
Abstract
Chronic, hard-to-heal wounds are a major public health concern, putting a strain on healthcare systems and causing significant psychosocial distress for patients. This article details a project that engaged 11 people with chronic wounds and their care partners as subject matter experts. We used a visual method called analytic sketching to analyze their experiences. Analytic sketches are a cognitive tool that helps researchers identify patterns, gain deeper insights, and uncover experiences that might not be obvious from text alone. This approach enhances the trustworthiness and rigor of the findings, especially when combined with verbal data and techniques like participant checking. The sketches visually revealed several key psychosocial themes. Color was used to depict the pain experienced by patients and their caregivers, the importance of support, and a sense of chaos. Ink lines and strokes highlighted the frustration and communication failures with healthcare professionals and the barriers to care. Finally, visual representations were presented to express a collective experience of navigating the complex political realities of wound care within a publicly funded system. By showcasing six representative sketches, this article demonstrates the effectiveness of using arts-based methods to analyze complex healthcare experiences. The findings have important implications for both clinical practice and policy development, offering a more holistic understanding of living with chronic wounds.
Introduction
The increasing prevalence of chronic/hard-to-heal wounds has become a global public health issue driven by aging populations and the rising burden of chronic conditions such as diabetes, peripheral vascular disease, venous insufficiency, and frailty. These wounds present both a significant medical challenge and a major public health concern, affecting millions of people worldwide and straining healthcare systems due to the prolonged resources required for long-term treatment. Long-term care treatment includes frequent dressing changes and the significant involvement of healthcare providers time, particularly nurses, in implementing care plans (Queen and Harding, 2023).
In 2019, the estimated global expenditure on wound care (measured in Purchasing Power Parity—PPP, International $ Billion) was highest in the USA ($126.86 billion), followed by China ($26.95 billion), Japan ($18.90 billion), Germany ($15.97 billion) among others. Canada’s estimated expenditure was $6.9 billion, ranking seventh in global spending for all types of wounds (Queen and Harding, 2023). These figures highlight the substantial financial burden of wound care across healthcare systems and emphasize the need for continued monitoring and policy responses to reduce costs and improve patient outcomes.
Beyond the economic strain, people living with hard-to-heal wounds face severe psychosocial repercussions, including stigmatization, social isolation—often due to pain, odor, or mobility limitations—economic hardship, depression, stress, and anxiety (Costa et al., 2022; Costa and Camargo-Plazas, 2023). These widespread challenges underscore the urgent need for global public health strategies that address both the clinical and psychosocial dimensions of wounds.
Despite the far-reaching impact of hard-to-heal wounds, research suggests that healthcare professionals lack a comprehensive understanding of the everyday experiences and psychosocial effects of living with these conditions (Costa et al., 2022). This knowledge gap persists even as health models draw attention to the need for person-centered care, recognizing that effective treatments must align with patients’ lived experiences and priorities (Tringale et al., 2022). Addressing this issue requires qualitative research methodologies that amplify the voices of those affected, ensuring that their perspectives shape more inclusive and responsive public health policies.
In this article, we employed digital storytelling (DST) as a method for data collection. DTS is a participatory research method that combines narrative, imagery, and sound to convey personal experiences in a compelling and accessible format (Chan and Sage, 2021). By engaging people with hard-to-heal wounds as subject experts, this approach places their voices, words, and lived experiences as central to the research process. The digital stories analyzed in this study were collected through the initiative “Our Voices Our Stories,” co-founded by the last author in 2021, which aimed to amplify the narratives of individuals experiencing hard-to-heal wounds. Building upon this work, we employed sketching as an analytic tool, offering a unique approach to understanding narrations of experience. In this article, we focus on analytic sketching and discuss how it informed critical insights about the delivery of wound care.
Background of study
Leveraging storytelling to inform healthcare practice and policy
In health research, there is growing recognition of the importance of engaging patients and care partners as active participants, while honoring their lived experiences (Easley et al., 2023). The inclusion of storytelling in healthcare marks a shift from a paternalistic model—where patients are viewed as passive recipients of care—toward an empowerment-based approach, in which patients actively participate in their own care and decision-making processes.
The concept of narrative agency is central to this shift. In The Wounded Storyteller, Frank (2013) argues that when individuals share their own stories, they not only articulate their personal experiences but also challenge dominant cultural narratives that position patients as passive objects of care. As Frank states, storytelling enables patients to reclaim their voices, fostering a sense of autonomy and engagement in the healthcare process. He writes: those who have been objects of others’ reports are now telling their own stories. As they do so, they define the ethic of our times: an ethic of voice, affording each a right to speak her own truth, in her own words (2013: xiii).
Storytelling is not only a personal act but also a political act and a practice. Stories can generate novel insights into addressing the complex social, emotional, and structural factors that influence health and well-being. Storytelling has the potential to inform health policy and best practices, extending its impact beyond clinical aspects such as wound management, dressings, and technology (Matthews and Sunderland, 2017). In health research, analyzing patient and care partner narratives is crucial in uncovering the social, emotional, and economic factors that shape both the experience of living with a wound for example, as well as the broader processes of healing and recovery.
Analytic sketching as an arts-based approach
This study employed an arts-based analytic method—specifically sketching—to interpret and analyze the narratives collected. Arts-based research is increasingly recognized for its ability to capture and materialize emotions, embodied experiences, and complex socio-political conditions, such as chronic illness (Harasymchuk et al., 2024). Arts-based research strategically integrates artistic practices—such as visual representation—into the research process to generate, analyze, and present data (Rose, 2023).
