
Abstract
Cognitive-behaviour therapy (CBT) is an evidence-based treatment for social anxiety. However, despite the high prevalence of social anxiety among autistic adults, much less is known about how autistic people experience each CBT component used in treatment. This qualitative study explores autistic adults’ perspectives on a modified cognitive-behaviour therapy group programme for social anxiety, focusing on the perceived effectiveness of CBT components and the identification of needed modifications. Twenty-seven participants who completed the intervention took part in semi-structured interviews. Thematic analysis identified core themes related to therapeutic impact (application of CBT group strategies) and participant experiences (suggestions for future iterations of social groups). Overall, exposure tasks were viewed as helpful in reducing anxiety, particularly when structured and predictable. Cognitive restructuring was often experienced as effective; however, its impact was sometimes limited by persistent and deeply held core beliefs and past negative experiences. Social strategies and anxiety management skills were appreciated for their structured format and educational elements, but generalizability was sometimes raised as a limitation. Participants also recommended additional adaptations, including flexibility in content delivery and modifications to the physical environment. Findings highlight overall support of cognitive-therapy components for reducing social anxiety in adults, but also benefit to tailoring CBT approaches to theneeds of autistic adults. Results from this study offer practical guidance from autistic people to enhance the acceptability and effectiveness of future CBT interventions.
Lay abstract
Many autistic adults experience social anxiety, making everyday interactions feel stressful or overwhelming. To help with this, clinical researchers developed a group therapy programme based on cognitive-behaviour therapy adapted for autistic adults. While cognitive-behaviour therapy is commonly used to treat anxiety, there has been relatively little research into how autistic people experience group-based versions of this therapy. This study aimed to understand how participants felt about the programme and how it could be improved. The intervention included eight group sessions where participants learned about social anxiety and autism, social strategies and took part in guided activities to build confidence. The programme encouraged a supportive environment where autistic individuals could safely try out new ways of connecting with others without feeling pressure to hide who they are. To understand how helpful the programme was, researchers interviewed participants about their experiences. Many said the programme helped them feel more confident and less anxious in social situations. For example, they found role-playing in a safe group setting especially useful. Participants also appreciated that the therapy was adapted to suit their needs. However, the study also highlighted some areas for improvement. Some participants found parts of the programme challenging, especially unstructured activities or settings. Others suggested the programme could be more flexible, offer clearer instructions or be better prepared for people who had past negative experiences with therapy. These early findings suggest that cognitive-behaviour therapy can be effective when thoughtfully adapted for autistic adults. This work helps lay the foundation for more inclusive, autism-informed mental health services that support social confidence in a way that feels safe and empowering.
Keywords
Background
The co-occurrence of autism and social anxiety has received increasing attention, reflecting the elevated rates of social anxiety among autistic individuals. Social anxiety is defined by a marked fear of social situations driven by concerns about negative evaluation (American Psychiatric Association, 2013) and affects approximately one in eight neurotypical adults (Ruscio et al., 2008). In autistic populations, prevalence estimates are substantially higher. Studies involving autistic children and adolescents report rates ranging from approximately 30% to over 50% (Bellini, 2004; Kuusikko et al., 2008; Simonoff et al., 2008; Spain et al., 2018). Estimates in autistic adults are more variable and depend on sampling methods, with clinical and psychiatric samples indicating that between 13% and 80% meet the criteria for social anxiety disorder (Boulton & Guastella, 2021; Joshi et al., 2013; Lugnegård et al., 2011; Russell et al., 2016). Maddox and White (2015) further estimate that around half of autistic adults without co-occurring intellectual disability experience clinically significant social anxiety, which can substantially disrupt daily functioning and social engagement (Smith et al., 2019; Van Steensel et al., 2011). Despite these elevated rates, research on mental health in autistic adults remains comparatively limited, with a disproportionate focus on childhood populations (Spain et al., 2016). Nonetheless, screening studies consistently indicate that more than half of autistic individuals report clinically significant anxiety and depression (Boulton & Guastella, 2021; Park et al., 2019), underscoring the heightened mental health burden in this population.
Beyond its prevalence, social anxiety in autism has profound functional and emotional consequences. Autistic adults often describe social anxiety as intertwined with repeated experiences of exclusion, sensory overload and communication challenges in social situations, which amplifies distress and restricts opportunities for meaningful social engagement (Bellini, 2006; Crompton et al., 2020; Spain et al., 2020). These difficulties can lead to significant impairment across education, employment and relationships, contributing to elevated rates of depression and reduced quality of life (Howlin & Magiati, 2017; MacKenzie et al., 2024; Park et al., 2019). Importantly, behaviours commonly associated with social anxiety, such as social withdrawal or rehearsed speech, may, at times, serve adaptive functions. This means that it may be important to discern whether the behaviour is adaptive or primarily an anxiety-driven avoidant response (Wilson & Gullon-Scott, 2024b). Given these complexities, interventions need to consider autism-informed principles that validate lived experiences and promote authentic social participation. Cognitive-behavioural therapy (CBT), particularly when adapted to meet these needs, can offer an evidence-based approach for reducing distress and enhancing functional outcomes (Bemmer et al., 2021; Spain et al., 2017; White et al., 2012).
Although social anxiety has been extensively examined in non-autistic populations, it remains unclear how established cognitive-behavioural models (Clark & Wells, 1995; Rapee & Heimberg, 1997), and related intervention components based on them, are experienced by autistic individuals (Bemmer et al., 2021). Core assumptions within traditional models may not fully account for autism-specific factors, including differences in sensory processing, emotion regulation differences and differences in social communication (Hull et al., 2019; Lei et al., 2024; Wilson, 2024). Commonly suggested modifications include using low-sensory therapeutic environments, incorporating special interests and strengths into social learning activities, and a strong focus on collaborative, transparent goal setting, all of which may support more meaningful social engagement and well-being and greater reductions in anxiety (Cummins et al., 2018, 2020; Lawson, 2020).
While some studies suggest that CBT-based interventions and social strategy support programmes can be helpful for autistic individuals, evidence remains mixed. Further research is needed to clarify effectiveness and acceptability. Emerging findings suggest that the process of delivering these interventions, may play a crucial role in determining outcomes. Structured role-plays, predictable practice formats and clear behavioural frameworks can reduce uncertainty and support gradual exposure (Bemmer et al., 2021; Gates et al., 2017; Roisenberg, Boulton, Thomas, & Guastella, 2025; Spain et al., 2017). Consistent routines, visual supports and opportunities for in-session practice enable participants to safely test their fears, receive feedback and build confidence, which may help generalize skills beyond therapy sessions (Roisenberg, Boulton, Thomas, et al., 2025). These process-focused components appear promising for fostering authentic engagement rather than reinforcing camouflaging and masking, which is associated with poorer mental health outcomes (Roisenberg et al., 2026).
At the same time, recent research highlights difficulties with CBTif applied in a way that prioritizes neurotypical norms. Programmes structured around such expectations have been argued to inadvertently create pressure for participants to appear socially ‘typical’, reinforcing camouflaging behaviours and stigma (Evans et al., 2024; Kupferstein, 2018; Petrolini et al., 2023, cf also see Roisenberg, Boulton, Thomas, & Guastella, 2025). Autistic adults have reported that at times CBT strategies can feel mismatched to their needs, and concerns have been raised about interventions that discourage authentic behaviours without considering long-term emotional consequences (Leaf et al., 2021; Monahan et al., 2021; Wilson & Gullon-Scott, 2024b). A critical gap remains in understanding autistic individuals’ perspectives on these approaches, what they find helpful, what they find challenging and how specific CBT components are experienced. Addressing this gap requires research that centres autistic voices to inform respectful, effective adaptations.
