
Abstract
Existing knowledge of how maternal autonomy relates to child undernutrition in Nigeria is few and limited to children under 24 months old. Nothing is known about how it affects older children. Therefore, this study investigated whether mothers’ household autonomy affects children 24–59 months, as do children under 24 months old. We used data from 2018 Nigerian Demographic and Health Survey, which is a nationally representative survey. Samples include 3502 and 5463 children under 24 months and between 24 and 59 months old, respectively. Three anthropometry indexes were used to determine child undernutrition: weight-for-height, height-for-age, and weight-for-age, which indicate wasting, stunting, and underweight, respectively. Three domains of maternal autonomy: decision-making, financial-control, and mobility, were operationalized using responses from mothers. Results from logistic regression analysis show that in unadjusted models, maternal decision-making autonomy and mobility were associated with undernutrition in both samples. After adding covariates, only associations between maternal decision-making autonomy and underweight in children 24–59 months old retained statistical significance. Findings show that gendered social inequalities are linked to differences in child nutritional outcomes. Future studies could investigate how feeding practices mediate associations between maternal autonomy and childhood undernutrition.
Keywords
Introduction
Child growth and development are assessed through various indicators like nutrition status (Dang et al., 2014; De Onis, 2017). Undernutrition is a public health issue related to deficiencies or imbalances in nutritional consumption (World Health Organization (WHO), 2013) or morbidity effects.
Several indicators may be used to measure nutritional status. These involve body composition, clinical signs of deficiency, physical function, biochemical compounds, metabolic processes, or dietary intake (Maleta, 2006). Body composition is widely used in survey studies because it is readily measurable. Weight and height, in combination with age and sex, are anthropometry measurements usually used. These measurements can reflect three main indexes: (i) height-for-age or stunting, which indicates chronic undernutrition, (ii) weight-for-height or wasting, which indicates acute undernutrition, and (iii) weight-for-age or underweight, which is a combination of both (Kassie and Workie, 2019; WHO, 2010, 2018).
Consequences of undernutrition in children may be immediate or long-term and include weight loss, proneness to morbidity, impaired cognitive and mental development, or mortality (Henninger and Luze, 2010; Kunwar et al., 2020; Maleta, 2006).
United Nations International Children’s Emergency Fund’s (UNICEF) statistics show that globally, 6.9% and 39.3% of children under 5 years of age were wasted and stunted, respectively, in 2019 (UNICEF et al., 2020). A regional decomposition shows that Nigeria ranks poorly, particularly in West African region, with 6.8%, 36.8%, and 21.8% prevalence in wasting, stunting, and underweight, respectively. Except for wasting that slightly reduced, stunting and underweight prevalence increased from 33.0% and 19.5%, respectively, from 2015 (UNICEF et al., 2020).
Feeding practices and morbidity are two proximal factors that can directly impact a child’s nutritional status; other distal factors include a mother’s knowledge of childcare and family socioeconomic conditions (Gewa and Yandell, 2012; Sheikh et al., 2020; UNICEF, 2008). Improved maternal social status (education and employment), mental health, and household autonomy have also been linked to a better childcare and nutritional outcome (Agu et al., 2019; Ariyo and Jiang, 2020; Khan et al., 2019; Saeed et al., 2017; UNICEF, 2013).
Maternal autonomy refers to a mother’s ability to decide and act on issues that affect her and her children (Carlson et al., 2015). Usually, it encompasses various domains, including decision-making, which refers to abilities to make daily household decisions, Financial-control, which refers to abilities to decide on how household financial resources are to be allocated; and mobility, which is freedom of traveling to or visiting places, attend social events, or visit family and friends (Carlson et al., 2015; Ridgway et al., 2020).
Studies investigating associations between maternal autonomy and child nutritional outcomes are primarily based out of South Asia and sub-Sahara Africa (SSA) (Carlson et al., 2015; Cunningham et al., 2015). This is influenced by gender and poor child health and nutrition-related factors peculiar to these regions (UNICEF et al., 2020; World Economic Forum, 2021).
Several studies used a composite measure to determine maternal autonomy (Bose, 2011; Brunson et al., 2009; Lépine and Strobl, 2013). While this approach offers simplicity as it creates a single autonomy index (Shroff et al., 2009), autonomy is a multidimensional concept. Using a composite measure dilutes distinctive effects of each autonomy domain (Shroff et al., 2011).
Most studies on domain-specific analysis are based out of South Asia (Rahman et al., 2015; Sethuraman et al., 2006; Shroff et al., 2009). Studies from SSA are mostly related to socio-demographic determinants of child nutritional status indicators (Acquah et al., 2019; Akombi et al., 2017a; Alemayehu et al., 2015; Nwosu and Orji, 2018), and just a few investigated associations between maternal autonomy and child nutritional outcomes (Brunson et al., 2009; McKenna et al., 2019).