Analytic sketching utilizes drawing, mapping, or visual representation to examine qualitative data. Drawing or sketching involves the intentional creation of marks (e.g. words and images) as a form of expression and communication (Lyon, 2019). Words in research sketches function as graphic gestures, rather than textual components. These visuals are not intended for esthetic purposes but as strategic tools for communication (Pink, 2011). Elements such as color and shape contribute to meaning-making, conveying movement and emotions (Banks, 2011).
Analytic sketching is rooted in the interpretivist paradigm, which values subjectivity and seeks to uncover deeper meanings and rich insights from individual experiences (Alharahsheh and Pius, 2020). Research evidences that analytic sketching: facilitates the identification of recurring themes, patterns and emotions (Leavy, 2018); organizes complex data by making relationships between concepts more apparent (Martikainen and Hakoköngäs, 2023); and supports the iterative development of theoretical insights from data (Kovats, 2019). Visual approaches to research can also make qualitative data more accessible (Wheeldon and Ahlberg, 2011) and enhance the exchange of ideas throughout the research process (Phillips and Bellinger, 2011). Analytic sketching is particularly effective in analyzing narrative data due to its ability to capture the complexity and depth of personal stories (Causey, 2017), while valuing the embodied and subjective nature of meaning-making (Pink, 2011). Researchers have successfully used analytic sketching to explore sensitive or complex issues. For example, it has been used to analyze historical data on the bodily regulation of sexuality (Phillips and Powell, 2025). As Kovats explains analytic drawings, “provide a focus, something to rest on, a place to drop an anchor—giving time and space. . .” (2019, 0.35). They give researchers a unique balance of intimacy and distance, helping slow down the analytic process to engage more deeply with their data and notice details they might have otherwise overlooked. This method fosters reflexivity by encouraging researchers to critically engage with their data, reflect on potential biases, and refine their interpretations (Pink, 2011).
While analytic sketching offers many strengths, it also presents some limitations and challenges. This method is time- and resource-intensive, adding a demanding stage to the analysis process, particularly when meticulous integration of verbal and visual data is required. Another limitation is the potential for misinterpretation. As Glegg (2019) notes, drawings can be ambiguous, and without a verbal explanation, researchers risk misinterpreting the intended meaning of a sketch. This highlights the necessity of reflexive discussions between the artist and researcher(s).
Furthermore, like many qualitative methods, the findings from analytic sketching can be subjective and highly context-specific, making generalizations difficult. However, as this research was interpretivistic, the focus was on the depth of interpretation rather than generalizability. Nonetheless, it is crucial to carefully navigate the subjective meanings embedded in visual data. In this study, we re-watched the video interviews after completing the sketches to ensure alignment between the drawings and participant experiences. Furthermore, to confirm that the drawings accurately reflected their stories, each participant validated their corresponding sketch. This process helped mitigate any misinterpretation while strengthening the rigor of our approach.
Methods
Summary: This section describes how the data was gathered and analyze. This study collected 11 diverse digital video stories from patients and caregivers living with hard-to-heal wounds. These stories were gathered through interviews and then analyzed using an arts-based research method where an artist created interpretive sketches for each narrative to gain deep, nuanced insights.
Participants recruitment
In September 2021 video stories were gathered from individuals living with and managing different types of hard-to-heal wounds (e.g. diabetes-related wounds, pressure injuries, venous leg ulcers). For this analysis, we included 11 digital stories that were publicly posted on Wounds Canada’s website and made accessible to a broad audience. Wounds Canada is a National and not-for-profit organization dedicated to promoting and advocating for evidence-informed wound care. As the community partner for the initiative “Our Voices Our Stories” led by the last author (IGC), one of the roles of Wounds Canada (2022) in this initiative is to host and disseminate all stories in its website and social media.
Participants were recruited through different ways: (1) Wounds Canada’s social media and newsletter by inviting those with lived experience or their care partners to complete a form if they wanted to be contacted. (2) Wound care clinicians affiliated to Wounds Canada or in its directory sending an e-mail and requesting to share the recruitment efforts.
Sample and rationale
A total of 11 digital stories were included in the analysis. The storytellers represented a diverse range of lived experiences, including those living with pressure injuries (n = 5), diabetic foot ulcers (n = 1), malignant wounds (n = 1), burn injury (n = 1), skin tears (n = 1), moisture-associated dermatitis (n = 1), and delayed surgical wound healing (n = 1). Three participants were caregivers for their parents and one a caregiver for a child. This diversity provided a rich array of perspectives on wound prevention, treatment, and the systemic barriers encountered in care pathways.
A sample size of 11 stories was appropriate for this qualitative, arts-based design, which prioritizes depth, creativity, and meaning-making over numerical representation. This number enabled us to capture diverse perspectives from patients and caregivers across multiple wound types and care contexts, while remaining manageable for a rigorous arts-based analytic process. The sample size supported an iterative cycle of listening, reflecting, and visual interpretation through drawing, allowing the research team to engage deeply with each narrative and generate nuanced insights.
Ethical considerations
Individuals willing to contribute their experiences were required to read and sign an informed consent form before participating. To maintain participant autonomy and accuracy, each digital storytelling (DST) narrative was reviewed and approved by the respective participant before being made publicly available. Participants had the opportunity to confirm that their digital story accurately reflected their experiences before it was uploaded to the Wounds Canada’s website. Lakehead University Research Ethics Board reviewed the project for the purpose of story collection, providing a waiver letter and providing ethical approval for analytical sketching (REB# 1470464).
Story collection
Participants’ stories were collected through individual semi-structured interviews that focused on the participant’s living with a complex wound and their experiences with health and social services. The interview guide was informed by the last author’s experience in providing care for people living with wounds for over 20 years as well as by social constructivism, which navigates to the past to understand what happened in the present (Charmaz, 2014). Interviews were conducted and recorded via Zoom Platform; each interview lasted between 60 and 90 minutes. To capture the essence of each participant’s story, the digital videos were professionally edited with the direction of each respective participant.