Recognizing these complexities and this gap in the literature, the Engage programme (Guastella & Thomas, 2020), is an evidence-based CBT group intervention that incorporates a structured social framework, while being specifically adapted to respect the unique needs and goals of autistic individuals. This programme aims to provide support that aligns with individual preferences and promotes meaningful engagement, while being based on CBT principles. This article explores the perspectives of autistic individuals who have participated in this therapeutic programme, offering insights into their experiences, priorities and challenges.
This study is part of a broader qualitative investigation into autistic adults’ experiences of a modified CBT group programme for social anxiety. Given the richness and scope of the data, we chose to present the findings across two complementary papers to allow for a detailed and nuanced analysis of distinct but interconnected domains. The present paper focuses on participants’ experiences with specific CBT components, such as cognitive restructuring, behavioural experiments, and social strategies. It examines how these strategies were perceived, adapted and applied in the treatment of social anxiety. In contrast, the companion paper explores group processes in depth, including the influence of peer dynamics and relational factors on therapeutic engagement (Roisenberg, Boulton, Thomas, Perry, et al., 2025a). While these areas are interrelated, combining them into a single manuscript would have limited the depth of analysis and obscured important insights. Together, the two papers provide an integrative understanding of both the mechanisms of individual CBT strategies and the social context that shapes their effectiveness. In addition, the current paper incorporates participants’ recommendations for improving group processes, offering a bridge between individual experiences and broader programme design considerations. A separate quantitative analysis of the intervention found significant reductions in social anxiety symptoms, alongside a trend towards reduced camouflaging behaviours. Notably, greater reductions in camouflaging were associated with larger decreases in social anxiety following the programme (Roisenberg, Boulton, Thomas, & Guastella, 2025).
Methods
This is a qualitative study that explores the perceived effectiveness of CBT strategies in a modified CBT group intervention, tailored for autistic adults who experience social anxiety.
Participants
Participants were 27 autistic adults who were recruited to take part in the Engage programme between May 2023 and July 2024. Participants were required to have received an autism diagnosis within the past 12 months, confirmed through the Autism Diagnostic Observation Schedule-2 (ADOS-2; Module 4; Lord et al., 2000) at study entry, and were required to be at least 16 years old. All participants were actively seeking assistance for difficulties related to social anxiety and fulfilled diagnostic criteria for Social Anxiety Disorder as determined through the Anxiety Disorders Interview Schedule (ADIS). Exclusion criteria included the presence of suicide risk or severe depression, a Full-Scale IQ (FSIQ) score below 70 as determined by the Wechsler Test of Adult Reading (WTAR; Wechsler, 2001), the identification of active psychosis during the intake assessment, limited proficiency in English, substance abuse, or significant impairments in vision or hearing that could interfere with participation in the programme’s audio/visual components. Most participants (79%) were taking at least one psychotropic medication. The most frequently reported categories were antidepressants (52%), stimulants (38%) and anxiolytic or sedative medications such as clonidine, propranolol or melatonin (41%). A smaller proportion were prescribed antipsychotic medication (14%) or mood stabilizers such as lithium or lamotrigine (17%). Seven participants (24%) reported no regular medication use. Participants were not excluded based on receiving concurrent or previous psychological or pharmacological treatments. Before their involvement in the study, all participants provided written informed consent. Participants were aged between 18 and 38 years (M = 25.2, SD = 5.09) and had a mean IQ score of 113 (SD = 5.84), with a median of 115. Participants reported a range of gender identities: 12 identified as women (44.4%), 8 as men (29.6%), 4 as another gender (14.8%) and 3 chose not to disclose their gender (11.1%). In terms of sex assigned at birth, 16 participants were assigned female (59.3%) and 11 were assigned male (40.7%).
Regarding the measures, at baseline and post-intervention, camouflaging behaviours were measured using the Camouflaging Autistic Traits Questionnaire (CAT-Q; Hull et al., 2019), which has demonstrated strong psychometric properties and measurement invariance in autistic adults. Social anxiety was assessed using the Liebowitz Social Anxiety Scale–Self-Report (LSAS-SR; Liebowitz, 2015), which has shown robust reliability and validity in autistic populations (Kanai et al., 2011). Complementary aspects of social anxiety were assessed using the Social Interaction Anxiety Scale (SIAS) and Social Phobia Scale (SPS; Mattick & Clarke, 1998), both of which have demonstrated good psychometric properties in autistic samples (Boulton & Guastella, 2021; Maddox & White, 2015). Social functioning and autistic traits were assessed using the Social Responsiveness Scale-2, Adult Self-Report (SRS-2; Constantino & Gruber, 2012), which demonstrates excellent internal consistency. Full details on measure administration, scoring and quantitative outcomes are reported in Bemmer et al. (2021) and Roisenberg, Boulton, Thomas and Guastella (2025).
At baseline, participants demonstrated pronounced social anxiety symptoms, as measured by the Liebowitz Social Anxiety Scale (LSAS; Kanai et al., 2011; Liebowitz, 2015). The mean total score of 82.50 (SD = 29.13) fell within the moderate to severe range, with substantial levels of both fear (M = 42.00, SD = 16.15) and avoidance (M = 40.50, SD = 13.99) in social situations. Broader psychological assessments indicated similarly elevated difficulties. On the Kessler Psychological Distress Scale (K10; Kessler et al., 2003), participants reported high distress (M = 29.04, SD = 7.85). Scores on the Depression Anxiety Stress Scales (DASS-21; Park et al., 2020) reflected moderate to severe depression (M = 33.05), anxiety (M = 14.92) and stress (M = 23.92). Quality of life, measured by the World Health Organization Quality of Life – BREF (WHOQOL-BREF; Whoqol Group, 1998), was reduced across all domains, with the lowest mean in the psychological domain (Domain 2: M = 35.26, SD = 13.76). World Health Organisation Disability Assessment Schedule (WHODAS 2.0; Üstün et al., 2010) scores indicated marked functional impairment (M = 81.39, SD = 22.93). Social functioning measures showed high camouflaging behaviours (CAT-Q Total: M = 120.31, SD = 30.56; Hull et al., 2019) and elevated social communication difficulties (SRS-2 SCI: M = 94.62, SD = 19.77; Total score: M = 114.27, SD = 25.65; White et al., 2010). Taken together, these findings underscore the complex clinical profile of the sample, characterized by significant social anxiety, psychological distress, functional challenges and social communication difficulties at the outset of the intervention.
Intervention programme
The intervention was designed to support the needs of autistic adults by using clear and concrete language, visual supports and a predictable session structure. A detailed description of the programme can be found in Bemmer et al. (2021) and Roisenberg, Boulton, Thomas, et al. (2025). Exposure tasks were introduced gradually, and sessions emphasized safety, peer connection and sensory accessibility. Groups were held in a low-stimulation environment, and participants were encouraged to use personal regulation strategies such as breaks or noise-cancelling headphones. Communication preferences were discussed at intake and revisited throughout the programme, allowing individuals to contribute in ways that best suited them (e.g. speaking or writing). Facilitators checked in regularly to ensure comfort, inclusion and accessibility. All sessions were delivered in person at a university-affiliated clinic.
