
Abstract
Indigenous peoples’ worldviews are intricately interconnected and interrelated with their communities and the environments in which they live. Their worldviews also manifest in a holistic view of health and well-being, which contrasts with those of the dominant western biomedical model. However, screening depression and/or anxiety in Indigenous peoples often occurs using standard western tools. Understandably, the cultural appropriateness of these tools has been questioned. The purpose of this scoping review was to map the literature that used any type of tool to screen depression or anxiety in Indigenous adults globally. A systematic scoping review method was used to search databases including, but not limited to, CINAHL, PubMed, Scopus and Google. Database-specific search terms associated with Indigenous peoples, depression and anxiety, and screening tools were used to identify literature. In addition, citation searches of related systematic reviews and relevant websites were conducted. The data set was limited to English language publications since database inception. Fifty-four publications met the review's inclusion criteria. Most studies were completed in community settings using standard western depression and anxiety screening tools. Thirty-three different tools were identified, with the Patient Health Questionnaire-9 being the most frequently used. The review's findings are concerning given repeated calls for culturally appropriate screening tools to be used with Indigenous peoples. Although there has been some work to cross-culturally adapt depression screening tools for specific Indigenous populations, clearly more clinicians and researchers need to be aware of, and use, culturally appropriate approaches to screening.
Introduction
The worldviews of Indigenous peoples are intricately interrelated and interconnected with those of their communities and the environments in which they live. Indigenous people conceptualise health and well-being more holistically (Gall et al., 2021) than the dominant western biomedical paradigm (Le Grande et al., 2017; Wilson & Richmond, 2009). Physical, mental, spiritual and psychosocial well-being are not discrete as they are in western conceptualisations of health (Wilson & Richmond, 2009).
For the purposes of this scoping review, the definition of an Indigenous person proposed by the United Nations (United Nations, 2013) has been adopted. Although the United Nations are of the view that a universal definition for Indigenous people is not necessary, they do identify that Indigenous people are peoples in independent countries who are regarded as indigenous on account of their descent from the populations which inhabited the country, or a geographical region to which the country belongs, at the time of conquest or colonization or the establishment of present state boundaries and irrespective of their legal status retain social, cultural, economic, and political characteristics that are distinct from those of the dominant societies in which they live (United Nations, n.d., p. 5).
Screening for mental health disorders such as depression and anxiety conducted in Indigenous populations has typically used western (hereafter referred to as standard) tools. However, several authors (Black et al., 2015; Gomez Cardona et al., 2021; Gray et al., 2016; Janca et al., 2015; Le Grande et al., 2017; Shore & Manson, 1981; Verney et al., 2008) have suggested that standard screening tools are inappropriate owing to the different cultural conceptualisations of mental health and well-being and language used. Tests may measure different constructs in other populations (Reynolds & Suzuki, 2012) and Gone and Kirmayer (2020, p. 235) argued that adaptation of ‘mental health theories, models and interventions’ is necessary to support the mental health of Indigenous peoples.
Bias and equivalence are two important methodological concepts that need to be attended to in cross-cultural research (He & van de Vijver, 2012). Statistically, bias is defined as a systematic error in the estimation of value (Reynolds & Suzuki, 2012). Bias can be found in the underlying construct being measured and its consequent items (questions) and the method (sampling, instrument and administration) (He & van de Vijver, 2012). Therefore, tests designed for and validated with the majority population as participants may measure different constructs in a minority population (Reynolds & Suzuki, 2012), whereas equivalence is related to cross-cultural comparisons. For example, where comparisons between Indigenous Australian and Anglo-Celt participants have been conducted (Davis et al., 2015), the tool used to screen for depression, in this case the Patient Health Questionnaire (PHQ-9), should lead to equivalent comparisons between the two groups. Both bias and equivalence have important implications for studies investigating depression and/or anxiety with Indigenous populations. In the example above, bias is present in the screening tool used with the Indigenous population because it was developed in the United States using predominantly White participants (Kroenke et al., 2001). Concomitantly, equivalence cannot be achieved. Equitable access to mental health support for people with depression and/or anxiety relies first on screening using a valid and reliable tool (instrument or scale). Ensuring that tools are equivalent and unbiased is the first step to achieving this aim.
This scoping review is situated in the context of a broader research project designed to develop a culturally appropriate depression and anxiety screening tool for Aboriginal and Torres Strait Islander communities in Far North Queensland, Australia. This project seeks to address the difficulties experienced by the research team (Russell et al., 2021, 2022) when using standard depression and anxiety screening tools in the Torres Strait. Issues emerged with the unfamiliar words and concepts used that resulted, at times, in questions being misinterpreted or viewed as offensive. This situation had the potential to impair the therapeutic rapport that the clinicians/researchers were trying to establish with participants. Consequently, the focus of this scoping review was to map the extant literature related to screening for depression and anxiety in Indigenous populations globally to inform this wider project. A scoping review was the most appropriate systematic approach because it permits mapping of published and grey literature (Arksey & O’Malley, 2005), including the approaches of various governments to obtaining mental health information from population-based surveys.
Preliminary searches of relevant databases indicated that there were no scoping reviews currently underway on this topic. Although several systematic reviews related to similar topics such as cultural concepts of distress (Kohrt et al., 2014) and mental health in Indigenous populations (Black et al., 2017, 2015; Bowen et al., 2014; Chan et al., 2021; Dingwall & Cairney, 2010; Jorm et al., 2012; Kisely et al., 2017; Nelson & Wilson, 2017) have been conducted, they are limited to specific Indigenous populations or cohorts within them. Consequently, the objective of this scoping review was to more broadly assess the extent of the literature related to tools used for screening depression and anxiety in Indigenous adults globally.
Method
The protocol for scoping reviews outlined by the Joanna Briggs Institute (Peters et al., 2020) was used to guide data collection. The scoping review was registered with The Open Science Framework database (https://osf.io/9azwd). In line with the recommendations of Peters et al. (2020), this scoping review did not undertake a critical appraisal of individual sources because the aim was to gather as much information as possible from both the published and grey literature, some of which was obtained from national health surveys of Indigenous peoples in which the methods of obtaining the information was difficult to ascertain. In addition, the focus of the review was to scope the range of tools used to screen depression and anxiety of Indigenous peoples, rather than the methods used to develop or implement such tools. Because this scoping review collected data from open sources ethical approval was not required.
Data was collected in three phases. Phase one focused on search strategy, phase two on data selection and phase three on data extraction. The research question that guided data collection was: What tools are used to screen depression and anxiety in Indigenous adults globally? Associated sub-questions that guided inclusion criteria included:
In what geographical, cultural, clinical or other contexts is screening for depression and anxiety in Indigenous adults taking place? Why are depression and anxiety screening tools being used? Are they valid and reliable for the population that they are being used with?
