
Abstract
Sensory reactivity differences are a diagnostic criterion of autism. Sensory hyperreactivity has been linked to intolerance of uncertainty and anxiety in autistic children. However, research is yet to explore the mediating relationships or sensory hyporeactivity, seeking and anxiety subtypes in preschool-age autistic children. Therefore, we aimed to elucidate the relationships between sensory reactivity, intolerance of uncertainty and anxiety subtypes in a heterogeneous group of 54 preschool-age autistic children, age 3–5 years, using observation and parent-report assessments. Correlational analysis found sensory hyperreactivity, intolerance of uncertainty and total anxiety were significantly intercorrelated. In addition, sensory hyperreactivity was significantly correlated with separation anxiety when controlling for autism traits. Serial mediation analyses indicated significant full mediation between sensory hyperreactivity and anxiety through intolerance of uncertainty, and significant full mediation between sensory hyperreactivity and intolerance of uncertainty through anxiety. Our results suggest that sensory hyperreactivity is a key early factor in the development of anxiety, and supports that intolerance of uncertainty is an important interrelated construct in the development and maintenance of anxiety in autism. Our findings have important implications for the development of effective interventions. However, due to limitations with the measures, our research also highlights a pressing need for objective assessments of anxiety and intolerance of uncertainty that can be used with preschool-age autistic children.
Lay abstract
This study found links between greater sensory hyperreactivity (e.g., over-sensitive to sensory input), intolerance of uncertainty and anxiety, including separation anxiety, in autistic pre-schoolers. Sensory hyperreactivity may predict both anxiety and intolerance of uncertainty, and anxiety and intolerance of uncertainty may both be mutually important, mediating factors. These findings have implications for early anxiety interventions. But there is a pressing need for objective assessments that can be used with preschool-age autistic children.
Introduction
Autism spectrum conditions (ASC) are neurodevelopmental conditions with characteristics related to restricted and repetitive behaviours and interests (RRBs), and social interaction and communication differences (Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013)). Sensory reactivity differences, including sensory hyperreactivity (e.g. strong reaction to touch), hyporeactivity (e.g. no or slower reaction to sounds) and seeking (e.g. fascinated by lights) are commonly experienced by approximately 65%–85% of autistic 1 children (Leekam et al., 2007; Miller et al., 2007; Tavassoli et al., 2016). Due to this prevalence, sensory reactivity differences have become a diagnostic criterion for ASC, under the RRBs domain (DSM-5; American Psychiatric Association, 2013). However, they are also common across other neurodevelopmental conditions, such as attention deficit hyperactivity disorder (ADHD; Miller et al., 2012). Sensory reactivity differences can be experienced differentially and across a range of modalities, such as vision, hearing and touch (Miller et al., 2007). Although some sensory experiences may be pleasant, others can be extremely distressing, which can greatly impact developmental outcomes and quality of life (Pfeiffer et al., 2005; Uljarević et al., 2016). Sensory hyperreactivity has previously been linked to anxiety and intolerance of uncertainty (IU) in autistic individuals (Carpenter et al., 2019; Green et al., 2012; Hwang et al., 2019; Neil et al., 2016; Pfeiffer et al., 2005; Uljarević et al., 2016). However, research has yet to explore the relationship between sensory reactivity differences, including hyperreactivity, hyporeactivity and seeking, IU and anxiety subtypes in preschool-age autistic children. Understanding the early emergence of these relationships has important implications for early anxiety interventions.
Sensory reactivity differences and anxiety
Autistic children are twice as likely to develop an anxiety condition compared to non-autistic children (van Steensel et al., 2011). Research has suggested that around 49% of autistic children will have at least one co-occurring anxiety condition: commonly generalised anxiety disorder (GAD), social anxiety, or specific phobia, or anxiety-related conditions such as obsessive–compulsive disorder (OCD) (Simonoff et al., 2008; van Steensel et al., 2011; White et al., 2009). Anxiety diagnoses are not always straight forward due to some degree of overlap between traits common in autistic children and anxiety symptomology, for instance, social avoidance which can be present in both autism and social anxiety (Kerns & Kendall, 2012; White et al., 2009). As well as presenting with traditional anxiety symptomology, autistic people can also present with some unique symptoms, such as unusual phobias, sensory fears, social distress unrelated to fears of negative evaluation and compulsive behaviours that are not driven by distress relief (Kerns et al., 2014, 2017, 2020; South & Rodgers, 2017). Anxiety symptoms develop early (i.e. before the age of 6 years) and are enhanced in autistic children and increase over time (Vasa et al., 2020). Thus, there is an imperative need to identify early risk factors.
Research has repeatedly shown links between sensory hyperreactivity and anxiety in autistic children (Green & Ben-Sasson, 2010; Green et al., 2012; Pfeiffer et al., 2005; Vasa et al., 2020; Wigham et al., 2015). Sensory hyperreactivity may be an early risk factor for the development of anxiety as it has been suggested to emerge earlier and to unidirectionally predict anxiety in both autistic and non-autistic samples (Carpenter et al., 2019; Green et al., 2012). Green et al. (2012) explored the bidirectional relationship between sensory hyperreactivity and anxiety in autistic toddlers in a longitudinal study. They found that while sensory hyperreactivity remained stable over time, anxiety increased. Furthermore, sensory hyperreactivity predicted an increase in anxiety; however, anxiety did not predict changes in sensory hyperreactivity (Green et al., 2012). There is also research in autistic children and adolescents to suggest that sensory hyperreactivity is implicated in specific anxiety conditions, such as separation anxiety, social anxiety and specific phobia (Black et al., 2017; MacLennan et al., 2020; Pickard et al., 2020). Understanding if sensory reactivity is an early predictor for certain anxiety symptomology pertaining to the current diagnostic criteria has important clinical implications for early identification and targeted intervention therapies.
