
Abstract
Requests for pathological demand avoidance diagnoses have increased over recent years but pathological demand avoidance remains a controversial issue. We undertook a systematic review of peer-reviewed studies of pathological demand avoidance, using standardised appraisal and synthesis methods, to assess how pathological demand avoidance is identified and to explore the relationships between pathological demand avoidance, autism and other developmental/psychiatric disorders. A search of PsycINFO/PubMed/MEDLINE/Embase identified 13 studies meeting inclusion criteria. Narrative synthesis was chosen due to methodological heterogeneity of the identified studies. Autistic children/adolescents constituted the majority of participants in most studies. Most studies provided clearly defined inclusion criteria together with adequate descriptions of participants and study settings. Almost all studies relied on the parental report of pathological demand avoidance symptoms/diagnosis. Identification of pathological demand avoidance in all studies seemed to be, directly or indirectly, based on the criteria developed by Newson et al. While eight studies used objective criteria for the identification of pathological demand avoidance, the measures used have methodological limitations. Though associations with anxiety have been reported, few studies took account of possible relationships between pathological demand avoidance and other conditions, such as anxiety. Methodological limitations restrict current conclusions regarding the uniformity or stability of the constellation of behaviours associated with pathological demand avoidance or the characteristics of individuals displaying them. Clinical implications of current research are discussed.
Lay Abstract
Requests for diagnoses of pathological demand avoidance have increased over recent years, but pathological demand avoidance remains a controversial issue. The concept of pathological demand avoidance has been criticised for undermining the self-advocacy of autistic people and neglecting the potential role of anxiety as a possible underlying or contributing cause. The current study was undertaken to summarise and review the methodological quality and findings from current research into pathological demand avoidance in children and adolescents. Further aims were to describe how pathological demand avoidance has been identified and to explore the relationships with autism and other developmental and psychiatric disorders. After a comprehensive search, 13 relevant studies using a wide range of methods were identified and systematic quality assessments were undertaken. All the studies had based the identification of pathological demand avoidance, directly or indirectly, on descriptions from the original study by Newson and colleagues. However, the methods used to develop these criteria were not clearly described. Most studies relied exclusively on parental report for data, and there was a general failure to take account of alternative explanations for the behaviours under study. No studies explored the views of individuals with pathological demand avoidance themselves. Problems concerning definition and measurement in the reviewed studies currently limit any conclusions regarding the uniformity or stability of the behaviours described, or the characteristics of individuals displaying them. Relationships between pathological demand avoidance and other emotional and behavioural difficulties should be explored in future research, as should the perspectives of individuals with pathological demand avoidance themselves.
Research, conducted largely in the United Kingdom, suggests that requests for diagnoses of pathological demand avoidance syndrome (PDA) by parents or caregivers have increased markedly over recent years (Green et al., 2018; Stuart et al., 2020). In their original paper, Newson et al. (2003) describe children with PDA as using ‘social manipulation’ to avoid demands; other features include a ‘challenging’ behavioural profile, characterised by resistance to everyday demands and requests; an apparent need to be in control in interactions with others and a tendency to go to extreme lengths to achieve avoidance and control, including socially ‘inappropriate’ behaviours (Newson et al., 2003; O’Nions, Christie, et al., 2014). PDA has been conceptualised, respectively, as a developmental disorder in its own right (Newson et al., 2003) or as a subtype, profile or trait occurring in autistic individuals (Gillberg et al., 2015; Stuart et al., 2020) or other developmental disorders (Gillberg, 2014). Alternative suggestions involve PDA being more accurately conceptualised as a set of symptoms rather than a syndrome (Green et al., 2018).
While some personal accounts indicate that the concept of PDA can be helpful (Thompson, 2019), other reports, including those by autistic academics, have criticised it for undermining the agency and self-advocacy of autistic people (Milton, 2013; Moore, 2020; Woods, 2017, 2018). A particular criticism is that existing accounts make little attempt to understand the behaviours described from the viewpoint of the individuals concerned and neglect the potential role of anxiety in the development of demand avoidant behaviours (Milton, 2013; Woods, 2018). Thus, Milton (2013) argues that demand avoidant behaviour must be understood as rational behaviour from the viewpoint of the autistic person when faced with situations perceived as highly stressful. Woods (2019) suggests referring to PDA as ‘demand avoidance phenomena’, while Gillberg (2014) has proposed replacing the term ‘pathological’ with ‘extreme’. Other clinicians have criticised the concept of PDA as an over-simplistic approach to understand the complex behaviours, leading to a lack of focus on potential contextual (especially social) and transactional factors (Green et al., 2018).
PDA has been mainly described in autistic individuals, a group that is particularly vulnerable to disorders related to stress and anxiety (Hollocks et al., 2019; Kerns et al., 2020; Rosen et al., 2018). However, identification of mental health problems in autism can be challenging for a number of reasons (Helverschou & Martinsen, 2011; Rosen et al., 2018). Autistic individuals frequently have difficulties conveying information about their emotional states or levels of anxiety (Hollocks et al., 2019); mental health problems may present in atypical or unusual ways (Kerns et al., 2020; Postorino et al., 2017) and may not always be easily observable to families, caregivers or clinicians (Bishop-Fitzpatrick et al., 2017; Helverschou & Martinsen, 2011; Postorino et al., 2017). The types of events or stimuli that can give rise to anxiety may also be different, or more varied, in autistic individuals than in the general population (e.g. Kerns et al., 2020; Kildahl et al., 2020b; Lau et al., 2020).
These issues are relevant to the understanding of PDA as they suggest anxiety and other mental health problems could be underlying or contributing causes, even if their presence or influence is not easily observable to others.
Given current controversy surrounding the concept of PDA, the objectives of the current review are to
Critically assess the methodological quality of peer-reviewed studies of PDA;
Describe the ways in which studies have identified or measured PDA;
Explore the relationships between (1) PDA and autism, (2) PDA and other neurodevelopmental conditions and (3) PDA and level of intellectual abilities;
Explore the relationships between PDA and psychiatric disorders.
Methods
Protocol and registration
A systematic review was undertaken according to the principles outlined in Preferred Reporting Guidelines for Systematic Reviews and Meta-Analyses (PRISMA; Moher et al., 2009). A systematic review protocol was registered prior to data extraction (https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=152573). Two changes were made to the protocol during the review: (1) the scope was extended from focusing on autistic individuals only, due to the authors becoming aware of suggestions that PDA may occur also in other neurodevelopmental conditions (Gillberg, 2014); (2) the decision was taken to focus the review on PDA in children and adolescents as the literature on PDA in adults was extremely limited.
Search
Some authors have replaced the word ‘pathological’ with alternatives, such as ‘extreme’; others include the term ‘syndrome’. To encompass these various terminologies, the search included only one term: ‘demand avoidance’. The search was performed in four databases: PsycINFO, PubMed, MEDLINE and Embase. Reference lists for identified papers were scrutinised; Google scholar was used for additional searches, although this yielded few further results. The search concluded on 3 January 2020.
Eligibility criteria and study selection
Any paper describing empirical data regarding pathological/extreme demand avoidance in children or adolescents published in a peer-reviewed journal was included. Studies not in English, or in books, book reviews, commentaries or position papers were excluded, as were papers concerning PDA in adults.
Authors A.N.K. and S.B.H independently screened all abstracts for relevance; a full-text review was performed on all papers referring to PDA or demand avoidant behaviours. Final study selection was completed independently by A.N.K. and S.B.H, and no discrepancies occurred in the final list of included studies.