Inclusion criteria
The Participant, Concept, Context framework was used to develop the inclusion criteria and search strategy employed during the data collection phase of the review. Studies whose participants were Indigenous adults (≥18 years) from any part of the world were included.
The concepts that framed the inclusion criteria included any tools used to screen for depression and anxiety in Indigenous peoples, whether or not they were specifically designed for this population. Published and unpublished/grey literature that specifically identified Indigenous participants who met the definition of Indigenous adopted for this scoping review were included in the data set. In addition to retaining distinct characteristics that are different from the dominant society (United Nations, n.d.), Article 33 of the United Nations Declaration on the Rights of Indigenous peoples stated that the right to identify as an Indigenous person (self-identification) is fundamental (United Nations, 2007). Consequently, published and unpublished literature in which participants were identified as Indigenous or where identifying titles were used such as, but not limited to, First Nations, Māori, Native American were included in the scoping review. For example, participants in Sorlie et al. (2018) study came from ‘Sami core, Sami affiliation, Sami background or majority Norwegian groups’ (p. 1). According to Northern Norway (n.d.) the Sami peoples inhabit Norway, Sweden, Finland and Russia, and have distinct languages that are unrelated to Norwegian and other Indo-European languages. Traditionally, they herded reindeer and are recognised as the oldest culture in large areas of northern Norway. The Norwegian Sami were subject to a rigorous assimilation policy between 1860 and 1960 (Sorlie et al., 2018) and are a minority in the Norwegian population. In this scoping review, the term Indigenous is respectfully used to be inclusive of global populations who identify as such and are distinct from the dominant population.
In addition, studies that compared participants from non-Indigenous cultures with Indigenous participants, and those that used tools to describe, identify issues, determine the psychometric properties of (including validation), or determine prevalence of depression and/or anxiety of Indigenous adults, were included in the data set. Inclusion criteria in order of priority were:
literature focused on depression and anxiety screening tools used with Indigenous adult populations; a specific tool used for screening depression and anxiety was identified; literature used primary data sources; tools were used with participants recruited from any setting (acute, primary healthcare, community); the publication constituted a complete paper or report (not an abstract, executive summary, editorial, etc.); only literature published in English was included.
The inclusion of data from primary data sources was chosen because the rationale for this scoping review is based on not only the use of depression and anxiety screening tools, but also the participant and researcher experience of interacting with the tool; for example, limitations to participation such as: Does written English literacy limit a participant's ability to self-report? Do western conceptualisations of depression and anxiety mean that questions in a screening tool are using words that are unfamiliar or do not relate to an Indigenous person's way of thinking and/or feeling about their mood? In addition, when the method for collecting the data is not described in detail, unintended limitations may not be able to be determined by the reader. Finally, often authors report limitations or difficulties that their participants had with interacting with the tool, or researchers found with tool administration, in the discussion section. Articles reporting the findings of secondary data analysis do not have this information to share in the discussion.
Search strategy
The search strategy located both published and unpublished studies and reports. The databases searched included CINAHL, Emcare, Medline (Ovid), PsychInfo, PubMed (Ovid) and Scopus. Google, Google Scholar and website searches were used to locate sources of unpublished studies and grey literature. In addition, citation searches of all included sources of evidence were screened for additional studies. The reference lists of systematic reviews on similar topics were also searched for appropriate papers, reports or other data sources. Unpublished studies and reports, once located, were downloaded if that was possible. If it was not possible a screenshot of the information was taken, or the information was copied and pasted into a Word document. These documents were subsequently saved with all the other data. In addition, if a reference was available (through Google Scholar, for example) it was downloaded and imported into EndNote. If a citation was not available, the capture reference function available through EndNote was used and the citation was directly imported into EndNote Online. The full search strategies for all databases are provided in the online Supplemental material. Data were collected between August and September 2022.
Data selection
Phase two of data collection was managed in EndNote (version 20.1; Clarivate Analytics) according to the method proposed by Peters (2017). Subsequently, a pilot test of the data collected using the search strategy (Peters et al., 2020) was conducted between the first two authors. An interrater reliability of 95% was achieved in the pilot test and discrepancies were discussed. This discussion facilitated further refinement of the inclusion criteria. The rest of the data collection process, including retrieval of full-text articles, website and citation searches, was conducted by the first author. Relevant citation information of all included literature was then entered into an Excel spreadsheet, where all subsequent screening took place. The second author used this database to independently screen full-text articles and reports. Any discrepancies were resolved through discussion. The data collection process is presented in a Preferred Reporting Items for Systematic Reviews and Meta-analyses extension for scoping review (PRISMA-ScR) flow diagram (2020) (Figure 1).
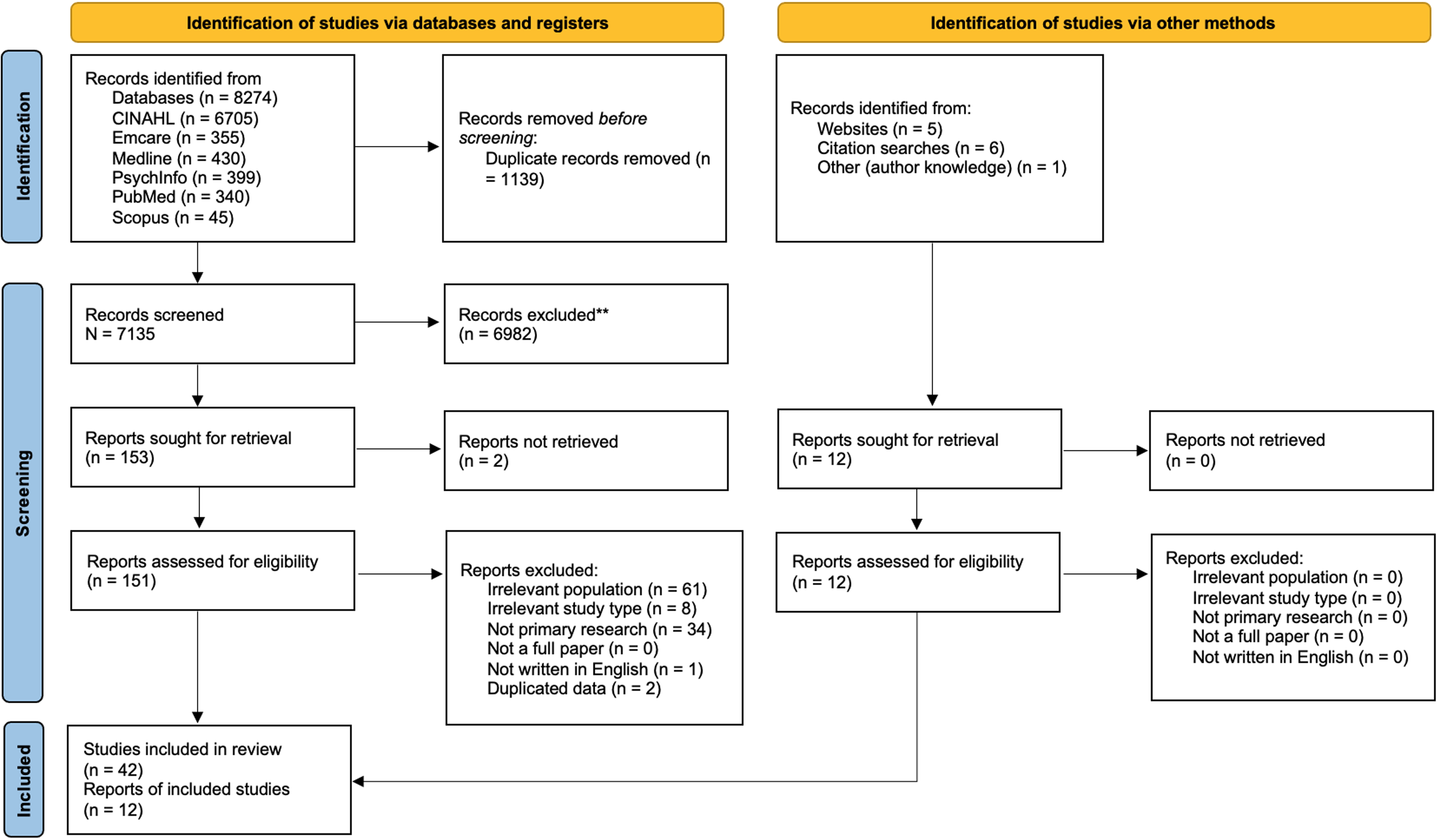
PRISMA study flowchart (adapted from Page et al., 2021).