There is limited and inconclusive research into the relationships between both sensory hyporeactivity, and sensory seeking and anxiety in autistic children. Some research has found links between sensory hyporeactivity and anxiety in autistic children and adolescents (Glod et al., 2019), as well as specific links to social anxiety (MacLennan et al., 2020). However, links between sensory hyporeactivity and anxiety have not been consistently found in research (Wigham et al., 2015). Sensory seeking is often neglected in research and direct links to anxiety have rarely been found (Levit-Binnun et al., 2014; Lidstone et al., 2014; MacLennan et al., 2020). There is evidence to suggest that sensory seeking may be indirectly linked with anxiety through sensory hyperreactivity and over-focussing behaviours (Liss et al., 2006). Therefore, it would be advantageous to continue to explore how both sensory hyporeactivity and seeking relate to anxiety in autistic children.
IU, sensory reactivity differences and anxiety
IU is broadly characterised by a difficulty with situations or contexts that are unforeseen or unpredictable (Buhr & Dugas, 2006). It is considered to be a key cognitive component in the development and maintenance of anxiety through negatively appraising ambiguous or uncertain events (Dugas et al., 1998; Freeston et al., 1994). Greater IU has been linked with anxiety in non-autistic populations, and may be a key transdiagnostic feature across anxiety conditions (Carleton et al., 2012). Although argued to be a distinct construct, there is also some degree of similarity between the characteristics of IU and some autistic traits, such as difficulty with change and unpredictability (Boulter et al., 2014; Chamberlain et al., 2013). However, IU has been identified as a recognisable construct in autistic children and has been found to be higher in autistic groups (Boulter et al., 2014; Hodgson et al., 2017; Vasa et al., 2018).
Existing research has aimed to elucidate the relationship between sensory reactivity, anxiety and IU. A key theoretical model of anxiety in autism by South and Rodgers (2017) proposes that IU is a principal mediator in the relationship between sensory reactivity and anxiety. In support of this, research has found IU to partially mediate the relationship between both sensory hyperreactivity, and hyporeactivity and anxiety in autistic adults (Hwang et al., 2019). However, there is currently mixed, and sometimes conflicting, evidence to support this. Research has found IU to mediate the relationship between autism traits and anxiety, as well as autism traits and sensory hyperreactivity (Boulter et al., 2014; Hwang et al., 2019; Neil et al., 2016). In addition, research has found anxiety to mediate the relationship between IU and sensory hyperreactivity in autistic children (Neil et al., 2016). Therefore, research is still needed to elucidate the relationship between sensory reactivity, IU and anxiety in autistic children.
The present study
Symptoms of anxiety are present in autistic children at an early age and there is an early, unidirectional association between sensory hyperreactivity and anxiety in autistic toddlers. Although there may be a differential relationship between sensory hyperreactivity and symptoms associated with anxiety subtypes, such as social anxiety and specific phobia, this is an under-researched area. In addition, sensory hyporeactivity and seeking are often neglected in research, and there is inconclusive evidence of the relationships between sensory reactivity, IU and anxiety.
Fundamentally, the links between sensory reactivity, IU and anxiety have only been explored in autistic children above the age of 6 years, without intellectual disability (ID) and with proficient language skills, and research with preschool-age autistic children (age 3–5 years) is yet to be done. Targeting risk factors for anxiety in its earliest stages is important to improve later outcomes (Rapee et al., 2010; Yap et al., 2016). Ages 3–5 years are a critical time when sensory reactivity differences and anxiety symptoms are emerging in autistic children, and early interventions for anxiety already show efficacy (Ben-Sasson et al., 2007, 2008; Driscoll et al., 2020; Green et al., 2012; Vasa et al., 2020).
Therefore, we aimed to elucidate the relationship between sensory reactivity differences, IU and anxiety in preschool-age autistic children. First, in line with previous findings (Carpenter et al., 2019; Neil et al., 2016; Pfeiffer et al., 2005; Uljarević et al., 2016; Wigham et al., 2015), we expected to find greater sensory hyperreactivity to be significantly related to greater anxiety symptoms, and for IU to be a mediator in the predictive relationship. Secondly, as previous work including ours has found a differential relationship between sensory hyperreactivity and anxiety subtypes in older children (Black et al., 2017; MacLennan et al., 2020), we explored if sensory reactivity and IU were differentially related to anxiety subtypes, including GAD, separation anxiety symptoms, OCD, physical injury fears and social anxiety symptoms.
Moreover, due to conflicting theoretical models in existing literature, we aimed to test the predictive relationship between sensory reactivity, anxiety and IU. We expected that sensory hyperreactivity would predict anxiety, as hyperreactivity has been shown to predict anxiety unidirectionally (Green et al., 2012). But that the relationship between sensory hyperreactivity and anxiety would be mediated by IU, as IU has consistently been found to be a mediating, transdiagnostic construct (Boulter et al., 2014; Hwang et al., 2019; Neil et al., 2016; Wigham et al., 2015).
Methods
Participants
In total, 65 children with (1) a clinical diagnosis of autism or (2) suspected autism were recruited for this study. Fifty-four children (41 males, 13 females) aged 3–5 years (mean (M) = 4.02, standard deviation (SD) = 0.77) met inclusion criteria of (1) having a formal clinical diagnosis of autism which included a direct observation as well as developmental history (n = 42) or (2) having suspected autism and meeting cut-off scores on the Autism Diagnostic Observation Schedule (ADOS-2; Lord et al., 2012) (Module 1 few-to-no words cut-off: 11; Module 1 some words cut-off: 8; Module 2 <5 years cut-off: 7; Module 2 ⩾5 years cut-off: 8), and the Autism Spectrum Quotient: Child Version (AQ; Auyeung et al., 2008) (cut-off ⩾76) (n = 12), and were therefore included in the final analysis. Thirty-one children completed a Module 1, 19 completed a Module 2 and 4 were unable to complete the ADOS-2 during testing; however, these children already had a formal diagnosis (see Table 1 for additional demographic information).
Demographic characteristics of participants.
