
Abstract
Elevated depressive symptoms among parents of autistic children are well documented and associated with poorer mental health. Mindfulness has been identified as a protective factor against mental health difficulties, but its day-to-day associations with depressive symptoms in this population remain unclear. A total of 210 Chinese parents of autistic children participated in this 15-day diary study, during which they completed daily measures of mindfulness and depressive symptoms. The data were analysed using dynamic structural equation modelling. Results indicated that (1) parents’ daily mindfulness and depressive symptoms exhibited autoregressive stability and showed significant negative reciprocal cross-lagged associations at the within-person level. At the between-person level, (2) higher perceived social support was associated with lower mean depressive symptoms and higher mean mindfulness, and it strengthened the negative cross-lagged effect of daily mindfulness on next-day depressive symptoms; and (3) child externalising problems were positively associated with parents’ overall mean depressive symptoms and negatively associated with both parents’ overall mean daily mindfulness and the autoregressive effects of daily mindfulness and depressive symptoms. Findings underscore the importance of fostering daily mindfulness within a supportive resource context and highlight the need to maintain the day-to-day persistence of mindfulness in families of autistic children with higher externalising problems.
Lay Abstract
Parents of autistic children tended to feel fewer depressive symptoms on the day after they felt more mindful; likewise, they tended to feel less mindful the day after they felt more depressed. We asked 210 parents in China to complete a short daily questionnaire for 15 days about their daily mindfulness and depressive symptoms. We also looked at two factors that might affect day-to-day mindfulness and depressive symptoms: the level of perceived social support and children’s challenging externalising behaviours directed towards parents. We focused on how parents’ mindfulness and depressive symptoms shift from one day to the next to identify practical ways to improve parents’ mental well-being. We found that more perceived social support was linked to a stronger next-day connection between feeling more mindful and feeling less depressed, whereas more frequent behavioural challenges were linked to more ups and downs from one day to the next in both mindfulness and mood. The findings of this work can guide researchers and practitioners to design simple, everyday actions, such as brief mindfulness moments and better support for families, that help parents feel less low from one day to the next.
Keywords
Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental condition that typically begins in early childhood and is characterised by differences in social communication and interaction as well as restricted and repetitive patterns of behaviour (World Health Organization, 2025). Many parents of autistic children experience substantial and ongoing caregiving demands and parenting stress, which may increase their risk of psychological distress (Dijkstra-de Neijs et al., 2026; Schnabel et al., 2020). Depression, one of the most common mental health challenges, is typically characterised by low mood, loss of interest, sleep disturbances, and fatigue (Piro-Gambetti et al., 2023). It co-occurs with higher parenting stress, thereby further undermining parents’ health-related quality of life and children’s mental health (Barańczuk & Pisula, 2022; Benson, 2006; Dijkstra-de Neijs et al., 2026; Van der Lubbe et al., 2025). However, the day-to-day dynamics of depression among parents of autistic children and its potential protective mechanisms remain unclear. Accordingly, it is necessary to identify the psychological resources that buffer parents of autistic children against daily depressive symptoms. The conservation of resources (COR) theory is a widely applied framework in the field of caregiver mental health (McGhan et al., 2023; Ng & Yeung, 2024). It posits that individuals strive to retain, protect, and build a range of valued resources and invest them to forestall losses and hasten recovery (Hobfoll, 1989, 2001). Thus, it can provide a theoretical basis to examine how personal resources may alleviate depression among parents of autistic children. Among these resources, mindfulness is salient as a personal resource expressed at both trait and daily levels and therefore warrants focused examination in relation to depression. Given that depression-related experiences and self-regulatory resources are often context-sensitive and exhibit substantial day-to-day fluctuations (Hankin, 2010), and that daily diary reports can reduce retrospective reconstruction of short-term experiences while enhancing ecological validity in natural caregiving contexts (Shiffman et al., 2008), this study further investigates the temporal dynamics between mindfulness and depressive symptoms at the daily level.
Mindfulness as a Personal Resource: From Trait to Daily Dynamics
Mindfulness refers to the awareness marked by intentionally sustained attention to present experiences on purpose, in the present moment, and non-judgementally, together with an open and accepting orientation (Bishop et al., 2004; Kabat-Zinn, 2003). Viewed through a COR lens, mindfulness functions as a valued trait personal resource that helps individuals cope effectively under stress (Kroon et al., 2015). Mechanistically, it can be conceptualised as two complementary yet distinguishable processes: the first process concerns attention regulation, that is, sustained awareness of present-moment experience and the intentional deployment of attention, whereas the second involves an open, accepting, and non-judgemental orientation towards experience (Bishop et al., 2004). Although the first process may explain mindfulness-related cognitive benefits, heightened awareness without acceptance may render aversive cues more salient, thereby increasing emotional reactivity in contexts of high stress or intense negative experience (Hoffmann et al., 2024). By contrast, when the first process is coupled with the second process, individuals adopt a more decentred, non-judgemental stance towards noticed experience, with less evaluative processing, entanglement, and self-criticism, making it more likely that awareness yields emotional benefits rather than affect amplification (Lindsay & Creswell, 2017).
In families of autistic children, cross-sectional evidence showed that higher parental mindfulness was associated with lower parenting stress and fewer depressive symptoms (Wang et al., 2022). Longitudinal research further demonstrated that mindfulness attenuated the impact of stigma on subsequent depression among these parents (Yip & Chan, 2022). More recently, there has been a shift from focusing on between-person differences in mindfulness and depressive symptoms to examining within-person day-to-day fluctuations in daily mindfulness and daily depressive symptoms. This shift is well-suited to daily repeated assessments, which can capture the within-person day-to-day dynamics between mindfulness and depressive symptoms in naturalistic contexts (Suelmann et al., 2018). Such designs also help disentangle within-person variability from between-person differences, thereby reducing the risk of misinterpreting between-person associations as within-person mechanisms (Shiffman et al., 2008). Accumulating evidence indicates that daily mindfulness predicts daily fluctuations in affect, including reductions in daily depressive symptoms among the general population (Li et al., 2023; Raynes & Dobkins, 2025). However, little is known to date about the relationship between daily mindfulness and daily depressive symptoms among parents of autistic children.