Data extraction
Data was extracted independently by the first two authors and entered into an Excel spreadsheet. Aside from citation information, other data fields included: the country where the study was conducted; context; study population and sample size (n); population mean age (and/or range); study aim/purpose; method; tool type; study outcome; and key findings as they related to the research question and sub-questions. The tool type categories were: (1) unmodified standard (western) tool; (2) language translation of a standard tool; (3) cross-culturally adapted standard tool; and (4) non-western country-specific tool.
The spreadsheet was iteratively refined by the first two authors through discussion of the emerging themes as data extraction progressed. For example, tool type had two additional categories added (2 and 4) after data extraction commenced in response to emerging themes. Tool type 4 was included to enable the categorisation of an anxiety and depression tool developed specifically for the Chakma and Marma population living in Bangladesh. This tool type was different from tool type 1 (standardised western tools) because it was developed in a non-western country.
Data analysis
Data was analysed quantitatively to identify geographic distribution and by context and date. Quantitative sums of tool types used were categorised according to the definitions provided above. Qualitative summing of the names of different types of tools and their related context was also conducted. Qualitative coding to develop themes focused on the rationale for tool use as well as its psychometric properties, limitations of the study and/or recommendations for future investigation was also conducted. The results are presented below.
Results
This scoping review focused on answering the research question: What tools are used to screen for depression and anxiety in Indigenous adults globally?
Yield of databases and other searches
Database searches yielded 8274 records, which were reduced to 7139 after duplicates were removed. Screening subsequently reduced the data set to 153 records. Full-text screening brought this number down to a total of 42 records, which were included in the final data set. While reviewing full-text records, a list of cited websites was made. This list was used to identify possible additional sources available on websites. Records obtained from searching the reference lists of all included papers, as