Artistic Interpretation of narratives in Sketching format
Once the stories were reviewed and approved by the participants and made publicly available, a graduate social work student (second author), who is also a visual and textile artist—henceforth referred to as “the artist”—was engaged. The artist is versed in interpretivist research methods. The artist did not review or engage with the data prior to creating the illustrations. The artist was instructed to “respond to the data visually” following the approach outlined by Jellema et al. (2023), in which each sketch is created during or immediately after engaging with the data. The artist describes her approach: The first sketch in pencil was done right after the first hearing of the story. On the very next day, I listened to the story again, sometimes stopped the video and watched certain parts over, adding more details onto the sketch and colouring as I listened to the story.
For the more chaotic sketches, the artist noted that she listened to the full story several times.
Data analysis and interpretation of the sketches
After the sketches were completed, Mitchell et al.’s (2011) guidance was followed whereby each sketch is read alongside the corresponding story, prompting further analysis as well as clarifying elements of the drawing or sketch. In keeping with the method of research sketching, the first and second authors engaged in iterative cycles of reflection, refining their interpretations with each additional sketch and conversation. These cycles of reflection served as opportunities to critically examine assumptions and minimize bias. This stage of analysis adds depth to the details in the story that have been highlighted by the artist, and it allows the researchers—who are not artists—to revisit their own interpretations and visualize analytic points they had not previously noticed when viewing only the videos. During this stage, the first author re-watched all of the stories. While all the sketches include elements of representational transparency, some are more multifaceted and complex, requiring close reading alongside the story for fuller intelligibility. The sketches do not tidy up or summarize the participants’ stories, rather they invite engagement with the emotional complexity of a hard-to-heal wound, and in this way benefit from another layer of interpretation added by the sketches. This is also part of the iterative process inherent in research sketching. This additional layer of interpretation—the visual analysis—is represented by a sample of six sketches accompanied by our interpretive commentary.
Findings
Summary: As this study followed a qualitative paradigm focused on in-depth understanding of specific phenomena, the full sample was analyzed. We present a set of six sketches that are representative of the entire sample. The six selected sketches convey both the uniqueness of individual narratives and the common experiences shared among participants. Three key analytical dimensions emerged: the use of color, ink lines and strokes, and visual imagery.
a. Color symbolized pain—experienced both by individuals with wounds and their care partners—as well as the role of support in healing and the experience of chaos within the healthcare system.
b. Ink lines and strokes reflected shared frustrations, communication breakdowns with healthcare professionals, and systemic barriers to care.
c. Visual imagery illustrated the collective participant experience, emphasizing the political realities of wound care within a publicly funded healthcare system.
The following sections explore each of these three dimensions in greater detail.
The use of color: Contradictions of the color red
In this section, we describe how the use of color by the artist revealed key experiences, including physical pain, social support, and chaotic care.
Pain
One color in particular stood out in the analytic sketches: red—a dramatic vibrant hue. In these sketches, red is a complex stroke and multilayered visual element. The artist explained that she chose red to reflect the physical and psychological pain conveyed in the stories. It serves as both a literal and symbolic representation of having a wound. After all, blood is red, and in the sketches, red droplets precisely mark the exact location of the wound (Figures 1, 3 and 5).
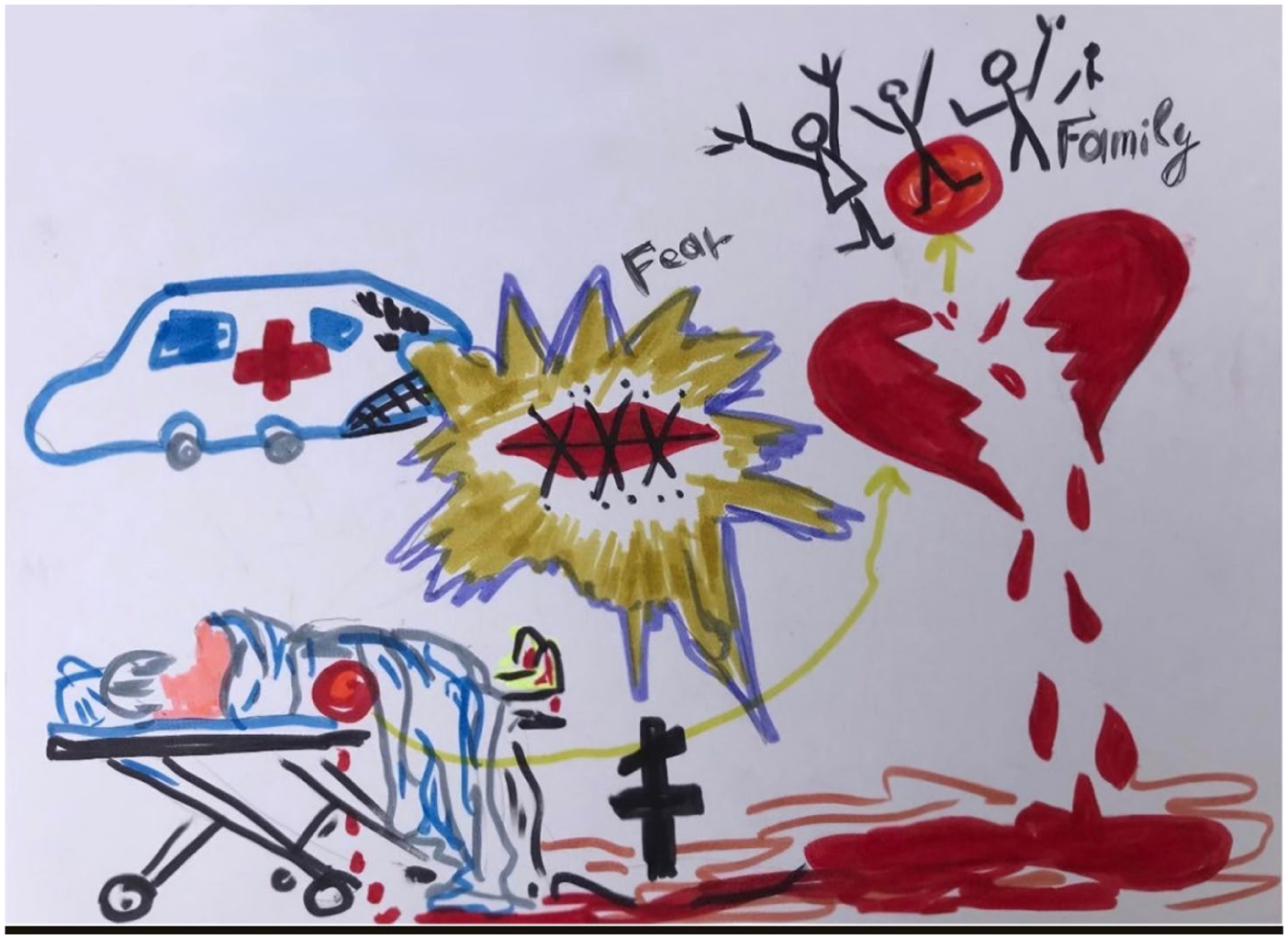
Sketch depicting the experience of a care partner of a loved one with pressure injury.