Studies based out of Nigeria on this subject are limited. Nigeria is a country in West African with more than 206 million people. It is a multicultural society, with access to health care, environment, housing, literacy, etc., similar within ethnicities (Morakinyo and Fagbamigbe, 2017). Agu et al. (2019) investigated a domain analysis of mothers’ autonomy and child undernutrition, using data obtained from fourth wave of Nigeria demographic and health survey (DHS). Their study focused on children under 24 months old, and they concluded that maternal autonomy domains, particularly decision-making and financial-control, had no adjusted association with indicators of child undernutrition. It is unknown if similar conclusions would hold when analysis extends to children 24–59 months old.
Aim
To use data from fifth wave of Nigeria DHS and re-analyze associations between mothers’ autonomy and indices of undernutrition among children under 24 months old in Nigeria, examining consistencies in findings with Agu et al. (2019). Additionally, to examine how different domains of maternal autonomy are associated with undernutrition in children 24–59 months in Nigeria.
Methods
Data source
This study analyzed data from fifth wave of Nigeria DHS. Data were collected through a cross-sectional survey from August to December 2018. The survey was conducted by National Population Commission (NPC) in collaboration with ICF International. Survey participants were selected using a stratified two-stage cluster design. These consisted of a selection of 1400 primary sampling units (PSUs) across both rural and urban strata. A nationally representative sample of 41,668 households was selected across PSUs. About 42,121 women aged 15–49 years old were identified as eligible for individual interviews in selected households, and 99% were successfully interviewed. Details of household socio-demography, maternal health, and well-being of children under-five years old were collected. Children’s anthropometry measurement was done using a digital-screened scale manufactured by UNICEF. More information about the survey and data collection is available in a separate report (National Population Commission and ICF International, 2019).
Sample selection
Children’s recode file was used for our analysis. Sample selection was restricted to children between 3 and 59 months old who live with their mother who is married (including cohabitation) and lives with her husband/partner. Additionally, children who were not de jure members of households were excluded. Children under 3 months were not included for analysis because prenatal factors such as prenatal maternal nutrition and maternal stress may account for children’s growth before 3 months (Agu et al., 2019; WHO, 2006).
Variables
Outcome variables
Indices of undernutrition, including wasting, stunting, and underweight, were outcome variables of interest in this study. They were calculated using anthropometry weight-for-height (WHZ), height-for-age (HAZ), and weight-for-age (WAZ) scores. We transformed scores into binary variables following guidelines published by WHO. Scores less than minus two indicate wasting, stunting, or underweight, while a score greater than or equal to minus two indicates a child not wasted, stunted, or underweight (WHO, 2006).
Independent variables
There were three independent variables of interest: autonomy of decision-making, autonomy of financial-control, and autonomy of mobility. These variables were operationalized based on a conceptual framework that included gender-related factors important in understanding health and nutritional outcomes (Kishor, 2005). The same framework was also used in designing DHS questionnaires. Several studies had also adopted similar operationalization (Agu et al., 2019; Rajaram et al., 2017; Singh et al., 2013), suggesting a concurrent validity.
Decision-making
This variable measured a woman’s involvement in household decisions relating to allocating resources and personal health. It was based on two components from the survey questionnaire. (i) Who decides on major household purchases? [involved (1), not involved (0)]. (ii) Who decides on personal healthcare? [involved (1), not involved (0)]. Values were summed together since both variables were measured on a similar scale. The total value, which ranged from a minimum of zero to a maximum of two, was grouped into three ordinal categories: low (0), substantial (1), and high (2).
Financial-control
This variable measured a woman’s involvement in deciding how household financial resources are to be spent. It was based on two components from the survey questionnaire. (i) Who decides on spending personal earnings? [involved (1), not involved (0)]. (ii) Who decides on spending partner’s earnings? [involved (1), not involved (0)]. Responses were categorized in same way as decision-making variable above.
Mobility
This variable measured a woman’s freedom of movement. It was based on one item from the survey questionnaire. (i) Who decides on visits to family/friends? [involved (1), not involved (0)]. Supplementary Material Table S1 contains a description and codings of independent variables.
Covariates
Several covariates adopted in this study have been discussed in other literature as possible determinants of child nutritional outcomes (Agu et al., 2019; Akombi et al., 2017a; Gewa and Yandell, 2012; Kim and Lee, 2020; Ramli et al., 2009). Child level variables were age and birth order (continuous), sex, an incident of diarrhea 2 weeks preceding the survey (binary), and breastfeeding status (categorical). Feeding practices were not collected for all age groups; therefore, we used breastfeeding status instead. Breastfeeding status was grouped into three categories: never breastfed, currently breastfeeding, and ever breastfed but no longer breastfeeding.
