
Abstract
Little is known about the nature of social anxiety in autistic people: What is similar and different about factors contributing to social anxiety in autistic and non-autistic people? There is also very limited research about autistic people’s experiences of therapy for social anxiety in current routine clinical practice. This study investigated these issues by analysing responses to an online questionnaire for 308 adults with elevated social anxiety (232 autistic people and 76 non-autistic people) using mixed-methods approaches. Distinct factors influenced social anxiety in autistic participants, including individual and environmental factors relating to autistic experiences in the social world. We propose a ‘distinct’ model of social anxiety in autism. In addition, many participants had not had helpful experiences in therapy, especially cognitive behaviour therapy, for social anxiety: They thought therapists did not always acknowledge the basis of their social fears, did not adapt the therapy process in an individualised way and did not understand neurodiversity or recognise neurodivergence. Our results suggest that social anxiety needs to be understood specifically in the context of autism, and if this is neglected, therapy is unlikely to be helpful. Based on participants’ comments, this article makes some practical recommendations for therapists supporting autistic adults with social anxiety.
Lay Abstract
The nature of social anxiety has been widely researched in non-autistic people. This existing research has allowed therapists to develop effective therapy for social anxiety in non-autistic people. Meanwhile, some research suggests that autistic people may have different experiences of anxiety compared to non-autistic people. In addition, there is some evidence that modified therapy may help autistic people with social anxiety, although we also know that many autistic people feel failed by existing mental health services.
This article provides a detailed picture of social anxiety in autistic people. This includes similarities and differences compared to non-autistic people. In terms of similarities, people often described feeling afraid that others would judge them, and this would have negative consequences. In terms of differences, autistic people commonly reported a clash between their traits and their social environment, which caused them distress and discomfort. This included factors only rarely reported by non-autistic people (such as struggling with too much sensory stimulation or inaccessible forms of communication and encountering discrimination for these problems). Based on this, we propose a ‘distinct’ model of social anxiety with particular relevance to autistic people. In addition, many participants reported negative experiences in therapy for social anxiety. They thought therapists wrongly viewed their fears of social situations as irrational and ungrounded. They thought therapists did not adapt the therapy process in an individualised way and did not understand neurodiversity or recognise neurodivergence.
Standard approaches for social anxiety may not always suit autistic people, so this needs further exploration. We highlight several practical recommendations for therapists offering therapy for social anxiety to autistic people.
Introduction
Social anxiety disorder is defined by a marked fear of being negatively viewed by other people in social situations (American Psychiatric Association [APA], 2013). Autistic people are particularly likely to develop fears of social situations: While prevalence of social anxiety is estimated to be approximately 12% in the general population (Ruscio et al., 2008), estimates in autistic people are as high as one in two experiencing clinically elevated social anxiety (Spain et al., 2018). However, we know relatively little about the nature of social anxiety in autistic people and how best to support those who seek support.
It has been suggested that anxiety may manifest in similar and different ways for autistic people compared to their neurotypical peers (Kerns & Kendall, 2012). Empirical research has supported the notion that autistic people may present with anxiety according to conventional definitions (e.g. categories of the Diagnostic and Statistical Manual of Mental Disorders (DSM) and International Classification of Diseases (ICD) diagnostic manuals) as well as more autism-specific presentations (Kerns et al., 2014). An autism-specific presentation of social anxiety has been proposed to involve distress in social situations without the fears of negative evaluation that are key to DSM and ICD diagnostic criteria for social anxiety disorder (Halim et al., 2018; Hunsche et al., 2022; Kerns et al., 2014). As this distress would not be strictly diagnosable as social anxiety disorder, it has been termed ‘atypical’ or ‘distinct’ social anxiety, as well as ‘social fearfulness’ (Kerns et al., 2014). Rather than caused by fears of negative evaluation, this distress may represent downstream consequences of autistic features (such as sensory sensitivity or uncertainty about the social situation) that cause anxiety in social situations (South & Rodgers, 2017). Studies to date have focused on autistic children, so we do not know whether this category of ‘social fearfulness’ necessarily applies to adults.
There are two additional points worth raising about possible differences in the nature of social anxiety in autistic compared to non-autistic people. First, difficulties applying social skills may be an important part of the development and experience of social anxiety for autistic people (Spain et al., 2018). By contrast, underdeveloped social skills are not conceptualised as central to social anxiety in neurotypical people (Clark & Wells, 1995). Instead, where social performance is affected in neurotypical people, this is thought to be due to negative expectations and avoidance behaviours – although there is some uncertainty about this account (Hopko et al., 2001). Second, autistic people may be more likely to experience negative interactions with others. This includes attracting negative reactions from others (Lim et al., 2022; Morrison et al., 2019; Sasson et al., 2017), as well as overt trauma and victimisation (e.g. Park et al., 2020; Trundle et al., 2022). As such, autistic people may often have reasonable grounds for fearing social situations. Indeed, the stigma and discrimination of being different to the neuro-majority has been shown to contribute to mental health difficulties (Botha & Frost, 2020), indicating that additional systemic factors are likely to impact social anxiety specifically for autistic people.
In addition to understanding the nature of social anxiety in autistic people, it is also important to identify the best ways of supporting individuals with social anxiety. This is a priority as the mental health needs of autistic people are not well met by current services (Camm-Crosbie et al., 2019; Crane et al., 2019), and necessary adjustments (e.g. having a therapist knowledgeable about autism) are not routinely made in clinical practice (Brice et al., 2021; Nicolaidis et al., 2015). The ‘gold-standard’ therapy for social anxiety in the general population is individual cognitive behaviour therapy (CBT; National Institute for Health and Care Excellence [NICE], 2013). There is some evidence to suggest that CBT may be helpful for supporting autistic adults with general anxiety and depression, although meta-analyses suggest there is significant uncertainty due to limited studies, small sample sizes and methodological weaknesses (Linden et al., 2023; Menezes et al., 2022; Weston et al., 2016). Specifically regarding CBT for social anxiety, two trials have shown reduced social anxiety among autistic people following a modified group intervention (Bemmer et al., 2021; Spain, Blainey, & Vaillancourt, 2017); however, these studies lacked control groups, and the effect sizes were rather smaller than treatment effects for CBT in non-autistic people (see meta-analysis of Mayo-Wilson et al., 2014). There are several case studies of individual CBT in autistic adults, which had promising results (Spain, Sin, et al., 2017). To our knowledge, there are no randomised controlled trials of CBT for social anxiety in autistic adults.