While red represents the reality of the wound, it also symbolizes the physical and embodied experience of living with it. However, in contrast to its association with suffering, red also conveys connection—relationships with family care partners and loved ones. Many of the sketches feature red hearts—some whole, some broken—underscoring this dual symbolism.
For example, in Figure 1 which depicts a care partner’s experience, a loved one is shown lying on a hospital bed with their back turned to the viewer, as blood leaks from their coccyx wound (i.e. pressure injury). Their legs are also wounded and bleeding. On the right side of the sketch, blood from the wound merges with the blood from a broken heart, visually conveying that the suffering extends beyond the individual with the hard-to-heal wound. This imagery illustrates how a loved one’s physical wounds leaves lasting psychological scars on family members, who carry the pain of knowing someone they deeply cared for endured profound suffering—both physically and emotionally.
The role of support in healing and recovery
In the analytic sketches, the color red serves as a metaphor for both love and support, while also symbolizing anger and frustration. Participants described the integral role that family and pets played in their healing journey, providing emotional and practical support as they coped with the challenges of living with hard-to-heal, painful wounds. Family members were often a source of strength, helping them navigate the many difficulties associated with accessing care for their pressure injuries. In contrast, some participants highlighted the emotional distress and additional challenges they faced when family support was absent. The lack of familial care not only exacerbated feelings of isolation but also complicated recovery, underscoring the profound impact of social and emotional support on wound management and healing.
Several participants emphasized the importance of seeking out a community of individuals who shared similar experiences with wounds, as this fostered a sense of connection, hope, and meaning. Others found emotional support and motivation through engagement in activities such as joining a gym or participating in a music group. Notably, individuals with hard-to-heal wounds underscored the critical role of family or community support in their recovery. Without such support, they expressed uncertainty about how to effectively manage their body injuries, highlighting the tangible and material contribution that family provided in facilitating their care. For instance, participants described how family members washed and cleaned their wounds, changed bloodied dressings, and took photographs to track progress and communicate with healthcare providers.
For care partners, love was also not only an emotional expression but also a tangible and material presence, playing a significant role during a family member’s hospitalization. Care partners ensured someone was always present at the hospital, brought in music to provide comfort, used physical touch to offer reassurance, and actively advocated for their loved one’s care. In the analytic sketch Figure 2, the loved one is depicted holding a big heart with his daughters’ names written on it. This visual representation symbolizes the profound and enduring support and love given to him by his family during his hospitalization.

Sketch depicting a care partner experience (daughter) of a loved one with pressure injury.
The multiple small hearts depicted in the sketch create a visual impression of the loved one surrounded by love. In listening to the story, this love emerges not only as an emotional expression but as a protective circle, shielding their loved one from a healthcare system perceived as inadequate. Other research participants similarly emphasized the need for protection within the healthcare system. One participant, for instance, expressed a profound sense of regret, feeling they had failed their loved one by placing trust in healthcare professionals who ultimately did not inform them about their loved one’s pressure injury. The injury was only discovered after the patient was transferred to another facility, by which point it was severely infected and had progressed into the bone.