Data extraction
Data from individual studies were extracted by A.N.K (see Table 1) and checked by A.L.R., E.W., J.M.H. and L.B.L. Because the included studies were few and methodologically heterogeneous, it was decided to synthesise data using a narrative and descriptive approach (Popay et al., 2006). For the current review, this constituted an iterative process, including developing a preliminary synthesis of findings from the included studies, exploring relationships in the data and assessing the robustness of the synthesis (see Popay et al., 2006).
Properties of the included studies.
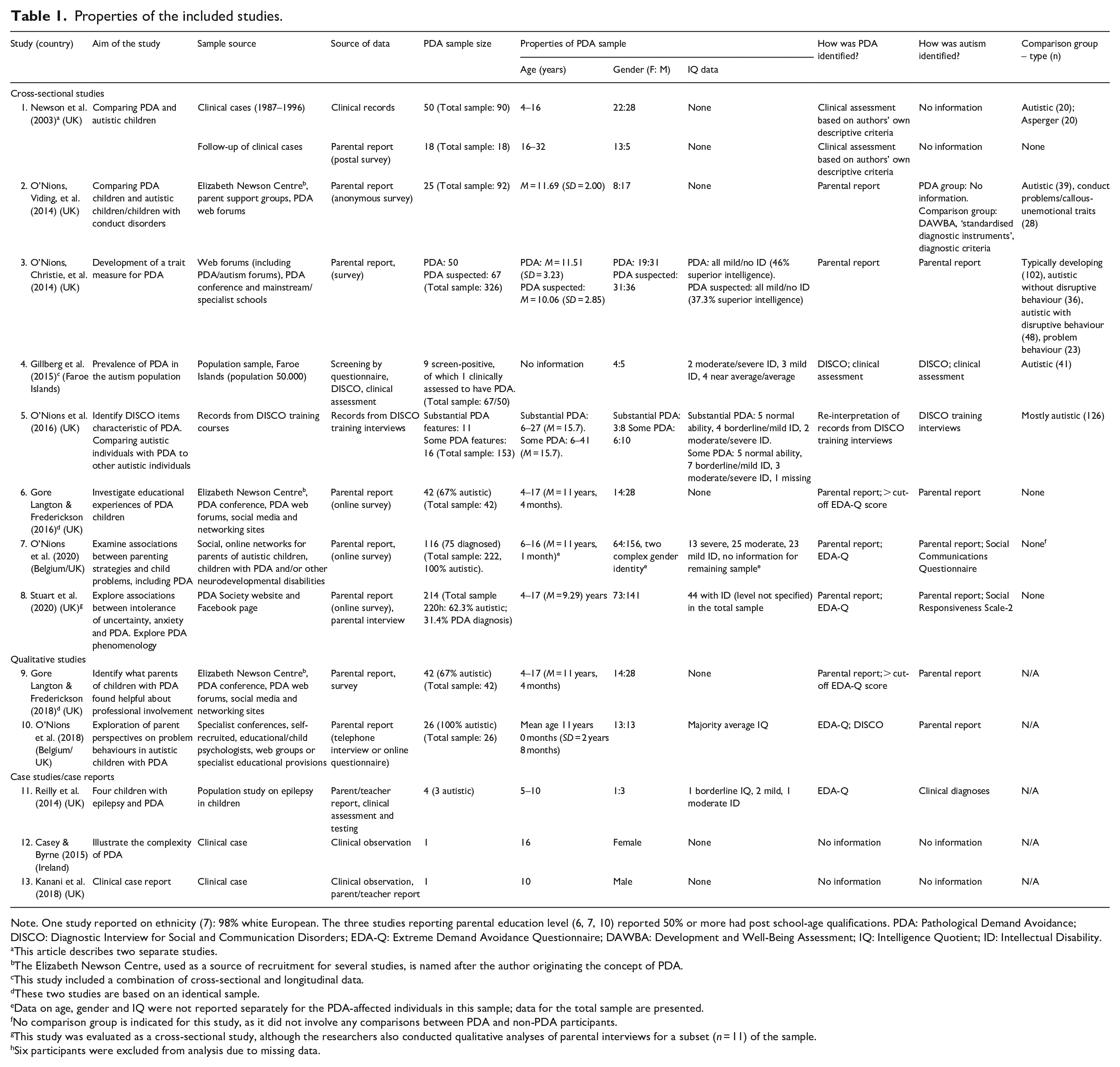
Note. One study reported on ethnicity (7): 98% white European. The three studies reporting parental education level (6, 7, 10) reported 50% or more had post school-age qualifications. PDA: Pathological Demand Avoidance; DISCO: Diagnostic Interview for Social and Communication Disorders; EDA-Q: Extreme Demand Avoidance Questionnaire; DAWBA: Development and Well-Being Assessment; IQ: Intelligence Quotient; ID: Intellectual Disability.
This article describes two separate studies.
The Elizabeth Newson Centre, used as a source of recruitment for several studies, is named after the author originating the concept of PDA.
This study included a combination of cross-sectional and longitudinal data.
These two studies are based on an identical sample.
Data on age, gender and IQ were not reported separately for the PDA-affected individuals in this sample; data for the total sample are presented.
No comparison group is indicated for this study, as it did not involve any comparisons between PDA and non-PDA participants.
This study was evaluated as a cross-sectional study, although the researchers also conducted qualitative analyses of parental interviews for a subset (n = 11) of the sample.
Six participants were excluded from analysis due to missing data.
Quality assessment
For quality assessment, the decision was taken to use the JBI critical appraisal tools, which have been especially developed for systematic reviews (Aromataris & Munn, 2020). Numerous such tools have been developed (Zeng et al., 2015) but the JBI tools were chosen because they use a similar approach (i.e. use of checklists) across different study types, allowing for transparency in quality assessments. Moreover, prior to the search, it was not clear to the authors what methodologies had been applied in the study of PDA, and the JBI system offers a wide range of appraisal tools for different kinds of studies, including single-case studies (Moola et al., 2020). These tools are generally regarded to be of good quality (Zeng et al., 2015).
Following inclusion, all studies were first rated on three general issues (Moola et al., 2020): (1) Were criteria/rationale for inclusion in the study clear? (2) Were study participants and setting described in detail? (3) Were objective, standard criteria used for the measurement of PDA?
Quality assessment was then conducted according to the JBI checklists for analytic cross-sectional studies (Moola et al., 2020), case reports (Moola et al., 2020) and qualitative research (Lockwood et al., 2020), see Appendix 1. Quality assessment criteria varied according to the study type but included adequate descriptions of participants and measures used; congruity between research methodology and research objectives; interpretation of findings, and research and participant involvement. Finally, risk of bias for individual studies and across studies, including issues of sampling and methodology, was assessed. Quality assessment was conducted independently by A.N.K. and P.H. (94.6% agreement). Discrepancies were resolved by discussion. Final assessments were reviewed by all authors and are presented in Tables 2–4.
Evaluation of cross-sectional studies.