The present study aims to address two gaps in the literature. First, there is currently no largescale study aiming to construct a model of potential differences in autistic experiences of social anxiety. In our previous research, we showed that the leading cognitive-behavioural model of social anxiety in neurotypical people – the Clark and Wells (1995) model – had some relevance for autistic people but did not fully account for social fears in autistic people (Wilson & Gullon-Scott, 2023). This is important because it is likely that individuals will have therapy influenced by this model (at least in the UK), as it is one of only two CBT protocols recommended by the National Institute of Health and Care Excellence as the first-line treatment for social anxiety in adults (NICE, 2013). However, as the model does not fully account for social fears in autistic people, therapists may not be targeting all the key factors affecting social anxiety in autistic people in current therapy approaches. Small qualitative studies have highlighted that core autism traits and contextual factors may make a unique contribution to social anxiety in autistic people (Black et al., 2023; Spain et al., 2020). The present largescale study aims to build on these previous studies by constructing a model of social anxiety and assessing the extent to which this is ‘distinct’ to autistic people. We aimed to build this model in a data-driven way based directly on the perspectives of autistic people. The second gap in the literature relates to a lack of data about how autistic people experience interventions currently available in routine clinical practice for social anxiety. As noted earlier, there is some preliminary evidence that modified group CBT may be helpful for social anxiety in autistic people (Bemmer et al., 2021; Spain, Blainey, & Vaillancourt, 2017). In the absence of more definitive evidence, it is helpful to hear the perspectives of autistic people on their experiences of CBT in routine clinical practice. This will help us understand more about the modifications autistic people may require in interventions for social anxiety.
This study uses a mixed-methods approach to survey data to explore the following questions:
What factors contribute to social anxiety in autistic people? How are these similar and different to factors relevant in the neurotypical population?
What are the experiences of autistic people in seeking support for social anxiety?
Method
This was a survey-based study that received approval from the Newcastle University Faculty of Medical Sciences Research Ethics Committee (Study No. 2231/13981). This study is part of a larger piece of work with further analysis reported in a companion article (Wilson & Gullon-Scott, 2023).
Participants
We recruited 336 adults aged 18 years or older through social media, charities such as Autistica (https://www.autistica.org.uk/) and snowball sampling. Adults were invited to complete a survey if they had Internet access, no major uncorrected sensory impairment and no significant history of neurological illness. For the analysis reported in this article, we required participants to have elevated social anxiety. We operationalised this as a score of 18 or over on the fear subscale of the Liebowitz Social Anxiety Scale – Self Report (LSAS-SR; Liebowitz, 1987). Only the LSAS-SR fear subscale was administered (and not the avoidance subscale) to reduce participant burden, as the individual subscales are very highly correlated (Liebowitz, 1987). However, predefined cutoffs only exist for the whole subscale, so we defined a priori a cutoff on the fear subscale to use for this study, which was a score of 18, representing 1.5 SDs above the mean (over 90th percentile) in non-anxious individuals in the study by Fresco et al. (2001). A total of 308 participants met this criterion: 232 autistic (183 reporting a clinical diagnosis and 49 self-identifying as autistic) and 76 non-autistic people. Individuals with a clinical diagnosis of autism were asked to give details about the place, date, process, outcome and professionals involved in the autism assessment. All individuals reported being diagnosed by a multidisciplinary team and/or relevant professionals including medical doctors or clinical psychologists. See Table 1 for demographic and clinical characteristics of the sample.
Numbers (percentages) and mean (SD) for demographic and clinical characteristics of the sample.
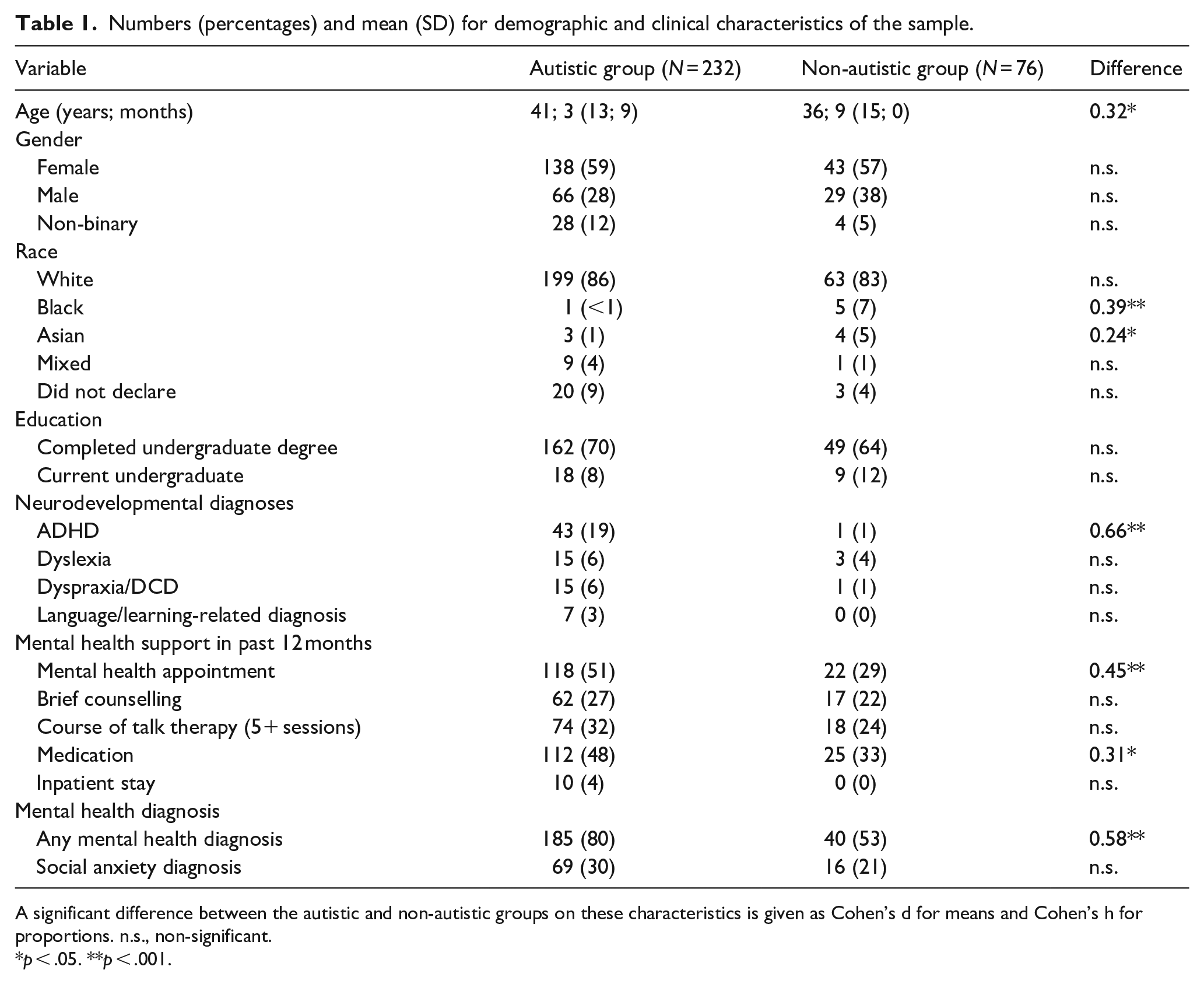
A significant difference between the autistic and non-autistic groups on these characteristics is given as Cohen’s d for means and Cohen’s h for proportions. n.s., non-significant.
p < .05. **p < .001.