The programme ran for 8 weeks and consisted of weekly 3-h group sessions with six to eight participants. Two clinically trained facilitators with experience working with autistic adolescents and adults led the group sessions. Sessions followed a consistent structure, and facilitators met for a 60-min debrief after every session to review progress and set goals for the following week.
Each session began with a review of the previous week’s homework, followed by discussion and practice of the session’s key topics. Homework tasks varied and included activities such as making phone calls, monitoring thoughts and feelings, and approaching social situations. At the end of each session, facilitators introduced the next week’s homework and dedicated the final 30 min to an informal ‘coffee time’. This provided a supported opportunity to practice skills in real-life interactions, during which facilitators also checked in with participants individually to help plan personalized activities and address emerging challenges.
This qualitative study examined a modified CBT programme adapted from established treatments for social anxiety in adults (Heimberg, 2002; Hofmann & Otto, 2008; Rapee et al., 2009). The programme incorporated clear goal setting and structured social strategies support to help participants approach exposure tasks with greater preparation and confidence. These elements were integrated throughout the sessions to support participants in testing unhelpful beliefs during real-world interactions and transferring these gains into everyday life. Overall, the programme aimed to equip autistic adults with both practical skills and the confidence needed to engage fully with the therapeutic process.
Positioning of the qualitative study
The qualitative study reported here was embedded within a broader mixed-methods evaluation of the Engage Programme, a modified CBT group intervention for autistic adults with social anxiety (Bemmer et al., 2021). The larger study included a quantitative component assessing intervention outcomes (e.g. changes in social anxiety, camouflaging behaviours and social functioning) using validated measures pre- and post-intervention (see Roisenberg, Boulton, Thomas, & Guastella, 2025). Following completion of the intervention, participants were invited to take part in semi-structured interviews to provide in-depth reflections on their experiences. This qualitative component was designed to complement the quantitative findings by exploring the mechanisms underlying observed changes and identifying factors that influence acceptability, feasibility and perceived effectiveness. Positioning the qualitative study within this framework enabled a focused examination of participants’ subjective experiences of the intervention, offering contextual insight into how outcomes may have been produced and how the programme was experienced in practice.
Procedures
Interviews
Individual, in-person interviews were conducted during the final week of the 8-week group programme, allowing participants to reflect on their experiences while still engaged with the intervention. Of the 46 participants who completed the programme, 27 consented to participate. Interviews were held in private rooms at the university to ensure confidentiality and comfort.
Participants could choose to be interviewed by a familiar group coordinator or an independent researcher to accommodate comfort and minimize bias. Interviews followed a semi-structured format designed to explore participants’ experiences with specific CBT components (e.g. exposure tasks, cognitive restructuring, social coping skills) and overall group processes. Sessions began with an open-ended question (‘What did you gain most from the groups?’) before moving to topics such as meaningful aspects of the programme and suggestions for improvement. Example questions for each CBT component are presented in Table 1, and a full copy of the interview guide is available in the supplementary materials. Interviews were audio-recorded with consent, supplemented by field notes, transcribed verbatim and imported into NVivo for thematic analysis.
Aspects of the group and corresponding example questions from the interview.
Note. The whole interview can be found in the supplementary materials.
Data analysis
Reflexive thematic analysis was used to analyse the interview data (Braun & Clarke, 2006, 2013, 2019). The analysis was situated within a critical realist framework, acknowledging the ontological reality of participants’ experiences while recognizing that themes are co-constructed through the analytic process (Wiltshire & Ronkainen, 2021). Coding and theme development were inductive and focused on semantic content, centring participants’ explicitly articulated experiences (Braun et al., 2019).
The first author led the initial phase of analysis, immersing herself in the data through multiple readings of the transcripts before developing preliminary codes that reflected repeated patterns across participants’ accounts. Coding proceeded iteratively and reflexively, with analytic memos used to record methodological decisions and developing insights (Chenail, 2015; Goundar, 2025; Mohajan & Mohajan, 2022). Credibility was supported by having a second researcher independently code a subset of the data (25%), enabling discussion and refinement of interpretations. The developing thematic framework was further examined by a third team member, who offered critical commentary throughout the analytic process.
The development of themes occurred through ongoing, collaborative engagement among the research team. Initial codes were iteratively grouped into higher-order patterns through reflexive discussion, allowing themes to be refined and elaborated. Input from a neurodivergent co-researcher informed both theme development and manuscript review, integrating lived experience into the analytic process. The final thematic structure reflects a situated understanding of participants’ experiences, encompassing both helpful and challenging aspects of the modified CBT programme. Percentages are reported descriptively to indicate the distribution of experiences across the sample; these figures are not intended to imply statistical generalization.
Researchers’ positionality
The research team recognize that both professional training and lived experience shape how participant accounts are interpreted. The primary academic authors identify as both neurotypical and with neurodevelopmental diagnoses and bring clinical and research expertise in autism and mental health, including extensive experience with CBT-based interventions. These backgrounds inevitably informed initial assumptions about therapeutic processes, outcomes and the role of interventions in addressing social anxiety. Reflexivity was therefore embedded throughout the analytic process. Analytic memos were used to document interpretive decisions, evolving understandings and the influence of researchers’ positional standpoints during coding and theme development (Chenail, 2015; Goundar, 2025; Mohajan & Mohajan, 2022). Regular team discussions created space to critically examine interpretations, question initial assumptions and consider alternative readings of the data. Crucially, an autistic member of the research team was also a former participant in the intervention, contributed as a co-researcher and co-author. Their involvement extended beyond consultation to active participation in interview guide development, qualitative interpretation, theme refinement and manuscript review. This collaboration ensured that analytic interpretations were continually grounded in lived experience, supporting more nuanced, balanced and community-informed accounts of both the benefits and challenges associated with the modified CBT programme.
Participatory methods
This study was co-produced in partnership with autistic individuals and neurodivergent researchers to ensure it aligned with community priorities and lived experience. A Community Consultation Committee, comprising autistic adults, including former participants of the CBT group programme, was actively engaged throughout the design and implementation, reviewing study aims, shaping the intervention format and advising on accessibility and relevance. In addition, a neurodivergent member of the research team, who was also a former participant, contributed as a co-researcher and co-author. Their role included co-designing the interview guide, interpreting qualitative data, collaborating on thematic analysis and reviewing manuscript drafts. This ongoing collaboration embedded lived experience into every stage of the project, from study design to dissemination.
Results
Baseline characteristics of consenting participants
An initial evaluation was conducted to understand the baseline characteristics of those participants in the group programme who agreed to complete the qualitative interviews in comparison to those participants who chose not to. A total of 46 individuals were invited to complete the qualitative interviews at the point of consenting to the group programme. Of the 46 individuals, 27 (58.7%) agreed to participate in qualitative interviews, while 19 declined. There were no significant differences across any baseline variables we had collected information on between groups, including age, gender, IQ, baseline social anxiety symptom scores, social responsiveness and camouflaging scores. There was also no significant difference in the amount of self-reported symptom reduction pre- to post-therapy. For further information about descriptive information about the group, please see Bemmer et al. (2021) and Roisenberg, Boulton, Thomas and Guastella (2025).