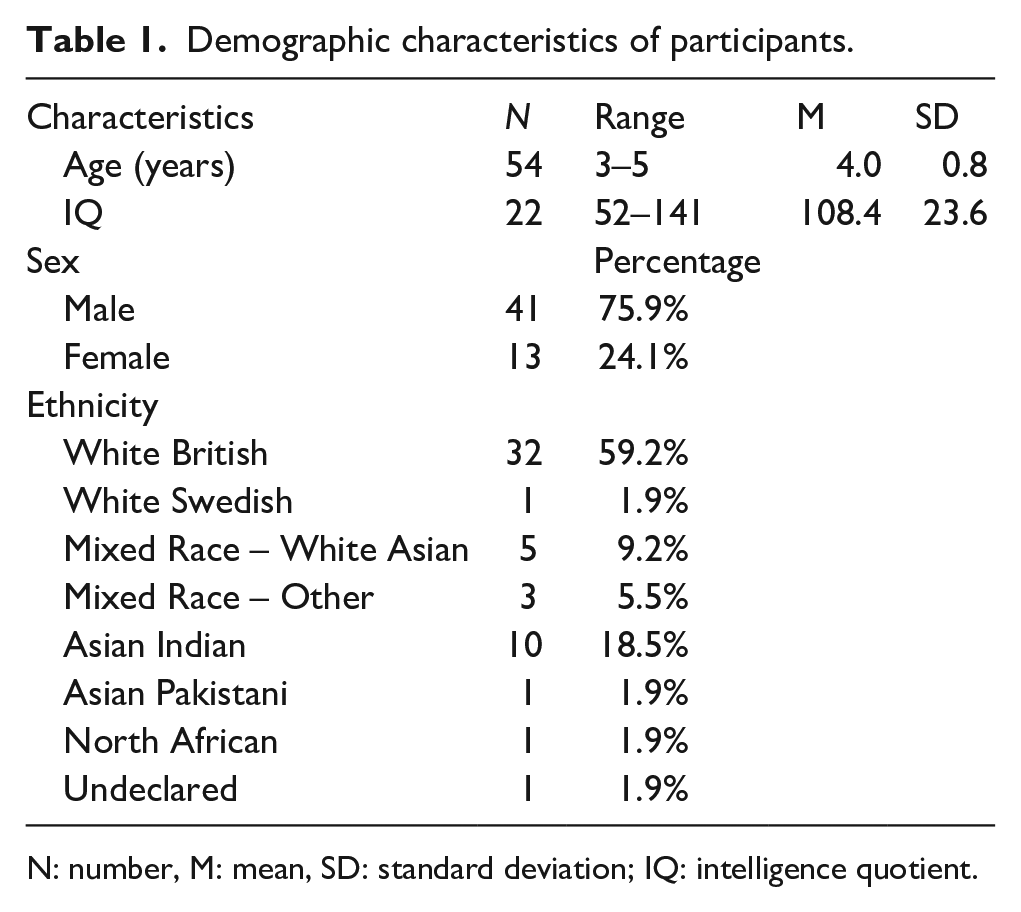
N: number, M: mean, SD: standard deviation; IQ: intelligence quotient.
To indicate the cognitive level of the sample, we conducted the Matrix reasoning subtests of the Wechsler Non-Verbal (WNV; Wechsler & Naglieri, 2006) and the British Ability Scale (BAS; Elliott et al., 1983). However, 31 participants were unable to complete the intelligence quotient (IQ) tasks either due to cognitive delay or behavioural difficulties (e.g. demand avoidance). Of these participants, 25 completed an ADOS-2 Module 1, 2 completed a Module 2 and 4 were also unable to complete the ADOS-2 assessment. IQ and verbal language level was taken into consideration in the analyses. Signed consent was obtained from parents, and verbal assent was obtained from children who were able to, otherwise, voluntary task compliance was considered assent. Families were provided with a social story for the children prior to testing to outline what their participation would entail. We recruited participants through the University of Reading Centre for Autism participant database, social media platforms, local NHS CAMHS services and through Autism Berkshire, a local autism organisation. Ethical approval was granted prior to the commencement of this study by the University of Reading Ethics Committee and the Berkshire Healthcare NHS Foundation Trust Health Research Authority.
Measures
Sensory Processing Scale Inventory
The Sensory Processing Scale Inventory (SPSI; Schoen et al., 2017) was used to measure sensory reactivity differences. It is a standardised, 96-item parent-report questionnaire that assesses the degree of sensory reactivity differences in children. It produces subscales for sensory hyperreactivity (47 items, e.g. ‘These garments bother my child: Seams in clothing’), sensory hyporeactivity (21 items, e.g. ‘My child has a less intense response than others to: Getting hurt, bruises or cuts’) and sensory seeking (28 items, e.g. ‘My child has difficulty disengaging from: Looking at spinning objects’). Items are scored dichotomously (1 = yes, 0 = no), with higher scores indicating a greater extent of sensory reactivity differences. The SPSI has strong internal reliability (hyperreactivity = 0.89; hyporeactivity = 0.88; sensory seeking = 0.93) (Schoen et al., 2017). As in our previous work (MacLennan et al., 2020), we chose to use the SPSI over other commonly used measures such as the Sensory Profile (SP; Dunn, 1999) as the SPSI has a comparatively greater representation of hyporeactivity and seeking compared to the SP, which more heavily represents hyperreactivity (Neil et al., 2017; Uljarević et al., 2016).
Sensory Assessment for Neurodevelopmental Differences
The Sensory Assessment for Neurodevelopmental Differences (SAND; Siper et al., 2017) was also used to measure sensory reactivity differences. It is a standardised observational assessment and associated caregiver interview, which assesses sensory reactivity differences in line with the ASC diagnostic criteria (DSM-5; American Psychiatric Association, 2013). In the direct observation, children are presented with a range of sensory toys with tactile (e.g. textured toy), auditory (e.g. musical toy) and visual (e.g. flashing toy) components. The assessment commences and concludes with 1–2 min of unstructured play to help the child familiarise with the situation, followed by presentation of the sensory toys. The children are scored for behavioural responses consistent with sensory hyperreactivity, hyporeactivity and seeking. The administration is conducted by a trained examiner, and behaviours are scored dichotomously (i.e. 1 = present, 0 = not present) across 36 items, and if a behaviour is present, there is the additional coding of a severity score (1 = mild, 2 = moderate to severe).