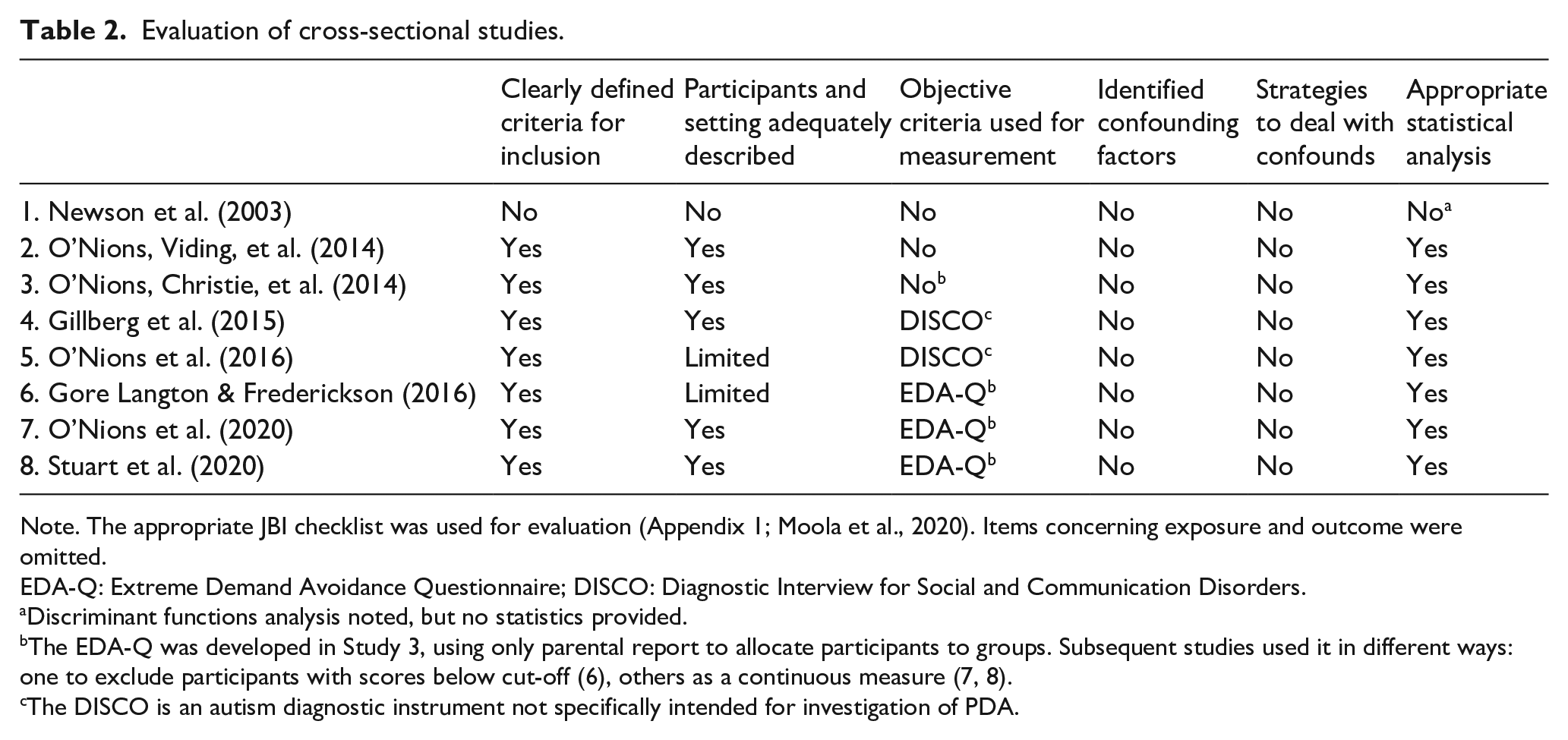
Note. The appropriate JBI checklist was used for evaluation (Appendix 1; Moola et al., 2020). Items concerning exposure and outcome were omitted.
EDA-Q: Extreme Demand Avoidance Questionnaire; DISCO: Diagnostic Interview for Social and Communication Disorders.
Discriminant functions analysis noted, but no statistics provided.
The EDA-Q was developed in Study 3, using only parental report to allocate participants to groups. Subsequent studies used it in different ways: one to exclude participants with scores below cut-off (6), others as a continuous measure (7, 8).
The DISCO is an autism diagnostic instrument not specifically intended for investigation of PDA.
Evaluation of qualitative studies.
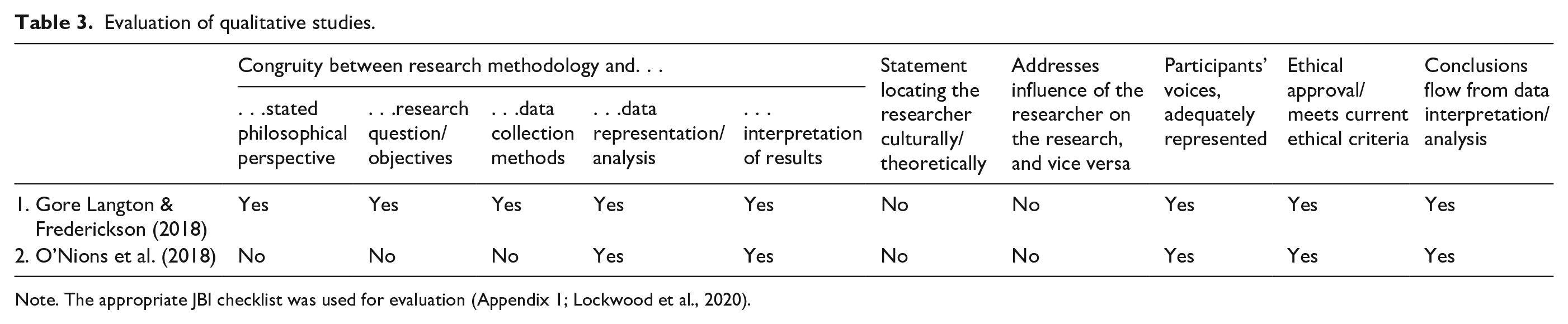
Note. The appropriate JBI checklist was used for evaluation (Appendix 1; Lockwood et al., 2020).
Evaluation of case studies.
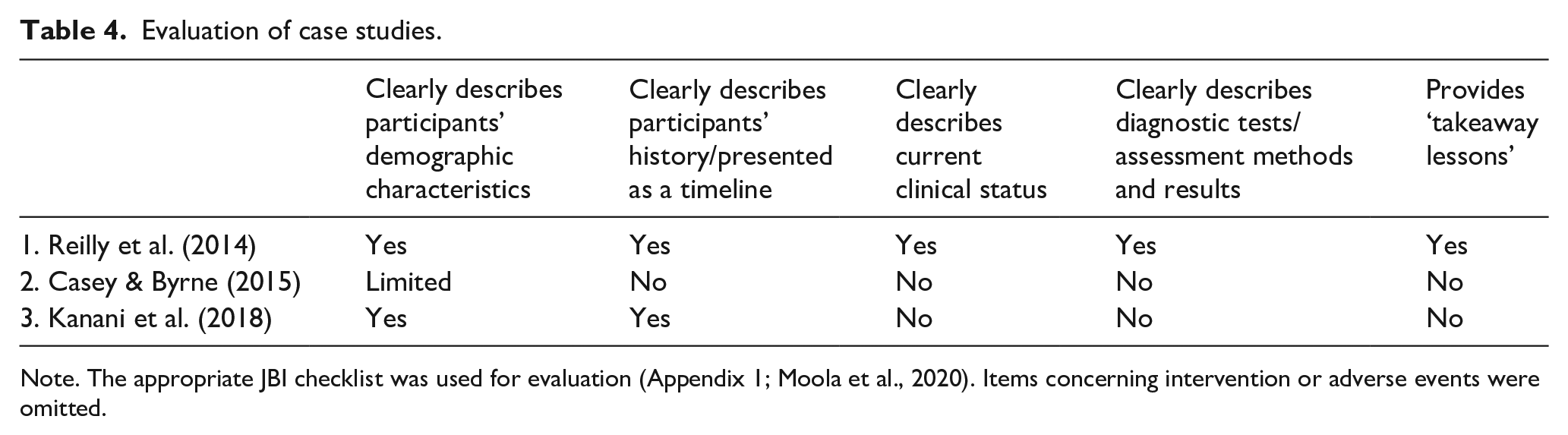
Note. The appropriate JBI checklist was used for evaluation (Appendix 1; Moola et al., 2020). Items concerning intervention or adverse events were omitted.