Materials
Participants completed an online survey about ‘experiences of social anxiety’. They were first presented with information about the study and signed a consent form to give informed consent to participate. They then completed a bespoke questionnaire recording demographics and clinical diagnoses (including autism and mental health conditions), before completing several self-report measures relating to autism-related traits, social anxiety and broader mental health. These measures are not the focus of this analysis but are summarised in Supplemental Material 1 and described in detail in our companion article (Wilson & Gullon-Scott, 2023). Within the survey, there were some free-text response questions which are the focus of this article. These questions were developed by the authors to elicit (1) factors influencing social anxiety and (2) ‘hot cognitions’ about social situations (such as questions therapists use to gain an understanding of the cognitive aspects of a person’s social anxiety in CBT). Questions were also designed to elicit perspectives on therapy for social anxiety that participants had experienced, in particular, what they found helpful and unhelpful. We also asked for some factual information about what happened in the therapy, so we could establish what the intervention was likely to have been. These questions were reviewed by four autistic people for sense and readability and finalised based on their feedback.
In the survey, participants were given the following information prior to the free-response questions: ‘Please think about social situations that make you feel anxious or uncomfortable. We would like to know more about how these situations affect you. The questions below are designed to be prompts. Please feel free to answer them however you like’. They then answered these questions:
What makes you feel anxious or uncomfortable in social situations?
What is the worst thing about these situations?
Are you concerned particular things might happen?
Do particular thoughts go through your mind in these situations?
At the end of the survey, participants were asked about therapy experiences:
Have you ever had therapy for social anxiety? This might have been counselling, CBT or some other talk therapy. What was the therapy? What did it involve? Please give detail so we know what the therapy was like.
Was it helpful?
Was there anything unhelpful or that you did not like about it?
Have you had therapy for other mental health difficulties? How was this?
Data analysis
Social anxiety experiences
We carried out qualitative analysis of responses participants gave to the questions stated above about the nature of their social anxiety. We used thematic analysis according to the method of Braun and Clarke (2006) and were also influenced by framework analysis (Gale et al., 2013), as we aimed to build a framework within which multiple coders could classify participants’ responses. We included all participants in this analysis, whether they had a diagnosis of autism or not, and all coding happened blind to diagnostic status.
First, data were read closely to familiarise ourselves with participants’ responses. Then, data-driven, inductive coding was used to capture information about factors influencing social anxiety as widely as possible in participants’ own words over multiple rounds until the dataset was saturated with codes. Where codes were very similar, they were collapsed into one. We then grouped codes into superordinate categories where there was a thematic connection between codes. This stage involved a shift towards a more combined inductive-deductive approach, as some superordinate categories were based on a theoretical understanding of social anxiety and autism. For instance, inductive codes ‘seen as stupid’ and ‘seen as weird’ were grouped under the more theoretically driven superordinate category of ‘fears of negative evaluation’ (as a key diagnostic element of social anxiety).
Once we had identified superordinate categories, we began examining relationships between these by attempting to group and represent them diagrammatically. We added arrows between superordinate categories, where there appeared to be an association. This was an iterative process of reviewing the superordinate categories, the codes, the data and our emerging diagrams. During this process, we began using the concept of ‘typical’ and ‘distinct’ to group and structure superordinate categories. Specifically, if the superordinate category related to DSM-5 social anxiety, it was classified as ‘typical’, whereas if it was not, it was classified as ‘distinct’. This dichotomy of ‘typical’ versus ‘distinct’ draws on existing research (e.g. Kerns et al., 2014), although we did not attempt to map any specific model of a ‘distinct’ form of anxiety onto the data. While developing the ‘typical’ versus ‘distinct’ diagrams, we intended these to be separate models, but we noticed that the ‘distinct’ model incorporates the ‘typical’ model. Therefore, the relationship between the models evolved through this process as we finalised the framework for understanding the data.
In order to establish whether this was a replicable framework for understanding the data, two independent raters returned to the data and identified participants they felt showed ‘distinct’ social anxiety. We assessed level of agreement with Cohen’s kappa, before discussing any cases where there was disagreement and made a consensus decision. Finally, we carried out some quantitative analysis to examine whether there were systematic differences between individuals with ‘typical’ or ‘distinct’ social anxiety on demographic and clinical characteristics. Group differences on these characteristics were quantified using Cohen’s d (for continuous variables) and Cohen’s h (for frequencies).
Experiences of therapy for social anxiety
We also looked at autistic participants’ descriptions of their therapy experiences, with a particular focus on CBT for social anxiety, as the NICE-recommended therapy for this condition. Where autistic participants had accessed therapy for social anxiety, we classified each person as finding therapy helpful, partly helpful or minimally helpful. In response to being asked whether therapy was helpful (as described in the aforementioned list of questions), most participants gave a ‘yes’ or ‘no’ answer with further explanation, so classification of helpful versus unhelpful was often unambiguously based on the ‘yes’ or ‘no’, whereas a more mixed response was conservatively classified as ‘partly helpful’. We used a thematic analysis according to the method of Braun and Clarke (2006) to identify factors that were felt to make therapy helpful or unhelpful. A semantic approach to coding was used, focusing on the surface meaning of participants’ words and taking them at their word. As with the analyses described earlier, overly similar codes were collapsed, and related codes were grouped under superordinate categories.
Community involvement
A small group of autistic adults commented on the content and language of the survey during a piloting stage. We shared our qualitative analysis of social anxiety and therapy experiences with all participants and requested feedback prior to finalising this analysis. Twenty-two autistic participants wrote back, all with positive feedback highlighting that they felt the write-up reflected their experiences as an autistic person. None of the non-autistic participants chose to provide feedback.
Results
Experiences of social anxiety
Figures 1 and 2 represent the codes developed from the dataset. There were many codes relating to fears of (1) not performing well in a social situation, (2) being negatively evaluated by others (perhaps due to performing poorly) and (3) suffering negative social consequences of being negatively viewed. These codes are organised as a flow diagram in Figure 1. It should be noted that this represents social anxiety as conventionally understood (e.g. in DSM-5).