The subsequent interview component requires the caregiver to indicate whether their child presents with the various sensory reactivity differences in visual, tactile and auditory domains (1 = present, 0 = not present), and to rate the severity if present (1 = mild, 2 = moderate to severe). The items of this interview map onto the scoring for the observation. Observed and reported scores can then combined to produce a total score (0–90) and subscales for sensory hyperreactivity, hyporeactivity and seeking (0–30), with higher scores reflecting greater sensory reactivity differences. The SAND has been found to have strong internal consistency (0.90), test–retest reliability (0.97, p < 0.001) and moderate convergent validity (−0.63) (Siper et al., 2017).
Preschool Anxiety Scale
The Preschool Anxiety Scale (PAS; Edwards et al., 2010) was used to measure anxiety symptoms. It is a standardised 30-item parent-report questionnaire that assesses anxiety symptoms in children aged 3–6 years, adapted from the Spence Children’s Anxiety Scale (SCAS; Spence, 1998). Items are scored on the scale 0 (no true at all) to 4 (very often true), with higher scores indicating a greater extent of anxiety symptoms, and scores above cut-off indicate clinically elevated symptoms. The PAS produces a score for total anxiety (total score 120) and subscales for symptoms related to GAD (five items, total score of 20, e.g. ‘Has difficulty stopping him/herself from worrying’), social anxiety (six items, total score of 24, e.g. ‘Worries that he or she will do something embarrassing in front of other people’), separation anxiety (five items, total score of 20, e.g. ‘Is reluctant to go to sleep without you or to sleep away from home’), physical injury fears (seven items, total score of 28, e.g. ‘Is afraid of crowded or closed-in places’) and OCD (five items, total score of 20, e.g. ‘Washes his or her hands over and over many times each day’). The PAS has moderate internal consistency (α = 0.70) (Edwards et al., 2010). The PAS was selected over other measures of anxiety as it has subscales for early symptomology relating to anxiety subtypes.
Responses to Uncertainty and Low Environmental Structure questionnaire
The Responses to Uncertainty and Low Environmental Structure (RULES; Sanchez et al., 2017) was used to measure IU. It is a parent-report questionnaire and is validated to assess IU in children aged 3–10 years. It contains 17 items (e.g. ‘My child has a hard time coping with even minor changes’), rated on a scale of 1 (not at all) to 5 (very much). Scores can range from 17 to 85 with higher scores reflecting greater IU. The RULES has strong internal consistency (α = 0.93) and convergent validity in (0.67) (Sanchez et al., 2017).
Analysis
The data were analysed using SPSS 27 (IBM Corp, 2020) and JASP (JASP Team, 2020). Following normality checks, we conducted a Spearman’s bivariate correlation analysis to elucidate the correlational relationship between sensory reactivity differences, anxiety, IU and potential covariates. We then conducted partial correlation analyses and subgroup comparisons to ensure the relationships were independent of the effects of covariates. Significance was indicated by a Bonferroni’s corrected p-value of p ⩽ 0.01.
We then conducted a series of simple mediation analyses to understand the mediating relationship between sensory reactivity, anxiety and IU. We defined the analysis to conduct bootstrapping with 1000 resamples to adjust for measurement error and generated accelerated 95% confidence intervals (CIs). Full mediation is present if the indirect effect between the predictor and outcome variable is significant, and the direct effect is not significant. Partial mediation is present if both the direct and indirect effects between the predictor and outcome variable are significant. Significance is indicated by CIs not overlapping with zero and Bonferroni’s corrected p-value of p ⩽ 0.008.
Community involvement
The research questions for this project aligned with Autistica’s research priorities, which were identified by stakeholders. Throughout our project, we sought feedback from the families who took part in this study on our testing sessions and procedures, interpretations of our results and the language used in the article.
Results
Descriptive analyses
Descriptive analysis showed that the data were not normally distributed as a Shapiro–Wilk test of normality was significant for total anxiety and the anxiety subtypes (p < 0.05). However, no outliers were present in the data (see Table 2 for descriptive statistics). To avoid inflated correlations due to bias and multiple comparisons, parent-reported and observed sensory reactivity measures were combined (Kim & Lord, 2012; Spain et al., 2018). SPSI and SAND construct scores were significantly correlated for sensory hyperreactivity (r(52) = 0.60, p < 0.001), hyporeactivity (r(52) = 0.38, p = 0.005) and seeking (r(52) = 0.50, p < 0.001), suggesting both sensory measures are assessing related constructs. Therefore, SPSI and SAND z-scores were averaged to create standardised sensory composite scores for sensory hyperreactivity, hyporeactivity and seeking (Song et al., 2013).
Descriptive statistics for sensory reactivity differences (SPSI and SAND raw scores; z-score composites), anxiety (PAS raw scores), intolerance of uncertainty (RULES raw score) and autism traits (AQ and ADOS raw comparison scores).