well as systematic reviews on a related topic, yielded an additional six records. A search of websites including Google, Google Scholar and other relevant sites, for example the Canadian First Nations Information Governance Centre (https://fnigc.ca/) and the Australian Bureau of Statistics yielded a further five records. One further record known to the authors but not located through any database or other search was also included. The alternate search strategy yielded 12 records. All search strategies located a final data set of 54 records that met the inclusion criteria for the scoping review (Figure 1 and Table 1). Abbreviations for scales included in the studies listed in Table 1 are included at the end of the table. In addition, scales used to validate adapted and/or new scales appear in parentheses after the scale abbreviation.
Characteristics of included records.
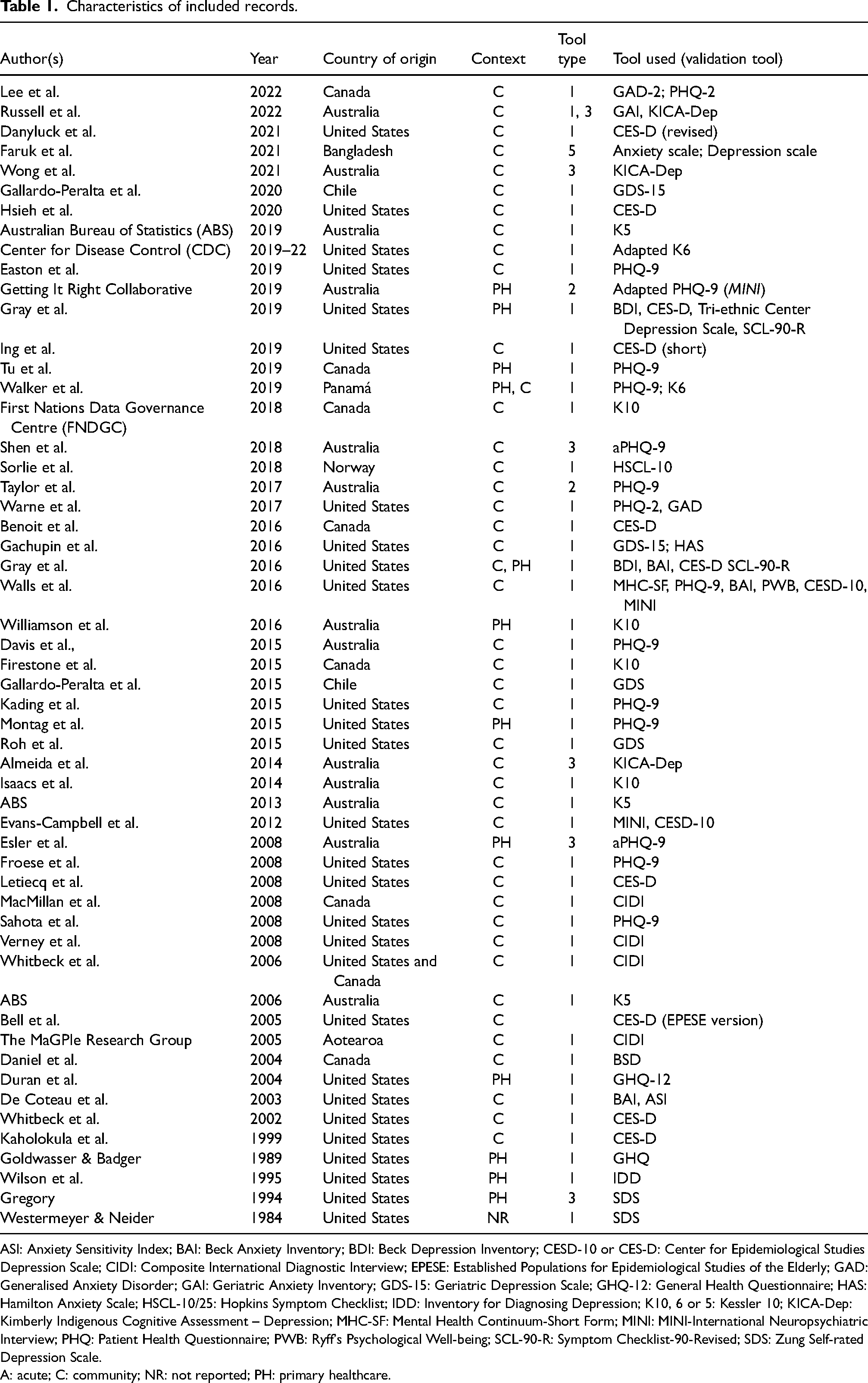
ASI: Anxiety Sensitivity Index; BAI: Beck Anxiety Inventory; BDI: Beck Depression Inventory; CESD-10 or CES-D: Center for Epidemiological Studies Depression Scale; CIDI: Composite International Diagnostic Interview; EPESE: Established Populations for Epidemiological Studies of the Elderly; GAD: Generalised Anxiety Disorder; GAI: Geriatric Anxiety Inventory; GDS-15: Geriatric Depression Scale; GHQ-12: General Health Questionnaire; HAS: Hamilton Anxiety Scale; HSCL-10/25: Hopkins Symptom Checklist; IDD: Inventory for Diagnosing Depression; K10, 6 or 5: Kessler 10; KICA-Dep: Kimberly Indigenous Cognitive Assessment – Depression; MHC-SF: Mental Health Continuum-Short Form; MINI: MINI-International Neuropsychiatric Interview; PHQ: Patient Health Questionnaire; PWB: Ryff's Psychological Well-being; SCL-90-R: Symptom Checklist-90-Revised; SDS: Zung Self-rated Depression Scale.
A: acute; C: community; NR: not reported; PH: primary healthcare.
Geographical context
Twenty-seven records were retrieved from studies conducted in the United States, which was the largest number of records sourced from one country. Thirteen studies were conducted in Australia and nine in Canada, with one of these studies being conducted and counted in the totals for both Canada and the United States. Two studies were conducted in Chile, and one each in Aotearoa (New Zealand), Bangladesh, Norway and Panamá. Figure 2 illustrates the spread of the studies globally.
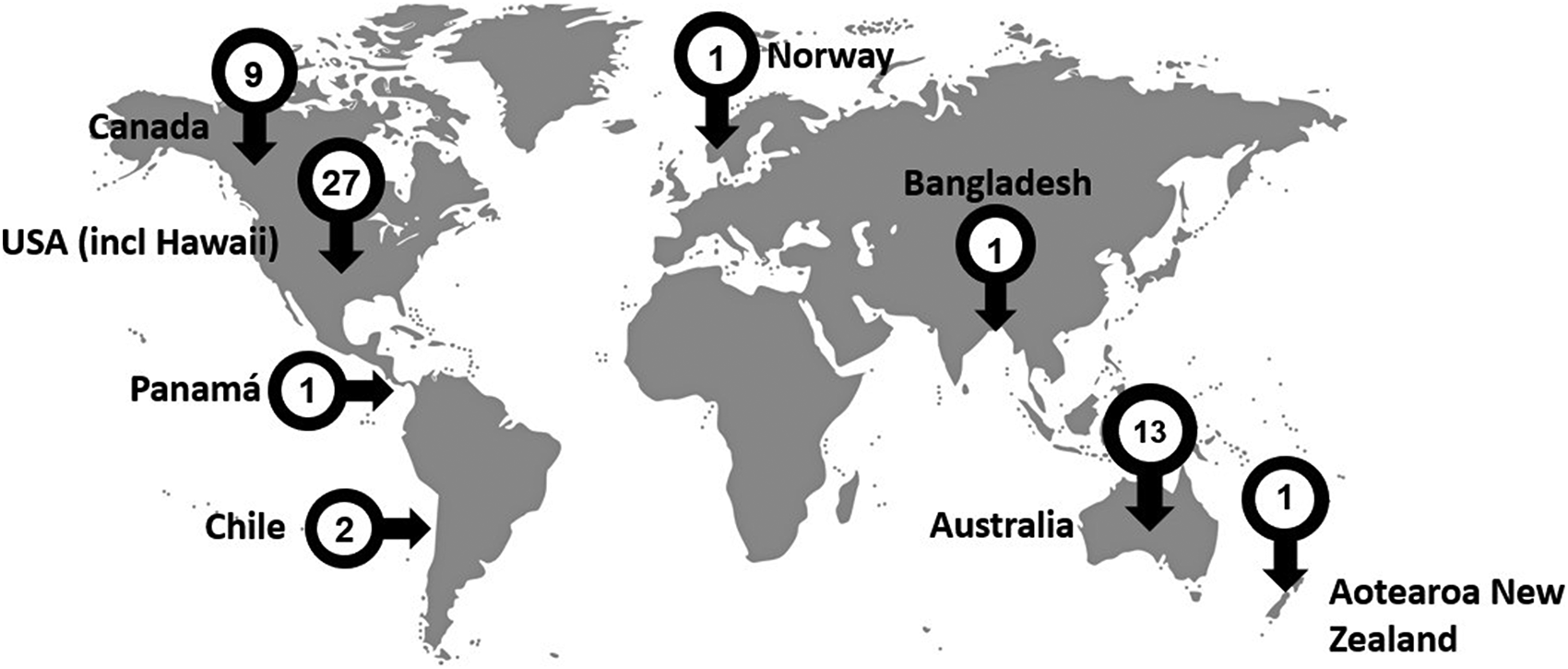
Spread of studies across the globe.