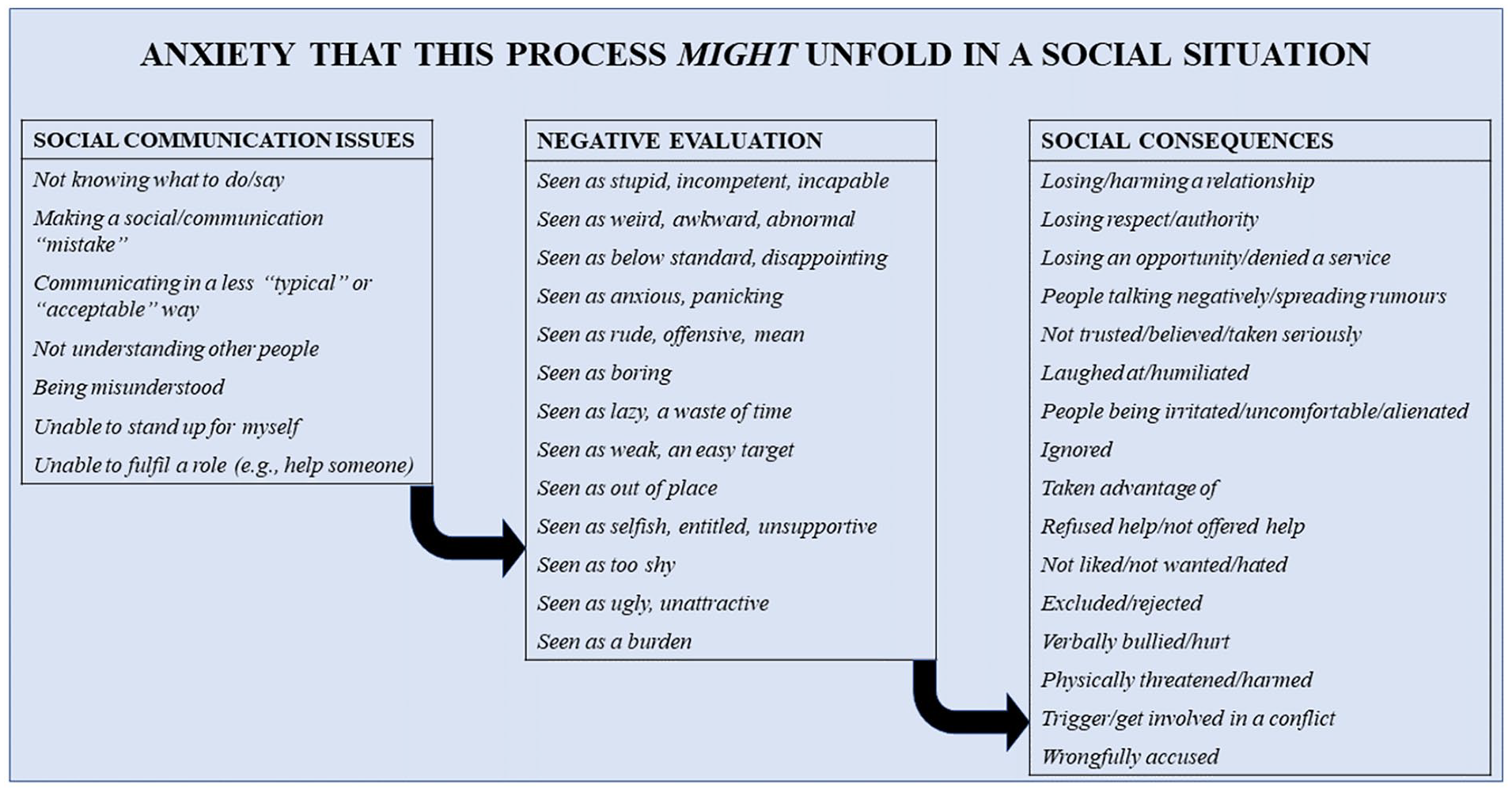
Schematic representation of social anxiety reported by individuals in the sample. Italic formatting represents a code derived from the free responses of participants. Codes have been structured into three superordinate categories, and these categories have been linked to indicate the process people may fear about social situations. This diagram is taken to represent ‘typical’ social anxiety (as recognised in DSM-5 and ICD-10).
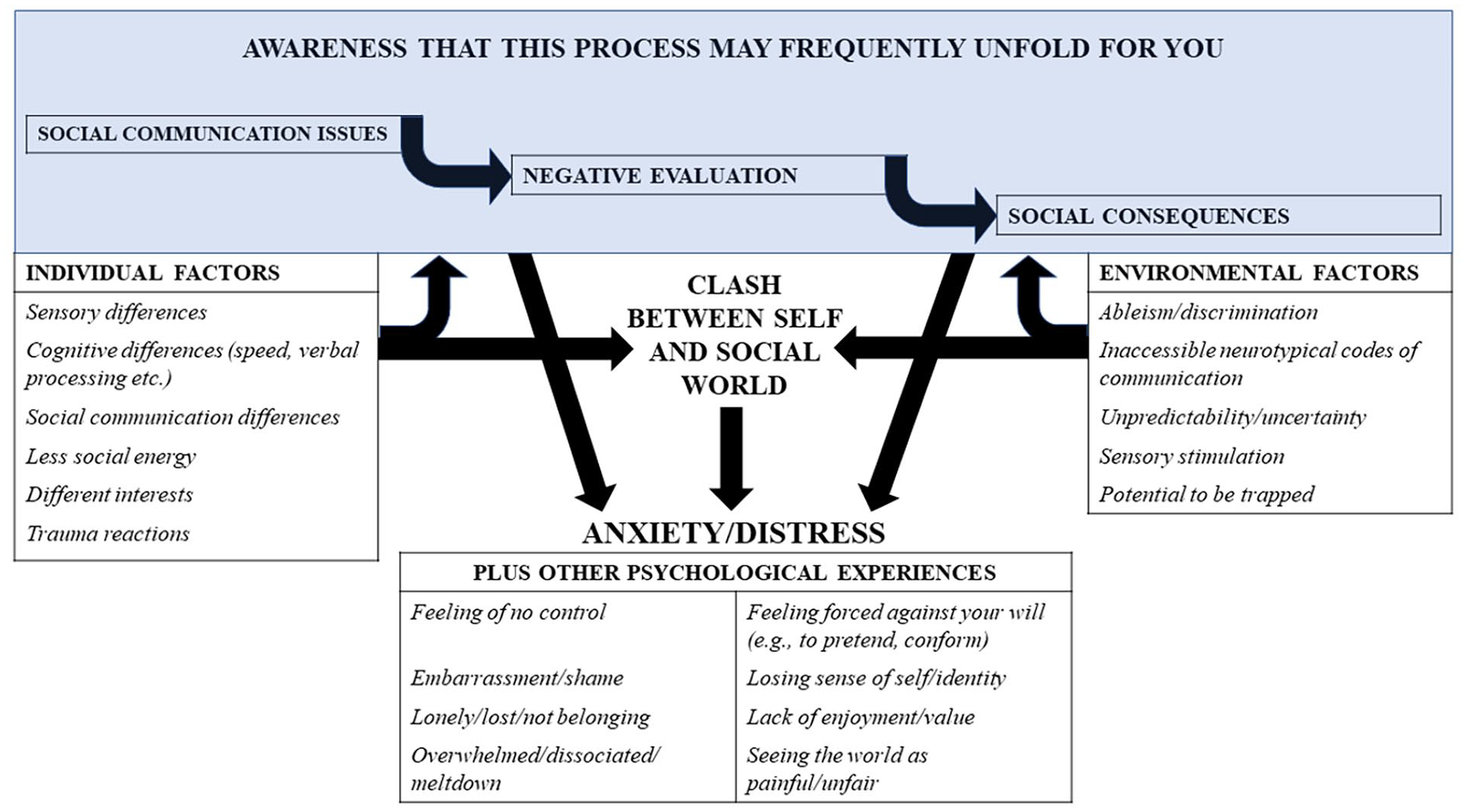
Schematic representation of a ‘distinct’ model of social distress. Italic formatting shows codes derived from free responses of participants. These codes have been grouped by superordinate categories and structured into a model of anxiety. The ‘typical’ model of social anxiety is embedded in this model at the top. In this conceptualisation, the clash between the self and an incompatible social world is key to social distress.