Community involvement statement
Five of the authors (A.N.K., A.L.R., E.W., J.M.H. and L.B.L.) are mental health professionals working directly with autistic people, their families, and their service providers. In addition, two of the authors (A.N.K., J.M.H.) are siblings of autistic people. There was no further community involvement.
Results
Study selection
Study selection is described in Figure 1. Initial reviews were by title and abstract only; all papers referring to PDA or demand avoidant behaviours were included for full-text review. At this stage, papers clearly not meeting eligibility criteria were excluded; 27 papers were retrieved for full-text review. Meanwhile, 11 papers were excluded for being commentaries, viewpoints or other position papers; 3 excluded as participants were adults. All included studies, together with brief details, are presented in Table 1.
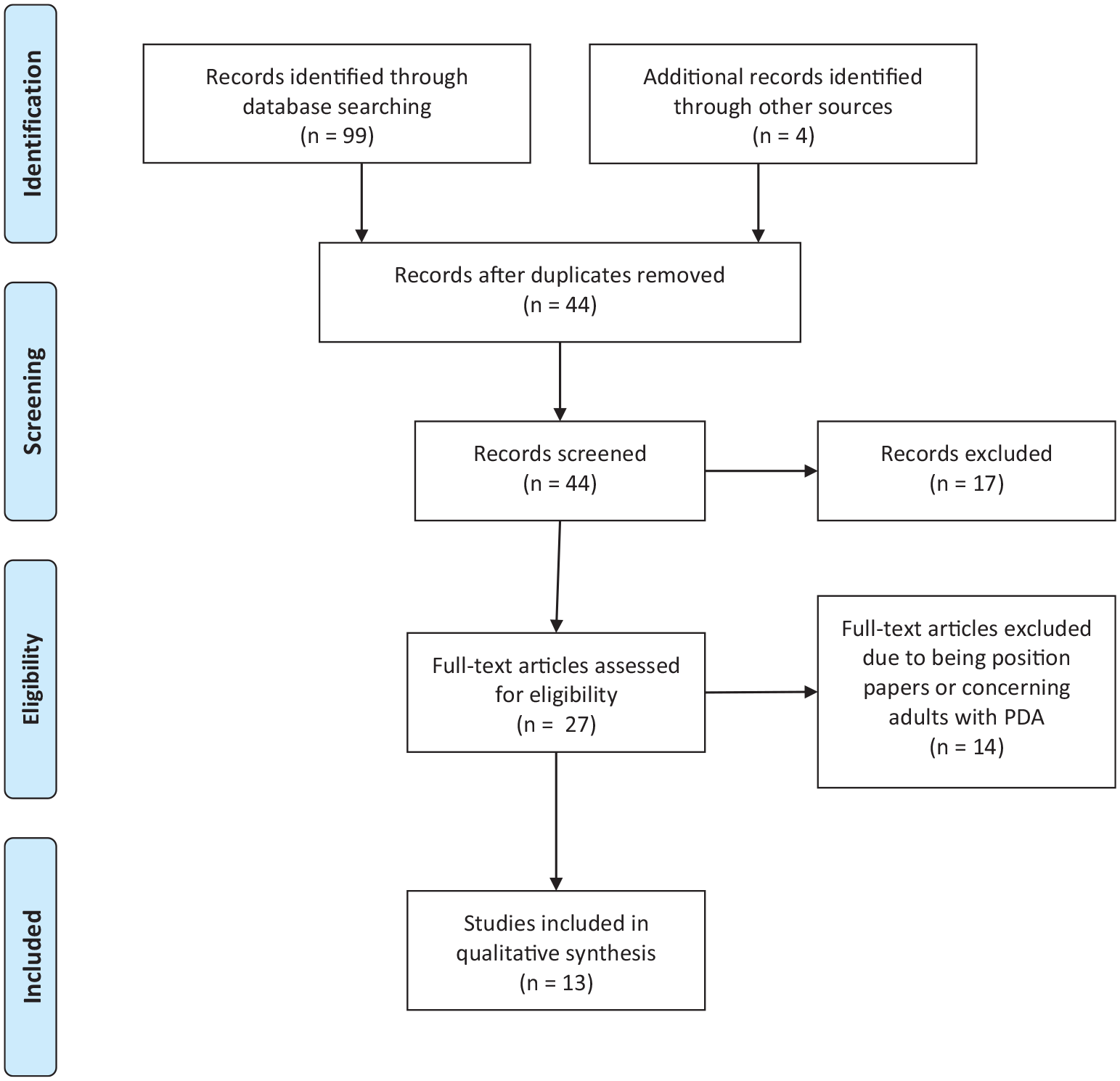
PRISMA flow diagram (from Moher et al., 2009).
Study/participant characteristics
Of the 13 studies, 11 were conducted in the United Kingdom (two of which also involved a collaboration with Belgium); one in the Faroe Islands and one in Ireland. The total number of PDA-affected participants was 650 (36% female; 64% male) with sample size for PDA in the cross-sectional and qualitative studies ranging from 9 to 214; case studies involved one to four participants. Ages ranged from 4 to 47 years, but the mean age in all studies providing this information was 16 years or below (see Table 1 for further details). Data for the cross-sectional and qualitative studies were obtained from parental surveys (postal, online and/or telephone) in eight of the ten studies; data for study (4) were derived from population screening using the Autism Spectrum Screening Questionnaire (Posserud et al., 2009) followed by the clinical assessment on the Diagnostic Interview for Social and Communication Disorders (DISCO; Wing et al., 2002); study (5) used records from DISCO training interviews.
Quality assessment
All included studies were first rated on the three general issues (Moola et al., 2020), see below. Overall quality assessments were then conducted according to the study type: cross-sectional (n = 8; Table 2); qualitative (n = 2; Table 3); and case studies/case reports (n = 3; Table 4). Numbers in brackets below refer to study numbers in the relevant tables.
Aim 1: critically assess the methodological quality of peer-reviewed studies of PDA
All studies (n = 13)
In total, 12 studies (2–13) provided clear criteria/rationale for inclusion in the study and provided details of participants and settings, but in four studies (5, 6, 9 and 12) these descriptions were limited. Meanwhile, 11 studies (2–11 and 13) clearly described how study data were obtained. The majority of studies (n = 8; 4–11) employed objective criteria for assessing PDA, either the Extreme Demand Avoidance Questionnaire (EDA-Q; O’Nions, Christie et al., 2014) or the DISCO.
Cross-sectional studies (n = 8)
With respect to the overall quality ratings (Table 2), seven cross-sectional studies (2–8) provided clearly defined inclusion criteria; applied appropriate statistical analysis and provided at least partial descriptions of participants and study settings. Five studies used the EDA-Q (6–8) or the DISCO (4, 5) for the measurement of PDA, the remainder used no objective, standard criteria. No studies identified confounding factors or described strategies to deal with these.