Within the COR framework, when individuals can mobilise relatively high levels of resources on a given day, they are better positioned to cope effectively and protect their existing resources, thereby reducing resource loss and facilitating recovery. Over time, such processes may extend resource acquisition and give rise to a potential resource gain spiral (Halbesleben et al., 2014; Hobfoll, 2001). Accordingly, when mindfulness is viewed as a personal resource, elevated mindfulness on a given day may serve as a protective factor against depressive symptoms on the following day among parents of autistic children. Conversely, elevated psychological distress may further deplete the coping resources and other valued personal resources needed to manage stress and may intensify negative experiences, thereby contributing to a potential resource loss spiral (Halbesleben et al., 2014; Hobfoll, 1989). Accordingly, elevated depressive symptoms on a given day may serve as a risk factor for lower mindfulness on the following day among parents of autistic children. In addition, daily psychological states typically exhibit autoregressive dynamics, such that levels of mindfulness and depressive symptoms on a given day tend to carry over to the next, a pattern documented in general population samples (Ebrahimi et al., 2021; Li et al., 2025; Luo et al., 2023). Therefore, it is anticipated that both mindfulness and depressive symptoms exhibit day-to-day autoregression among parents of autistic children, such that part of each day’s relative level carries over to the next.
Perceived Social Support as Perceived Resource Availability
Social support is a key psychosocial resource and a robust marker of resiliency resources, whereas perceived social support reflects individuals’ global judgement of whether support is accessible when needed and has been operationalised as the “perceived availability of resources” within the COR framework (Halbesleben et al., 2014; Hobfoll, 2011). Cross-sectional evidence suggested that perceived social support was linked to higher mindfulness and lower depressive symptoms among Chinese parents of autistic children (Chen et al., 2024; Yang et al., 2023). Given its relative temporal stability, perceived social support is often treated as a person-level characteristic (Uchino, 2009). Accordingly, higher perceived social support is expected to be associated with higher mean daily mindfulness and lower mean daily depressive symptoms after separating between-person differences from within-person fluctuations.
Moreover, individuals who perceive resources as more available are better positioned to accrue resource gains, whereas those who perceive resources as scarce are more likely to experience resource losses (Halbesleben et al., 2014). Notably, resource gains and losses are not synonymous with gain and loss spirals which capture the mutually reinforcing accumulation of resources and outcomes over time. Thus, it remains unclear whether perceived resource availability, operationalised as perceived social support, further shapes gain spirals (e.g. the cross-lagged effect, whereby higher daily mindfulness predicts lower next-day depressive symptoms) and loss spirals (e.g. the cross-lagged effect, whereby higher daily depressive symptoms predict lower next-day mindfulness). In light of this, we conduct exploratory analyses examining whether perceived social support is associated with the strengths of these two day-to-day cross-lagged relations among parents of autistic children.
Child Behaviour Problems as Environmental Stressors
Behaviour problems are among the most common difficulties in parenting autistic children and have been consistently linked to heightened parental psychological distress (Estes et al., 2013; Lecavalier et al., 2006). These problems have been shown to be independent of age or gender, and to persist from adolescence into adulthood in autistic individuals, indicating a chronic course (Chua et al., 2023). Among these difficulties, child externalising problems, such as hyperactivity-inattention and conduct problems, showed the strongest association with child-related parenting stress, demonstrating predictive power even greater than that of ASD diagnosis (Olson et al., 2022). According to COR theory, although individuals strive to retain, protect, and accrue valued resources, high-intensity, chronic environmental stressors hasten resource depletion and precipitate resource loss spirals (Hobfoll, 1989, 2001). Within this framework, child externalising problems can be seen as ongoing, salient environmental stressors that are likely to significantly deplete parents’ resources, thereby precipitating resource loss spirals. Thus, at higher levels of child externalising problems, parents of autistic children may show greater depressive symptoms and reduced mindfulness. In addition, child internalising problems, such as emotional symptoms and peer problems, were reported to show weaker associations with parenting stress than child externalising problems and were less readily observable, more difficult to recognise, and often overlooked (Briesch et al., 2022; Olson et al., 2022). However, prior studies linking child behaviour problems to greater psychological distress and lower mindfulness among parents of autistic children typically focused on overall child behaviour problems rather than distinguishing between internalising and externalising problems (e.g. Beer et al., 2013; Jones et al., 2014). This may obscure potentially meaningful differences in how distinct types of child behaviour problems relate to parents’ psychological functioning. Accordingly, we further differentiate child behaviour problems into externalising and internalising problems and conduct exploratory analyses to examine their respective associations with parents’ mean levels of daily mindfulness and daily depressive symptoms.
In summary, although trait mindfulness has been shown to be protective against depression, the mechanisms through which daily mindfulness sustains the psychological health of parents of autistic children in day-to-day life remain insufficiently understood. Within the context of child behaviour problems as chronic environmental stressors, and incorporating perceived social support as perceived resource availability, this study investigates mindfulness-related day-level dynamics in parents of autistic children. This provides empirical evidence to inform the optimisation of support systems for families of autistic children and the selection of targets for mindfulness-based interventions. We employ a 15-day daily diary design and dynamic structural equation modelling (DSEM) to examine the cross-day dynamics between daily mindfulness and daily depressive symptoms among parents of autistic children at the within-person level. Meanwhile, we assess how perceived social support and child behaviour problems are associated with these dynamic processes and with parents’ mean levels of daily mindfulness and depressive symptoms at the between-person level. Figure 1 illustrates the autoregressive and cross-lagged paths as well as the between-person predictors. Based on this framework, we propose the following hypotheses.
H1: Autoregressive Effects.
At the within-person level, daily mindfulness and daily depressive symptoms will show daily inertia, such that levels on one day carry over to the next day in parents of autistic children.
H2: Cross-lagged Effects.
H2a: At the within-person level, mindfulness on one day will have a negative next-day effect on depressive symptoms in parents of autistic children.
H2b: At the within-person level, depressive symptoms on one day will have a negative next-day effect on mindfulness in parents of autistic children.
H3: Main Effects of Perceived Social Support.
At the between-person level, parents of autistic children with greater perceived social support will show lower mean daily depressive symptoms and higher mean daily mindfulness than those with less perceived social support.
H4: Exploratory Moderation of Perceived Social Support.