In line with the geographical context in which studies took place, most were conducted with Indigenous peoples who identified as American Indian and/or Alaskan Native and/or Native Hawai’ian. Australian Aboriginal and/or Torres Strait Islanders peoples and Canadian First Nations, Metis and Inuit peoples participated in 13 and 9 studies, respectively. Smaller numbers of studies that met the inclusion criteria for this scoping review were conducted with the Aymara and Mapuche from Chile (n = 2), the Māori from Aotearoa, (n = 1), the Chakma and Marma from Bangladesh (n = 1), the Sämi from Norway (n = 1) and the Kuna Indians from Panamá (n = 1).
Study contexts
Publication year and study setting were examined as part of the study context for the included studies. Only five papers (9%) published before 2000 met the inclusion criteria. Between 2000 and 2010, 14 (25%) papers that met the inclusion criteria for this scoping review were published. By contrast, between 2010 and 2022, 35 (65%) papers meeting the inclusion criteria were published. The greatest number of studies (n = 8, 15%) were published in 2019. However, six (11%) studies were published in 2008, which was the largest annual number for the decade 2000–2010. This shows an increased trend in screening for depression and anxiety in Indigenous populations and sharing the findings through publication. Figure 3 illustrates the number of studies (count) per year as well as the cumulative count overall.
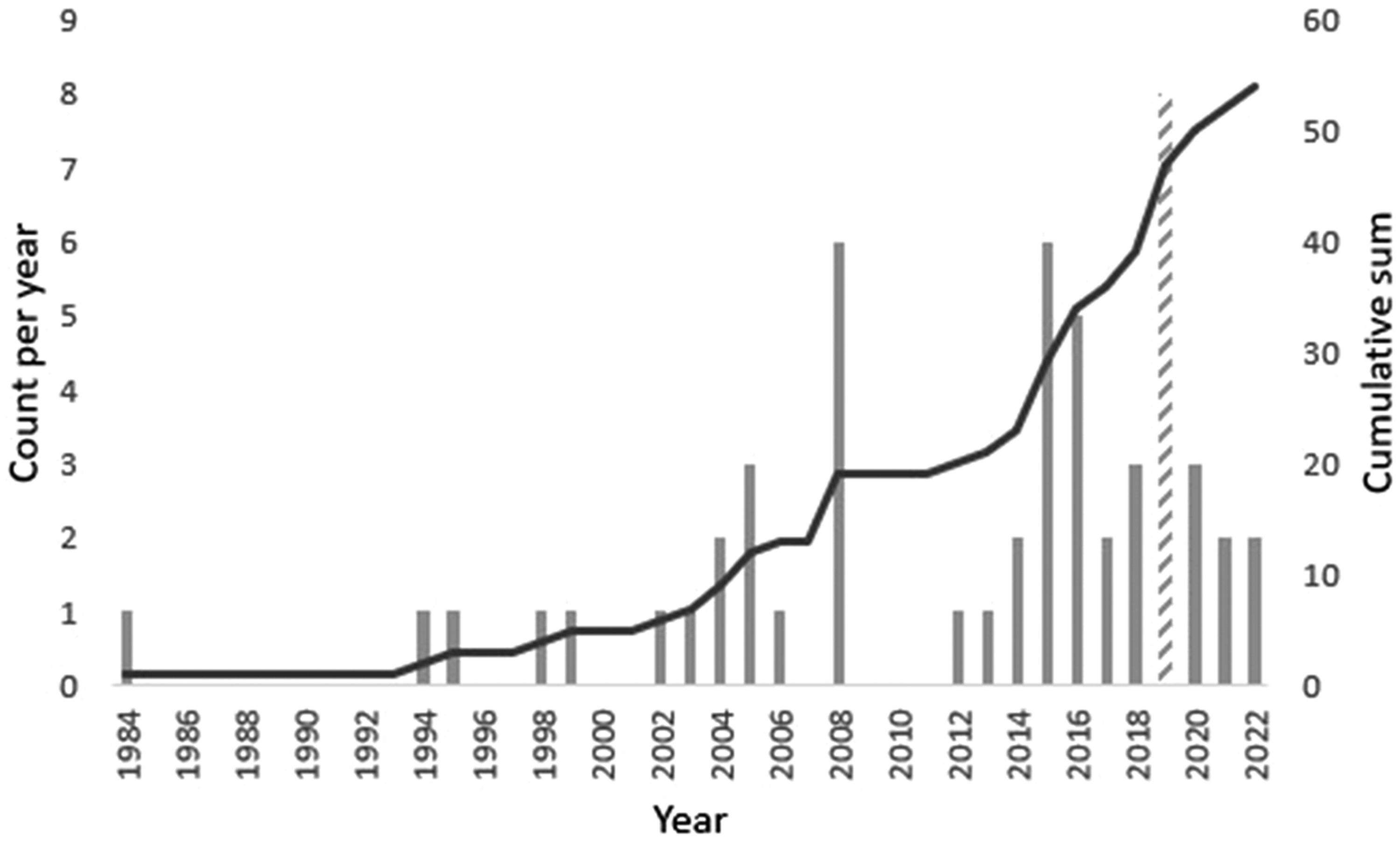
Publication dates of the included studies.
Most studies took place with participants recruited from their community (n = 43, 80%). Participants recruited from primary health contexts accounted for the remainder of the studies (n = 12, 22%). Two studies took place in both community and primary care settings, which is why the percentages above equal more than 100%. No studies took place in acute care settings. One study did not report its setting. Four studies were conducted with participants who identified as female (7%) and one (2%) with males. However, most studies (n = 49, 90%) took place with male and female participants. In 28 studies the mean age or age range of participants was above 40 years.
Tool type
The depression and anxiety screening tools identified in the studies included in this scoping review were divided into four categories. Standard tools such as the PHQ-9, Kessler 10 (K10) and Center for Epidemiological Studies Depression Scale (CES-D) used in their unmodified form were included in category 1. For the purposes of this scoping review, standard tools are defined as those that have been developed in western countries and validated predominantly with people of an Anglo/European background. For example, the PHQ-9 was developed in the United States during the late 1990s and validated with participants, 79% of whom identified as White and 66% as female (Kroenke et al., 2001). Likewise, the CES-D (Radloff, 1977) was developed in the United States with a predominantly White population (Comstock & Helsing, 1977). A standard tool was used in most studies (n = 46, 85%) to screen for depression and anxiety in Indigenous peoples globally.
Category 2 included two studies that modified the standard tool by directly translating it into another language. For example, the PHQ-9 has been translated into more than 100 languages (Kroenke, 2021). Two studies (4%) included in this scoping review fitted into this category.
Adaptations of standard screening tools to make them more culturally appropriate (category 3) were used in six (11%) of studies. For example, Almeida et al. (2014) developed the Kimberly Indigenous Cognitive Assessment–Depression (KICA-Dep) by adapting the PHQ-9 for use with older Indigenous peoples from the Kimberly and Derby regions of Western Australia.