Most cross-sectional studies (2, 3, 6–8) relied exclusively on parental report for all data, including information regarding inclusion criteria. The remaining studies relied either on data from small clinical cohorts (1); data sets originally collected for other purposes such as an autism population study (4) or protocols from autism diagnostic training courses (5). None of the cross-sectional studies systematically examined possible alternative explanations for the behaviours reported. Five cross-sectional studies included comparison groups, but these were either described in very limited ways (1); recruited in different ways to the PDA group (2); relied exclusively on parental report for assignment to the comparison group (3) or were identified post hoc (4, 5).
Qualitative studies (n = 2)
Study (9) met 8 of the 10 criteria assessed for qualitative studies; Study (10) met only 5 out of 10 (see Table 3). Neither study addressed issues of the researchers’ cultural or theoretical background or the possible influence of the researcher on the research and vice versa.
Both studies (9, 10) recruited parents with previous knowledge of PDA, relied exclusively on parental report and were guided by the original descriptions of Newson et al. (2003). Study (9) used an online survey; Study (10) used a combination of online survey and telephone interviews.
Case studies (n = 3)
Only one paper (11) described more than one case. Two of the three case studies/case reports clearly described participants’ demographic characteristics and provided an adequate history/timeline; one (11) clearly described the current clinical condition and the diagnostic assessment and provided ‘takeaway lessons’, see Table 4.
Overall risk of bias
As indicated in Tables 2–4, on the basis of the assessment criteria used, all included studies had significant methodological limitations and other sources of bias. Five of the eight cross-sectional studies (2, 3, 6–8) and both qualitative studies (9, 10) were based exclusively on data obtained from parental report, both for inclusion criteria and symptom measures. None of the studies included information from individuals with PDA themselves.
There were also fundamental issues in sampling in both the cross-sectional and the qualitative studies. Several studies (2, 6 and 9) recruited parents from the clinic where the term PDA originated and from PDA web forums and conferences (2, 3, 6–10). If the same researchers repeatedly recruit anonymous informants from the same web forums, there is a significant risk of duplication; thus, the total number of cases included in these studies may be lower than it appears. Of the three cross-sectional studies that did not employ these strategies (1, 4, 5), one (1) was based on limited descriptions of a small, clinical cohort from the clinic where the term PDA was conceived; two (4, 5) were based on the adaptation of data collected using an existing autism diagnostic instrument (DISCO; Wing et al., 2002), which is not specifically intended for investigation of PDA. Study (5) was based on the analyses of existing protocols from DISCO training courses, that is, data not primarily collected for research purposes. The one study (4) using a population sample identified just nine cases with possible PDA, only one of whom was clinically assessed to have PDA.
Aim 2: describe the ways in which studies have identified or measured PDA
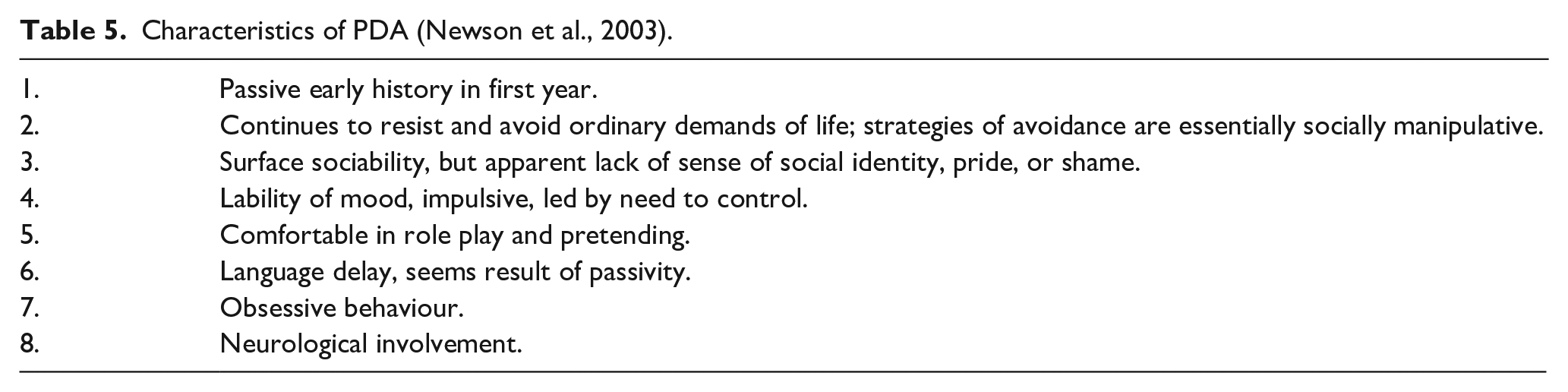
Characteristics of children with PDA were first described by Newson et al. (2003), see Table 5. Their criteria included a mix of broad behavioural descriptions and speculations regarding underlying causes, emotional experiences and motives for demand avoidant behaviours. However, the process of developing these criteria was not clearly specified and some criteria, for example, ‘neurological involvement’, lack specificity. In addition, although groups in the study were clinically defined (as PDA and non-PDA; Newson et al., 2003), findings are compromised by the risk of circularity – that is, the researchers first identified the groups and then studied the differences between them (Green et al., 2018).
Characteristics of PDA (Newson et al., 2003).
The instrument subsequently developed for the identification of PDA, the EDA-Q (O’Nions, Christie, et al., 2014), was used in seven of the included studies. It is based on Newson et al.’s (2003) criteria, previously ‘unpublished material by Newson’ (O’Nions, Christie, et al., 2014, p. 759) and PDA-related items from the DISCO (Wing et al., 2002). A total of 40 candidate items were rated by two authors (O’Nions, Christie, et al., 2014) and by eight other experienced UK clinicians with an interest in PDA; 30 items were selected as being typical of and/or specific to PDA. The resulting questionnaire was administered to six groups of parents who had identified their child as either typically developing (TD, n = 102); autistic with (n = 48) and without (n = 36) ‘disruptive behaviour’ (n = 48); PDA suspected (n = 67) or identified by a professional (n = 50); having ‘disruptive behaviour’/behaviour problems in absence of PDA and autism (n = 23). Several parents completed the questionnaire for more than one of their children, and 23 children in the TD group were siblings of children with PDA (identified or suspected), involving a risk of interdependence of reports including possible contrast effects. The final measure included 26 items, each scored on a 4-point Likert-type scale that differentiated between the PDA and comparison groups. Scores ranged from 0 to 78 with the scores highest for the PDA groups (‘suspected’ M = 56.92, SD = 12.67; ‘identified’ M = 56.51, SD = 11.00) and lowest for the TD group (M = 7.85, SD = 4.41). Autistic children with ‘disruptive behaviours’ scored significantly lower than the PDA groups (M = 42.89, SD = 12.52) but significantly higher than the other comparison groups. Autistic children without ‘disruptive behaviours’ (M = 24.80, SD = 14.91) and children with other kinds of ‘disruptive behaviours/behaviour problems’ (M = 33.94, SD = 12.96) also scored significantly higher than the TD group but not significantly different from each other.
As noted by Stuart et al. (2020), the EDA-Q has good content validity and internal consistency in children with PDA; high levels of internal consistency have been reported (α = 0.87 in Study 3, α = 0.83 in Studies 6, 8) and (in Study 3) good sensitivity/specificity for detection of PDA in children ages 5–11 years (n = 50, sensitivity 0.85, specificity 0.80) and ages 12–17 years (n = 45, sensitivity 0.88, specificity 0.78). In the case study using the EDA-Q (11), three of the four cases scored above these cut-offs.