At the between-person level, we exploratorily examine whether differences in perceived social support moderate cross-day dynamics between daily mindfulness and daily depressive symptoms.
H5: Exploratory Impact of Child Behaviour Problems.
H5a: At the between-person level, we exploratorily examine whether higher levels of child externalising problems are associated with lower mean daily mindfulness and higher mean daily depressive symptoms among parents of autistic children.
H5b: At the between-person level, we exploratorily examine whether higher levels of child internalising problems are associated with lower mean daily mindfulness and higher mean daily depressive symptoms among parents of autistic children.

Dynamic Structural Equation Model of Daily Mindfulness and Daily Depressive Symptoms.
Methods
Procedure
Parents of autistic children were recruited using convenience sampling supplemented by purposive sampling from autism intervention centres in Jiangsu Province, Mainland China. All research procedures and materials were approved by the university’s ethics committee, and written informed consent was obtained from all enrolled parents. All participants reported that their children had been formally diagnosed with ASD by experienced clinicians, based on assessments conducted with the Autism Diagnostic Observation Schedule-2 (ADOS-2) or the Chinese Classification of Mental Disorders (CCMD) (Chinese Society of Psychiatry, 2001; Lord et al., 2012).
Prior to the commencement of the daily diary, all parents were fully informed of the procedures and provided family demographic information. Following the preparatory procedures, parents completed the same short (i.e. 2–3 min) questionnaire each night via Wenjuanxing, a widely used online survey platform in China, before bedtime over a 3-week period (15 consecutive weekdays, Monday–Friday for 3 weeks), reporting their depressive symptoms and mindfulness levels for that day. The link to the questionnaire was sent at 10:00 p.m. each night, with a submission deadline of 11:00 p.m. Parents who had not yet completed the questionnaire received a reminder at 10:40 p.m. Contact with participants was limited to completion reminders and technical assistance, with no counselling, emotional support, or supportive intervention provided during the diary period. Within 3 days after the completion of the daily diaries, parents were asked to complete additional questionnaires via Wenjuanxing, reporting on their overall perceived social support and their children’s externalising and internalising problems during the 15-day period. Overall, parents completed 2850 of 3150 possible daily questionnaires (90.48% compliance; range = 53.33%–100%, SD = 11.48%), indicating high compliance. Incentives were prorated according to individual completion rates.
Participants
The initial sample included 216 parents of autistic children. Six participants were excluded from the analyses due to having more than 50% missing data on all daily measured variables, yielding a final analytic sample of 210 parents (e.g. Luo et al., 2025). Descriptive statistics summarising the family demographic characteristics are shown in Supplementary Table 1. Regarding parent gender, 81.9% were mothers and 18.1% were fathers. Fathers’ mean age was 37.419 years (SD = 4.074) and mothers’ mean age was 34.929 years (SD = 3.865). Among the children, 21.9% were girls and 78.1% were boys. The children’s mean age was 6.319 years (SD = 2.333; range = 3–10 years). With respect to annual household income in 2024, 25.7% of families earned less than 50,000 RMB (approximately USD6944), 67.1% earned between 50,000 and 300,000 RMB (approximately USD6944–41,667), and 4.8% earned more than 300,000 RMB (approximately USD41,667). Regarding fathers’ educational level, 11.0% had completed junior high school or below, 23.8% had completed high school, 32.9% had completed a vocational degree, and 32.4% had earned a bachelor’s degree or higher. Regarding mothers’ educational level, 20.5% had completed junior high or below, 29.5% had completed high school, 28.6% had completed a vocational degree, and 21.4% had earned a bachelor’s degree or higher.
Measures
Within-Person Variables
Daily Depressive Symptoms
Daily depressive symptoms were assessed using three items adapted from the Chinese version of the 9-item Patient Health Questionnaire (PHQ-9), with adjustments made to capture the daily dynamics of three dimensions: anhedonia, depressed mood, and fatigue (Kroenke et al., 2001). Specifically, anhedonia and depressed mood were selected as the two core depressive symptoms (i.e. the PHQ-2), which has been extensively validated as a brief measure of depressive symptom severity and has been widely used in diary studies for repeated daily assessment (Levis et al., 2020; Oh et al., 2023). Fatigue was included as the third item because it is highly salient in high-demand caregiving contexts and carries substantial informational value in ultra-brief PHQ-based screening, serving as a useful complement to the core items (Halki et al., 2024; Xu et al., 2026). An example item was “Today, I had little interest or pleasure in doing things.” Parents indicated the extent to which they experienced each item on a 7-point Likert-type scale ranging from 1 (not at all) to 7 (extremely). The total score was calculated by summing the three items, with higher scores reflecting greater levels of daily depressive symptoms. Two-level factorial validity was examined using multilevel confirmatory factor analysis (MCFA) and all three items loaded positively on a single latent factor at both levels. Level-specific reliability was evaluated using McDonald’s ω (Geldhof et al., 2014). The results indicated excellent reliability coefficients, with ω = 0.754 at the within-person level and ω = 0.939 at the between-person level.
Daily Mindfulness
Daily mindfulness was assessed using three items adapted from the Chinese version of the Multidimensional State Mindfulness Questionnaire (MSMQ), with adjustments made to capture the daily dynamics of three dimensions: acting with awareness, non-judgemental acceptance, and present-moment attention (Blanke & Brose, 2017; Zhou et al., 2021). The MSMQ did not include nonreactivity because this dimension was difficult to adapt equivalently for time-contingent experience sampling assessments at fixed time points, and nonreactivity showed relatively weaker multilevel measurement support and was therefore not retained in the final MSMQ factor structure (Blanke & Brose, 2017). An example item was “Today, I did tasks with awareness of what I was doing.” Parents endorsed each statement on a 7-point Likert-type scale ranging from 1 (not at all) to 7 (extremely). The total score was calculated by summing the three items, with higher scores reflecting greater levels of daily mindfulness. Two-level factorial validity was examined using MCFA and all three items loaded positively on a single latent factor at both levels. The results indicated excellent reliability coefficients, with ω = 0.749 at the within-person level and ω = 0.973 at the between-person level.