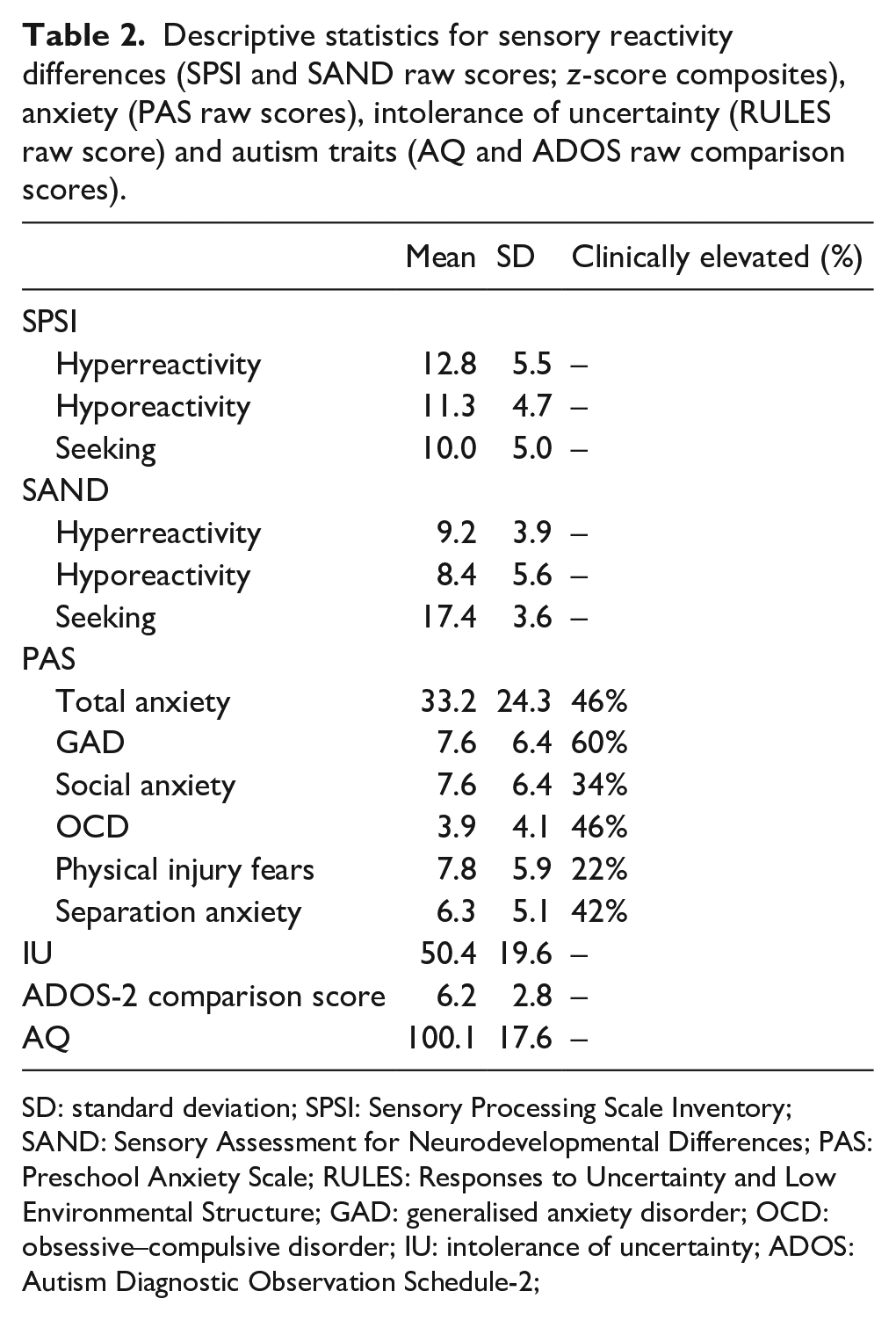
SD: standard deviation; SPSI: Sensory Processing Scale Inventory; SAND: Sensory Assessment for Neurodevelopmental Differences; PAS: Preschool Anxiety Scale; RULES: Responses to Uncertainty and Low Environmental Structure; GAD: generalised anxiety disorder; OCD: obsessive–compulsive disorder; IU: intolerance of uncertainty; ADOS: Autism Diagnostic Observation Schedule-2;
Correlational analyses
Spearman’s correlation analysis showed that sensory hyperreactivity was significantly positively correlated with total anxiety, GAD, social anxiety, OCD, physical injury fears, separation anxiety and IU. IU was also significantly positively correlated with total anxiety, GAD, social anxiety, OCD, physical injury fears and separation anxiety (see Table 3 for correlations).
Spearman’s correlations between sensory reactivity differences (SPSI and SAND composite z-scores), anxiety (PAS), intolerance of uncertainty (RULES), autism traits (AQ) and age.
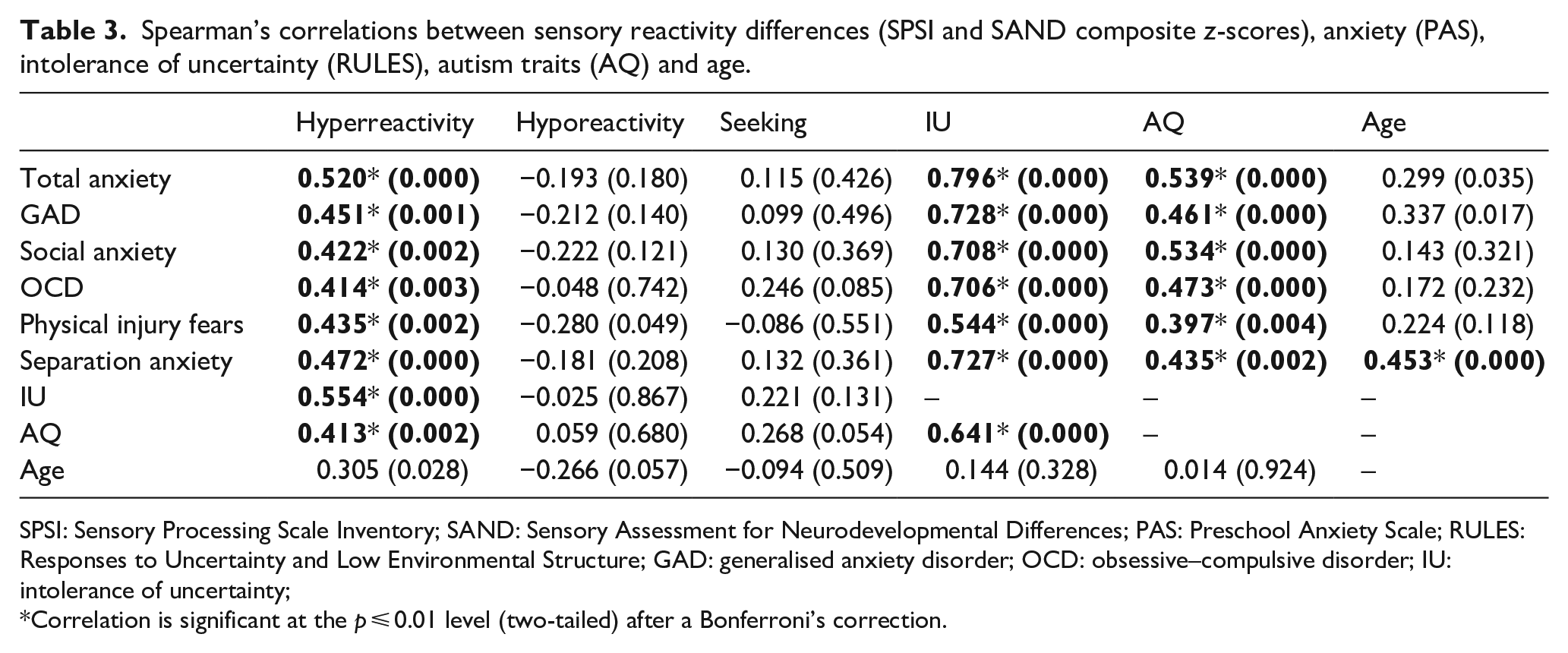
SPSI: Sensory Processing Scale Inventory; SAND: Sensory Assessment for Neurodevelopmental Differences; PAS: Preschool Anxiety Scale; RULES: Responses to Uncertainty and Low Environmental Structure; GAD: generalised anxiety disorder; OCD: obsessive–compulsive disorder; IU: intolerance of uncertainty;
Correlation is significant at the p ⩽ 0.01 level (two-tailed) after a Bonferroni’s correction.