Maternal and household variables were: age of mother in years, education of mother in years, education of father in years, number of children under-five years old in household, wealth index of household (continuous), family type [Monogamy and polygamy], and ethnicity [Hausa/Fulani, Igbo, Yoruba, and Others]. Household wealth index was constructed by assigning scores based on ownership of certain household assets. These ranged from a television to a bicycle or car and housing characteristics such as toilet facilities and flooring materials. These scores were derived using principal components analysis and were already available as part of DHS dataset.
Ethical approval
This study was based on a secondary analysis of an existing dataset with all participant identifiers removed. Survey protocols followed Helsinki guidelines and was reviewed and approved by ICF Institutional Review Board (132,989.0.000.NG.DHS.01) and National Health Research Ethics Committee of Nigeria (NHREC/01/01/2007). Before enrollment for survey, participants gave their written consent and were told that any information they submitted would be kept confidential. No financial compensation was attached to their participation.
Analysis
Characteristics of analysis sample are described relative to each outcome variable using weighted percentages—sampling weight used to adjust for over or under-sampling of population groups. Statistically significant differences in distributions were tested using Pearson chi-square test for categorical variables and t-test, or Wilcoxon rank-sum test (non-normal distribution) for continuous variables. Collinearity diagnostics were checked among predictors and covariates to identify potential multicollinearity issues. All variance inflation factors (VIF) were below 10, with an average VIF of 1.76.
Two separate weighted regression analyses were performed. These included children under 24 months and children 24–59 months old. Maternal autonomy variables were first analyzed independently in unadjusted logistic regression models. A full analysis model included all covariates and all measures of maternal autonomy. Sensitivity analysis was conducted using continuous measures of dependent variables- HAZ, WHZ, and WAZ scores. All analyses were done using STATA software version 13.0 (StataCorp, College Station, TX, USA), and results were reported at a 95% significance threshold.
Results
Description of sample characteristics
A total of 12,806 children were identified as eligible for anthropometry measurements based on the survey report. About 11,471 (89.6%) children were successively measured. Of those measured, 11,314 (98.6%) measurements were valid. Invalid measures were primarily due to implausible values. Based on our inclusion criteria, sample selection generated a total of 8965 observations (3502 and 5463 children under 24 months and between 24 and 59 months old, respectively).
Overall, male children were 4599 (51.3%). About 637 (7.1%) of children were wasted, 3478 (38.8%) were stunted, and 2008 (22.4%) were underweight. Average age of children was 29.9 months (Standard deviation (SD) = 16.47). A larger proportion of children, 6176 (68.9%), were ever breastfed but no longer breastfeeding, 2644 (29.5%) were currently breastfeeding, and a small fraction of 143 (1.6%) were never breastfed. Concerning mothers’ autonomy, 4518 (50.4%) of mothers had low involvement in decision-making, 3334 (37.2%) had low financial-control, and 3729 (41.6%) had limited mobility. Mothers’ average age was 30.1 years (SD = 6.64), and their average years of education was 6.0 years (SD = 5.66). Average household wealth index was −0.06 (SD = 0.98), showing that most households had a low wealth index. A slightly bigger proportion of households, 5020 (56.0%), were rural residents.
Bivariate analysis
Distribution of independent variables and socio-demographic characteristics of analysis sample by children’s undernutrition (N = 8965); 2018 Nigerian Demographic and Health Survey.