Between-Person Variables
Perceived Social Support
The Multidimensional Scale of Perceived Social Support (MSPSS) was utilised to evaluate perceived social support (Kazarian & McCabe, 1991; Zimet et al., 1988). The Chinese version of the MSPSS has demonstrated strong reliability and validity among family caregivers of individuals with special needs (Wang et al., 2022). The scale comprises three dimensions, namely family, friends, and significant other support, with 12 items in total. In the current study, parents reported their perceived social support on a 7-point scale ranging from 1 (strongly disagree) to 7 (strongly agree), with higher scores reflecting greater levels of perceived social support. An example item from the scale is “I get the emotional help and support I need from my family.” The scale in this study indicated excellent reliability coefficients, with Cronbach’s α = 0.942. Model fit was evaluated using commonly cited cutoffs, with comparative fit index (CFI) ⩾ 0.95, root mean square error of approximation (RMSEA) ⩽ 0.06, and standardised root mean square residual (SRMR) ⩽ 0.08 indicating good overall fit (Hu & Bentler, 1999). Confirmatory factor analysis showed a good fit for the scale, with CFI = 0.987, RMSEA = 0.049, and SRMR = 0.028.
Child Externalising and Internalising Problems
The emotional symptoms, conduct problems, hyperactivity-inattention, and peer problems dimensions of the Strengths and Difficulties Questionnaire (SDQ) were utilised to evaluate child externalising and internalising problems (Goodman, 2001). In the current study, parents reported their children’s externalising and internalising problems on this 3-point scale ranging from 1 (not true) to 3 (certainly true). Child internalising problems were computed from the emotional symptoms and peer problems subscales, totaling 10 items. Child externalising problems were computed from the conduct problems and hyperactivity-inattention subscales, also totaling 10 items. Higher scores on the emotional symptoms and peer problems dimensions indicate that autistic children have more internalising problems. Similarly, higher scores on the conduct problems and hyperactivity-inattention dimensions indicate more externalising problems in children. An example item from the scale is: “Rather solitary, tends to play alone.” The scale in this study indicated excellent reliability coefficients, with Cronbach’s α for child internalising problems and child externalising problems being 0.895 and 0.900, respectively. Confirmatory factor analyses showed a good fit for the scale, with χ2/df = 1.209, CFI = 0.982, RMSEA = 0.032, and SRMR = 0.041.
Data Analysis
To examine the complex dynamics between daily mindfulness and daily depressive symptoms, the DSEM was conducted using Mplus version 8.3 (Asparouhov et al., 2018). The analytical framework involved days (within-person level) nested within individuals (between-person level). This method integrates multilevel modelling, allowing for the examination of interindividual variation (differences between parents) and intra-individual variation (daily fluctuations within each parent) over time (Hamaker et al., 2018). This analytic strategy enabled the testing of core research hypotheses, including the autoregressive effects of daily mindfulness and daily depressive symptoms, the cross-lagged relationships between them, and the influence of parents’ perceived social support and child externalising and internalising problems on these dynamics.
The first step involved modelling daily depressive symptoms and daily mindfulness. The observed variables were decomposed into between-person components (i.e. the latent mean) and within-person components (i.e. deviations of the observed scores from the latent mean) (see Figure 1). At the within-person level, depressive symptoms and mindfulness scores at time T were regressed on their respective scores at time T-1 to estimate autoregressive effects, and on each other’s scores at time T-1 to estimate cross-lagged effects. The contemporaneous residuals between the two variables were allowed to correlate. All within-person parameters were specified as random effects to capture individual differences, and at the between-person level, correlations among the random intercepts (i.e. person means) and among the random slopes (i.e. person-specific autoregressive and cross-lagged effects) were estimated. Based on the preliminary model and guided by theoretical assumptions, parents’ perceived social support, child externalising and internalising problems were further incorporated to examine the cross-level effects of these between-person variables on the dynamic relationship between mindfulness and depressive symptoms.
The parameters of the DSEM model were estimated using a Bayesian estimator and the model convergence was assessed using the potential scale reduction (PSR). We used the Mplus default non-informative prior specifications: regression-type parameters were assigned diffuse normal priors N(0, ∞), selected variance components used inverse-gamma priors IG(−1, 0), and covariance parameters used inverse-Wishart priors, including IW(0, −3) and IW(0, −7). The Bayesian estimation was conducted using Markov chain Monte Carlo (MCMC) sampling. The chains were run for up to 50,000 iterations with a thinning interval of 10 (i.e. only every 10th iteration was used for estimation) to obtain more stable results (Asparouhov et al., 2018). The 95% credible intervals (CrIs; i.e. the 2.5th and 97.5th percentiles of the posterior distribution) were reported for all parameters through MCMC sampling. A path was considered statistically significant when its 95% CrI did not include zero (McElreath, 2016). The within-person lagged variables were all latent person-mean centred, while the between-person variables were all grand-mean centred. When employing DSEM, careful consideration must be given to the time interval between measurement occasions, particularly in intensive longitudinal designs where lagged effects are inherently interval-dependent (Asparouhov et al., 2018; McNeish & Hamaker, 2020). In this study, questionnaires were delivered at a fixed time each evening (10:00 p.m.), with responses permitted only within a narrow window (10:00–11:00 p.m.) and limited to one submission per day. Data were collected on weekdays across three consecutive weeks. To maintain a 1-day time metric despite the weekend gaps, we defined a calendar-day time variable spanning the full study period and specified a 1-day interval using the TINTERVAL option in Mplus. Under this time-grid specification, unobserved weekend days are treated as missing occasions on the underlying daily time scale, so that lag-1 effects consistently reflect day-to-day carryover, rather than effects across unequal gaps between observed assessments (McNeish & Hamaker, 2020).
Results
Preliminary Data Analysis
The rates of missing data were low across key variables: 9.52% for both daily depressive symptoms and daily mindfulness, 1.43% for both externalising and internalising problems, and 0.95% for perceived social support. Little’s (1988) test of missing completely at random (MCAR) yielded a non-significant result, χ² = 2473.816, p = 0.095, suggesting that the data satisfied the MCAR assumption. Missing values were subsequently handled in Mplus through the Kalman filter procedure (Asparouhov et al., 2018).