Chaotic care and the fragility of healthcare structures
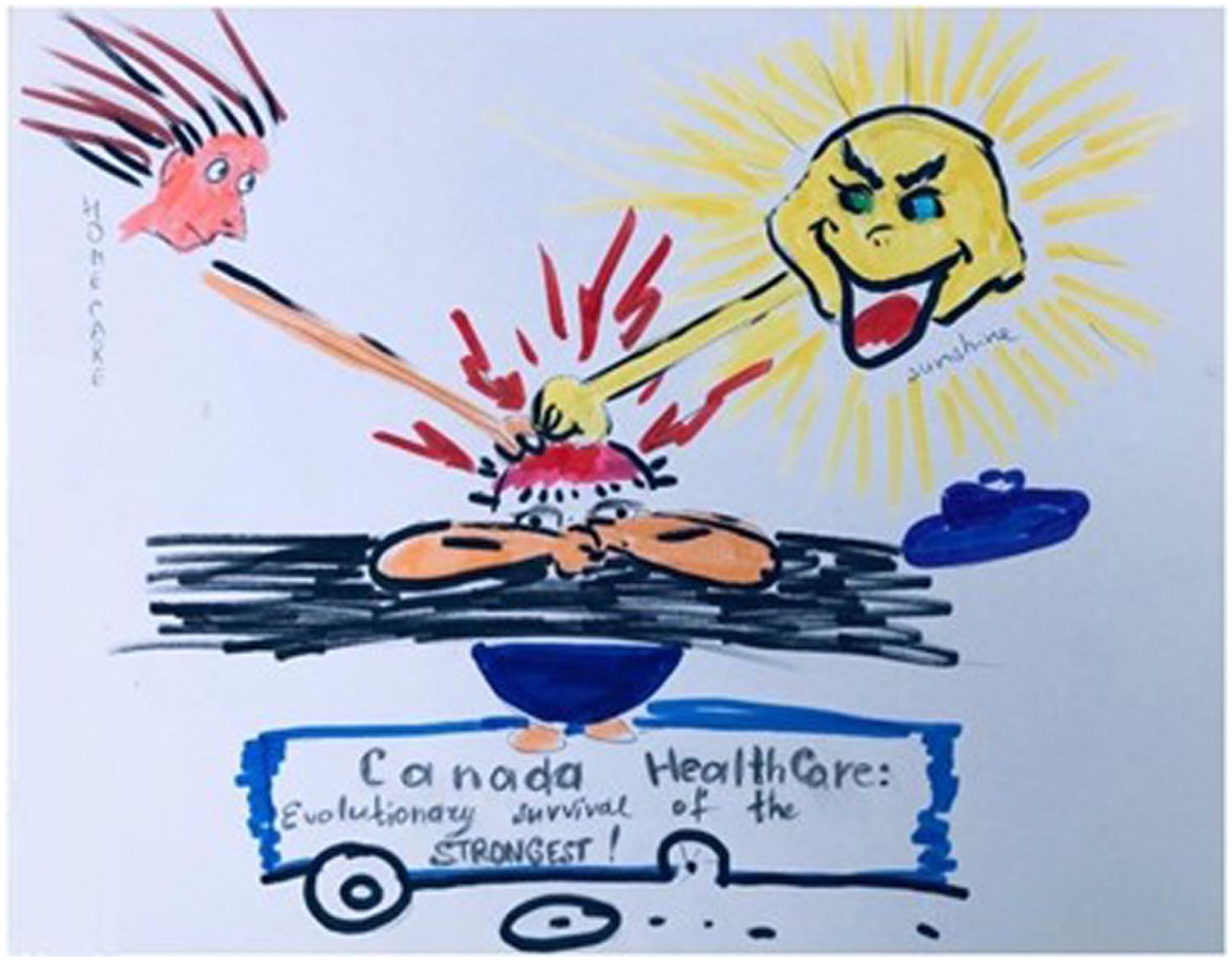
Red was prominently used as a symbolic color within the sketches, drawing attention to key themes within the stories. Red symbols signified aspects of the narrative such as the red cross, ambulance, hospital, and stop signs. These are all universal icons that resonate outside of the artist’s immediate context, transcending geographical and cultural boundaries. As analytic points, these symbols must be examined within the context of the story itself. For example, in Figure 3 the apple depicted in the sketch represents knowledge. This symbol takes on particular significance in the participant’s story, as she was a retired health professional who sustained a traumatic wound (i.e. skin tear) while gardening. Despite her professional background, she found herself needing to ask numerous questions and independently seek out specialized wound care knowledge.

Sketch depicting a story of patient who acquired skin tears during gardening.
The use of red also highlights the fragility of healthcare structures. In the sketch, the phrase “nurse superpower” is broken in two places, while a snake —a widely recognized symbol of healthcare—gazes leftward at the participant’s bleeding wound. In this sketch, the snake metaphorically represents the healthcare system, which has diminished participant’s “power” to access appropriate wound care. The participant, depicted with her mouth wide open, appears to be screaming—an evocative expression of the urgent need for specialized wound care support.
Other symbols, including some in red, featured grammatical strokes such as question marks and exclamation marks. These universal graphic gestures served as visual cues, alerting the researcher to critical moments in the narratives—instances of uncertainty, unanswered questions or expressions of frustration and chaos.
In Figure 3, the participant is depicted with numerous question marks above her head and shoulders, symbolizing her uncertainty despite her background as a retired nurse. Although she possesses medical knowledge, she struggles to feel confident navigating current best practices in wound care. The sun and the apple both personified with expressions of concerns, appear to ask whether she can manage the complexities of wound care on her own. Surrounding the question marks, the blending of clouds and land visually represents the chaos this participant experienced regarding the wound care protocols provided. This overarching theme of chaos and confusion was echoed by all research participants.
Similarly, in Figure 4 there are multiple question marks in a red-orange color that further emphasized a profound lack of knowledge regarding wound management. The artist described these symbols as representing the participants’ unanswered questions and the uncertainty surrounding their wounds. Chaos is palpable in this sketch, reflected in the artist’s emotional response. When listening to this care partner’s story the artist imagined a young woman holding a baby lost in deep woods, desperately searching for a way out. The only sign of direction is the word “HELP” painted green on the right side of the composition, signifying the urgent need for guidance and support in wound care.

Sketch depicting the story of a care partner (mother) of a son who developed skin lesions.