Parental report using the EDA-Q was used in three subsequent cross-sectional studies (6–8), both qualitative studies (9, 10) and one case study (11). Study (7) used a shorter, 23-item version of the EDA-Q, based on a principal components analysis. For two studies (2–3), identification of PDA was based on parental accounts of whether their child had been diagnosed with PDA or if PDA had been ‘suspected’ or ‘considered’. Two cross-sectional studies (4, 5) and one qualitative study (10) also based their assessment of PDA on the DISCO (Wing et al., 2002). Study (4) used 15 items suggested by the DISCO authors as describing PDA, while the remaining two Studies (5, 10) used 11 DISCO items which the authors considered to match items from the EDA-Q; however, only eight of these corresponded with those items used in Study (4).
Clinical assessments for PDA were only conducted in three cross-sectional studies, but the criteria used in these studies remain unclear (1, 2, 4), and Study (4) only identified a single case. Only one of the case studies (11) clearly described clinical assessment.
Aim 3: explore the relationships between (1) PDA and autism (2) PDA and other neurodevelopmental conditions (3) PDA and level of intellectual abilities
PDA and autism
Although Newson et al.’s original study (1) noted that children in the PDA group failed to meet criteria for autism, they also stated that these children would frequently be diagnosed by other clinicians as having atypical autism. In most subsequent cross-sectional and qualitative studies of PDA, autistic children and adolescents have comprised the majority of participants. Study (2) found that children with PDA did not differ from autistic children with regard to levels of autism ‘traits’. In the case studies, five of the six cases described were reported to be autistic. The two studies using samples that were not specifically recruited for the study of PDA (4, 5) both concluded that the behaviours referred to as PDA may be relatively common across the autism spectrum.
PDA and other neurodevelopmental conditions
No cross-sectional or qualitative studies were identified that explored PDA in children or adolescents with other neurodevelopmental conditions. Studies in which autistic children and adolescents comprised the majority of participants rarely reported formal diagnoses beyond autism and PDA. The exception was one case study (11), in which all four cases were reported to have PDA, co-occurring epilepsy and attention-deficit hyperactivity disorder (ADHD).
PDA and level of intellectual abilities
PDA has been identified throughout the intellectual ability spectrum, ranging from severe intellectual disability (4, 5, 7) to parents reporting superior intelligence (3).
Aim 4: explore the relationships between PDA and psychiatric disorders
Two cross-sectional studies (2, 8) found that PDA was correlated with higher levels of anxiety, while Study (3) reported that the levels of emotional problems in children with PDA were similar to those of children with conduct problems and to those of autistic children with and without other types of disruptive behaviours. Study (2) found that children with PDA did not differ from children with conduct problems on conduct problem measures.
In one of the qualitative studies (10), parents reported phobias, sensory sensitivities, novelty, real or perceived provocation, uncertainty, and negative emotional responses to demands, as possible triggers for PDA. In one of the cross-sectional studies (8), qualitative content analysis of interviews with parents of a subset of the sample (n = 11) revealed themes relating to the need for certainty and responses to uncertainty.
Only one of the case studies (11) examined possible psychiatric symptoms, and two of the four included cases met criteria for Oppositional Defiant Disorder. None met criteria for depression or anxiety. While possible co-occurring conditions were not systematically examined in the remaining case studies, one (13) described an 11-year-old boy with PDA who had a rare genetic mutation that seems to be associated with an increased risk of psychiatric disorder (Kolevzon et al., 2019).
Discussion
The methodological quality of peer-reviewed studies of PDA
The reviewed studies suggest that there is a subset of autistic children and adolescents who display behaviours involving persistent avoidance of perceived demands. However, methodological limitations of the studies reviewed restrict conclusions regarding the specific behaviours or constellation of behaviours that are characteristic of PDA; why and/or how they develop; or the distinguishing features of individuals displaying them. If demand avoidant behaviours do comprise a separate developmental disorder or a trait or subtype in autism, this requires greater evidence of behavioural stability. However, to date there have been no longitudinal studies of the trajectories of PDA behaviours, although two cross-sectional studies (Gillberg et al., 2015; O’Nions et al., 2016) described individuals who had displayed these behaviours in the past but no longer did so when the research was conducted. Currently, we still lack adequate information regarding the uniformity of demand avoidant behaviours, across individuals or over time. Notably, all identified studies had been conducted in Western Europe (mainly in a small number of UK centres), and knowledge from other countries and cultures is lacking.
Methods of identifying or measuring PDA
Despite its ongoing influence on the field, the study that originally described PDA (Newson et al., 2003) does not provide systematic information on how the criteria for PDA were developed; it is also unclear whether these criteria remained exactly the same over the time period that data were collected (1975–2000), and there is a risk of circularity due to its design (Green et al., 2018). These are important limitations since all subsequent studies, including the construction of the EDA-Q, are, to some degree, based on Newson et al.’s criteria. Furthermore, while the development and selection of items for the EDA-Q is fully described by O’Nions, Christie, et al. (2014), the pre-identification of groups in that study (again based on parental report) remains a significant methodological limitation. While the current review only included studies on PDA in children and adolescents, studies involving adults (Eaton & Banting, 2012; Egan et al., 2019; Trundle et al., 2017) also rely on the Newson’s criteria. Moreover, the three studies (4, 5, 10) using the DISCO to aid in the identification of PDA used differing sets of DISCO items.
With regard to differentiation between PDA/non-PDA, only one study (3) has examined group differences using the EDA-Q. While the group of autistic children with other kinds of ‘disruptive’ behaviours had significantly lower scores than the PDA groups, their scores were significantly higher than the remaining comparison groups. As no further group comparisons have been conducted, it remains unclear whether PDA constitutes a distinct condition or merely reflects a difference in severity of ‘disruptive’ behaviours.
Most of the studies relied exclusively on parental report for inclusion criteria and identification of PDA. This heightens the risk of relationships between measures being confounded by common method, reporting, and confirmation bias (Green, 2020). Diagnostic studies in autism suggest that the validity of proxy reports varies according to informants’ expectations, competence, observational skills and relationship with the autistic person (Havdahl et al., 2017; Helverschou & Martinsen, 2011) and are not always in line with reports from the autistic individuals themselves (e.g. Kalvin et al., 2020). Moreover, there is a possibility that parental reports may also have been affected by pre-existing ideas and understandings of PDA gleaned from the PDA web forums and conferences from which they were recruited.
The relationship between PDA, autism and other neurodevelopmental conditions
The majority of participants with PDA in most of the included studies were autistic, and apart from Study (3), there have been few comparisons or analyses of PDA symptoms in other groups. Although one of the case studies reported co-occurring ADHD and epilepsy (Reilly et al., 2014), information about any wider associations with these or other neurodevelopmental conditions is lacking. The association with intellectual ability is also unclear. One study specifically excluded individuals with severe intellectual disabilities from analyses because ‘it is difficult to envisage the whole PDA phenotype developing in an individual with severe or profound general cognitive dysfunction’ (Gillberg et al., 2015, p. 981). In other studies, information about IQ was often lacking. Those studies reporting level of intellectual abilities included participants across the IQ range, from individuals with severe intellectual disability to those reported as being of superior intelligence.