Finally, only one study used a depression and anxiety screening tool specifically designed for a non-western country (category 4). Faruk et al. (2021) used a depression scale and an anxiety scale specifically developed for the Chakma and Marma peoples of Bangladesh, to screen Indigenous peoples of the Chittagong Hill Tracts.
Tools used
Thirty-three different tools were used in the studies included in the scoping review. They were grouped into two categories: screeners and intermediaries. Screening tools are designed to identify people exhibiting signs of disturbances in their mental well-being who need to be referred to a doctor or psychiatrist for diagnosis and treatment (Cairney et al., 2007; Roberts & Vernon, 1983). They are designed to be used by a range of health professionals and take a short time to complete and are consequently economical (Roberts & Vernon, 1983). In contrast, intermediaries such as the Composite International Diagnostic Interview (CIDI) and MINI-International Neuropsychiatric Interview (MINI) take longer to complete and must be administered by a trained individual who is familiar with the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) classification and diagnostic criteria. However, because they do not have to be administered by a psychiatrist, they are suitable for use in community and primary healthcare settings. Table 2 presents the three most used screening and intermediary tools and their adaptations.
Top three tools used to screen depression and anxiety in Indigenous populations.
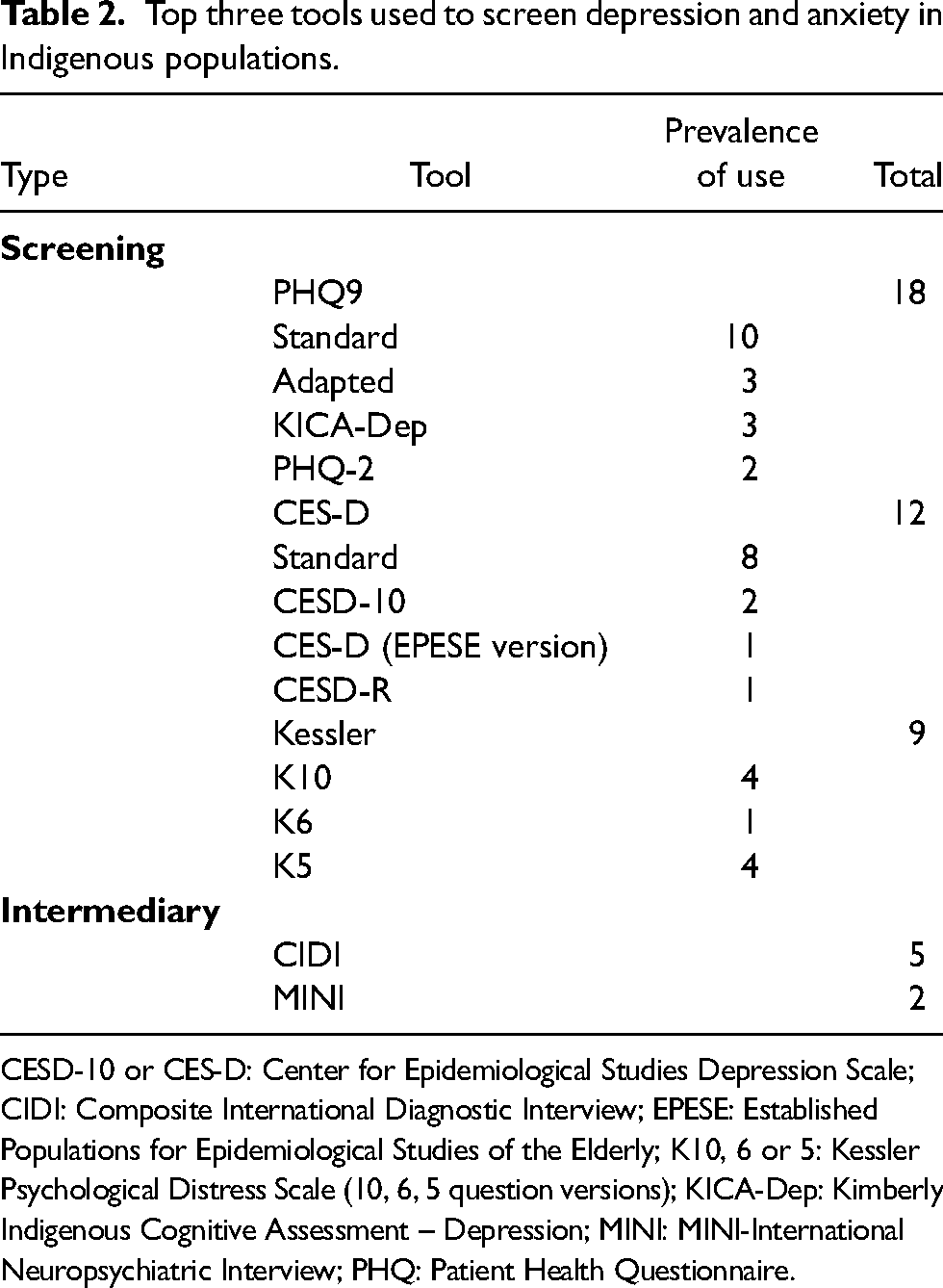
CESD-10 or CES-D: Center for Epidemiological Studies Depression Scale; CIDI: Composite International Diagnostic Interview; EPESE: Established Populations for Epidemiological Studies of the Elderly; K10, 6 or 5: Kessler Psychological Distress Scale (10, 6, 5 question versions); KICA-Dep: Kimberly Indigenous Cognitive Assessment – Depression; MINI: MINI-International Neuropsychiatric Interview; PHQ: Patient Health Questionnaire.
The standard tool used most often was the PHQ-9 (18 times). In its standard form, this tool was more commonly used for clinical studies determining the interactions between depression and diabetes (Davis et al., 2015; Sahota et al., 2008; Taylor et al., 2017) and sleep (Froese et al., 2008). It was also used to evaluate clinical interventions (Montag et al., 2015; Tu et al., 2019), examine distal and proximal factors related to depression and population prevalence in an Indigenous population in Panamá (Walker et al., 2019) and in the United States (Kading et al., 2015; Walls et al., 2016). Adapted forms of the PHQ-9 have been used with Australian Aboriginal and Torres Strait Islander populations (Almeida et al., 2014; Esler et al., 2008; Getting It Right Collaborative, 2019; Russell et al., 2022; Shen et al., 2018; Wong et al., 2021).