Reflexive thematic analysis identified a set of themes, subthemes and codes that capture key aspects of participants’ experiences in the adapted CBT group for social anxiety (see Table 2 and Figure 1).
Themes, subthemes and codes.
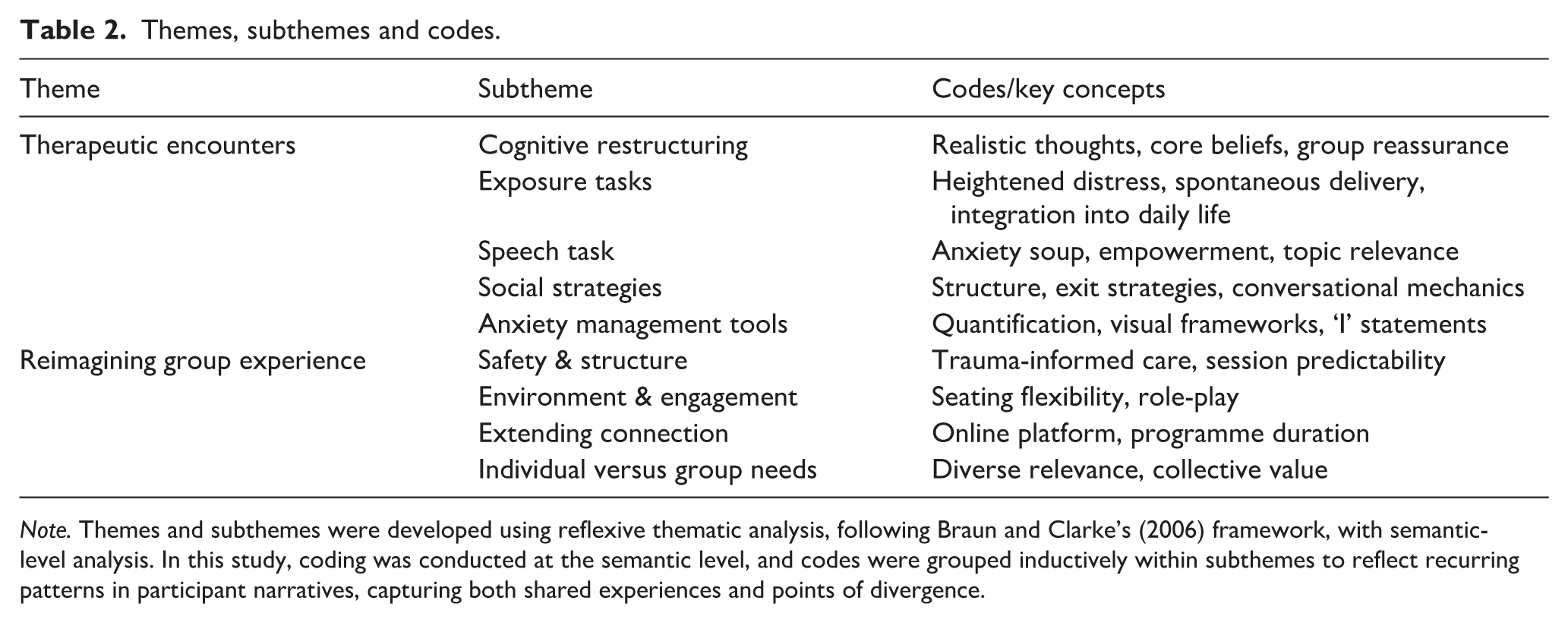
Note. Themes and subthemes were developed using reflexive thematic analysis, following Braun and Clarke’s (2006) framework, with semantic-level analysis. In this study, coding was conducted at the semantic level, and codes were grouped inductively within subthemes to reflect recurring patterns in participant narratives, capturing both shared experiences and points of divergence.
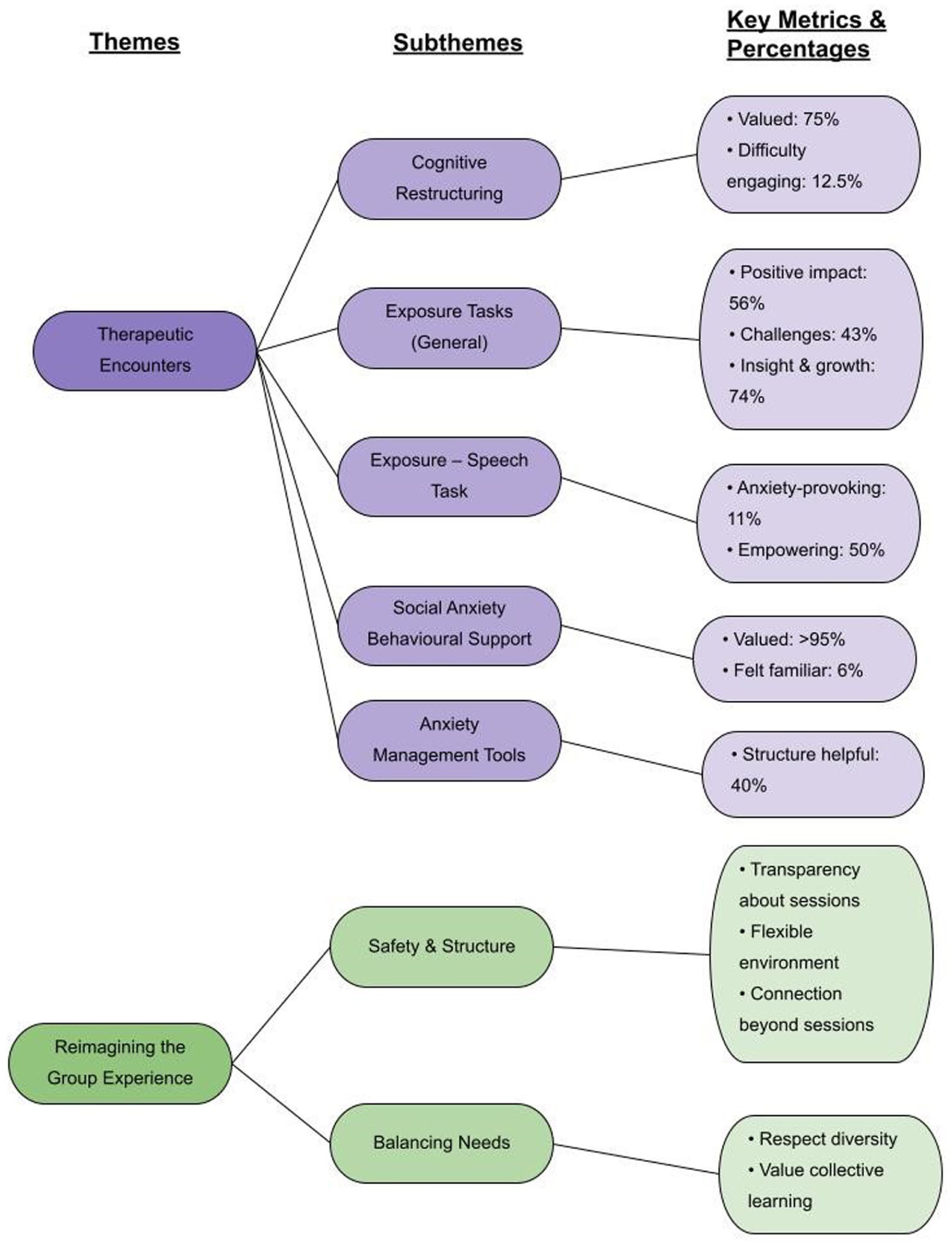
Conceptual map of qualitative findings.