The care partner’s eyes are covered with a cloth, symbolizing the sense of darkness and uncertainty as she struggles to navigate the complexity of the healthcare system and communicate with professionals providing care to her son. Drawing on imagery from Ancient Greek mythology, the doctor is depicted as a god sitting atop Mount Olympus, holding a mobile phone. This representation reflects the care partner’s perception that the doctors treating her son communicated with her solely through phone calls, rather than seeing her loved one in person. This disconnect is further emphasized by the red broken line, signifying the fragmented and impersonal nature of these interactions. Surrounding and above the care partner’s head, numerous question marks illustrate the many unanswered questions she faced, reinforcing the broader theme of uncertainty.
The use of the inks lines and strokes
In this section, we examine how the use of lines and ink marks visually conveyed key experiences of frustration, failed communication, and barriers to care.
Stitched mouths: frustration and silenced voices in healthcare
Frustration was a recurring theme in the visual analysis, symbolized by the artist through small ink strokes representing stitches—stitches across closed mouths, signifying silenced voices. These stitched mouths appeared in multiple drawings (Figures 1 and 4), visually capturing a critical tension within the stories: the courage to ask questions or raise concerns to healthcare staff, alongside the fear that doing so might lead to worse care for themselves or their loved ones. As a result, care partners often chose to remain silent at key moments during their loved ones’ healthcare journeys, suppressing their concerns to avoid further complications or reduced quality of care.
For example, in Figure 1 a stitched mouth in the middle of the sketch —clearly a central feature of this story—is surrounded by sharp purple and yellow lines with the word “fear” positioned above it. This composition highlights the participant’s experience of feeling unable to speak up or ask questions about their care. Other participants similarly expressed fear that advocating for their loved one’s care could result in negative consequences, including a decline in the quality of care.
The overwhelming sense of frustration conveyed in these stories was directly linked to participants’ experiences within the healthcare system, particularly regarding poor communication. Specific concerns included: (a) lack of communication among healthcare professionals regarding wound care prevention and education; (b) disregard for boundaries, with home care professionals arriving late or failing to attend to scheduled appointments; (c) unhygienic wound care practice and; (d) rushed wound redressing changes that caused unnecessary pain. One participant described home care support as a “nightmare,” reinforcing the distressing and often chaotic nature of their experiences.
Bold, short strokes: Failed communication
Care partners reported that inadequate communication had direct material and physical consequences for their loved ones. Examples of this failure included loved ones not being repositioned in hospital beds (Figures 1, 2 and 5), leading to the development of pressure injuries, and families not being informed that their loved ones were receiving wound care visits. In some cases, families were not even told about the presence of preventable wounds until the wound had progressed to an advanced stage—at which point their loved ones had either been discharged home (Figure 5) or transferred to another hospital (Figure 2). Participants also highlighted the lack of health education provided to them, leaving them uninformed about the implications of wounds and how to properly care for them.

Sketch depicting the story of a care partner (daughter) of an Indigenous mother who developed pressure injury while recovery from hip surgery.
The absence of quality of care emerged as a significant theme in the analysis. For example, in Figure 5, a care partner is depicted with six hands, symbolizing her numerous attempts to secure medical care for her loved one. Three of these hands are stretched outward in a desperate plea for help, drawn using bold, short strokes of red. One hand reaches for wound dressings (top right), another extends to a hospital health provider, and a third reaches out to a wound care clinic specialist (top left). However, in this figure healthcare professionals are shown turning away from the care partner, symbolizing avoidance.
Participants also expressed profound frustration regarding the lack of timely and appropriate interventions for wound treatments. Common points of frustration included: (a) long wait times (ranging from days to weeks) before receiving wound care treatment; (b) a lack of a clear treatment plan following wound assessment; (c) inconsistent professional advice, leading to confusion about proper wound care, and (d) lack of referral to a wound care clinic thus ensuring they were on the correct care path.
As a result of these systemic failures, many participants described how their wounds worsened before they finally received care or were referred to a wound care specialist. This chaotic and confusing experience was vividly reflected in the sketches, which visually communicated overwhelming frustration, uncertainty, and distress throughout the care-seeking process.
Visual imagery
The following visual imageries captured two key elements reflecting systemic challenges in accessing wound care services: Barriers to Patient-Centered and Culturally Inclusive Care and a “broken cart,” symbolizing a fragmented and ineffective healthcare system.
Barriers to patient-centered and culturally inclusive care
Participants shared experiences of stigma and a lack of empathy from healthcare professionals. One participant, for example, described how assumptions were made about their commitment to their own health based solely on their physical appearance, such as being overweight. This implicit bias resulted in feelings of judgment and neglect rather than supportive and patient-centered care.
Care partners also reported challenges in advocating for their loved ones, particularly when individuals with dementia were labeled as difficult patients (Figure 2). This designation negatively affected communication between healthcare professionals and the care partner, ultimately influencing the quality and responsiveness of care. A particularly significant barrier was cross-cultural communication failure. One care partner described how their loved one was unable to receive services in their preferred language, limiting their ability to fully engage in treatment decisions (Figure 5). Additionally, despite being hospitalized, their loved one was not offered traditional Indigenous medicines as a potential treatment option. This lack of culturally responsive care highlights systemic inequities that hinder access to appropriate and inclusive healthcare for diverse populations.
Broken cart: A fragmented and ineffective healthcare system
In this final section, we examine a sketch (Figure 6) that encapsulates a key theme expressed by all the research participants—the political reality of wound care within the healthcare system that is not always effective in addressing chronic issues such as chronic hard-to-heal wounds.
Sketch depicting the story of a participant who developed skin cancer on the scalp and faced numerous challenges in accessing wound care.
Participants not only highlighted failures in communication but also pointed to the broader systemic and structural shortcomings, including a lack of wound education, limited access to specialists, and scarce wound care clinics. Additionally, several participants described the impact of overburdened and stressed healthcare professionals. For example, in Figure 5 the artist depicts a nurse sitting in the bottom left corner of the sketch, appearing exhausted. The nurse is looking away from the patient and is notably absent from the circle of hearts, symbolizing emotional and physical detachment from patient care.