Spearman’s correlation analysis also showed that age was significantly positively correlated with separation anxiety. In addition, autism traits were significantly positively correlated with sensory hyperreactivity, total anxiety, GAD, social anxiety, OCD, physical injury fears, separation anxiety and IU. Post hoc partial correlation analyses controlling for age found that the correlations between sensory reactivity, anxiety subtypes and IU sustained their significance (p ⩽ 0.01) or non-significance (p > 0.01), suggesting the relationships are independent from the effects of age. However, when controlling for autism traits, the relationships between sensory hyperreactivity and GAD, social anxiety, OCD and physical injury fears were no longer significant (p > 0.01). Fisher’s z-test was conducted to test if the significant correlation coefficient between sensory hyperreactivity and separation anxiety was significantly different from the non-significant correlation coefficients between sensory hyperreactivity and the other anxiety subtypes. This showed that the significant relationship with separation anxiety was significantly stronger than GAD, OCD and physical injury fears (p < 0.05), but was not significantly stronger than social anxiety.
In addition, we explored the effects of IQ and verbal language ability. As we only had IQ scores for 41% of the sample, we conducted a Spearman’s correlation analyses independently for the group with IQ scores and the group without to see if correlations between sensory reactivity and anxiety differed between groups. The analysis showed that sensory hyperreactivity was significantly related to anxiety in those who were unable to do an IQ test (without IQ score) (r(30) = 0.56, p = 0.001), but not in those who were able to conduct an IQ test (with IQ score) (r(20) = 0.38, p = 0.09). However, Fisher’s z-test confirmed that these correlation coefficients were not significantly different (p > 0.05). As for verbal language, correlation analysis showed that sensory hyperreactivity was significantly related to anxiety in those who had few-to-no words and completed the ADOS-2 Module 1 (r(28) = 0.62, p < 0.001), but not in those who were able to use sentences and completed the ADOS-2 Module 2 (r(18) = 0.29, p > 0.05). However, Fisher’s z-test confirmed that these correlation coefficients were not significantly different (p > 0.05). Furthermore, independent samples t-test indicated that there were no significant group differences in sensory hyperreactivity or anxiety scores for those with or without an IQ score, or those who did the ADOS-2 Module 1 or Module 2 (p > 0.05). Therefore, we did not take IQ or verbal language ability into account in further analyses as the non-significant subgroup findings are likely due to lack of power.
Mediation analyses
As sensory hyperreactivity, IU and total anxiety were intercorrelated, we conducted a series of simple mediation analyses to understand the predictive relationship between these constructs. To achieve this, we tested all possible iterations of the model, including sensory hyperreactivity, IU and total anxiety as predictor, outcome and mediating variables (see Table 4 for mediation analyses). As correlational analyses indicated that these relationships were independent from the effects of age, autism traits, IQ and verbal language level, we did not control for these in the analyses. We applied a Bonferroni’s significance correction to control for type 1 error due to multiple analyses (p ⩽ 0.008).
Mediation analyses between sensory hyperreactivity (SPSI and SAND composite z-score), anxiety (PAS) and intolerance of uncertainty (RULES).
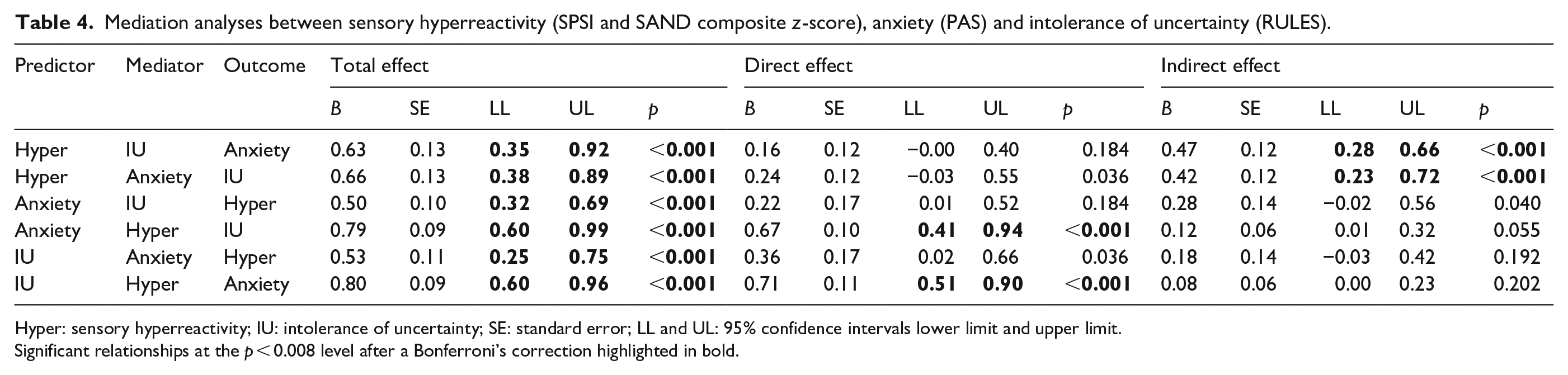
Hyper: sensory hyperreactivity; IU: intolerance of uncertainty; SE: standard error; LL and UL: 95% confidence intervals lower limit and upper limit.