Table 1 presents the descriptive statistics and bivariate correlations for parents’ daily mindfulness, daily depressive symptoms, perceived social support, and child externalising and internalising problems. The intraclass correlations for daily mindfulness and depressive symptoms were 0.711 and 0.699, respectively, indicating that approximately 70% of the variance in these variables was at the between-person level. At the within-person level, daily mindfulness was significantly negatively correlated with daily depressive symptoms. At the between-person level, mindfulness was significantly correlated with depressive symptoms, perceived social support, child externalising problems, and internalising problems; depressive symptoms were also significantly correlated with perceived social support, child externalising problems, and child internalising problems. Perceived social support was negatively and significantly correlated with child internalising problems and externalising problems. Child externalising and internalising problems were significantly positively correlated. The equivalent income index (EQI) was calculated as annual household income divided by household size. Family socioeconomic status (SES) was then derived based on the EQI, the higher occupational status of the father or mother, and the educational level of both parents. Daily depressive symptoms and daily mindfulness were not significantly correlated with family SES, parental age, or child age (see Supplementary Table 2 for details). Prior to the primary analyses, the DSEM included family SES, parental age, and child age at the between-person level as covariates. Their inclusion did not materially change the focal parameter estimates in terms of direction, magnitude, or statistical significance. Therefore, the main text reports the model without these covariates for parsimony and to reduce model complexity.
Descriptive Statistics and Correlations Between All Variables Included in DSEM.
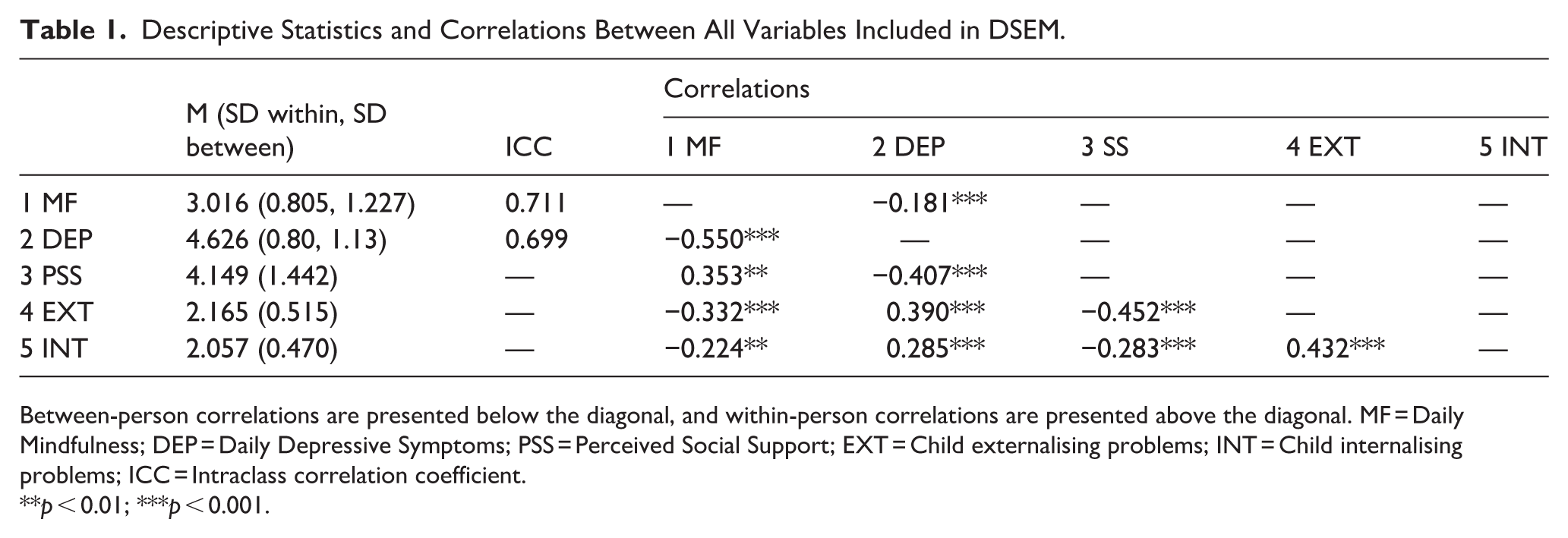
Between-person correlations are presented below the diagonal, and within-person correlations are presented above the diagonal. MF = Daily Mindfulness; DEP = Daily Depressive Symptoms; PSS = Perceived Social Support; EXT = Child externalising problems; INT = Child internalising problems; ICC = Intraclass correlation coefficient.
**p < 0.01; ***p < 0.001.
Within-Person Effects
First, the model demonstrated satisfactory convergence, with the PSR factor values ⩽ 1.011 for all parameters. The results revealed significant autoregressive effects for both mindfulness and depressive symptoms with coefficients of 0.285 and 0.254, respectively (see Table 2). This suggested that both mindfulness and depressive symptoms exhibited temporal stability. When parents experienced higher (or lower) levels on one day, they tended to maintain correspondingly higher (or lower) levels on the following day, confirming H1 regarding the autoregressive effects. However, the difference between the autoregressive effects of mindfulness and depressive symptoms was not credibly different from zero (β = 0.030, 95% CrI = [−0.081, 0.118]) (see Table 2). Second, cross-lagged coefficients revealed dynamic interactions between mindfulness and depressive symptoms. The lagged effect of mindfulness on next-day depressive symptoms was significant and negative (β = −0.074, 95% CrI = [−0.123, −0.025]), indicating that an increase in mindfulness one day significantly predicted a reduction in depressive symptoms on the following day. Thus, H2a was supported. The lagged effect of depressive symptoms on mindfulness was significant and negative (β = −0.049, 95% CrI = [−0.096, −0.000]; the upper bound rounds to 0.000), and thus H2b was supported.
DSEM Results for Standardised Within-Person Effect (N = 210).

φ11 = autoregressive effect of mindfulness; φ22 = autoregressive effect of depressive symptoms; φ12 = cross-lagged effect of mindfulness on the next-day depressive symptoms; φ21 = cross-lagged effect of depressive symptoms on the next-day mindfulness; ΔAR = difference between autoregressive effects; Credible intervals (CrI) represent the range within which the parameter lies with 95% probability based on the posterior distribution.