In addition to codes relating to ‘typical’ social anxiety shown in Figure 1, there were other codes relating to (1) stable individual factors and (2) features of the social environment, which together made socialising less accessible for some participants. These codes were more ‘distinct’ from ‘typical’ social anxiety. They are shown in Table 2 alongside illustrative quotations and also in Figure 2.
Codes relating to individual and environmental factors that participants felt made social situations less accessible for them and contributed to social distress.
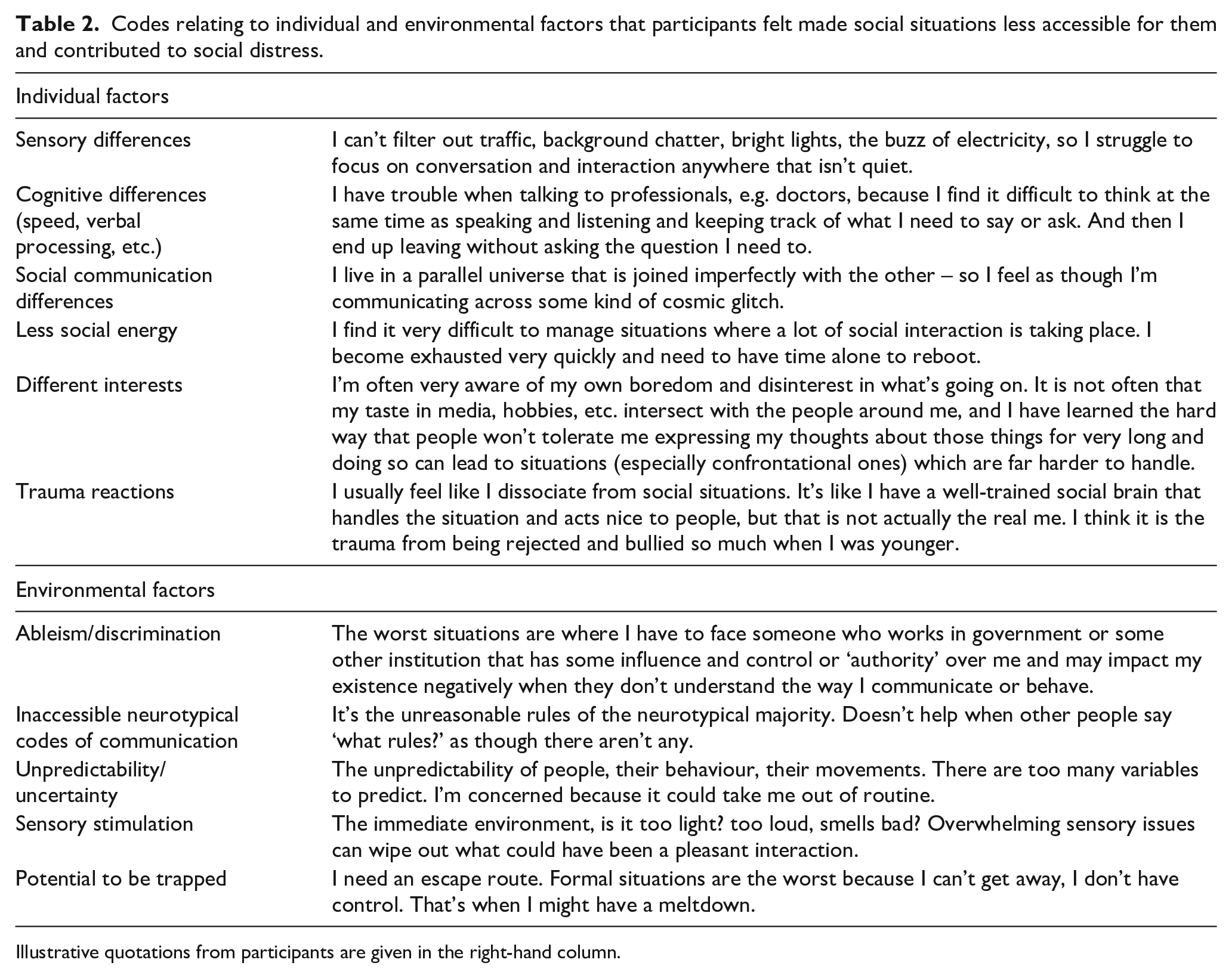
Illustrative quotations from participants are given in the right-hand column.
Participants often felt that these individual and environmental factors made negative evaluation by others (i.e. the process described in Figure 1) more likely. As one participant stated, ‘after fifty years of bullying and exclusion, I know that this fear is not irrational or unfounded’. In addition to anxiety, participants identified other psychological experiences resulting from the incompatibility between themselves and the social world, including loneliness, meltdown, a lack of enjoyment and feeling forced against your will. All the types of code described in this paragraph were organised in a second flow chart (Figure 2) as a ‘distinct’ representation of social distress present in some people.
In the next stage of analysis, two independent raters returned to the data to identify participants describing experiences consistent with the ‘distinct’ model of social distress shown in Figure 2. This was carried out to ensure this model could be reliably identified. Agreement between raters was substantial (kappa = 0.70; absolute agreement = 86%). Where there were disagreements, resolution was sought through discussion. This left 110 individuals consistent with the ‘distinct’ model. In terms of odds ratio, autistic people (whether clinically diagnosed or self-identifying) were 11 times more likely than non-autistic people to be rated as showing the ‘distinct’ model, χ(1) = 42.02, p < .001. Autistic people showing the ‘distinct’ model tended to be slightly older (Cohen’s d = 0.26) than autistic people showing a more ‘typical’ social anxiety and also reported greater social anxiety (d = 0.55), general anxiety (d = 0.31) and depression (d = 0.37; all ps < .05). Supplemental Material 2 shows full demographic and clinical characteristics of these two groups of autistic people, and Supplemental Material 3 provides additional quotations from autistic participants to demonstrate the types of responses coded as ‘distinct’ rather than ‘typical’ social anxiety.
Experiences of therapy for social anxiety
Seventy-four autistic participants had accessed CBT specifically for social anxiety (or with a significant focus on social anxiety). Fifty-nine autistic people also had had other therapies for social anxiety (sometimes in addition to CBT) or did not state the type. Other types of therapy included counselling, mindfulness, dialectical behaviour therapy, interpersonal psychotherapy, psychodynamic therapy, acceptance and commitment therapy and systemic psychotherapy. Table 3 shows numbers of autistic people who found CBT and other forms of therapy helpful, partly helpful or not helpful. Very few indeed found CBT helpful (just 11%), and most described it as unhelpful (65%). Some autistic people said that CBT was harmful: ‘CBT was extremely damaging and made me feel even worse after each session’ and ‘None of it was helpful. Most of it made me worse’. By contrast, participants were evenly split whether other forms of therapy they had experienced were helpful or not.
