
Abstract
‘Pathological Demand Avoidance’ is a term increasingly used by practitioners in the United Kingdom. It was coined to describe a profile of obsessive resistance to everyday demands and requests, with a tendency to resort to ‘socially manipulative’ behaviour, including outrageous or embarrassing acts. Pathological demand avoidance is thought to share aspects of social impairment with autism spectrum disorders, but autism spectrum disorder–appropriate strategies, such as routine and repetition, are described as unhelpful. Outrageous acts and lack of concern for their effects draw parallels with conduct problems and callous-unemotional traits. However, reward-based techniques, effective with conduct problems and callous-unemotional traits, seem not to work in pathological demand avoidance. Despite increasing interest and controversy over the pathological demand avoidance label, there is only one published study to date. We present the first systematic comparison of the behavioural profile of children receiving the term pathological demand avoidance (N = 25) to children with autism spectrum disorders (N = 39) or conduct problems and callous-unemotional traits (N = 28), using parent-report indices of psychopathology. The pathological demand avoidance group displayed comparable levels of autistic traits and peer problems to the autism spectrum disorders group and anti-social traits approaching those seen in the conduct problems and callous-unemotional traits group. Emotional symptoms in pathological demand avoidance exceeded both comparison groups. Findings highlight the extreme behavioural impairment associated with pathological demand avoidance and the need to explore whether behavioural overlap reflects a similar neurocognitive basis to existing groups.
Keywords
Introduction
A major challenge in clinical practice is that cases fail to respect diagnostic or conceptual boundaries, often presenting a confusing or atypical picture. While it is acknowledged that the social presentation of individuals with autism spectrum disorders (ASD) can vary substantially (Wing, 1991), most accounts indicate diminished social motivation, social naivety or social peculiarity. These typical social presentations, indexed via difficulties developing a rapport, maintaining to and fro conversation and responding in a socially appropriate manner, form a key component of our concept of autism.
In the clinic, however, not all children presenting with a qualitative impairment in social interaction and communication fit the autism pattern. ‘Pathological Demand Avoidance’ (PDA) is a term coined by Newson et al., (2003) to describe children who, while ‘reminiscent of autism’, show surprising and challenging features within autism services. PDA has become increasingly widely used by some clinicians, teachers and parents in the United Kingdom and has come to arouse strong emotions. There is disagreement and debate as to whether PDA is truly a syndrome, or whether it labels specific behaviours seen in children with a range of disorders. A further issue is whether it is distinct from ASD, or a manifestation of similar socio-cognitive profile. The depth of interest is demonstrated by a number of over-subscribed conferences on PDA organized by the UK-based National Autistic Society (NAS) in 2011 and inclusion of items measuring PDA traits in the Diagnostic Interview for Social and Communication Disorders (DISCO; Wing et al., 2002). There is clearly a pressing need to accumulate a stronger evidence base with regard to PDA. To date, only one descriptive study, which identified key features from 150 retrospective case reports, has been published (Newson et al., 2003). The aim of this article is to report, for the first time, the profiles of children labelled PDA compared to groups with behavioural overlap, using standardized parent-report instruments.
Descriptively, the key characteristics of PDA are an obsessive resistance to everyday demands and requests, use of socially manipulative or outrageous behaviour to avoid demands, sudden changes in mood apparently associated with a need to control, and ‘surface’ sociability, reflected in social peculiarity, difficulties with peers and lack of social constraint (Newson et al., 2003). Newson described non-compliance in PDA as obsessive, not limited to unpleasant tasks, but at worst, a blanket resistance to accept suggestions, to talk, sit down, take part in fun activities or walk in the same direction as their parents. Children with PDA are described as resorting to extreme, aggressive or socially shocking behaviour if pressed to comply. Newson et al. (2003) described them as ‘socially manipulative’; unlike most children with ASD, they tended to subvert requests by distraction, diversion, threats or behaviour intended to shock or upset. In addition, they lacked a sense of responsibility to others and failed to moderate their behaviour for others’ benefit. Strikingly, many of Newson’s participants seemed oblivious to the fact that they were children, identifying with adults and adopting domineering roles with peers (Newson et al., 2003). Friendships failed and these children were viewed as odd or frightening by others their age. Although apparently of normal intelligence, the demands of complying in the school environment meant that many were excluded or unable to access education (Newson et al., 2003).
Unlike children with oppositional defiant disorder (ODD) or conduct disorder (here referred to as ‘conduct problems’), Newson’s participants behaved publicly in provocative or infantile ways that peers would find humiliating, such as removing their clothes, drawing attention to themselves at a concert or play, asking personal questions, making loud inappropriate comments or having a meltdown in front of peers. Although some studies have reported deficits in social response selection and reading of social situations in children with conduct problems (e.g. Matthys et al., 1999), the nature of these deficits appears different in character to the outrageous or shocking behaviour reported in PDA. Children with conduct problems are usually motivated to maintain their reputation with peers and would be less likely to behave in personally embarrassing ways. Although they might lack respect for authority, it would be unusual for them to believe themselves adults, with the right to insist, for example, that their parents’ guests leave the house.
Rewards are anecdotally described as ineffective in children with PDA; because they are contingent on compliance, this appears a further form of control. In contrast, findings indicate that children with conduct problems are strongly motivated by rewards (O’Brien and Frick, 1996). Although these are clear differentiating features from most children with conduct problems, there may be conceptual overlap between PDA and forms of ‘undersocialized’ conduct disorder included in Diagnostic and Statistical Manual of Mental Disorders (3rd ed.; DSM-III), where aberrant social relating was a prominent feature, potentially reflecting underlying socio-cognitive difficulties (for discussion see Frick and Moffitt, 2010). Other potentially overlapping terms include pervasive refusal syndrome (Taylor et al., 2000), schizoid personality in childhood (Wolff and Barlow, 1979) and ‘borderline’ states (Weil, 1953).