Therapeutic encounters: how CBT strategies were experienced
Navigating cognitive restructuring in group-based CBT
Participants described a range of experiences with cognitive restructuring, a core component of the group-based CBT intervention. Their reflections revealed both the transformative potential and the limitations of this strategy, shaped by individual histories, expectations and the shared group context. This component of the group sessions was raised by 70% of participants, and over 51% of those participants expressed that it had a positive impact throughout the course of therapy.
Challenges in engaging with cognitive restructuring
Some participants (12.5%) expressed difficulty engaging with cognitive restructuring, particularly when their thoughts reflected lived experiences and accurate appraisals of past or ongoing social challenges, rather than being perceived as inaccurate or unhelpful appraisals. For autistic adults, many negative cognitions arise not from unfounded fears but from repeated experiences of social exclusion. This created a tension in therapy, as challenging these thoughts risked invalidating concerns that participants felt were realistic and protective. One participant explained, ‘I often perceived my thoughts as neutral or realistic, not negative’ (Participant 2). Similarly, another participant questioned the relevance of the technique altogether, stating ‘I didn’t find it helpful’ (Participant 1). These accounts underscore the importance of carefully distinguishing between thought patterns that can be usefully restructured (such as overgeneralizations or catastrophizing) and those that reflect genuine risks or recurring social experiences of exclusion. Without this nuance and individualized care, cognitive restructuring may fail to resonate with autistic adults, or worse, contribute to feelings of invalidation.
For some, the challenge lay in the depth and persistence of core beliefs. One participant reflected on long-standing struggles with self-perception:
If the core belief is ‘I’m incapable’, I don’t know if I’ve ever had an experience that’s helped me reshape those. (Participant 4)
For other participants, this sense of hopelessness was compounded by previous therapeutic experiences that had failed to address these deeply rooted beliefs. Another participant acknowledged the partial effectiveness of cognitive restructuring, suggesting that it was ‘not the only kind of solution’ (Participant 3), and raised the need for more individualized support to complement group-based strategies.
Benefits and emerging insights
Despite these challenges, many participants (75%) described cognitive restructuring as valuable to their therapeutic process. One participant, initially sceptical, shared: ‘Cognitive restructuring seems too good to be true to someone with the well-worn neural pathways of a decade of depression’ (Participant 5) and went on to describe how the technique helped them ‘locate better, brighter metaphysical routes’ in their thinking (Participant 5).
The group setting itself emerged as an effective facilitator of cognitive restructuring, offering reassurance in a context in which participants’ experiences of negative thinking were validated rather than dismissed. Within the group, participants witnessed peers dealing with the same doubts and sometimes distorted predictions, which helped normalize their struggles and made the cognitive restructuring part of the intervention feel more authentic. One participant described the collective experience of confronting difficult tasks:
Having that same response but in a group of other people who also think they can’t, and then we all end up doing it. It’s very reassuring. (Participant 6)
Others highlighted how cognitive restructuring increased their awareness of habitual self-criticism. One participant reflected,
I realized how often I have negative thoughts . . . Often, you just think you’re being hard on yourself to push for improvement, but it’s not always true. (Participant 7)
Recognizing these patterns and learning that such thoughts could be challenged was described as ‘really beneficial’ (Participant 7).
Facing the challenge together: autistic adults’ experiences with exposure tasks
General experiences with exposure tasks
Cognitive restructuring appeared to be integrated with participants’ engagement in exposure tasks. While restructuring created space to reflect on negative thought patterns, exposure exercises provided a tangible context in which these thoughts could be tested in real-life situations. This component of the programme was raised by 85% of participants, with most (56%) expressing that it had a positive impact throughout the course of therapy, while 43% also reported challenges.
Exposure as a source of heightened distress. For some participants (26%), exposure tasks triggered emotional responses that persisted during, and sometimes after, the proposed exercises. Rather than producing the expected reduction in anxiety, the tasks amplified distress for some participants. One participant described how the tasks exacerbated their anxiety:
The exposure tasks . . . made me more anxious in general. (Participant 8)
Another participant raised concerns about the potential for harm, noting that the group format did not always meet the needs of those with trauma histories or dissociative responses. For these individuals, exposure tasks were more demanding and signalled the value of additional support.
Exposure as a catalyst for insight and growth.
While some participants found exposure tasks overwhelming, others described them as among the most meaningful and transformative components of the programme (74%). These contrasting experiences show the diversity of autistic adults’ responses to structured anxiety interventions and suggest that, when carefully supported, exposure can foster meaningful change and improve confidence. One participant appreciated the way the task was introduced, noting:
I think it worked well that it was sort of dropped on us suddenly . . . if we had been let know a week in advance, I would have spent the whole week worrying. (Participant 2)
This comment reflects how spontaneous implementation may reduce anticipatory anxiety, making the experience more manageable.
Others described how the tasks bridged the gap between theoretical discussion and lived experience. One participant shared,
At first, we were just talking about them in theory . . . But when we actually did them, it clicked . . . Afterwards, I spent the week thinking about my actions and whether they were, in some way, exposure tasks themselves. (Participant 7)
This reflection demonstrates how experiential engagement can enable participants to recognize and extend therapeutic principles beyond the group setting and into everyday life.
The group setting also emerged as a significant factor in shaping participants’ experiences. For some, the collective undertaking of exposure provided reassurance and support, transforming what might otherwise have been an isolating challenge into a shared accomplishment:
I think I really liked doing it with a group . . . It’s helpful to kind of prove to yourself that you can go into situations on your own without having to rely on others. (Participant 3)
Autistic adults’ reflections on the speech task
The speech task, an exposure exercise adapted from straight social anxiety interventions, represented a more focused and social application of exposure within the group, designed to simulate a spontaneous public speaking, one of the most anxiety-provoking situations for individuals with social anxiety. By inviting participants to select a topic and deliver a brief speech in front of peers, the exercise aimed to elicit heightened anxiety in a controlled, supportive setting. In this way, the task extended the broader exposure principles discussed earlier, offering participants the chance to test cognitive shifts in real time and to experience both the challenges and potential rewards of confronting feared situations.
Tensions between structure and emotional safety. Despite its therapeutic intent, the speech task revealed tensions between exposure-based challenge and the need for emotional safety. Some participants (11%) described the speech task as anxiety-provoking, particularly due to its open-ended structure and lack of ideal preparation time. One participant reflected on the discomfort of waiting for others to volunteer to do the task, describing the atmosphere as ‘anxiety soup’, where prolonged anticipation intensified distress rather than alleviating it:
Waiting for other people to decide on their topics made everything kind of worse . . . it just sort of meant everyone sat in that anxiety soup. (Participant 8)
Others found the absence of clear topic guidance disorienting, noting that the open-ended format placed additional cognitive demands on participants already managing heightened anxiety. Several participants suggested that providing a list of simple, non-threatening themes might have reduced this burden and made the task feel more accessible. For some, the challenge of topic selection also intersected with the nature of the content chosen. When participants selected themes that touched on deeply held negative core beliefs, the task often intensified distress rather than reducing it. One participant noted that the task did not produce the expected reduction in anxiety, stating:
I feel like it didn’t get . . . what was expected to happen, like a drop in anxiety. (Participant 9)
In contrast, choosing topics aligned with personal interests or areas of confidence appeared to lessen the emotional load, making the task more manageable and even enjoyable.
