81(23.8%) were able to prepare the area for resuscitation (clean hands, prepare an area for ventilation and check equipment and secure the area, and set time) correctly. The majority 236 (69.4%) were able to dry thoroughly and remove wet cloth on a baby and put dry, clean, and soft clothes. Only a total of 125(36.8%) nurses and midwives managed to show or say the baby is not crying and call for help. Approximately 70% of nurses and midwives dried and stimulated the baby and cleared the baby’s airway while positioning the head correctly, and keeping the baby covered and warm. A majority (66%) were able to appropriately begin positive pressure ventilation, but only 60% of the participants were able to properly ventilate at the appropriate rate (Table 3).
Description of nurses and midwives skills on neonatal resuscitation.

When the total score was computed, results showed that 199 (59%) of observed nurses and midwives had inadequate skills in neonatal resuscitation while only 141(41%) had adequate skills in neonatal resuscitation (Figure 2).

Nurses’ and midwives’ skills on neonatal resuscitation (N = 340).
Relationship between nurses’ and midwives’ characteristics and skills in neonatal resuscitation
The variables which showed a significant relationship between nurses’ and midwives’ characteristics and neonatal resuscitation skills were gender [male had adequate skills [n = 60(51.7%), χ²:7.626, p = 0.006] worked more than 7–9 years had adequate skills [n = 22(56.4%), χ²:19.341, p < 0.001], together with the participant who had diploma level had adequate skills also [n = 82(42.1%), χ²:14.191, p = 0.007], those who were working on the regional hospital had adequate skills [n = 70(50%), χ²:13.826, p = 0.003] compared to those who worked in other facilities, those who were living near the hospital less than 5 km [n = 115(48.1%), χ²:20.920, p < 0.001] had shown adequate skills compared to others who live far away and also the number of nurses in each shift showed that 4–5 nurses and midwives per shift showed they had adequate skills [n = 44(57.9%), χ²:21.622, p < 0.001], this relationship was significant. Other independent variables did not show a significant relationship with neonatal resuscitation skills (Table 4).
Chi-square test for the relationship between nurses’ and midwives’ demographic characteristics and neonatal resuscitation skills (N = 340).

Factors associated with nurse/midwives’ neonatal resuscitation skills
Concerning age groups, it was observed that those respondents who were aged 20–34 (adjusted odds ratio (AOR) = O.082, p = 0.008) and 35–49, (AOR = 0.087, p = 0.010) were significantly less likely to have adequate skills as compared to respondents aged 50 and above. For working experience, it was observed that those respondents who worked 4–6 (AOR = 2.905, p = 0.003) and 10 > years and above (AOR = 12.825, p < 0.001) were significantly more likely to have adequate skills as compared to respondents who worked <4 years. At the facility level, it was noted that respondents who were working at the district level were significantly more likely to have adequate skills (AOR = 1.544, p = 0.032) as compared to those who were working at the dispensary level. Concerning distance from the place of residence, it was observed that those respondents that lived in 6–10 km (AOR = 0.090, p < 0.001) and > 16 km (AOR = 0.049, p < 0.001) were significantly less likely to have adequate skills in neonatal resuscitation as compared with respondents lived near the hospital 1–5 km. About nurses/midwives entering each shift it was noted that respondents who were working 4–5 in each shift were significantly more likely to have adequate skills as compared to those who were working 2–3 in each shift (AOR = 2.396, p = 0.012). For the number of deliveries per day, it was observed that those respondents who were conducting 6–10 (AOR = 1.385, p = 0.031), 11–20 (AOR = 2.693, p = 0.016), and >20 delivery per day (AOR = 6.007, p < 0.001) were significantly more likely to have adequate skills in neonatal resuscitation as compared with respondents who perform 1–5 delivery per day (Table 5).
Binary logistic analysis for factors associated with nurse/midwives’ neonatal resuscitation skills.