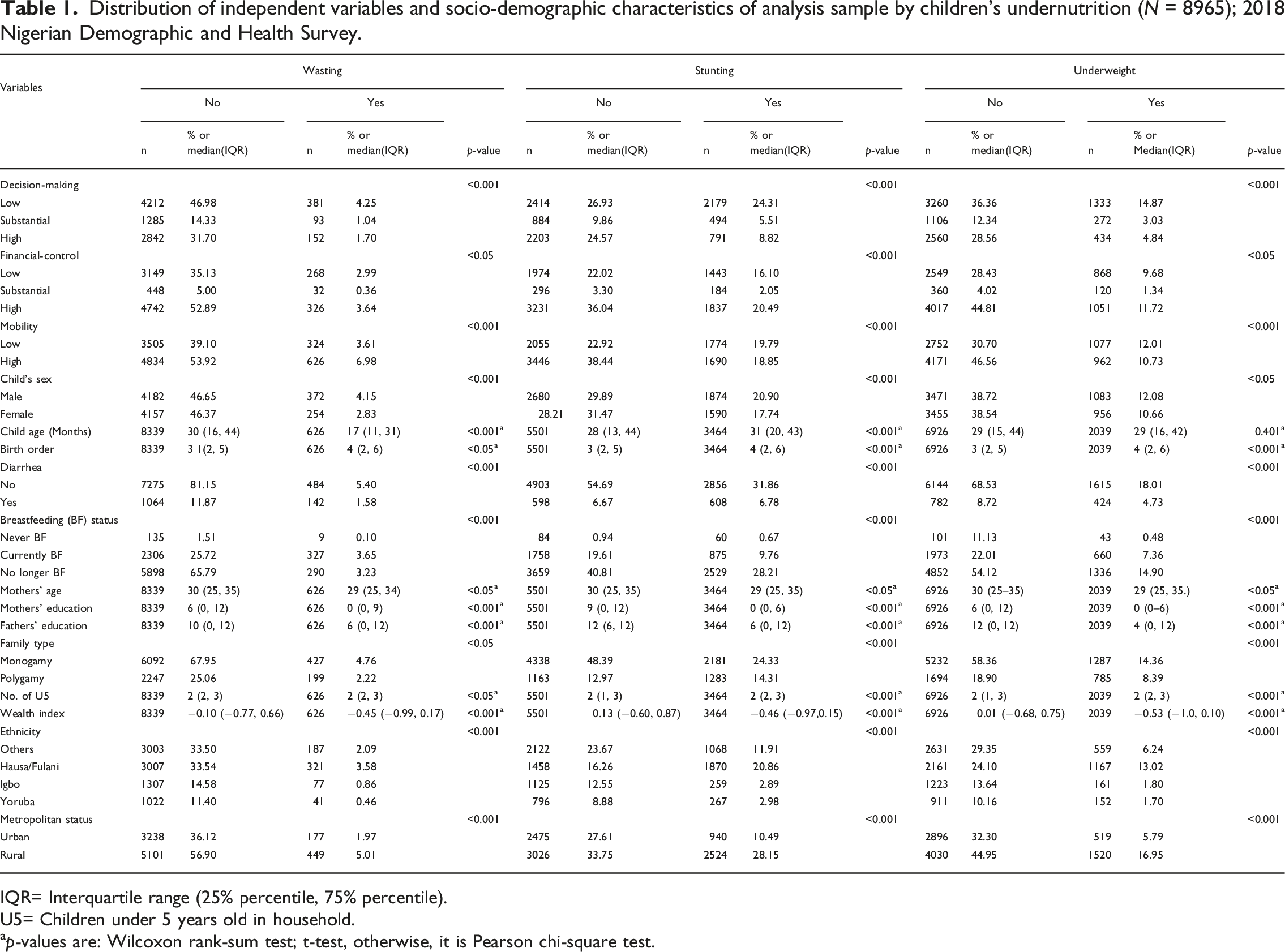
IQR= Interquartile range (25% percentile, 75% percentile).
U5= Children under 5 years old in household.
p-values are: Wilcoxon rank-sum test; t-test, otherwise, it is Pearson chi-square test.
There were statistically significant differences between expected and observed observations within categories of each autonomy variable by indices of child undernutrition. Expectedly, proportions of wasted, stunted, or underweight children were highest when mothers had low decision-making involvement or limited mobility. Even though proportions of wasted, stunted, or underweight children were not highest among mothers with low financial-control, they were still relatively high. About 2,179 (24.3%), 1,443 (16.1%), and 1,774 (19.8%), for wasting, stunting and underweight, respectively.
Multivariate analysis
Association between maternal autonomy and child undernutrition for children under 24 months old
Results from unadjusted associations between components of maternal autonomy and indices of undernutrition among children under 24 months old are presented in Supplementary Material Table S2. When compared to children of mothers who had low involvement in decision-making, children of mothers who had substantial involvement in decision-making were 14% less likely to be wasted OR = 0.86; 95% CI [0.59, 1.23], 27% less likely to be stunted OR = 0.73; 95% CI [0.58, 0.90] and 29% less likely to be underweight OR= 0.71; 95% CI= [0.54, 0.93]. Wasting was not statistically significant at p < .05. Children of mothers who had high autonomy of decision-making were 49% less likely to be wasted OR = 0.51; 95% CI [0.37, 0.70], 54% less likely to be stunted OR = 0.46; 95% CI [0.37, 0.56] and 56% less likely to be underweight OR = 0.44; 95% CI [0.34, 0.56].
Financial-control had no statistically significant association with indices of undernutrition for children under 2 years. Mothers’ freedom of mobility, on the other hand, had a statistically significant association. Compared with children of mothers who had low mobility, children of mothers who had high freedom of mobility were 30% less likely to be wasted OR = 0.70; 95% CI [0.53, 0.92], 33% less likely to be stunted OR = 0.67; 95% CI [0.56, 0.80], and 39% less likely to be underweight OR = 0.61; 95% CI [0.50, 0.73].