Opportunities for empowerment and connection. Despite these challenges, many participants (50%) found the speech task to be a meaningful experience. One participant described how the timing of the task aligned with a real-world presentation, allowing them to rehearse in a low-stakes, supportive environment:
It was fantastic! I had a presentation the very next day . . . It also reduced my anxiety for the actual presentation. Plus, the feedback I got from the group was so positive and supportive. (Participant 7)
Others shared the personal and relational value of the task. One participant stated that it became their favourite session, noting how the experience facilitated connection with other members of the group:
It ended up being my favourite session because it felt more personal and connected. (Participant 10)
Another participant found the task approachable and engaging, particularly because they spoke about a topic they were interested in:
I think it helped a little, mainly because I was talking about a topic I’m interested in, so that made it easier for me. (Participant 11)
These reflections suggest that the speech task, when appropriately scaffolded by the group and adapted to the needs of participants, became a space for practicing coping skills and receiving affirming feedback.
Building confidence through connection: autistic adults’ experiences with social strategies as part of therapy
The speech task functioned as a structured opportunity for participants to practise social anxiety management strategies, as well as an exposure exercise. For many participants, standing up to speak in front of the group required drawing on the conversational strategies introduced in the programme to support exposure. In this sense, the speech task acted as a bridge between the anxiety-focused and social strategies aspects of therapy.
More than 95% of participants reflected on the social strategies component of the CBT programme as a valuable and often transformative part of their therapeutic experience. For many, the explicit focus on conversational strategies and interpersonal dynamics provided practical tools that supported exposure and a more intentional engagement in social situations.
Structure and clarity in social interaction
Several participants described this component as offering a sense of structure and predictability in navigating conversations. One participant shared,
That was one of the most helpful parts . . . seeing there are these things you can do . . . or like having a pattern to follow helped. (Participant 12)
Others emphasized how the social structuring aspect of the intervention provided an important foundation. One participant reflected,
It gave me a kind of structure to social situations. Like, not in a strict or formal way, but it provided a foundation, something I never really got before. (Participant 12)
This shows the importance of accessible, concrete strategies that support autistic individuals in developing their own social and communication style. Participants also appreciated talking about specific strategies, such as how to exit conversations. One individual noted,
Learning concrete strategies gives me something to hold onto and practice . . . I also liked learning about how to exit conversations. I often feel trapped in them because I’m too afraid of hurting someone’s feelings. (Participant 13)
Refining familiar skills and gaining new insights. While most participants found the social strategies, a few expressed that the content felt familiar due to prior experiences with therapy or self-directed learning (6%). One participant remarked,
The first three or four weeks were probably the least useful to me . . . I’ve lived through those experiences, and I’ve sort of learned to . . . lessen the curve of anxiety. (Participant 14)
However, for participants who came in with previous exposure to similar strategies, the sessions offered opportunities for refinement and deeper understanding. One participant found value in the breakdown of conversational mechanics:
The conversation skills . . . like exiting conversations, maintaining them . . . that was probably the most useful strategy. (Participant 15)
Another participant reflected on how the social coping skills component of the therapy provided support for evaluating and adjusting their communication:
Better understanding social skills . . . it provides a support to assess conversation . . . so you can identify flaws which could be used as potential prospects in your conversation. (Participant 16)
Participants reinforced that the social strategies part of the program strengthened exposure tasks by providing practical support that could be applied and consolidated during the speech exercise.
Autistic adults’ reflections on tools for managing social anxiety
The social strategies component described earlier provided participants with practical frameworks for navigating social interactions, but many emphasized that these strategies became most useful when paired with concrete strategies for managing the anxiety that accompanied them. In this way, the anxiety management strategies introduced in the programme equipped participants with methods of regulating the emotional intensity of social interactions. Participants reflected on this combination as key to feeling more confident and capable in social situations.
The anxiety management tools, ranging from structured exercises to communication strategies, were experienced as both empowering and, at times, limited in their relevance.
Structure as a source of stability
Several participants (40%) found the structured nature of the anxiety management tools particularly helpful in making sense of their emotional experiences. One participant described how assigning numerical values to their anxiety provided a sense of control, allowing them to externalize and evaluate their emotional state more objectively. Others appreciated the use of visual frameworks, such as behavioural experiment tables, which allowed them to compare predictions with actual outcomes. These exercises were described as useful in bridging the gap between abstract concepts and lived experience, offering a tangible way to reflect on anxiety-provoking situations and their consequences.
Communication strategies and self-awareness
Participants also highlighted the value of learning new communication strategies, particularly the use of ‘I’ statements. These strategies were seen as tools for expressing oneself more clearly and reducing interpersonal conflict. One participant noted that such strategies helped them feel more confident in social interactions, as they provided a language for articulating needs and boundaries without escalating tension. Across these reflections, participants shared the importance of having practical, adaptable tools and strategies that could be applied beyond the therapy setting.
Reimagining the group experience: participant recommendations for future iterations
While participants described in detail how they engaged with specific CBT strategies such as cognitive restructuring, exposure, social strategies and anxiety management, their accounts rarely ended there. These encounters prompted reflection on what aspects of the programme felt most supportive and where gaps or tensions arose. This way, the lived experience of the therapeutic components became the foundation for envisioning a more responsive and inclusive programme. The second theme, Reimagining the Group Experience: Participant Recommendations for Future Iterations, captures these reflections. Here, participants moved beyond recounting what happened in the group to actively considering how the intervention might be reshaped, not only to ease practical barriers but also to create a therapeutic space marked by greater transparency, flexibility and inclusivity.
Creating safety through structure and sensitivity
For many participants, their direct encounters with CBT strategies not only shaped their therapeutic process but also prompted reflection on what could be improved in the group intervention. The experience of engaging with exposure tasks, cognitive restructuring and role-play highlighted the importance of feeling safe enough to take risks. Safety, in this context, was not taken for granted. Participants reflected on ways the programme could further integrate trauma-informed principles, noting that past experiences in therapy often heightened their apprehension. Maintaining a setting that felt both structured and sensitive was viewed as important for supporting meaningful engagement.
One way participants envisioned enhancing their sense of safety was through greater transparency about what each session would involve. For some, unpredictability increased anxiety and made it harder to stay engaged in the therapeutic work. As one participant explained,
Having a kind of . . . this is vaguely what we’ll be covering over the weeks before we start doing it . . . I think would have been helpful to me. (Participant 1)
Environment and engagement
Safety was also connected to the physical and social environment of the group. Some participants suggested that offering more flexible seating options, such as sitting in a circle or on the floor, could further support a sense of inclusivity. Alongside environmental adjustments, participants shared the value of hands-on learning as a means of making CBT strategies more tangible. For instance, role-playing exercises were remembered as moments where theory gave way to practice:
Give maybe more practical . . . more like actually doing the actions . . . doing role-playing that . . . after would be useful. (Participant 17)
Extending connection beyond the room
Some participants noted that they wanted more time to consolidate learning, whether through a longer programme duration or additional spaces for connection between sessions. One suggestion was to create an online platform for sharing resources:
‘Potentially we could have . . . an online space where resources can be uploaded and we can all access . . . it’s a way to build rapport or have accountability, stay communicating . . . and access the resources not in email’. (Participant 4)
Safety was framed as continuity, having reliable ways to remain connected to peers, facilitators and materials so that therapeutic progress did not feel fragmented.