In Figure 6 the concept of a broken cart is used to represent the failures of the healthcare system. The artist portrays a patient struck down by the very system that was meant to support them in their healing journey. The participant is depicted lying face down on the cart, with their mouth covered by their hand on the cart—suggesting helplessness and silence. The cart itself, symbolizing the Canadian healthcare system, is broken, with one of its wheels missing. The artist describes the lasting impression from this depiction as a stark critique of the system, suggesting that, without urgent healthcare reform, only the strongest patients are able to survive.
Discussion
Summary: The research highlighted three key areas: the vital role of family and caregivers must be formally recognized and supported by policy; there is an urgent need for early, continuous public education and prevention strategies to mitigate complications; and, systemic inequities must be addressed to prevent delays in treatment. In this section, we discuss policy changes, such as implementing mandatory referral guidelines to specialists and creating dedicated wound care coordinator roles.
Chronic hard-to-heal wounds represent a critical public health issue due to their widespread impact on individuals’ quality of life, healthcare delivery, and broader public health outcomes. Chronic wounds—including diabetic foot ulcers, pressure injuries, and venous leg ulcers—are becoming increasingly prevalent, particularly with an aging population and rising rates of chronic conditions such as diabetes and obesity (Cotterell et al., 2024). As Canada’s population continues to age, the incidence of these wounds will place growing pressure on the healthcare system, necessitating research that articulates both the financial and psychosocial costs of chronic wounds and identifies effective, systemic-level changes to support successful and humane healing. This study demonstrates how qualitative research methods offer an in-depth understanding of patients’ and care partners/families’ experiences. The use of analytic sketches, in particular, provides a powerful visual representation, reinforcing the emotional and systemic challenges involved in wound care. These visuals deliver a deeply resonant analysis. Three themes emerged from the data that we will now discuss: social support, public education, and barriers to care. We will then conclude with a discussion about the implications for policy and practice.
The role of social support
Social support is a well-established determinant of health, influencing both physical and mental well-being. It includes emotional and practical assistance from family, friends, community, and broader social networks. As described by participants in this study, both the quality and availability of social support significantly shaped how individuals coped with chronic wounds, navigated the healthcare systems, and engaged in their healing process.
Participants emphasized the vital role care partners played during recovery, both in hospital and at home. Existing research supports this, evidencing that emotional support from care partners is associated with faster recovery, improved patient satisfaction, and reduced feelings of isolation (Lupo et al., 2024). In addition, social support can buffer against stress-related health complications (Li et al., 2023).
Beyond emotional care, participants described how family members played a crucial material role in wound management—assisting with dressing changes, advocating for referrals to wound specialists, and supporting mobility. Care partners were actively involved in physical care tasks, such as repositioning and encouraging movement to prevent wounds and support circulation. Research further supports the benefit of care partners engagement in loved ones’ mobility, indicating positive outcomes for both patients and families (Yasmeen et al., 2020). Care partners also provide valuable insights into a patient’s medical history and personal preferences, helping healthcare teams develop personalized, co-created and effective treatment plans.
Healthcare providers should acknowledge the significant impact that chronic wounds have on patients, care partners, and overall family dynamics. Doss and Popejoy (2023) emphasize that care partners do not express a wish to cease caregiving responsibilities. Instead, they consistently placed the highest importance on the patient’s pain management, progress in wound healing, and emotional well-being. The strong dedication demonstrated by care partners highlights the importance of providing appropriate support and resources to sustain their role.
Individuals with strong social networks are more likely to access quality healthcare services, health information, and resources, while those with limited social support often encounter significant barriers to care (Drageset, 2021). Moreover, social support has been shown to reduce the risk of premature death by providing networks of care partners and resources that assist individuals in managing chronic illnesses, seeking timely medical attention, and maintaining social connections (Chen et al., 2021). Participants in this study emphasized the crucial role of social networks in addressing existing health inequities.
Participants also described how family members often served as advocates, ensuring that their loved ones’ wound concerns were communicated to the healthcare team. This advocacy becomes especially critical when patients face communication barriers due to language barriers, dementia, or cognitive decline, as several participants noted.
While previous research shows that family involvement in decision-making promotes more personalized and person-centered care (Tringale et al., 2022), findings from our study revealed that care partners often felt excluded from conversations about wound treatment and were hesitant to raise concerns fearing it might negatively affect their loved one’s care. Acknowledging and supporting the role of family care partners in healthcare decision-making can foster a more collaborative care environment—one that benefits both patients and healthcare providers.
Public education and prevention
Primary care plays a central role in wound management, not only through clinical interventions but also by leading public education and prevention efforts aimed at reducing the incidence and severity of chronic wounds (Norman et al., 2016). Preventive care programs that target high-risk groups—such as individuals with diabetes or those at risk for pressure injuries—are essential to lowering the prevalence and severity of chronic wounds. Participants in this study expressed the need for early intervention and patient education, particularly for conditions like diabetes-related wounds. Without appropriate and timely management, these wounds can result to severe complications, including amputations and increased mortality rates (Molina and Faulk, 2022). Similarly, pressure ulcers, commonly seen among hospitalized patients, often require specialized and costly interventions. This highlights the importance of preventive strategies and person-centered care approaches (Jaul et al., 2018).
Study participants expressed a strong desire for early and continuous education on wound prevention and management. Their perspectives underscore the value of equipping both patients and caregivers with the knowledge and tools needed to take proactive measures. Continued investment in prevention and early detection is essential to reducing the long-term impact of chronic wounds—both for individuals and the broader healthcare system. Indeed, existing research confirms that prevention and early intervention programs can significantly lower the incidence of chronic wounds and related complications (Squitieri et al., 2020). In our research, those with wounds and care partners discussed the desire to have early and ongoing education regarding their wounds.