Between-Person Effects
Table 3 presents the effects of the between-person-level covariates. First, perceived social support was significantly related to the intercept of depressive symptoms (β = −0.262, 95% CrI = [−0.403, −0.110]), indicating that parents with higher levels of perceived social support exhibited lower overall mean levels of depressive symptoms. Perceived social support was also significantly related to the intercept of mindfulness (β = 0.255, 95% CrI = [0.095, 0.403]), suggesting that parents reporting greater perceived social support tended to maintain higher overall mean levels of mindfulness. Thus, H3 was supported. Second, perceived social support was significantly related to the cross-lagged effect of daily mindfulness on next-day depressive symptoms (β = −0.389, 95% CrI = [−0.655, −0.085]) (see Table 3). As shown in Figure 2, higher perceived social support was associated with a more negative lagged effect of daily mindfulness on next-day depressive symptoms, whereas under lower perceived social support this lagged effect was attenuated and close to zero. In contrast, perceived social support was not significantly related to the cross-lagged effect of daily depressive symptoms on next-day mindfulness (β = −0.179, 95% CrI = [−0.491, 0.163]). Taken together, these results yielded evidence of cross-level moderation as posed in H4, such that perceived social support moderated the cross-lagged association from daily mindfulness to next-day depressive symptoms, but did not moderate the cross-lagged association from daily depressive symptoms to next-day mindfulness (see Figure 3 and Table 3).
DSEM Results for Standardised Between-Person Effect (N = 210).

Note. Bold values indicate estimates whose 95% credible intervals do not include zero.

Moderation by Perceived Social Support of the Cross-Lagged Association From Daily Mindfulness to Next-Day Depressive Symptoms.

DSEM Path Diagram.
Third, in the case of child externalising problems, significant positive associations were found with the overall mean levels of depressive symptoms (β = 0.236, 95% CrI = [0.067, 0.395]), and significant negative associations were found with the overall mean levels of mindfulness (β = −0.196, 95% CrI = [−0.360, −0.016]), thereby yielding evidence consistent with H5a (see Figure 3 and Table 3). Regarding child internalising problems, the results indicated weak and non-significant associations with parents’ overall mean levels of mindfulness and depressive symptoms, suggesting that internalising problems were not reliably related to these between-person outcomes in the present sample. Accordingly, these findings yielded no clear evidence consistent with H5b. In addition, child externalising problems were negatively associated with the autoregressive effects of both daily mindfulness (β = −0.298) and depressive symptoms (β = −0.281), indicating weaker day-to-day stability at higher levels of externalising problems.
Discussion
To our knowledge, this is the first daily diary study to use DSEM to examine day-to-day processes between mindfulness and depressive symptoms among parents of autistic children. At the within-person level, the results demonstrated that daily mindfulness and daily depressive symptoms exhibited significant autoregressive effects, and significant negative reciprocal cross-lagged effects emerged between the two constructs across consecutive days. At the between-person level, perceived social support had a significant negative effect on mean depressive symptoms, a significant positive effect on mean mindfulness, and significantly moderated the cross-lagged association from daily mindfulness to next-day depressive symptoms. Child externalising problems had a significant positive effect on mean depressive symptoms, a significant negative effect on mean mindfulness, and a significant negative effect on the autoregressive parameters of both mindfulness and depressive symptoms, whereas child internalising problems showed no significant associations with daily means or dynamic parameters.
Within-Person Dynamics of Daily Mindfulness and Daily Depressive Symptoms (H1 and H2)
The findings showed that daily mindfulness was a significant predictor of subsequent daily depressive symptoms at the within-person level. This result extends previous between-person conclusions, which showed that higher trait mindfulness was associated with lower levels of depressive symptoms among parents of autistic children (Wang et al., 2022; Yang et al., 2023). Daily mindfulness can be conceptualised as the day-to-day availability and enactment of a valued personal resource that may help parents build resilience over time, thereby interrupting the spiral of resource loss and mitigating daily depressive symptoms (Kroon et al., 2015; Schwartzman et al., 2022). Another possible explanation for the finding is from the perspective of mindfulness-related cognitive mechanisms. Mindfulness involves the self-regulation of a metacognitive attentional state, characterised by nonreactive and nonevaluative monitoring of moment-to-moment cognition, emotion, perception, and sensation without fixation on past or future, thereby modifying maladaptive thinking patterns (Baer, 2003; Garland et al., 2010). Prior research has highlighted the non-judgemental acceptance as particularly relevant to depressive symptoms, including day-to-day dysphoric mood, and as a potential buffer against stress-related negative affective responding (Barcaccia et al., 2019; Ciesla et al., 2012). Mechanistically, a non-judgemental attitude and nonattachment inherent in mindfulness can help parents of autistic children release negative experiences such as self-shame or self-blame and view their distress from a broader, more balanced perspective, thereby allowing them to live with greater ease and composure (Brown-Iannuzzi et al., 2014; Rayan & Ahmad, 2016; Yip & Chan, 2022).
In addition, daily depressive symptoms were also a significant predictor of subsequent daily mindfulness, suggesting that depressive symptoms can act as a “loss trigger” that makes it more difficult to sustain mindfulness on the next day, thereby increasing vulnerability to a continued loss spiral in high-demand caregiving contexts. Frequent and unpredictable challenging behaviours and sensory difficulties in autistic children, greater child support needs, parental worries about the child’s future, and affiliate stigma jointly contribute to elevated and chronic parenting stress (Cheung et al., 2019; Ilias et al., 2018; Wang et al., 2022). Under such circumstances, parents may become caught in a resource loss spiral where depressive stress leads to the loss of more personal resources, which in turn further exacerbates stress (Hobfoll, 1989; Ng & Yeung, 2024). Notably, COR theory posits that resource loss spirals are often more consequential than gain spirals, reflecting an asymmetry that prioritises loss processes (Hobfoll, 1989). This suggests that enhancing mindfulness alone may be insufficient to fully counter resource erosion among parents of autistic children. More effective intervention and support efforts may need to combine timely identification and alleviation of depressive symptoms (e.g. improving sleep, emotion regulation training, and stress management) with strategies that promote sustained mindfulness practice, thereby reducing the risk of resource loss spirals. As for the autoregressive effects, both daily mindfulness and daily depressive symptoms exhibited significant inertia, suggesting that each carried over from one day to the next. Consistent with affect dynamics research, the significant autoregression of depressive symptoms may reflect perseverative negative affect maintained by rumination and by a slower recovery from emotional perturbations (Koval et al., 2012; Ong et al., 2025). Together, these processes foster the persistence of low mood from one day to the next.