The CES-D was the second most frequently used standard tool (12 times). This screening tool was used in eight studies in its standard form and four in an adapted form. The CES-D (and its adapted forms) was used almost exclusively in studies conducted with community samples investigating the correlation between depression and other lifestyle (Benoit et al., 2016; Evans-Campbell et al., 2012; Kaholokula et al., 1999) and/or environmental/social factors (Hsieh et al., 2020; Ing et al., 2019; Letiecq et al., 2008; Roh et al., 2015; Whitbeck et al., 2002). Depression prevalence was also determined using the CES-D (Bell et al., 2005) as well as the psychometric properties of other scales using the CES-D as a validator (Gray et al., 2019). Finally, Walls et al. (2016) used both the PHQ-9 and CES-D to describe the mental well-being of American Indians.
The Kessler screening tools (K10, K6, K5) were the third most commonly used tool; being cited nine times. They have been used in Indigenous population-based screens (ABS, 2006, 2019; CDC, 2019–2022; FNDGC, 2018), as well as more general studies (Firestone et al., 2015; Isaacs & Lampitt, 2014; Williamson et al., 2016). Walker et al. (2019) also used the K6 to measure serious psychological distress with the PHQ-9 in a primary health and community sample in Panamá.
Intermediary tools such as the CIDI and the MINI have been used five and two times, respectively. Both tools have been used as a stand-alone (MacMillan et al., 2008; The MAGPIe Group, 2005; Whitbeck et al., 2006) or with other screening tools (Evans-Campbell et al., 2012; Walls et al., 2016).
Some studies used more than one tool, especially when validating adapted tools. For example, the Getting It Right Collaborative (2019) validated Brown et al. (2016) adapted PHQ-9 against a MINI. Gray et al. (2016, 2019) used the Beck Anxiety Inventory (BAI), Beck Depression Inventory (BDI), CES-D and Tri-Ethnic Depression Scale to evaluate psychometric properties of these scales for Northern Plains Indians.
Reason for tool use
Tools used to screen depression and anxiety were categorised into nine reasons for use: determining prevalence; assessing the psychometric properties (including validation); population comparison; tool development; identifying of mental health needs; evaluating interventions; generating new knowledge; establishing the relationship of depression with (an)other variable(s); and establishing the relationship of anxiety with (an)other variable(s).
The greatest use of depression screening tools has been to determine the correlation between it and other lifestyle and/or environmental and/or social factors. Twenty-nine studies (54%) were categorised by this use. The second highest use (n = 15, 28%) was to determine the prevalence of depression and/or anxiety in Indigenous peoples. Often, these studies were responding to the observation that Indigenous peoples experience increased mental health support needs, and therefore were looking to establish prevalence rates. Comparing depression and/or anxiety in different population groups (n = 8, 15%) was the third highest reason for use. Assessing the psychometric properties (including validation) (n = 5, 9%) of tools was the fourth highest reason for use, whereas generating new knowledge (n = 3, 5%) was fifth. Fewer studies used screening tools to identify mental health needs (n = 2, 4%), develop new tools (n = 2, 4%), evaluate an intervention (n = 2, 4%) and determine the correlation between anxiety and other lifestyle and/or environmental and/or social factors (n = 1, 2%). Some studies were focused on more than one reason for using a depression and/or anxiety screening tool, consequently the totals are greater than total number of studies in the data set and percentages are greater than 100.
Reliability and validity
The overarching quality of a screening tool is determined by its reliability and validity for the population it is being used with (Alarcón et al., 2002; Sorlie et al., 2018). Given its importance, surprisingly few authors determined tool reliability (n = 16, 30%) and even fewer validity (n = 6, 11%). However, more authors measured reliability as opposed to assuming it (n = 5, 9%) based on the findings of other studies. In contrast, more authors assumed tool validity (n = 10, 19%) rather than measuring it in their sample. The number of studies that did not address tool reliability (n = 33, 61%) or validity (n = 37, 69%) is a significant limitation given that the majority used standard tools not originally developed for Indigenous populations.
Discussion
The findings of this scoping review highlight that standard tools, the PHQ-9, CES-D and the Kessler Psychological Distress Scale (and their respective adaptations), remain the most frequently used, despite calls for mental health screening of Indigenous peoples to be achieved using culturally appropriate tools (Adams et al., 2014; Brinckley et al., 2021; Gomez Cardona et al., 2021; Le Grande et al., 2017). The findings of this scoping review also respond to a recent call to critically assess mental health theories, models and interventions for, and with, Indigenous peoples (Gone & Kirmayer, 2020), by providing evidence of current approaches to screening for depression and anxiety.
Contexts for the use of depression and/or anxiety screening tools
Half of the data set for this scoping review contained studies conducted in the United States (including Hawai’i). These studies were predominantly conducted with participants recruited from the community and were more likely to be investigating the relationship of depression with lifestyle, environmental or social variables. The second highest number of studies came from Australia. Similarly, Australian studies were predominantly conducted with participants recruited from community settings and also investigated the relationship of depression with other variables. However, proportionally more studies in Australia were focused on validation or adaptation/new screening tool development when compared with the United States. No tool adaptation for Indigenous peoples took place in the United States and only two studies that met the inclusion criteria for this scoping review focused specifically on validation (Gray et al., 2016, 2019). Gray et al. (2016, 2019) also validated depression and anxiety screening tools [BDI, BAI, CES-D, Tri-ethnic Centre Depression Scale, Symptom Checklist-90-Revised (SCL-90-R)] that, according to the findings of this scoping review, are less commonly used. By contrast, Australian validation and new tool development studies were focused on adapting the most used tool – the PHQ-9 – for use with Australian Indigenous peoples.
Cross-cultural adaptation of standard tools
As stated previously, the quality of screening tools is dependent on their reliability and validity. Australian studies that met the inclusion criteria for this scoping review focused on cross-cultural adaptation of the PHQ-9. Rationales for tool adaptation have been focused on cultural acceptability, which includes ensuring cultural relevance and revising the wording of each item. For example, the Getting It Right Collaborative (2019) validated the previously adapted PHQ-9 (Brown et al., 2016, 2012) for use with Aboriginal and Torres Strait Islanders living in urban, rural and remote Australia. When reviewing adaptations made to the PHQ-9 by Brown et al. (2012, 2016), the Getting It Right Collaborative noted that many key symptoms of western conceptualisations of depression were not present in the Central Desert Aboriginal men that participated in Brown et al.’s (2012, 2016) studies. By contrast, Aboriginal men reported ‘anger, weakened spirit, irritability, excessive worry, rumination, and drug or alcohol use’ (Getting It Right Collaborative, 2019, p. 24). To make the PHQ-9 culturally relevant these symptoms needed to be reflected in the adapted PHQ-9. In addition, the construct of hopelessness was omitted because participants felt that their perceptions of depressed mood encapsulated it (Brown et al., 2012).