The relationship between PDA and psychiatric disorders
Findings from three studies suggest links between PDA and anxiety (O’Nions et al., 2018; O’Nions, Viding, et al., 2014; Stuart et al., 2020). Stuart et al. (2020) also noted the relationship with intolerance of uncertainty, which is associated with the development of anxiety both in autism and in the general population (Boulter et al., 2014; Joyce et al., 2017). Relationships with other mental health conditions have not been explored.
Avoidant behaviours are an inherent component of many mental health conditions, including anxiety, that are common in autism (Hollocks et al., 2019; Rosen et al., 2018). Indeed, it has been suggested that stress and anxiety are so frequent in autism that they may partly explain ‘core’ features, such as insistence on sameness (Boulter et al., 2014; Joyce et al., 2017; Wigham et al., 2015). Being autistic may also influence how or what events are perceived as stressful or traumatic (Bishop-Fitzpatrick et al., 2017; Kerns et al., 2020; Kildahl et al., 2020b). Thus, it can be challenging for caregivers to understand that autistic children and adolescents have experienced an event, or events, they perceived as stressful or traumatic, and how this may affect development of avoidant behaviours (see Kildahl et al., 2020a; Milton, 2013).
There is also evidence that caregivers and mental health clinicians may struggle with recognition of mental health symptoms, including anxiety, in autistic individuals (e.g. Helverschou & Martinsen, 2011; Postorino et al., 2017). Moreover, parental ratings of such symptoms, including their influence on behaviour, do not always seem to be in line with reports from autistic individuals themselves (Kalvin et al., 2020; Santore et al., 2020). Milton (2012; Davis & Crompton, 2021) has suggested that understanding of autism by those who are not autistic, is hampered by the ‘double empathy problem’. Thus, not only may autistic individuals have problems understanding other people, but others, including parents and caregivers, also have difficulties understanding autistic people. Bolis et al. (2017) propose that a mismatch of interpersonal dynamics (described as ‘dialectical misattunement’) is an underlying factor in the social and communicative difficulties experienced by autistic people. This theory suggests that repeated and reciprocal ‘misattunements’ over time lead to ‘increasing divergencies in communication styles and interactions between non-autistic people and autistic people’ (Davis & Crompton, 2021, p. 2). Failure to recognise, or respond effectively, when an autistic child is experiencing anxiety, discomfort or distress, may lead to the child feeling misunderstood and alone. To alleviate distress, the child may then engage in behaviours perceived by others as socially ‘inappropriate’ or ‘disruptive’, resulting in negative social consequences or sanctions. An accumulation of such experiences over time leads, in turn, to increased use of these ‘problematic’ strategies (see Mitchell et al., 2021).
While there are indications that anxiety, stress, intolerance of uncertainty, or trauma may contribute to the development of avoidant behaviours (Kildahl et al., 2020a; O’Nions et al., 2018; O’Nions, Viding, et al., 2014; Stuart et al., 2020), there is a lack of studies systematically exploring possible associations between PDA and anxiety or traumatic experiences. Instead, current reliance on parental information means that individual psychological experiences influencing these behaviours are under-researched and likely under-reported. These perspectives also highlight the importance of further exploration of the developmental trajectories of PDA behaviours, including what factors may contribute to exacerbating or maintaining them.
Directions for future research
Several authors (Green, 2020; Green et al., 2018; Milton, 2013; Orm et al., 2019) have highlighted the importance of transactional perspectives in understanding demand avoidant behaviours. Demand avoidant behaviours are complex social phenomena, and thus likely to develop over time in interaction between individuals and their surroundings. Critics suggest that referring to these behaviours as PDA situates the difficulties within the individual, thus obscuring the influence of contextual factors (Milton, 2013; Orm et al., 2019). Studies to date have focused almost exclusively on the avoidance aspect of PDA, while the demands eliciting these behaviours have not been systematically investigated. In some cases, it may be that the expectations and demands of caregivers or teachers are perceived as unreasonable, unrealistic or irrelevant by the young people themselves (Milton, 2013). The possible impact of adult expectations or demands, and the contexts and circumstances in which PDA behaviours occur and/or change over time are important topics for further research. This will require more sophisticated approaches, utilising longitudinal and cross-sectional designs, child and adult report, observational and video studies, and qualitative methodologies investigating the subjective experiences of individuals with PDA behaviours. Comprehensive, clinical case studies, providing information about contextual factors will also contribute to further knowledge regarding these behaviours and their developmental trajectories, in particular, if such studies also include information concerning successful and unsuccessful treatment strategies.
Systematic research into the relationships between PDA behaviours and other conditions is lacking and there is a particular need to examine the relationships between mental health issues, social-cognitive abilities and PDA. Conceptualisation of PDA as a distinct phenomenon would require that these behaviours are not sufficiently explained by other conditions, such as anxiety, depression and trauma-related disorders, that typically involve avoidance.
The psychometric properties reported for the EDA-Q to date indicate that this instrument has the potential to be helpful in exploring the degree to which persistent demand avoidant behaviours constitute a distinct condition (Stuart et al., 2020) and investigations into the possible relationships with other psychological and behavioural constructs. However, there is a need for further validation of this measure using independent research teams, larger samples and appropriate statistical methods to identify robust symptom clusters associated with PDA beyond comparing scores between pre-selected groups. More systematic and independent validation of the criteria and assessments developed by Newson and colleagues (2003) will help to resolve the many controversies that currently surround this issue and will be a crucial step in addressing the many problems faced by the children/adolescents who are affected and their parents.
Clinical implications
According to O’Nions et al. (2020): ‘descriptions of PDA include a formulation that places child anxiety as the driver of reactivity, and in doing so de-stigmatises the child and the parent for failures to enforce or conform with norms’. (p. 398). However, if these behaviours are conceptualised as an anxiety-related attempt to increase predictability (c.f. Stuart et al., 2020), it remains possible that this could be just as effectively communicated using existing diagnostic categories, such as anxiety, trauma- and stress-related disorders. If PDA constitutes an autistic behavioural manifestation of experiences such as anxiety or trauma, creating a separate diagnostic label for autistic people may be unhelpful in aiding these individuals to access appropriate services and care (see Camm-Crosbie et al., 2019; Maddox et al., 2020). Different labels for similar experiences in autistic and non-autistic people may also obscure the commonality of these experiences, making it more challenging for non-autistic people to recognise, understand and identify with these experiences in autistic individuals, consequently exacerbating the double empathy problem.
It has also been suggested that making PDA a formal diagnosis risks PDA becoming an explanation for behaviour rather than just a description (Orm et al., 2019). This, again, could lead to an increased risk that underlying difficulties, such as anxiety or trauma, are not adequately addressed. In light of the heterogeneity of autism (Lai et al., 2014), the transactional perspective suggests that the developmental path is unlikely to be identical for all individuals who show demand avoidant behaviours and highlights the importance of assessing and understanding the dynamics of these behaviours in each individual, working in collaboration with affected individuals and their families (Green et al., 2018). Transactional perspectives further suggest that the behaviours described as PDA may develop gradually (Orm et al., 2019) or appear in circumscribed settings (such as school) prior to becoming more generalised. In such cases, conceptualising PDA as a categorical phenomenon (i.e. a formal diagnosis which one either has or not) may be counterproductive to its early detection and prevention.
Finally, it should be noted that, despite the many challenges associated with PDA, none of the studies identified focused specifically on treatment. To develop effective interventions, there is a crucial need to be able to confirm the uniformity of the profile of behaviours related to PDA, the characteristics of individuals displaying them, and relationships with anxiety and other emotional difficulties.