Balancing individual needs and group dynamics
Alongside suggestions to build on existing strengths in safety, structure and continuity, participants also made suggestions on how the programme might better accommodate the diversity of needs present in a group context. They reflected on the reality that not every CBT component would resonate equally with every participant, yet they reinforced the importance of respecting this variation as part of the collective learning process. Engaging with CBT strategies in a group setting inevitably meant that not every session or activity spoke directly to everyone’s individual circumstances. Participants often expressed an appreciation for the collective dimension of the group, acknowledging that what felt less relevant for them might be essential for others. One participant acknowledged this dynamic:
The first three or four weeks were probably the least useful to me, and that would not apply to everyone else in the group, and I understand that. (Participant 14)
This reflection illustratesrecognition of the diversity of needs within the group and also respect for the therapeutic process as something more than an individual journey. For some, this meant developing patience with content that felt less personally applicable; for others, it meant recognizing value in listening to peers’ experiences, even when those experiences diverged from their own.
These reflections expand the idea of what it means to ‘benefit’ from the group. They suggest that a successful programme balances individual trajectories with collective dynamics, creating a space where variation is not a limitation but a resource. In this sense, participants’ recommendations for future iterations extend beyond practical adjustments; they envision a group culture that values inclusivity, reciprocity and respect for the diverse ways people grow within a shared therapeutic journey.
Discussion
This study explored autistic adults’ experiences of participating in a modified group CBT intervention for social anxiety, focusing specifically on how core CBT components were perceived, and how they could be adapted and applied in practice. Participants reflected on the usefulness and limitations of core CBT components, including cognitive restructuring, exposure tasks, speech exercises, social strategies, and offered recommendations for future iterations. Their insights revealed the overall value of CBT-based approaches for social anxiety intervention, while emphaising how to align therapeutic techniques with the lived experiences and specific needs of autistic individuals.
Effectiveness of tailored CBT techniques
Participants generally perceived cognitive restructuring as effective for increasing self-awareness and challenging habitual negative thought patterns, aligning with evidence that CBT can promote cognitive flexibility, giving clear strategis and reduce anxiety in autistic populations (Spain et al., 2017; White et al., 2012). However, its impact was less pronounced when social fears reflected perceived realistic concerns or were linked to strong negative core beliefs that were shaped by past negative experiences. In this regard, participants reported concern that cognitive-restructuring can be less helpful when it is viewed as invalidating and dismissing real perceived needs. Similarly, some autistic people reported greater difficulty identifying contrary evidence to thoughts, with some reporting an absence of perceived successful past social interactions. Similar tensions have been reported by Wilson (2024), who found that autistic individuals can perceive cognitive restructuring as invalidating if it is used to disregard the legitimacy of social anxieties. Overall, however, these findings suggest that autistic people reported benefit from cognitive restructuring approaches when used in a collaborative context. In this population, there may be a greater role of persistent core beliefs that can make restructuring more difficult (Benevides et al., 2020).
Exposure tasks were frequently described as beneficial for reducing anxiety and encouraging behavioural experimentation, particularly when activities were clearly explained, scaffolded and embedded in a predictable group routine. These accounts are consistent with recommendations that exposure-based strategies for autistic individuals prioritise structure, preparation and opportunities for graded practice (Bemmer et al., 2021; Spain et al., 2016). At the same time, a subset of participants reported that exposure exercises could be emotionally overwhelming, especially in the context of trauma histories or highly stimulating environments. For these participants, exposure tasks felt more demanding, suggesting a need for additional supports and greater flexibility in the delivery of these components. Overall, this study shows that exposure can be both an effective and a challenging component of CBT for autistic adults, and its implementation may need to be carefully tailored to individual histories, sensory profiles and coping strategies (Roisenberg, Boulton, Thomas, et al., 2025; Rumney & MacMahon, 2017).
Social strategies and the ethics of adaptation
The social strategies component of the intervention was widely regarded as beneficial, offering structured strategies that supported confidence and reduced uncertainty in social interactions. These findings differ from some concerns in the literature about ‘social skills training’ approaches inadvertently causing harm through deficit based models that emphasise alignment with neurotypical communication norms. (Ashman et al., 2017; Bottema-Beutel et al., 2018; Monahan et al., 2021; Spain et al., 2017). Our findings suggest that when social strategies are framed as a choice to implement, rather than a correction of a perceived deficit, social strategies are almost uniformly seen as supportive and beneficial. Such strategies were viewed as promoting an individual’s efficacy, autonomy and authenticity, while also reducing confusion, helplessness and fear (Evans et al., 2024; Kupferstein, 2018). Overall, participants reported appreciation and value in being able to understand social interaction mechanics and to be empowered to make their own choices about participation.
Consistent with this approach, Roisenberg, Boulton, Thomas and Guastella (2025) found that autistic adults who participated in a modified CBT group intervention experienced significant reductions in social anxiety, while camouflaging levels remained largely stable, with reductions evident among participants who showed the greatest social anxiety symptom improvement. When considered alongside the present qualitative findings, this pattern suggests that CBT-based interventions can support meaningful change without increasing pressure to mask. Supporting individuals to flexibly choose strategies based on context, function and personal values may help address social anxiety while respecting autonomy, authenticity and the protective role some behaviours may serve (Johnson et al., 2025).
Psychoeducation and emotional insight
Participants valued the psychoeducational aspects of the programme, particularly those who were newly diagnosed. Group discussions helped normalize common challenges and fostered a sense of shared understanding. These findings are consistent with research suggesting that psychoeducation can enhance therapeutic engagement and emotional insight among autistic individuals (Wilson & Gullon-Scott, 2024a, 2024b).
Several participants noted difficulties in identifying and articulating their emotional states, including challenges in rating anxiety levels. This aligns with existing literature on alexithymia in autism (Cai et al., 2018) and recent findings that CBT may support improvements in emotional awareness (Kuroda et al., 2022), underscoring the importance of integrating emotion-focused strategies into CBT programmes to enhance accessibility and effectiveness.
Challenges in implementing CBT strategies
The challenges identified in this study reveal broader concerns in adapting CBT for autistic adults. Existing literature argues that traditional CBT frameworks can assume fears are disproportionate or irrational, which can conflict with autistic individuals’ lived experiences of exclusion and stigma (Wilson, 2024). Our findings reinforce this critique, as many participants viewed their social anxiety as rooted in repeated invalidation, suggesting that interventions must validate these experiences rather than pathologize them (Benevides et al., 2020).
Exposure-based strategies illustrate this tension clearly. While widely regarded as a cornerstone of CBT, exposure tasks can evoke distress when introduced without adequate scaffolding, a concern echoed in Wilson and Gullon-Scott’s (2024a) work, which cautions that rigid exposure protocols may disrupt existing coping mechanisms. Literature increasingly advocates for flexible adaptations, such as individualized pacing, collaborative planning and integration of sensory accommodations, to mitigate these risks (Bemmer et al., 2021; Spain et al., 2017).
Cognitive restructuring presents similar complexities. Research suggests that deeply rooted negative beliefs about the self, often shaped by long-standing experiences of rejection, are difficult to modify within short intervention windows (Wilson, 2024). This raises questions about the feasibility of addressing such beliefs in group-based formats alone. Scholars have proposed supplementing group CBT with individualized sessions to allow for deeper exploration of these beliefs and their relational context (White et al., 2012). Importantly, our findings align with evidence that peer support can enhance therapeutic engagement by normalizing fears and fostering validation (Rumney & MacMahon, 2017), showing the value of group processes even when individual challenges persist.