Numbers (percentages) of people finding CBT and other forms of therapy helpful, partly helpful and not helpful for social anxiety.

The end column indicates whether the pattern of responses was significant.
Autistic participants identified many reasons that made therapy less effective for them, which can be seen in Table 4.
Thematic analysis of reasons that therapy was unhelpful for autistic people with social anxiety.
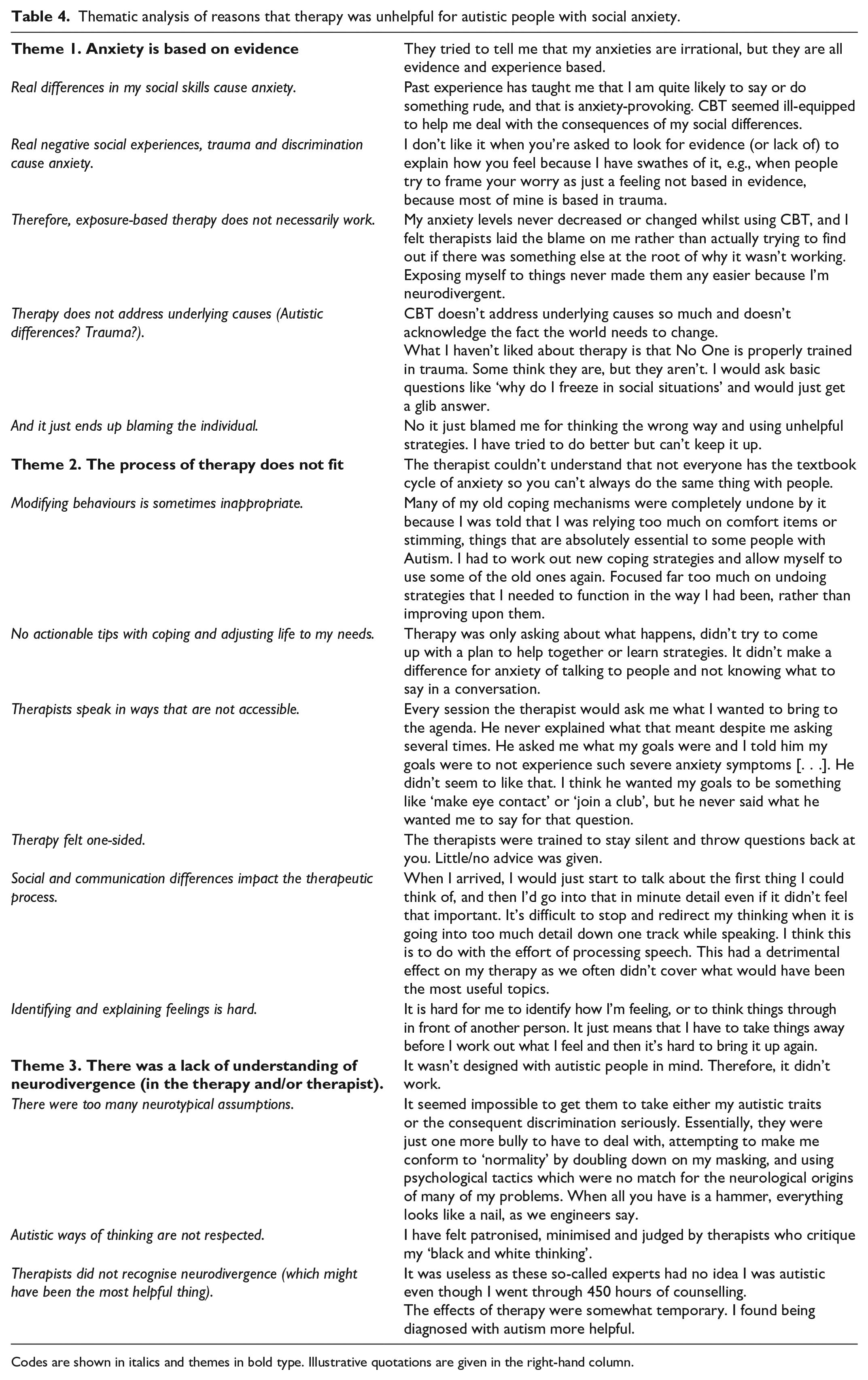
Codes are shown in italics and themes in bold type. Illustrative quotations are given in the right-hand column.
In addition, participants highlighted some helpful aspects of therapy. These are shown in Table 5.
Helpful therapy experiences of autistic people accessing support for social anxiety.
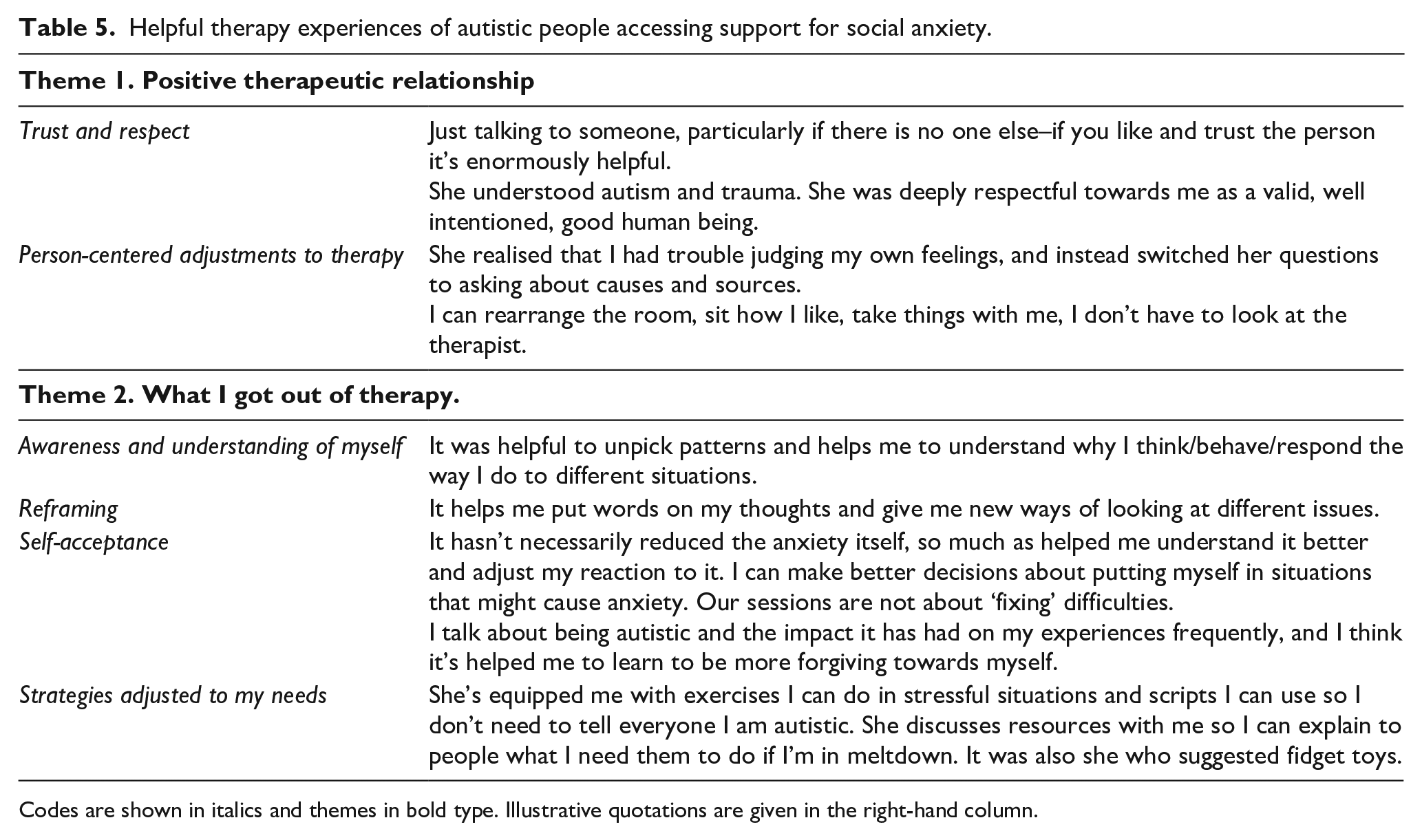
Codes are shown in italics and themes in bold type. Illustrative quotations are given in the right-hand column.