Full models showing adjusted odds ratio of factors associated with measures of undernutrition in children under 24 months old in Nigeria (n = 3502); 2018 Nigerian Demographic and Health Survey.
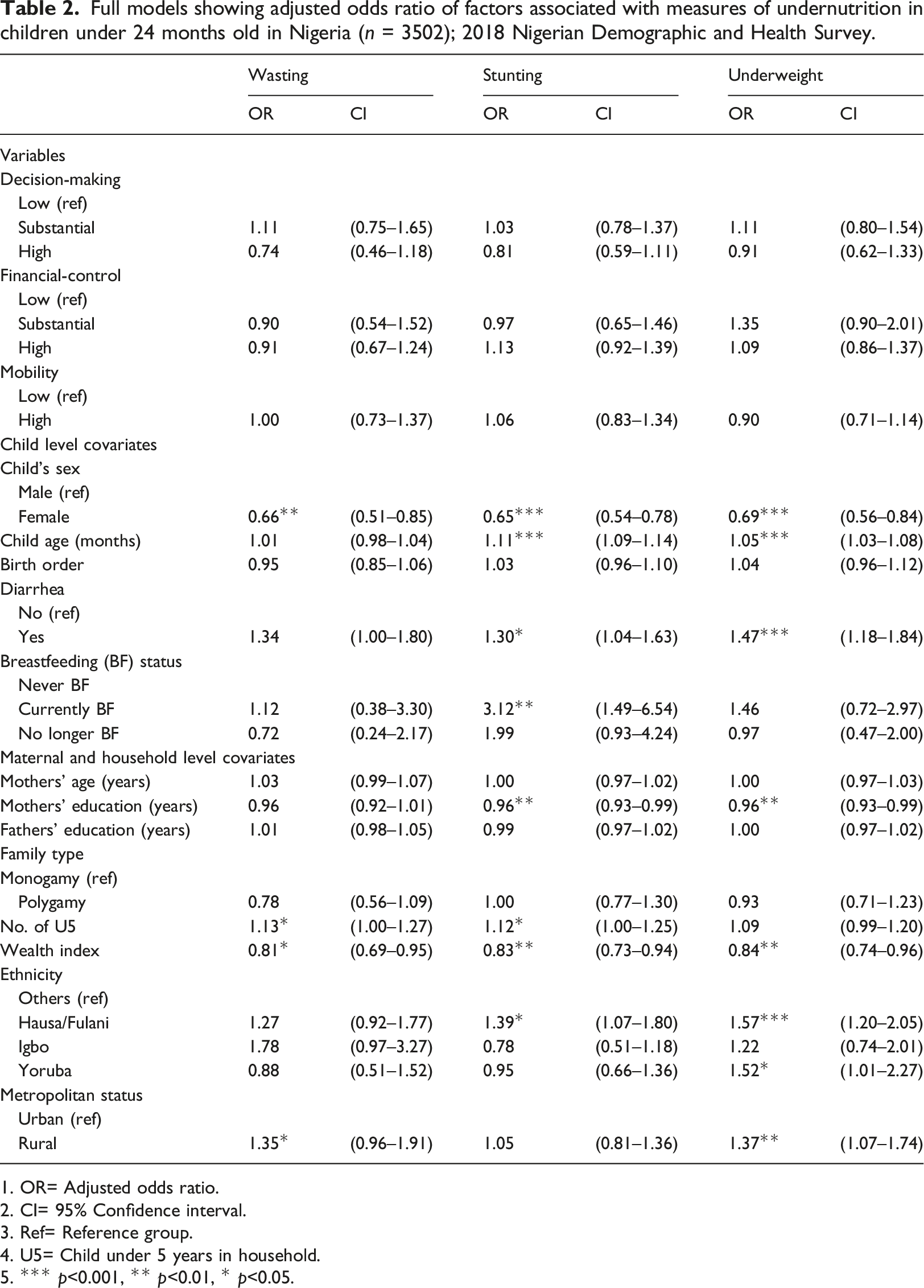
1. OR= Adjusted odds ratio.
2. CI= 95% Confidence interval.
3. Ref= Reference group.
4. U5= Child under 5 years in household.
5. *** p<0.001, ** p<0.01, * p<0.05.