Conclusion
To date, research examining PDA has been hampered by problems concerning definition, construct validity and measurement. Consequently, evidence that PDA is either a separate disorder or constitutes a stable subtype or trait in autistic individuals is currently lacking. Demand avoidant behaviours are clearly a profound challenge for some individuals and their families, and these may be associated with anxiety, trauma or the perception of demands and expectations as fundamentally threatening. Current evidence suggests these behaviours involve an identifiable cluster of parent-reported behaviours in autistic children and adolescents, but it remains unclear whether they represent a distinct condition or primarily differ from other conditions with regard to severity or impact of symptoms. Possible associations with anxiety have been reported, and the EDA-Q may be a helpful tool in further investigations of the relationships between PDA and mental conditions typically involving avoidance. It also remains unclear whether demand avoidant behaviours are more prevalent in autism than in other neurodevelopmental conditions, as there has been no systematic examination of this issue.
In summary, this review highlights many questions about PDA that remain unresolved and demonstrates the need for more systematic and methodologically sound research to examine the relationships between demand avoidance and anxiety, and other mental health conditions, both in autism and other neurodevelopmental conditions.
Footnotes
Appendix 1
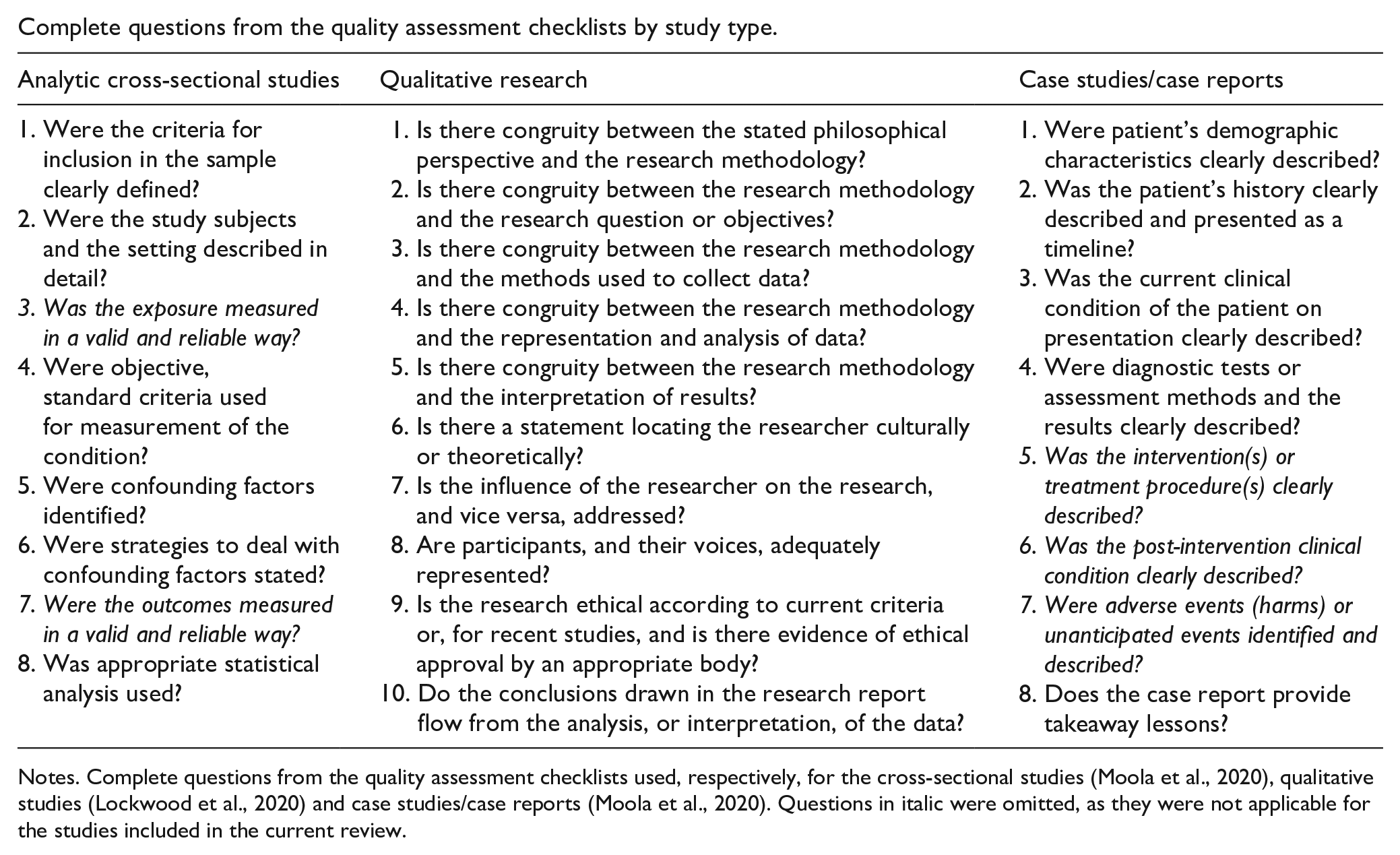
Complete questions from the quality assessment checklists by study type.
| Analytic cross-sectional studies | Qualitative research | Case studies/case reports |
|---|---|---|
| 1. Were the criteria for inclusion in the sample clearly defined? 2. Were the study subjects and the setting described in detail? 3. Was the exposure measured in a valid and reliable way? 4. Were objective, standard criteria used for measurement of the condition? 5. Were confounding factors identified? 6. Were strategies to deal with confounding factors stated? 7. Were the outcomes measured in a valid and reliable way? 8. Was appropriate statistical analysis used? |
1. Is there congruity between the stated philosophical perspective and the research methodology? 2. Is there congruity between the research methodology and the research question or objectives? 3. Is there congruity between the research methodology and the methods used to collect data? 4. Is there congruity between the research methodology and the representation and analysis of data? 5. Is there congruity between the research methodology and the interpretation of results? 6. Is there a statement locating the researcher culturally or theoretically? 7. Is the influence of the researcher on the research, and vice versa, addressed? 8. Are participants, and their voices, adequately represented? 9. Is the research ethical according to current criteria or, for recent studies, and is there evidence of ethical approval by an appropriate body? 10. Do the conclusions drawn in the research report flow from the analysis, or interpretation, of the data? |
1. Were patient’s demographic characteristics clearly described? 2. Was the patient’s history clearly described and presented as a timeline? 3. Was the current clinical condition of the patient on presentation clearly described? 4. Were diagnostic tests or assessment methods and the results clearly described? 5. Was the intervention(s) or treatment procedure(s) clearly described? 6. Was the post-intervention clinical condition clearly described? 7. Were adverse events (harms) or unanticipated events identified and described? 8. Does the case report provide takeaway lessons? |
Notes. Complete questions from the quality assessment checklists used, respectively, for the cross-sectional studies (Moola et al., 2020), qualitative studies (Lockwood et al., 2020) and case studies/case reports (Moola et al., 2020). Questions in italic were omitted, as they were not applicable for the studies included in the current review.
Acknowledgements
The authors thank the Norwegian AUP (Autism, Intellectual Disability, Mental Illness) network group for helpful discussions of PDA, and their colleagues Espen Arnfinn Winther Matre, Trine Lise Bakken, Tale Gjertine Bjørgen and Trine Elisabeth Iversen for their input.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors’ work on this paper was funded by their employers. Open access publishing was funded through an agreement between Sage and the Norwegian consortium for higher education and research (Unit).