Social inequities and barriers
A growing body of research has identified a range of systemic and structural barriers that limit timely and equitable access to care for individuals with chronic wounds—including those with diabetic foot ulcers, veterans, and populations facing structural disadvantage (Charbit et al., 2024; Frasier et al., 2024). Delayed referral to specialized wound care emerged as a significant concern, with some individuals waiting 3 months or longer after wound onset before receiving expert attention (Charbit et al., 2024). These delays are often linked to limited access to primary care, as people struggle to find family physicians due to provider shortages, clinic closures, overbooked practices, or the need to travel long distances—particularly in rural and remote communities (Frasier et al., 2024).
Beyond access issues, gaps in provider training and wound care knowledge contribute to mismanagement that can worsen conditions and delay healing (Charbit et al., 2024; Frasier et al., 2024). Emergency care settings present further barriers, with long wait times, lack of coordination across services, and limited continuity of care. The scarcity of specialized services often forces individuals to seek care across multiple facilities, compounding delays and adding to the burden of navigating a fragmented system.
These challenges reflect broader structural inequities in healthcare that disproportionately affect equity-deserving communities. Geographic disparities are especially pronounced, with individuals in rural areas facing reduced access to wound care specialists and lower overall healthcare utilization. In Canada, Indigenous people, as well as people living on lower incomes, are more likely to experience delays in care due to the combined effects of geographic isolation, underfunded services, and historical inequities in healthcare delivery (Blanchette et al., 2023).
Participants in our study described how these inequities led to prolonged suffering and worsened health outcomes. Many also noted experiences of being dismissed or not taken seriously, particularly when presenting with complex health needs or coexisting health conditions such as depression or post-traumatic stress disorder. These conditions are common among people living with chronic wounds and can impede self-care, delay help-seeking, and contribute to poor wound healing. Additional barriers—including transportation challenges, financial constraints, language differences, and lack of culturally safe care—further limit access for communities historically excluded or underserved by healthcare systems. These overlapping factors deepen existing inequities.
Addressing these issues requires coordinated, equity-informed action at multiple levels. This research underlines that public health and clinical strategies must prioritize accessible, culturally safe, and inclusive wound care services. This includes expanding telehealth to improve geographic reach, integrating mental health supports, and enhancing provider training to ensure care is responsive to individuals’ social and cultural contexts. Healthcare systems must also implement policies that support timely, equitable access to specialized wound care, ensuring care pathways reflect the needs and realities of equity-deserving populations.
Policy and practice recommendations
The findings of our study reveal specific policy and practice changes needed to address the systemic failures in wound management. Through this arts-based method, we provide unique insights that translate directly into actionable recommendations for healthcare delivery transformation.
At the policy level, our participants’ experiences of delays before receiving specialized wound care highlight an urgent need for mandatory referral guidelines within primary care settings. Health care systems should establish time-sensitive pathways that automatically trigger specialist consultations when wounds fail to improve within specified timeframes. Care partners were often the primary advocates for securing these referrals, yet many reported feeling excluded from treatment conversations. This exclusion led to hesitancy in voicing concerns for fear of jeopardizing their loved one’s care. This paradox underscores the need for policy changes that formally recognize care partners as essential members of the health care team, with documented rights to participate in care planning discussions. Participants also described struggling to navigate multiple, at times disconnected, services while managing already complex wound care needs. Regional authorities can address this fragmentation by creating wound care coordinator positions—individuals who would serve as consistent points of contact and help ensure continuity as patients transition between providers and care settings.
When we examined what our findings mean for clinical practice, communication failures appeared as a central concern. Family members provided essential daily support, including changing dressings, helping with mobility, and monitoring wound progress, yet as noted, they consistently felt excluded from clinical conversations about treatment. These care partners held invaluable knowledge about patients’ histories, preferences, and daily realities that could inform better care decisions. Healthcare teams need documentation systems that capture and integrate these observations into treatment planning. Throughout our interviews, participants expressed frustration about the lack of early education on wound prevention and management. They wanted healthcare encounters that went beyond treating immediate crises to include time for learning practical skills and prevention strategies.
Conclusion
This research offered a vital look into the lived reality of individuals with chronic, hard-to-heal wounds, revealing profound impacts on their daily life and emotional well-being. By engaging participants as experts, we gained insights essential for developing more person-centered care approaches.
Methodologically, this research validated analytic sketching as a powerful visual tool for interpreting complex qualitative data. Externalizing experiences into visual form enhances the research process, offering a nuanced understanding of participants’ experiences.
Our analysis pinpointed several critical themes: pervasive poor communication within the healthcare system, the need for public education and the vital role of social support. Participants expressed deep frustration over barriers to timely specialist care, negatively affecting their physical and psychosocial health. Conversely, strong social support networks proved crucial for resilience and healing. These findings underscore the urgent need for holistic care models that move beyond provider-driven systems, treating patients as active partners and addressing both the physical and emotional dimensions of chronic wound management.
Footnotes
Acknowledgements
Thank you to Sahar Khoshchereh for her research assistance.
Ethical considerations
The Lakehead University Research Ethics Board reviewed the project for the purpose of analytical sketching and provided ethical approval (REB# 1470464). This research was conducted ethically in accordance with the Canadian Tri-Council Policy on Ethical Conduct for Research Involving Humans.
Consent to participate
The participants provided consent to conduct the study, publish the study, and have the drawings of their stories used and published, including in open access publications. All names have been redacted.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Social Sciences and Humanities Research Council of Canada (grant number 611-2021-0146).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.