Making the PHQ-9 culturally relevant for Australian Aboriginal people has also meant that additional items have been included in the screener. For example, Almeida et al. (2014) split the item about suicidal ideation making their KICA-Dep adaptation of the PHQ-9 an 11-item screener. In addition, in the precursor to the publication included in this data set (Esler et al., 2008), Esler and colleagues included an item about anger in their modification of the PHQ-9 (Esler et al., 2007). Also, changes to word use in some items included using the word sad rather than depressed (Esler et al., 2008), and use of the words slack and shame (Almeida et al., 2014) for feelings of lethargy and guilt, respectively.
Finally, cross-cultural adaptation makes the screener more acceptable. This was highlighted by both Esler et al. (2008) and the Getting It Right Collaborative (2019) who stated that the adapted PHQ-9 screener that they used was acceptable to their Aboriginal and Torres Strait Islander participants. Consequently, tools that have undergone cross-cultural adaptation are more likely to be appropriate for the Indigenous population for which they have been validated compared with standard tools.
Standard tools may continue to be used because researchers and practitioners in this area do not have the resources to cross-culturally adapt or develop new tools for screening for depression and/or anxiety in Indigenous populations. As studies that have undertaken these activities have indicated, it is critical that Indigenous peoples are involved in this process (Brown et al., 2013; Carlin et al., 2019; Janca et al., 2015). Ideally, Indigenous people should lead the work so that both Indigenous conceptualisations of depression and anxiety, as well as data interpretation, are undertaken through a culturally appropriate lens (Chan et al., 2021). Therefore, key resource issues such as relationships with Indigenous peoples, cultural knowledge, and the associated time and money required to undertake this work may impact on the ability of some researchers and practitioners to either cross-culturally adapt and validate a standard tool or develop an entirely new one.
Implications of the findings
The most used screening tool was the PHQ-9 and its adaptations. Although two adaptations have already been made for specific groups of Indigenous Australians, researchers should consider adapting the PHQ-9 either as a language translation or cross-cultural adaptation and validating it for their population as part of their research. We acknowledge that there are resourcing implications for projects when this takes place, but we argue that it is necessary because of the cultural inappropriateness of standard tools.
Many authors (Brinckley et al., 2021; Brown et al., 2013; Butler et al., 2007; Chan et al., 2021; Janca et al., 2015; Le Grande et al., 2017; Nelson & Wilson, 2017) have highlighted the inappropriateness of using standard tools to screen mood and anxiety in Indigenous peoples. Indigenous peoples conceptualise health and well-being holistically, which is interconnected and interrelated with the well-being of their communities and their land (Gall et al., 2021; Sørly et al., 2021; Wilson & Richmond, 2009). Consequently, the individualistic western model does not capture Indigenous holistic conceptualisations of well-being (Le Grande et al., 2017; Wilson & Richmond, 2009). In addition, Brown et al. (2013, p. 2) highlighted that ‘labelling Indigenous people with western diagnostic classifications without assessing their equivalence, relevance, acceptability or utility serves little purpose if such labels are devoid of the context and realities’ of their lives. Also, cultural understandings of word use are different (Brinckley et al., 2021; Brown et al., 2013; Chan et al., 2021; Snodgrass et al., 2017), as are expressions of distress (Kohrt et al., 2014; Snodgrass et al., 2017). Furthermore, questionnaires written in the English language that rely on written responses may be affected by literacy and education levels, as well as different conceptualisations of time and numbers (Janca et al., 2015). Hence, the findings of this review indicate that more work is required to support the needs of Indigenous peoples, starting with the development, validation and use of culturally appropriate screening tools.
Findings related to the broader study which scoping review is situated
This scoping review identified one paper (Taylor et al., 2017) that used PHQ-9 to investigate the relationship between diabetes and depression in Torres Strait Islanders living in the Torres Strait. The authors acknowledged that the PHQ-9 was not validated for use with the population. Another paper (Russell et al., 2022) identified that the Geriatric Anxiety Inventory (GAI) and KICA-Dep were also culturally inappropriate for use with Torres Strait Islanders living in the Torres Strait. This scoping review therefore presents evidence for the importance of cross-culturally adapting or creating a new tool/approach to screen depression and anxiety (the mental well-being) of people living in the Torres Strait or the Northern Peninsula Area of Australia.
Limitations of the scoping review
Including only English language publications was a limitation of this study, because we may have missed studies in other populations globally. For example, there are a limited number of studies from the countries of South America included in this scoping review, which may have been published in other languages such as Spanish. Therefore, collaborating with researchers who speak other languages could have enhanced the global reach of the scoping review.
Conclusion
This scoping review gathered evidence of the tools used to screen depression and/or anxiety of Indigenous peoples globally. The overarching finding indicates that standard tools developed using the western biomedical model of mental health predominate when screening depression and anxiety in Indigenous peoples. However, the cross-cultural adaptation and validation of standard tools has begun to emerge in the past decade, with Australian researchers leading this work. This is important given identified issues with the cultural appropriateness of standard tools used with Indigenous peoples including: holistic conceptualisations of health and well-being, cultural expressions of distress, word use and written English language literacy.
Implications of the scoping review findings indicate that national governments, researchers and clinicians should review their approach to screening depression and anxiety in Indigenous peoples. The PHQ-9 has been adapted in Australia. Population-based screening of Indigenous peoples by governments using standard tools such as the K10 and, in Australia, the K5, would benefit from cross-cultural adaptation. This work has already been done in Australia by Brinckley et al. (2021) – not included in the data set because participants included people <18 years – which could be used as a model by other governments.
Opportunities for future research in this area are provided by our narrow approach to selecting the inclusion criteria for this scoping review. The inclusion criteria selected excluded publications that did not provide an outcome of the screening tool used with Indigenous peoples. For example, a prevalence of depression and/or anxiety disorders, the identification of issues, the outcomes of an intervention or comparison data. This choice excluded some studies that reported approaches to adapting culturally appropriate tools or developing new ones. In addition, the validity, specificity and sensitivity of tools were not reported in this scoping review. Therefore, systematic reviews of approaches to cross-cultural adaptation or the development of new tools, as well as their validity, specificity and sensitivity present potential avenues for further research.
Supplemental Material
sj-pdf-1-tps-10.1177_13634615231187257 - Supplemental material for Screening depression and anxiety in Indigenous peoples: A global scoping review
Supplemental material, sj-pdf-1-tps-10.1177_13634615231187257 for Screening depression and anxiety in Indigenous peoples: A global scoping review by Kathryn Meldrum, Ellaina Andersson, Torres Webb, Rachel Quigley, Edward Strivens and Sarah Russell in Transcultural Psychiatry
Footnotes
Acknowledgements
The authors thank Janet Caterall subject-specific liaison librarian for support with the database searches.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was funded by The Ian Potter Foundation (Grant Number 31110728).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.