Implications for clinical practice
The findings suggest several implications for adapting CBT with autistic adults. First, structured and predictable sessions, alongside advance notice and collaborative planning of exposure tasks, may help reduce anticipatory anxiety and enhance a sense of control (Wilson & Gullon-Scott, 2024a). Sensory accommodations, including flexible seating arrangements and access to quiet spaces, are also essential for creating accessible therapeutic environments (Bemmer et al., 2021). Some participants also suggested that supplementary online platforms or between-session resources could help maintain continuity and support skill consolidation outside the group space.
Cognitive interventions that validate social fears and recognise the protective and self-regulatory role of some safety behaviours may be more responsive to participants’ lived experiences. Approaches that emphasize authenticity and self-acceptance can support engagement in social situations in ways that feel emotionally safe and personally meaningful (Benevides et al., 2020).
Collectively, these findings reinforce the need for nuanced, multi-layered approaches that combine structured CBT techniques with trauma-informed care and flexible delivery models. In its true form, CBT should never be rigid and dismissing of individual need. However, when these approaches have been reported to be applied poorly in practice, many participants reported experiencing these reactions (Brookman-Frazee et al. 2012). Future adaptations should prioritize autonomy, emotional insight and relational safety to promote long-term well-being (Wilson & Gullon-Scott, 2024a). Further research is warranted to examine how these principles influence outcomes across diverse autistic populations and to explore strategies for integrating individual therapy alongside group interventions to address complex cognitive and emotional needs.
Although the present study focused on autistic adults, many of the principles identified align closely with established CBT adaptations for older children and adolescents on the autism spectrum. Prior research indicates that structured and predictable sessions, sensory and environmental accommodations, and flexible, modular delivery formats are commonly recommended in youth-focused interventions (Reaven et al., 2023; Storch et al., 2013; White et al., 2012; Wood et al., 2009). This convergence suggests that core principles in the current findings, such as prioritizing predictability, validating lived experiences and supporting autonomy, may have relevance across developmental stages, while requiring age-appropriate tailoring and caregiver or school-based involvement for younger populations.
Limitations
Several limitations should be considered when interpreting these findings. First, the sample was not representative of the broader autistic population. All participants were help-seeking adults whose cognitive profiles met the requirements of the programme and who voluntarily enrolled in a CBT group for social anxiety. As such, the findings may not reflect the experiences of autistic individuals with intellectual disability, those from a broader age range, or individuals who are not actively seeking therapy. In addition, we did not collect data on participants’ ethnicity, which limits our ability to comment on the cultural or racial diversity of the sample. Future research should aim to include and report on a wider range of demographic characteristics to enhance the inclusivity and generalizability of findings.
Second, the study relied on self-reported experiences, which introduces the possibility of response bias. While some participants provided rich, detailed reflections, others offered more limited accounts, potentially affecting the depth and balance of the thematic analysis. The 8-week intervention time frame may also have constrained participants’ ability to assess the long-term impact of the strategies introduced. Although the study incorporated strong community involvement, including the contribution of a neurodivergent co-researcher who was also a former participant of the group, formal member checking or respondent validation was not conducted. This may limit opportunities for participants to directly verify interpretations. Future research could integrate these strategies to further enhance credibility and transparency.
Third, the study focused exclusively on participant perspectives and did not include input from facilitators or clinicians. This limits insight into implementation challenges, therapist adaptations and potential biases that may have influenced participant engagement. Future research should incorporate facilitator perspectives to better understand how therapeutic delivery interacts with participant experience.
Fourth, to contextualize the qualitative findings, we examined whether participants who took part in the qualitative interviews differed systematically from those who did not. Baseline comparisons showed no significant differences in demographics (age, gender, IQ), social anxiety severity, social responsiveness, functional impairment or camouflaging behaviours. Exploratory analyses also indicated no differences in pre- to post-intervention changes in social anxiety or camouflaging. These findings suggest the qualitative sample was broadly representative of the intervention cohort. However, because interview participation was voluntary, unmeasured factors (e.g. comfort with verbal reflection, research engagement) may have influenced participation. Future studies should examine predictors of qualitative follow-up more directly.
Finally, participants were given the option to choose their interviewer. Most selected a group coordinator, likely due to feelings of safety and familiarity. While this may have fostered openness, it could also have led to hesitancy in expressing critical feedback. Those who opted for an independent interviewer may have felt freer to share more candid reflections. In addition, individuals who declined participation in the qualitative component or the group programme altogether may hold different views that were not captured in this study.
Future directions and conclusions
This study highlights the need for continued refinement of CBT for autistic adults, with approaches that prioritize psychological safety, sensory accessibility and validation of lived experiences. Future interventions should further integrate autism and trauma-informed principles and explicitly acknowledge the impact of discrimination and social invalidation. Strategies such as coping with stigma, fostering self-advocacy and strengthening community connections may enhance resilience and support authentic social engagement. This study highlights an urgent need for training programmes that can integrate autistic needs and perspectives into high quality CBT therapies for community practice.
This article forms part of a broader qualitative investigation into autistic adults’ experiences of a modified CBT group programme for social anxiety. In the companion paper, we reported that relational elements, such as feeling understood by peers, reduced pressure to mask and a sense of belonging, were central to engagement (Roisenberg et al., 2025a). The present analysis extends those findings by showing how specific CBT components were experienced within that relational context. For example, exposure tasks and speech exercises were often described as more manageable when embedded in a trusted group, while cognitive restructuring felt more impactful when peers validated shared doubts and fears. Together, the two studies suggest that CBT components and group processes interact, and both contribute to meaningful change.
According to participants' recommendations, adaptations should include structural and environmental modifications, such as predictable session formats, flexible pacing and sensory accommodations. Embedding peer-led or co-facilitated components can further promote belonging and mutual understanding, while reducing reliance on neurotypical communication norms.
Overall, this study provides a qualitative evaluation that largely endorses many aspects of CBT for social anxiety. Ultimately, these findings emphasise flexible, autonomy-supportive frameworks that centre emotional insight and relational safety. Future research should examine how these principles influence outcomes across diverse autistic populations and explore integrated models that combine group-based CBT with individualized support to address complex cognitive and emotional needs.
Supplemental Material
sj-docx-1-aut-10.1177_13623613261424830 – Supplemental material for A qualitative evaluation of cognitive-behavioural therapy components for social anxiety in autistic adults: Lived experiences from a modified group program
Supplemental material, sj-docx-1-aut-10.1177_13623613261424830 for A qualitative evaluation of cognitive-behavioural therapy components for social anxiety in autistic adults: Lived experiences from a modified group program by Bruna B Roisenberg, Kelsie A Boulton, Emma E Thomas, Nina Perry, Dorothy Yu and Adam J Guastella in Autism
Footnotes
Programme and ethics approval
Approval for this study was granted by the University of Sydney Human Research Ethics Committee (Approval No. 2015/365). Before their involvement in the study, all participants provided written informed consent.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the University of Sydney Tuition Fee Scholarship and University of Sydney International Stipend Scholarship.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data availability statement
Interviews questions and other materials can be made available on request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.