Significant relationships at the p < 0.008 level after a Bonferroni’s correction highlighted in bold.
Mediation analysis indicated significant indirect effects between sensory hyperreactivity and anxiety through IU (B = 0.47, lower limit (LL) = 0.28, upper limit (UL) = 0.66, p < 0.001). A significant indirect effect was also found between sensory hyperreactivity and IU through anxiety (B = 0.42, LL = 0.23, UL = 0.72, p < 0.001). As the direct effects were not significant for both of these models (Bonferroni’s corrected p > 0.008 and 95% CIs containing 0), this indicates full mediation (Figure 1). No mediation was indicated when IU was entered as the predictor for sensory hyperreactivity through anxiety, and for anxiety through sensory hyperreactivity, or when anxiety was entered as the predictor for IU through sensory hyperreactivity, or for sensory hyperreactivity through IU, as the indirect effects were not significant (Bonferroni’s corrected p > 0.008 and 95% CIs containing 0).
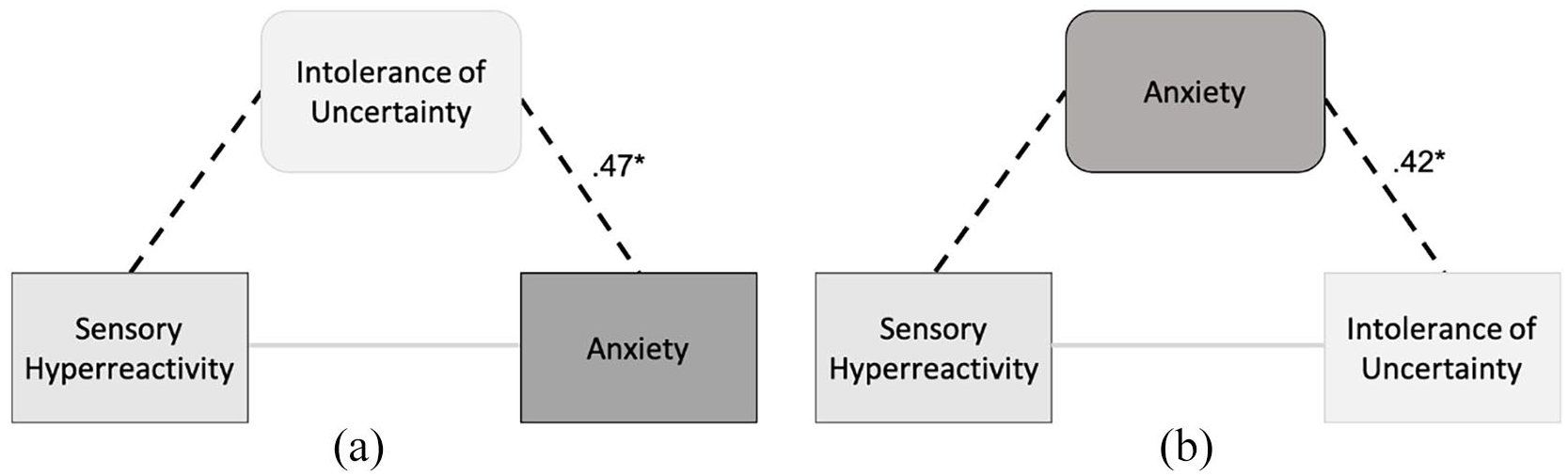
(a) Depicting the relationship between sensory hyperreactivity and anxiety fully mediated by IU and (b) the relationship between sensory hyperreactivity and IU fully mediated by anxiety.
Discussion
This study has been the first to explore the relationship between sensory reactivity differences, IU and anxiety in a heterogenous group of preschool-age autistic children. In line with our expectations, we found sensory hyperreactivity, IU and anxiety to be interrelated. In addition, we found that IU fully mediates the relationship between sensory hyperreactivity and anxiety, but that anxiety also fully mediates the relationship between sensory hyperreactivity and IU. We did not find sensory hyporeactivity or seeking to be significantly related to anxiety or IU.
We found, in line with previous findings (Hwang et al., 2019; Neil et al., 2016; Wigham et al., 2015), sensory hyperreactivity to be significantly related to total anxiety in autistic children. In our initial correlation analysis, we did not find sensory hyperreactivity to be differentially related to anxiety subtypes. However, when controlling for autism traits, we found sensory hyperreactivity to be significantly related to separation anxiety. As suggested in our previous work, controlling for AQ may limit measurement or response bias, or variability from trait–symptom overlap (MacLennan et al., 2020). Although existing findings have also shown links between sensory hyperreactivity and separation anxiety (Black et al., 2017), our previous work with older children found sensory hyperreactivity to be related to symptoms associated with physical injury fears and specific phobia (MacLennan et al., 2020). Inconsistencies across studies could be due to the use of different measures or the differing age and developmental level of the participants, as research has found differential prevalence of anxiety conditions across ages of autistic children and adolescents (van Steensel et al., 2011). This may be due to differential conditioning implicated in the development of certain anxiety conditions, such as context conditioning in GAD (Green & Ben-Sasson, 2010). It would be beneficial for future research to explore differential relationship over time and to further understand the association of IU when relationships are differential.