Association between maternal autonomy and child undernutrition among children 24–59 months old
Results from unadjusted associations between domains of maternal autonomy and indices of undernutrition among children 24–59 months old are presented in Supplementary Material Table S3. When compared with children of mothers who had low involvement in decision-making, children of mothers who had substantial involvement in decision-making were 31% less likely to be wasted OR = 0.69; 95% CI [0.42, 1.11], 45% less likely to be stunted OR = 0.55; 95% CI [0.45, 0.67], and 46% less likely to be underweight OR = 0.54; 95% CI [0.41, 0.71]. Wasting was not statistically significant. Children of mothers who had high autonomy of decision-making were 48% less likely to be wasted OR = 0.52; 95% CI [0.36, 0.75], 70% less likely to be stunted OR = 0.30; 95% CI [0.26, 0.35] and 66% less likely to be underweight OR = 0.34; 95% CI [0.28, 0.41].
Mothers’ financial-control was not statistically significantly associated with wasting, but it had a statistically significant association with stunting and underweight. Compared with children of mothers who had low financial-control, those of mothers who had high financial-control were 27% OR = 0.73; 95% CI [0.63, 0.85] and 24% OR = 0.76; 95% CI [0.64, 0.89] less likely to be stunted and underweight, respectively.
Mothers’ freedom of mobility was significantly associated with measures of undernutrition among children between 24 and 59 months old. Compared with children of mothers who had low mobility, children of mothers who had high freedom of mobility were 45% less likely to be wasted OR = 0.55; 95% CI [0.40, 0.74], 53% less likely to be stunted OR = 0.47; 95% CI [0.41, 0.54], and 45% less likely to be underweight OR = 0.55; 95% CI [0.47, 0.64].
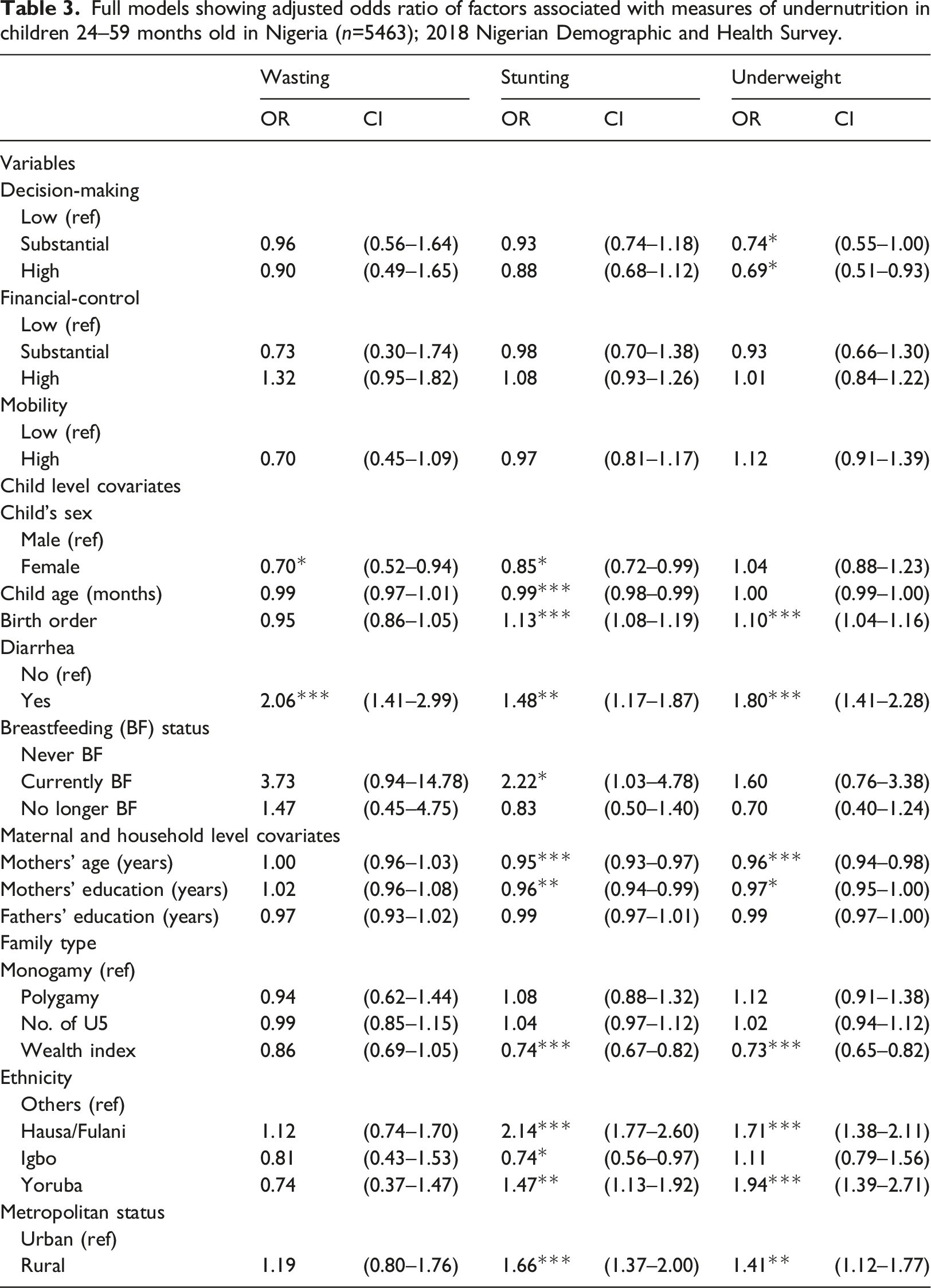
Full models showing adjusted odds ratio of factors associated with measures of undernutrition in children 24–59 months old in Nigeria (n=5463); 2018 Nigerian Demographic and Health Survey.