Between-Person Perceived Social Support: Mean-Level Benefits and Stronger Daily Carryover (H3 and H4)
Consistent with prior evidence, perceived social support was significantly associated with lower average levels of depressive symptoms and higher average levels of mindfulness (Schiller et al., 2021; Yang et al., 2023). This finding underscores the role of perceived social support as a protective factor that simultaneously alleviates psychological distress and fosters positive psychological functioning among parents of autistic children (Drogomyretska et al., 2020; Liu et al., 2024; Wang et al., 2025; Zhang et al., 2024). Beyond mean-level associations, perceived social support acted as a contextual moderator that amplified the negative cross-lagged effect from daily mindfulness to next-day depressive symptoms among parents of autistic children. In other words, the protective effect of daily mindfulness on next-day depressive symptoms was stronger for parents with higher perceived social support. Mechanistically, when parents of autistic children perceive high perceived social support, including parent-to-parent support, spousal calming and shared caregiving, and professional guidance and resources, they are better able to reduce rumination, a resource-draining cognitive process (Pepperell et al., 2018; Xu et al., 2024). In this context, they are more likely to regulate in a non-judgemental, nonreactive manner, thereby enhancing psychological flexibility and resilience and fostering more adaptive stress appraisal, which facilitates relief from negative affect (Feng et al., 2025; Kashdan & Rottenberg, 2010; McKenna et al., 2022).
However, a significant association between perceived social support and the strength of the day-to-day lagged effect of daily depressive symptoms on next-day mindfulness was not observed. The carryover effect of daily depressive symptoms on next-day mindfulness may operate through pathways such as fatigue, motivational depletion, and impairments in attentional control (Grahek et al., 2019). These processes are relatively endogenous and automatic, and may directly reduce individuals’ capacity to enter a non-judgemental and nonreactive mindful state within a short time window (Bishop et al., 2004). Accordingly, even when parents generally perceive social support resources as available, such perceived availability may be insufficient to meaningfully attenuate the adverse impact of depressive symptoms on mindfulness over a 24-h lag. This pattern further suggests that interrupting such depletion processes may depend more on the mobilisation and actual use of support than on subjective perceptions of its availability in high-demand caregiving contexts. For example, when spouses share concrete caregiving responsibilities and specific task demands, or when parents receive guidance from professional services, the depleting influence of depressive symptoms on next-day mindfulness may be attenuated. Taken together, while social support acts as a critical environmental baseline, mindfulness provides an actionable daily strategy. Our findings suggest that interventions should prioritise building social networks (e.g. family support programmes) to maximise the impact of mindfulness, potentially yielding greater clinical gains than isolated mindfulness training.
Between-Person Externalising Problems: Mean-Level Detriments and Weaker Day-to-Day Carryover (H5)
Child externalising problems were significantly associated with a higher mean level of depressive symptoms and a lower mean level of mindfulness among parents. In contrast, child internalising problems were not significantly related to parents’ mean depressive symptoms or mindfulness. One possible explanation is that externalising problems are outwardly directed, readily observable, and highly disruptive in context (Degnan et al., 2008). Externalising problems such as hyperactivity and noncompliance have been shown to increase caregiving demands in families of autistic children, because these behaviours are more noticeable and disruptive in social contexts than internalising problems (e.g. social withdrawal) (Chua et al., 2023). Two complementary processes may account for this difference: first, in public settings, the visibility of externalising outbursts invites misinterpretation and blame, exposing parents to associative stigma and prompting them to reduce public participation, which in turn heightens emotional distress (Papadopoulos, 2021); second, managing externalising problems typically requires on-the-spot, high-intensity responding, including hypervigilance, prompt intervention, and redirection which may deplete parents’ cognitive and emotion regulation resources over time (O’Nions et al., 2018). This suggests that in families of autistic children similar to those in this study’s sample, with younger children and respondents predominantly mothers, prioritising intervention resources towards externalising problems may reduce parents’ day-to-day personal self-regulatory resource depletion and depressive stress.
In addition, beyond expectations, child externalising problems were negatively associated with the autoregressive parameters of both daily mindfulness and daily depressive symptoms. This indicates that parents’ mindfulness and depressive symptoms are more easily disrupted and show attenuated day-to-day carryover in families of autistic children where externalising problems are higher. In terms of mindfulness, although daily mindfulness can be replenished and exerts a protective next-day effect on depressive symptoms, its day-to-day retention appears weaker under higher levels of child externalising problems, rendering it a renewable yet less persistent resource that is less readily accumulated across days (Brown & Ryan, 2003).
Moreover, elevated levels of externalising problems are typically characterised by frequent conflicts, emotional outbursts, and noncompliance in families of autistic children, which require substantial daily parental time and attention for caregiving, thereby increasing parents’ event load and stress intensity on a given day (Davy et al., 2022; O’Nions et al., 2018; Smith et al., 2010). Thus, depressive symptoms reported on a given day may be driven more by child-related stressors occurring that day than by depressive carryover from the prior day (Pottie et al., 2009; Schilling et al., 2022). In particular, because depressive symptoms were assessed each evening in this study, reports may be relatively more sensitive to experiences occurring earlier that day, which could further reduce the apparent contribution of prior-day depressive carryover. Alternatively, high-demand caregiving contexts may activate a potential adaptive or compensatory mechanism, whereby parents rapidly reconfigure their context and resources on the following day by engaging in adaptive coping and implementing more effective parenting strategies or intervention efforts (Benjamin et al., 2024). Therefore, depressive symptoms on the following day may be more contingent on that day’s resource mobilisation and coping outcomes.
Practically, our findings suggest that interventions for parents of autistic children could potentially transition from intensive, clinical-level treatments towards sustainable, daily maintenance strategies. These include “micro-mindfulness” practices that are feasible for busy caregivers and the strengthening of social support networks to provide a necessary resource foundation. Crucially, in families where child externalising behaviours are prominent, extra support is needed to prevent the daily erosion of parental mindfulness, thereby breaking the cycle of day-to-day resource loss. For example, multiple brief mindfulness practices each day (e.g. breathing space, mindful pause, or compassion practices) can serve as maintenance strategies for emotion regulation (Economides et al., 2018).