COR: crude odds ratio; CI: confidence interval; AOR: adjusted odds ratio.
Discussion
The study found that less than half of 141 (41%) observed nurses and midwives had adequate skills in neonatal resuscitation. The majority had inadequate skills in neonatal resuscitation. Among the observed nurses and midwives more than half skipped or perform incorrectly the following steps in neonatal resuscitation as per WHO guidelines: to show or say the baby is not crying, look for chest movement, continue with ventilation until there was chest movement, properly squeeze the resuscitation bag, evaluate breathing and heart rate, continue ventilation until the breathing and heart rate were normal and stop ventilation, monitor the neonate and communicate with mother. This is a worrisome situation as nurses and midwives attend most births at the facility level in Dodoma, Tanzania. As such, they are responsible for providing care for mothers and neonates at the time of birth and well-performed neonatal resuscitation, which has the potential to save lives and decrease or reduce complications of birth asphyxia. 11 A similar study done in Ethiopia by Sintayehu et al, 20 reported even lower proportions of 11.5% of nurses’ and midwives’ who have adequate skills in neonatal resuscitation, demonstrating a shared challenge among nurses and midwives in other low-resource settings.
Factors associated with nurses’ and midwives’ adequate skills in neonatal resuscitation were the age of nurses and midwives, working experience, working in a hospital setting, living nearby to the health facility (1–5 km), working with more than three colleagues nurses and midwives per shift and assisting more than five deliveries per shift.
Young nurses and midwives were less likely to have adequate skills in neonatal resuscitation when compared to those aged 50 years and above. This could be due to the advance in age going in hand with working experience. The study also showed that nurses and midwives with more than 3 years of working experience were more likely to have adequate skills in neonatal resuscitation if compared to those with less working experience Those with more than 3 years of working experience may have benefited from on-job training. A similar study done in Tanzania has reported similar finding. 21 The finding shows the necessity to prepare and conduct induction courses on neonatal resuscitation for newly employed nurses and midwives in Tanzania. It is evidenced that on-the-job training has a significant impact on the improvement of neonatal resuscitation. 22
The study also found that nurses and midwives who were working in district hospitals were significantly almost twice more likely to have adequate skills in neonatal resuscitation compared to those working in dispensaries. Those from the regional hospital were almost 3 times more likely to have adequate skills when compared with those from the dispensaries but the association was not statistically significant. This could be due to nurses and midwives working in the regional hospital having the opportunity for training. A previous study exploring factors influencing the practice of neonatal resuscitation with bags and mask in Ethiopia reported that those working in hospitals were 3 times more likely to have the required skills compared with those working in lower-level health facilities. 23
The study also found that the nurses and midwives who were living near health facilities were more likely to have adequate skills in neonatal resuscitation compared with those living more than 5 km from health facilities. The job demand created by the shortage of nurses/midwives in health facilities in Tanzania can be minimized by facilitating the accommodation of nurses and midwives near health facilities. 24 Living more than 5 km from the working station could have added the burden and lowered their morale for work.
In addition, it was noted that respondents who were working with at least four other nurses and midwives in each shift were significantly more likely to have adequate skills in resuscitation compared with those who are working with only two to three colleagues in each shift. The adequate staffing of nurses and midwives per shift could be an important proctor for the enhanced provision of comprehensive care. When nurses and midwives are overwhelmed by the nurse-to-client ratios, this hinders their ability to provide the required comprehensive care. 25 This may lead to the creation of shortcuts in care to meet the demand of work. As a result, when tasked to resuscitate in a simulation room, nurses and midwives have forgotten the key principles and end up missing the important steps. Similarly, this study uncovered a clear need for health policy and health education leaders to strengthen both pre-service and in-service education and training to support improved skills in neonatal resuscitation among nurses and midwives in Dodoma, Tanzania. Previous studies demonstrate that in-service training enhances the retention of knowledge and skills. 26
For the number of deliveries per day, it was observed that those respondents who were conducting > 6 delivery per day were significantly more likely to have adequate skills in neonatal resuscitation compared with respondents who make < 6 delivery per day. This could be because facilities with many deliveries per day are the higher level facilities, health facilities, and hospitals. These nurses and midwives have more opportunities to practice compared to nurses and midwives who work in lower-level facilities. Higher-level facilities may also have more training opportunities or access to better equipment. The study recommends a deliberate effort to empower nurses and midwives in lower-level facilities with the key knowledge, skills, and supplies for neonatal resuscitation. Regular in-service training is a key strategy for enhanced skills retention.
The study was not without limitation, it used an observation checklist which could have an observer bias. This was minimized by training the research assistants on the key aspects of the observation, but still a possible factor. The study also was a cross-sectional study design that lacks the causal effect relationship. However, through regression analysis, the confounders were controlled, and the reported factors set the ground for an interventional study. The study also confined itself to the assessment of the skills of nurses and midwives in neonatal resuscitation without assessing the facility work environment, which is a key factor in neonatal resuscitation skills. The authors recommend a further study to assess the facility-based environment factors in terms of the availability of equipment for resuscitation of neonates.
Conclusion
Less than half of the observed nurses and midwives had adequate skills in neonatal resuscitation in this study. Nurses and midwives with at least 4 years of work experience, working in sites with more births and with at least four colleagues per shift—were more likely to have adequate skills in neonatal resuscitation. Among the nurses and midwives sampled, there are many knowledgeable and skilled birth attendants. However, this study demonstrates a dire need for action and also uncovers numerous opportunities to enhance the knowledge and skills of all frontline nurses and midwives in this setting and empower them with the necessary training, skills, and supplies for neonatal resuscitation.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221100991 – Supplemental material for Identifying factors associated with neonatal resuscitation skills among nurses and midwives in Tanzania, sub-Saharan Africa
Supplemental material, sj-docx-1-smo-10.1177_20503121221100991 for Identifying factors associated with neonatal resuscitation skills among nurses and midwives in Tanzania, sub-Saharan Africa by Mathias Anthony Mbinda and Fabiola Vincent Moshi in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank the University of Dodoma for providing ethical clearance for this study. We also thank the Dodoma Region administration for allowing us to conduct the study, also we thank the study respondents for volunteering to participate in this study.
Author contributions
Conceptualization: Mathias Mbinda. Data curation: Mathias Mbinda. Formal analysis: Mathias Mbinda. Methodology: Mathias Mbinda. Supervision: Fabiola Moshi. Writing—original draft: Mathias Mbinda. Writing—review and editing: Fabiola V. Moshi.
Availability of data and materials
The data and material used in the current study are available from the corresponding authors upon request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
Approval to conduct the study was given by the University of Dodoma Research and Publication Committee. Approval number/ID Ref No MA.84/261/02/85. Government authorities at regional and council levels in Dodoma Region were contacted for permission to conduct the study. A written permit was obtained to conduct the study.
Informed consent
Written informed consent was obtained from all subjects before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.