Discussion
This study found evidence for similarities and differences in autistic people’s experiences of social anxiety compared to how social anxiety is typically understood in the general population. In terms of similarities, autistic people often had fears of negative evaluation in social situations, with resulting fears over the consequences of being seen negatively by others. In terms of distinct factors, autistic people often described their social distress as affected by their autism traits and environmental factors relating to autistic experiences in the social world. We also found that many participants had not had helpful experiences in therapy for social anxiety: They thought therapists did not always acknowledge the basis of their social fears, did not adapt the therapy process in an individualised way and did not understand neurodivergence. Based on participants’ comments, we make some recommendations for supporting autistic adults with social distress.
Our research echoes previous research that autistic people may show both ‘typical’ and ‘distinct’ presentations of mental health difficulties (e.g. Kerns et al., 2014). In our sample, approximately half of autistic adults with elevated social anxiety showed a ‘distinct’ type of social distress, whereas the other half were identified as showing a more ‘typical’ presentation. In both cases, fears of negative evaluation were prominent in this study. This differs from conceptualisations of ‘distinct’ social anxiety in previous research (Hunsche et al., 2022; Kerns et al., 2014), which highlighted that some autistic participants experienced social distress without accompanying thoughts of negative evaluation by others. Importantly, these studies were based on autistic children, so there may be some developmental change as the individual grows up. Certainly, in this study, fears of negative evaluation were key in autistic adults – although participants appeared to claim these fears differed from ‘typical’ social anxiety in being well-founded. They said that fears of being viewed negatively were due to (1) objective differences in their social interaction and (2) the inaccessible/inhospitable environments in which they often find themselves and which may be associated with negative and traumatic experiences. Previous research does support this view of well-founded fears, as neurotypical people often do form negative perceptions of autistic people (Lim et al., 2022; Morrison et al., 2019; Sasson et al., 2017). This is a key point because clinicians’ diagnostic assumptions are typically that fears of negative evaluation are disproportionate to the sociocultural context (APA, 2013), which calls into question the extent to which ‘social anxiety disorder’ can be validly diagnosed in socially distressed autistic people. Moreover, CBT for social anxiety focuses on helping individuals re-evaluate these fears; however, if these fears are in fact well-grounded, a typical CBT approach may be less helpful and potentially invalidating. Indeed, participants often made this point, indicating that therapists did not seem to recognise that their social fears were often grounded in experience.
For autistic people showing the ‘distinct’ presentation of social distress, it was clear that fears of negative evaluation by other people were not the whole story. Participants perceived a clash between their own abilities and needs as an autistic person and the wider social environment, which made social situations difficult, overwhelming and stressful. This echoes previous qualitative studies, which also suggested that a person’s autism traits and social/non-social environmental factors contribute to their social distress (Black et al., 2023; Spain et al., 2020). In this study, individual autism factors included sensory and cognitive differences that make social interaction more challenging than rewarding and having low levels of energy for social interaction, whereas environmental factors included unpredictability, high sensory stimulation and discrimination/stigma towards neurodiversity. Therapy likely needs to take these factors into consideration so that we can support people with the actual source of their distress.
Many autistic participants in this study had accessed therapy – especially CBT – for social anxiety, but CBT for social anxiety was rarely found to be helpful. People felt that therapists did not always recognise the reality of their social struggles, did not adapt therapy in a person-centred way, and did not necessarily understand (or respect) neurodivergence. This complements existing research, which has found that existing CBT approaches may not always be the best fit for autistic people (Menezes et al., 2022). There is some emerging evidence that modified CBT for social anxiety may be helpful for autistic adults (e.g. Bemmer et al., 2021; Spain, Blainey, & Vaillancourt, 2017); however, it is notable that studies have not included control groups, and effect sizes are modest compared to those for CBT in the general population. Further research is required to understand the optimal treatment approach for autistic adults seeking support with social anxiety. There does seem to be awareness among therapists that CBT may need adaptation for autistic people (Spain & Happé, 2020), although therapists may be underskilled in delivering these adaptations (Corden et al., 2022). In addition, ‘adaptation’ may not go far enough, but a different approach may be required. Typically, in CBT for social anxiety, a key target for intervention is reducing an individual’s use of safety behaviours to test out their fears of social situations (Clark & Wells, 1995), but it was notable that people in this study sometimes felt that their resources were removed by CBT, so intervention may need to be approached differently if it inadvertently depletes an individual’s coping skills. Where therapy experiences were more helpful, this tended to rely on a good understanding of neurodiversity and neurodivergence, a strong therapeutic relationship and slightly different focuses in therapy, including (1) more emphasis on understanding/acceptance rather than change and (2) helping a person find workaround solutions to deal with stressful situations.
How should we approach therapy for social anxiety in autistic people? Suggestions for therapists
We offer a few reflections in the following sections based on our close engagement with participants’ comments and our own personal and professional experience as clinical psychologists working with autistic adults. These reflections have all been shared with autistic participants, who offered positive feedback about them. It should be noted that these suggestions have not been tested in therapy but represent suggestions for further exploration and largely align with other practice-based recommendations for modified CBT (e.g. Spain & Happé, 2020).