Notably, the observed finding that higher mindfulness on one day predicts lower depressive symptoms on the next day can be understood as a resource gain spiral. Guided by COR theory, such gain spirals may have the potential to interrupt or slow down resource loss spirals among parents facing high caregiving demands. From an effect size perspective, the estimated cross-lagged effect of daily mindfulness on next-day depressive symptoms should be interpreted in the context of benchmarks for longitudinal models.
According to Orth et al. (2022), this effect represents a medium effect size, as cross-lagged coefficients in daily diary designs are typically attenuated by high autoregressive stability and short time lags. This interpretation is particularly relevant for parents of autistic children who often experience chronic and low-grade depressive symptoms alongside persistent caregiving stress. Over time, these small day-to-day increases in mindfulness may accumulate, thereby helping to prevent the gradual escalation of more severe depressive symptoms and yielding meaningful long-term change in this population. Moreover, unlike intensive mindfulness interventions, this study captures naturally occurring, momentary mindfulness in everyday life. Its value may therefore lie more in interrupting acute stress responses than in producing rapid and large reductions in depressive symptoms, thereby helping to prevent the compounding of resource loss over time.
Limitations and Future Directions
Interpretation of the findings of this study warrants consideration of several limitations. First, this study relied on a geographically bounded sample drawn only from Jiangsu Province, comprising primarily mothers of autistic children aged 3 to 10 years, with relatively limited participation of fathers and limited coverage of parents of autistic adolescents. In particular, stress-coping patterns may differ by parent gender, and parenting stress and mindfulness may also vary across developmental stages among autistic children. Future studies should recruit more gender-balanced samples, conduct stratified analyses by parent gender and child age, and extend recruitment to other regions to strengthen external validity. It would also be important to assess additional potentially relevant child and family characteristics (e.g. co-occurring intellectual disability and single-parent status) to better account for heterogeneity in caregiving contexts. Second, the observation window of this study was relatively limited, covering only 15 consecutive weekdays and excluding weekends. Although this design helped maximise adherence and data integrity while minimising disruption to families’ weekend rest and routines, it may have missed systematic weekend-related fluctuations and limited the examination of longer-term dynamic processes. As a result, this study could not determine whether sustained high levels of mindfulness over weeks or months would produce lasting reductions in depressive symptoms. Future studies should incorporate both weekday and weekend sampling and extend the follow-up period to better capture the day-to-day dynamics of mindfulness and depressive symptoms. Such evidence may also inform the development of brief mindfulness interventions with sustained practice components to test whether continued mindfulness practice leads to more durable reductions in depressive symptoms. Third, although the brief PHQ-based diary measure capturing anhedonia, depressed mood, and fatigue is well-suited to detecting day-to-day within-person symptom fluctuations, its time frame and scoring format are not aligned with those of the standard PHQ-9 used for clinical screening. As a result, we could not ascertain whether parents’ depressive symptoms exceeded the PHQ-9 clinical cutoff prior to the diary period, nor could we determine the clinically interpretable level to which symptoms changed by the end of the diary period. In addition, this daily measure did not assess domains such as sleep disturbance and self-blame, which may have constrained content coverage and the precision of estimating depressive symptom severity. Future research should incorporate the PHQ-9 alongside diary assessments and further adopt a micro-intervention design to test whether brief daily mindfulness practice can reduce depressive symptoms to clinically meaningful levels among parents of autistic children. Fourth, perceived social support reflects parents’ global appraisal of the availability of supportive resources. Its accuracy as a proxy for actual perceived social support may be compromised by recall bias in retrospective reporting and by pre-existing mental health status. Prior research has shown that perceived social support is only moderately correlated with received social support (Haber et al., 2007). As such, relying solely on global perceptions of perceived social support may not adequately capture day-to-day perceived social support acquisition and resource use processes. Accordingly, future intensive longitudinal studies should incorporate daily objective indicators of social support and resource investment. Such designs would also enable clearer comparisons of the relative contributions of contextual resources (e.g. actual perceived social support) and personal resources (e.g. mindfulness) to parents’ depressive symptom levels and their changes over time, thereby providing more actionable evidence for intervention prioritisation and resource allocation.
Conclusion
To our knowledge, this study is the first to use DSEM to trace the daily dynamics of mindfulness and depressive symptoms among parents of autistic children. At the within-person level, the results indicated that both daily mindfulness and daily depressive symptoms exhibited significant autoregressive effects, and significant negative reciprocal cross-lagged effects emerged between daily mindfulness and depressive symptoms across consecutive days. At the between-person level, higher levels of perceived social support were associated with lower mean depressive symptoms and higher mean mindfulness, and also amplified the cross-day protective pathway by which same-day mindfulness predicted lower next-day depressive symptoms. Child externalising problems were associated with higher mean depressive symptoms, lower mean mindfulness, and weaker day-to-day carryover in both mindfulness and depressive symptoms, whereas child internalising problems did not show any significant associations. This study demonstrates that mindfulness, a personal resource, forms a protective pathway for the mental health of parents of autistic children within a context of higher perceived social support. These findings highlight the importance of prioritising the provision of supports that incorporate brief daily mindfulness practices to sustain parents’ self-regulatory capacity and reduce day-to-day depressive symptoms.
Supplemental Material
sj-docx-1-aut-10.1177_13623613261439930 – Supplemental material for Daily Mindfulness and Depressive Symptoms Among Parents of Autistic Children: A Dynamic Structural Equation Modelling Study
Supplemental material, sj-docx-1-aut-10.1177_13623613261439930 for Daily Mindfulness and Depressive Symptoms Among Parents of Autistic Children: A Dynamic Structural Equation Modelling Study by Lin Wang, Meng Hua, Xinyi Hu, Yifan Wang, Qinxing Xie, Guang Yang and Yuan Chen in Autism
Footnotes
Ethical Considerations
This study received ethical approval from the appropriate institutional ethics committee. All procedures involving human participants complied with the ethical standards of institutional and/or national research committees and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Consent to Participate
Written informed consent was obtained from all individual participants prior to data collection.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Qing Lan Project of Mid-career Academic Leader in Jiangsu Province (2023) and Qing Lan Project of Excellent Teaching Team in Jiangsu Province (2025).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analysed during the current study are not publicly available due to ethical restrictions but are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.