Discussion
There is little understanding of how maternal autonomy contributes to childhood undernutrition in Nigeria. Our study examined this association using three domains of maternal autonomy and three indices of childhood undernutrition. Data were obtained from fifth wave of Nigeria DHS. Our sample included a total of 8965 mother-child dyad (3502 and 5463 children under 24 months and between 24 and 59 months old, respectively). We performed logistic regression analysis to determine associations between maternal autonomy and childhood undernutrition.
According to our findings, associations between all domains of maternal autonomy and indices of childhood undernutrition in children under 24 months became attenuated when covariates were included in the models. Analysis results of children 24–59 months showed that household decision-making was associated with children underweight but not wasting and stunting. When all covariates are included, mothers’ financial autonomy and mobility were not associated with all three indices of childhood undernutrition among children aged 24–59 months.
This study validates findings reported in Agu et al. (2019), also set in Nigeria, and extends it by showing how results compare with children 24–59 months old. Additionally, these findings are similar to others based out of India (Rajaram et al., 2017; Shroff et al., 2009), Bangladesh (Rahman et al., 2015), Nepal (Dancer and Rammohan, 2009), Kenya (Brunson et al., 2009), and Congo (McKenna et al., 2019).
Although our study and Agu et al. (2019) utilized different waves of data, results regarding associations between maternal autonomy domains and undernutrition indices among children under 24 months old were consistent. In our study and theirs, results’ statistical significance became attenuated after including covariates.
Based on the analysis sample of children 24–59 months old, mothers’ decision-making autonomy is inversely associated with children underweight, but not with wasting and stunting. This specific finding conforms with conclusions stated in Santoso et al. (2019). Their study reviewed 62 peer-reviewed articles on associations between maternal autonomy and indices of child nutrition and reported underwhelming evidence of a significant association for wasting and stunting.
Underweight is a measure of both acute and chronic undernutrition—a combination of wasting and stunting (Kassie and Workie, 2019; WHO, 2010, 2018). Children who are wasted may also be stunted, suggesting that one form of malnutrition can contribute to another over time (Briend et al., 2015). Inadequate healthcare, or feeding practices are possible pathways of association (UNICEF, 2008). In our study, decision-making was formed from two components—healthcare and household purchases.
First, mothers who can decide on personal health are likely to be health-conscious (Ariyo and Jiang, 2020; Ickes et al., 2015). This could translate into paying more attention to health matters of their children as it relates to good nutritional practices as a way of maintaining a healthy living (Obonyo, 2018). As Ogbo et al. (2015) reported after analyzing 2003–2013 Nigeria DHS, recommendations on infant and young child feeding (IYCF) practices are more likely to be met by mothers who frequently utilize healthcare services. Secondly, being involved in deciding what household resources (e.g., food supplies) to purchase, mothers may be compelled to make choices beneficial to their children (Carlson et al., 2015; Cunningham et al., 2015). Older children usually require more nutrient intake for better linear growth and development than younger children (Nelson et al., 1989). This may explain why results were statistically significant for children 24–59 months but not children under 24 months.
Results based on unadjusted analysis showed that financial autonomy was not statistically significantly associated with any indices of undernutrition in children under 24 months old but associated with at least two indices in children 24–59 months old. A similar mixed finding has also been seen in previous studies from India and Nepal (Dancer and Rammohan, 2009; Sethuraman et al., 2006). While it is expected that a woman will be more likely to divert resources for child upkeep, a qualitative study found some evidence to suggest that this may not always be true. Having access to finances does not ensure that she will divert such to child well-being (Myntti, 1993).