As previous literature has proposed disputing theoretical models that have included sensory hyperreactivity, IU and anxiety, here we tested a series of mediation models. We found that IU fully mediates the relationships between sensory hyperreactivity and anxiety in preschool-age autistic children, and that anxiety fully mediates the relationship between sensory hyperreactivity and IU. Critically, in line with our predictions, we found that sensory hyperreactivity was the predictor in both significant mediation models. This reflects previous longitudinal research in younger children that found sensory hyperreactivity to unidirectionally predict anxiety symptoms, suggesting that sensory hyperreactivity emerges earlier than anxiety (Green et al., 2012). However, our results also suggest that IU is an important early factor in the development and maintenance of anxiety in autism. Aversive sensory experiences can be unpredictable and not always specific to an object or situation, which is associated with greater avoidance and anxious behavioural responses, and associated amygdala activation (Green et al., 2015; Herry et al., 2007). Altered sensory interpretation in autism can enhance the perceived unpredictability of sensory input (Fiser et al., 2010; Pellicano & Burr, 2012). As IU is associated with alerting in attentional networks, individuals with higher IU may be more hypervigilant and biased to process uncertain information as threatening (Dugas et al., 2005; Fergus & Carleton, 2016). Thus, IU and anxiety may reciprocally be maintained in response to sensory hyperreactivity. Due to the constraints of cross-sectional mediation models, next steps in research would be to longitudinally test these mediating relationships.
As our results support that sensory hyperreactivity is a predictive factor for anxiety early in development, this could be an important target for early interventions. Sensory integration-based approaches are widely used and are deemed to be effective in targeting early sensory reactivity difficulties (Schaaf et al., 2017; Schoen et al., 2019), but little is known about how these impact anxiety development. Alternatively, Cognitive Behavioural Therapy (CBT) could be adapted to target sensory hyperreactivity (Edgington et al., 2016), as CBT has shown efficacy in young autistic children (Driscoll et al., 2020). However, IU may also be an important transdiagnostic mechanism to target in intervention (Hallett et al., 2021; Rodgers et al., 2017). There is evidence that targeting IU in clinical interventions effectively reduces anxiety in non-autistic cohorts (Boswell et al., 2013; Buhr & Dugas, 2006; Dugas et al., 2010; McEvoy & Mahoney, 2012). This has recently been extended into autism research, with the development of a manualised parent group-based intervention programme, such as Predictive Parenting (Hallett et al., 2021) and Coping with Uncertainty in Everyday Situations (CUES©; Rodgers et al.,2018, 2017). These interventions aim to enable children to become more tolerant of uncertainty and have shown promise in their efficacy.
In contrast to previous research (Glod et al., 2019; Hwang et al., 2019; MacLennan et al., 2020), we did not find sensory hyporeactivity to relate to anxiety or IU in this study. This may be due to the varying measures and age groups across studies. Alternatively, sensory hyporeactivity may be more related to depressive conditions, characterised by suppressed arousal, rather than anxiety (Lane, 2002; Neal et al., 2002; Pfeiffer et al., 2005). Or it may be more related to other autistic traits, such as communication differences, emotional, cognitive and behavioural differences, or RRBs (Glod et al., 2015; South & Rodgers, 2017; Wigham et al., 2015). As for sensory seeking, we did not find it to be significantly related to anxiety in autistic children, which reflects previous findings (MacLennan et al., 2020). Sensory seeking may be indirectly linked to anxiety or interlinked with sensory hyperreactivity and hyporeactivity, such as being a stimulatory strategy in response to sensory hyporeactivity (Lidstone et al., 2014; Liss et al., 2006). Future directions should aim to further understand how sensory hyporeactivity and seeking are related to anxiety.
There is a pressing need for research to include participants with few-to-no words or ID (Russell et al., 2019), thus, our heterogenous sample is a key strength of the study. However, our relatively small sample size may have impacted the power of our subgroup analysis, as well as relationships with anxiety subtypes. In addition, there are a few suitable objective assessments for IU and anxiety, especially for this demographic, and therefore, we had to rely on parent-reports. Although total anxiety scores have been found to be reliable in autistic populations, subscales for anxiety on parent-reports may need to be interpreted with caution in autistic children, especially those with co-occurring ID and who speak few-to-no words (Kerns et al., 2020; Toscano et al., 2020). Understanding the risk factors for traditional anxiety symptomology has clinical significance for existing anxiety interventions; however, it is also important that distinct anxiety symptoms in autistic children are recognised (Kerns et al., 2020). Therefore, there is a need for the development of autism-specific, measures that can be used to screen for early anxiety symptomology in young autistic children. But also, further research examining anxiety in autistic subgroups, such as those with few-to-no words or ID, is needed.
In conclusion, this study is the first to explore the relationship between sensory reactivity differences, anxiety subtypes and IU in preschool-age autistic children. Our findings indicate that sensory hyperreactivity, IU and anxiety are interrelated in preschool-age autistic children, and that sensory hyperreactivity may be specifically related to separation anxiety when taking broader autism traits into account. In addition, they suggest sensory hyperreactivity is an early predictor of anxiety and IU, which may both be reciprocally mediating factors in the maintenance of anxiety and IU in autism. The results of this study have important clinical implications for early anxiety interventions in preschool-age autistic children. However, there is still an imperative need to develop objective assessments, especially for IU and anxiety, for preschool-age autistic children, and those who speak few-to-no words. This is fundamental for research and clinical services that aim to support autistic individuals.
Footnotes
Acknowledgements
The authors specially thank all the families who participated. The authors also thank Francesca Englezou, Charlotte Daniels and Khadija Kapadia of the University of Reading for assisting with data collection, and the Centre for Autism at the University of Reading, Autism Berkshire and NHS Berkshire Healthcare CAMHS for helping with recruitment.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The authors are funded by MQ and Autistica.