With this caveat, we highlight our recommendations. First, therapy needs to take into consideration the individual and environmental factors that contribute to social distress in autistic people (such as those identified in this study), alongside a broader understanding of neurodiversity, discrimination and trauma. This might involve education of therapists and collaborative case formulation and psychoeducation to co-create with clients an understanding of which factors make social situations distressing for them. This may also involve developing materials based on findings of the current study alongside findings from other research into the specific presentation of social anxiety in autistic adults (Black et al., 2023; Spain et al., 2020). Second, therapy needs to be truly validating and recognise the challenges and well-founded anxieties autistic people experience about social interaction. Social interaction is hard and can be unpleasant, and the therapist needs to try and understand this from the autistic perspective of the client. As reflexive practitioners, we need to be mindful of our own knowledge of neurodiversity and our own traits (whether neurotypical or neurodivergent) and develop curiosity about how our norms, assumptions and preferences sit alongside those of our clients. This might involve explicit training of therapists, as research indicates that mental health professionals are often lacking in confidence and expertise in working with autistic people (Corden et al., 2022). In addition, especially if the therapist and client have different neurotypes, it might be important to reflect on the ‘double empathy problem’ – i.e. the mutual difficulties autistic and non-autistic people may have in understanding each other’s perspectives (Milton, 2012). Third, we need to establish what a good outcome for therapy is likely to be for individuals who may always struggle with social situations; this might include some reduction in social distress, but it may also include acceptance/forgiveness towards oneself and finding practical solutions to particular stresses relevant to the individual. Fourth, if using CBT, therapists need to consider how appropriate it is to ask individuals to drop ‘safety behaviours’, which is central to the CBT protocol of Clark and Wells (1995). We might need to identify with the client how well certain behaviours are serving them (without making assumptions about this) and focus on adding to a person’s coping strategies rather than depleting them. What looks like a safety behaviour to a therapist may have a different function for the autistic person – it may be a stim, a way of coping with sensory overwhelm or a processing difference or a necessary form of camouflaging. With respect to camouflaging, we may need to establish with clients whether the benefits (in terms of access to social spaces and opportunities, through appearing more ‘neurotypical’) outweigh the costs (in terms of wellbeing; Bradley et al., 2021). Fifth, some autistic participants indicated they wanted therapists sometimes to be more explicit and take more of a lead. Examples included (1) giving the client more scaffolding when coming up with appropriate agenda items and goals for therapy and (2) giving more direct information around understanding emotions and coping strategies that have worked for others (i.e. using more psychoeducation). Sixth, we need to be mindful that all the issues affecting day-to-day social situations identified in this study may come into the therapy room – i.e. factors in Figure 2 may show up with the therapist, including communication differences and environmental (e.g. sensory) factors. For instance, an individual may struggle to process verbal content and formulate thoughts and verbal expression in the here-and-now in response to questions. It may be helpful, for instance, to use communication supports, such as written questions in advance, written summaries after and agreeing on strategies for checking the discussion is helpful to the client. This echoes other research that indicates autistic people benefit from adaptations to the delivery of therapy to increase accessibility, but that this is not always forthcoming in current clinical practice (Brice et al., 2021; Spain & Happé, 2020). Implementing such communication supports in therapy could be an opportunity for learning for both the client and therapist, but if communication needs are not attended to, it could be detrimental to the process. It will be important for the therapist to consider their own communication needs too and the potential impact of the ‘double empathy problem’ (Milton, 2012) if their neurotype differs from the client.
Limitations
There are several issues and limitations to bear in mind with this study. Although there was a large sample for a qualitative study, it was skewed towards educated white women, and it will be important to establish whether the findings are relevant to a range of autistic groups. In particular, we cannot be sure how well our results generalise to autistic people with a learning disability and autistic children. A second limitation of the study is that it was not always possible to get a fine-grained picture of each individual’s social anxiety or therapy experiences, due to the nature of completing a survey on one occasion – e.g. some participants gave very brief answers, ambiguities cannot be clarified in a survey and so on. This became an issue when we returned to the data to check which participants likely showed the ‘distinct’ model of social anxiety, as some participants did not give much information to make a reliable judgement. This was the key factor causing discrepancies during the assessment of inter-rater disagreement. There was also the related issue that we could not verify the information participants gave – for instance, a participant might briefly state they had had CBT. Often, participants gave sufficient detail for us to be confident that they were describing a typical CBT intervention, but on some occasions, there was not enough information to be sure they were describing a full evidence-based intervention, and it was not possible to cross-validate this. Our analysis therefore reflects experiences in routine clinical practice rather than therapy controlled to a research-level standard. Third, we could not systematically analyse whether the helpfulness of therapy depended on a participant already having been diagnosed with autism at the onset of therapy. There is reason to suspect that helpful therapy did depend on this based on the thematic analysis, but this could not be properly examined in detail. Fourth, our study did not survey clinicians, who might have given different perspectives on the issues discussed here. Fifth, this study only represents an initial exploration of an alternative model of social anxiety in autistic people. To validate the model, we would need to measure the variables identified in the model and assess how well they predict social fears in an independent sample. There may also be some missing factors from the model. For instance, one of our reviewers highlighted that the neurotype of the social contacts may be an additional factor relevant to the ‘distinct’ model. This is plausible based on existing research (Black et al., 2023) but was not present our data – potentially because it was not something our survey questions touched on. We should also highlight that relatively few autistic people described positive therapy experiences, so analysis of these factors may not generalise to other people.
Conclusion
This study investigated the nature of social anxiety in autistic adults and heard from autistic adults about their experiences of therapy for social anxiety. We found evidence for both typical and distinct factors influencing social distress in our autistic participants, including the interaction between autism traits and environmental factors causing distress in social situations. Notably, autistic adults felt that their social fears were well-grounded in multiple and ongoing negative experiences with other people. Other research does suggest that autistic people do experience negative reactions from others (e.g. Sasson et al., 2017), which would suggest that social fears may not be out of proportion with the sociocultural context as required for a diagnosis of ‘social anxiety disorder’ (APA, 2013). In addition, many autistic adults reported not benefitting from therapy for social anxiety that they had experienced in routine clinical practice: They thought therapists did not always take the basis of their social fears seriously, did not adapt the therapy process in an individualised way, and did not understand neurodivergence. There is some emerging evidence that modified CBT for social anxiety may be helpful for autistic adults (Bemmer et al., 2021), although results were modest. The concerning experiences of therapy reported by participants in this study call for increased efforts in testing and implementing modifications for therapy for social anxiety. This should include optimising how social anxiety is conceptualised (as well as how therapy is delivered). In the meantime, services should offer autistic people therapies for social anxiety that are empirically validated in the general population, through a principle of person-centred care. Some autistic people will show a ‘typical’ presentation of social anxiety (as some did in the present study), and they may particularly benefit from current therapies for social anxiety. Therapists are also encouraged to use adaptations for autism according to practice-based recommendations set out in this and existing research (e.g. Brice et al., 2021; Spain & Happé, 2020) and to consider what autistic participants in the present study reported with regards to what made for a positive therapeutic experience. It will be important to understand how these work in practice as we optimise therapy to help autistic people deal with social distress.
Supplemental Material
sj-docx-1-aut-10.1177_13623613241251513 – Supplemental material for ‘It’s not always textbook social anxiety’: A survey-based study investigating the nature of social anxiety and experiences of therapy in autistic people
Supplemental material, sj-docx-1-aut-10.1177_13623613241251513 for ‘It’s not always textbook social anxiety’: A survey-based study investigating the nature of social anxiety and experiences of therapy in autistic people by Alexander C Wilson and Fiona Gullon-Scott in Autism
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.