Working nursing mothers who may have to schedule their time between work and childcare could be another reason why no statistically significant association was found in the analysis sample of children under 24 months. Financial-control and employment status are different yet closely related constructs (Agarwala and Lynch, 2006; Basu and Koolwal, 2005; Carlson et al., 2015). Several studies often include employment status as a component of financial-control (Carlson et al., 2015; Cunningham et al., 2015). In assessing implications of women’s work on a child’s nutritional outcomes in Nigeria, Ukwuani and Suchindran (2003) reported that a mother’s income has no remarkable positive associations with nutritional status of children at infancy. Working nursing mothers may be compelled to adopt inappropriate IYCF practices, for example, early termination of breastfeeding (Oddo and Ickes, 2018; Ogbo et al., 2015) or rely on social support or paid child care services—availability of which is affected by social and economic variables.
Attenuation of statistical significance after including covariates, particularly for children under 24 months, suggests that other factors alongside maternal autonomy strongly influence children’s nutrition. Based on results that correspond to each covariate, such factors are likely to be child’s sex, mother’s educational attainment, and household wealth index.
Being a female child protects from being wasted, stunted, or underweight. Although there is no known biological explanation for why this may be so, it is consistent with several other studies from Africa (Akombi et al., 2017b; Gewa and Yandell, 2012; Tosheno et al., 2017). Akombi et al. (2017a) suggested that male children tend to engage in more physically intense activity than females; as a result, using up large amounts of energy that would have been rather conserved for proper growth and development.
Expectedly, mothers’ educational level and family wealth were also inversely associated with child undernutrition. Educated mothers are better informed about good nutritional practices (Akombi et al., 2017a). Also, they are more likely to participate in household decision-making (Carlson et al., 2015; Dancer and Rammohan, 2009), therefore, influencing their children’s well-being positively. Also, family wealth could substitute as a proxy for household food security (Saaka and Osman, 2013), serving as a protective factor against poor nutritional outcomes in infants and young children (Bahorski et al., 2019; Mahumud et al., 2021; Ramsey et al., 2011).
Limitations
Some limitations are associated with this study. Using data from a cross-sectional survey prevents us from drawing causal relationships. Also, variables used were limited to what was captured by the survey. Specifically, social support from a partner was not captured. A woman undertaking decisions alone may also be due to a lack of support from her partner. Additionally, data on child’s feeding practices were not collected for children over 2 years old. As such, we could not control this factor.
Domains of maternal autonomy are not uniformly measured in studies. This makes it difficult to make a solid comparison of results with other studies. Finally, information gathered during the survey may only reflect happenings at that moment. Autonomy is dynamic and could be subject to change over time.
Implication for practice
Findings from this study suggest that improving women’s empowerment could be associated with better nutritional outcomes in children. To incorporate this as a policy measure, programs to pursue are also in tandem with the United Nation’s SDGs related to poverty eradication, quality education, and gender equality.
First, there is a need to improve female education. Female education will, in adulthood, translate into decision-making abilities, increased employability, and economic stability. Secondly, governmental and non-governmental agencies will have to sensitize low-income population groups on cost-effective methods and benefits of good nutritional practices for children. Regional-specific policies may be warranted based on evidence of proportion and likelihood variations across regions.
For other SSA and South Asian countries that have similar phenomena, international agencies and government policymakers should, in addition to women’s agency approach, explore other approaches, including encouraging fathers’ active participation in childcare, particularly during early development. Active involvement of fathers in childcare has been associated with better maternal autonomy, social and psychological support for childcare, and better child health and development outcomes (Abate and Belachew, 2017; Alio et al., 2010; Nsamenang, 2010).
Conclusion
Findings in this study show that certain domains of maternal autonomy are associated with indices of undernutrition in infants and young children. Other covariates, such as female sex, mothers’ educational level, and family wealth index, were also related to protection against childhood malnutrition. Policies aimed at reducing undernutrition in children should be framed to address gendered social inequalities. Future studies could investigate how feeding practices mediate associations between maternal autonomy and childhood undernutrition.
Supplemental Material
Supplemental Material—Maternal autonomy and childhood undernutrition: Analysis of 2018 Nigeria demographic and health survey
Supplemental Material for Maternal autonomy and childhood undernutrition: Analysis of 2018 Nigeria demographic and health survey by Tolulope Ariyo and Quanbao Jiang in Journal of Child Health Care.
Footnotes
Acknowledgments
The authors thank the Demographic and Health Surveys (DHS) for permission to use the NDHS data for the present study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
This study was based on a secondary analysis of an existing dataset with all participant identifiers removed. The survey protocol followed the Helsinki guidelines and was reviewed and approved by ICF Institutional Review Board (132989.0.000.NG.DHS.01), and the National Health Research Ethics Committee of Nigeria (NHREC/01/01/2007). Written consent was obtained from participants, and they were notified of the confidentiality of information collected before their recruitment into the survey. No financial compensation was attached to the respondent’s participation.
Data availability
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.