At least three aspects of Newson’s description of PDA also do not appear to fit straightforwardly within the autism spectrum. First, children with PDA are described as responding best to spontaneity, humour and unpredictability – very distinct from the structure and repetition at the core of educational strategy with autism (Kunce and Mesibov, 1998). Second, PDA is described as showing a fairly balanced gender distribution (Newson et al., 2003) in contrast to the strong male bias in ASD (Fombonne, 2003).Third, a preoccupation with role play and fantasy, even difficulty telling pretence from reality, is said to be characteristic of PDA, while absent or delayed pretend play is a marker for ASD (Frith et al., 1991; Leslie, 1987).
The aim of this study was to compare parent-reported behavioural difficulties in children receiving the PDA label and children with autism or conduct problems and callous unemotional traits. Children with conduct problems and callous-unemotional traits (CP/CU), a specifier for DSM-V (2013) indexing a persistent pattern of anti-social behaviour and remorselessness, were included because of the overlap of disruptive and manipulative behaviour (Frick and Moffitt, 2010; Frick and Viding, 2009). Reported instrumental use of shocking or aggressive behaviour in PDA (to avoid or control situations) without concern for the effects on others might resemble instrumental aggression associated with CP/CU, where it is typically employed for material gain or social dominance (Frick et al., 2003; Jones et al., 2011; Viding and Jones, 2008).
New data (collected for the purpose of this study) for children who had received the PDA label were contrasted with existing data from children with ASD, or CP/CU, obtained from a population cohort. Behavioural difficulties, including autistic and anti-social traits, were measured using standardized parent-report questionnaires. The existing data were taken from a large population-based sample, which also provided an indicator of ‘normal’ levels of traits and behaviours, allowing us to estimate the severity of difficulties in PDA.
Method
Participants
PDA group
Parents of 25 children clinically identified as having PDA (mean age = 11.69 years, standard deviation (SD) = 2.00 years, 68% males) participated in the study anonymously, giving informed consent. Questionnaires were distributed via the Elizabeth Newson Centre, parent support groups and PDA web-forums. Parents confirmed that their child had been identified as having PDA by a healthcare professional (paediatrician, educational psychologist, clinical psychologist, child psychologist, psychiatrist). The study was approved by the Psychiatry; Nursing & Midwifery college ethics review board.
Comparison groups
Two comparison groups (children with ASD or CP/CU) were identified from the 12-year follow-up of the Twins Early Development study (TEDS), a population-based longitudinal survey of twins ascertained from national registers of all children born in England and Wales from 1994 to 1996. Of the 16,810 twin pairs on the register, 8438 were contacted for the 12-year study (50.2%). Inclusion criteria were consent for/participation in a recent TEDS study. Of the 8438 approached, 5876 families returned the parent questionnaire. This sample is representative of the UK population, based on census data, in terms of ethnicity, parental employment and educational level (Greven et al., 2011; Hanscombe et al., 2010). Data from only one twin from each pair were used to standardize scale and sub-scale scores for questionnaires and to identify individuals within the population cohort who met criteria for the ASD or CP/CU comparison groups.
Subgroups from within population cohort
For the ASD group (N = 39; mean age = 11.28 years, SD = 0.74 years, 85% males), participants with an autism/atypical autism/Asperger syndrome diagnosis confirmed with the Development and Well-Being Assessment (DAWBA; Goodman et al., 2000) or standardized diagnostic instruments, according to diagnostic criteria, Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000) or International Statistical Classification of Diseases and Related Health Problems, tenth revision (ICD-10) (World Health Organization, 1992), were included. Criteria for inclusion in the CP/CU group were a score of 25 or above on the Anti-social Process Screening Device (APSD) measure of anti-social traits, in line with previous studies (e.g. Budhani and Blair, 2005), resulting in a sample of 28 (mean age = 11.32 years, SD = 0.67 years; 82% males). Four individuals who met criteria for ASD according to the DAWBA and scored above threshold on the APSD were excluded.
Scales
Standardized measures
Measures distributed to parents were as follows: the APSD (Frick and Hare, 2001) with sub-scales callous-unemotional (CU), narcissism and impulsivity; the Childhood Autism Spectrum Test (CAST; Scott et al., 2002) with sub-scales social, communication and restricted and repetitive behaviours and interests (RRBI) (Ronald et al., 2006) and the Strengths and Difficulties Questionnaire (SDQ; Goodman, 1997) with sub-scales pro-social, peer problems, emotional symptoms, hyperactivity and conduct problems. All scales are reported to have good validity and reliability. Participants also received a measure of socio-economic status (SES), derived from the age at which the mother had first child, parental educational qualifications and parental job titles. There was no significant difference in SES across the three groups (F(2, 75) = 2.36, p > .1).
Results
Comparing scale scores across groups
Multivariate analysis of variance (MANOVA), analysis of variance (ANOVA) and t-tests were used to compare scores for questionnaire scales/sub-scales across the three groups (PDA, ASD and CP/CU), using z-scores, standardized based on the mean and SD of the TEDS population cohort. Pair-wise comparisons (PDA vs ASD and PDA vs CP/CU) were conducted on sub-scales if a main effect or interaction was significant. Results are summarized and statistics presented in Table 1 and in relevant figures. Mean raw scores for each group on the measures are detailed in the Supplementary Material.
Post hoc t-tests exploring differences between PDA versus CP/CU and PDA versus ASD across sub-scales.
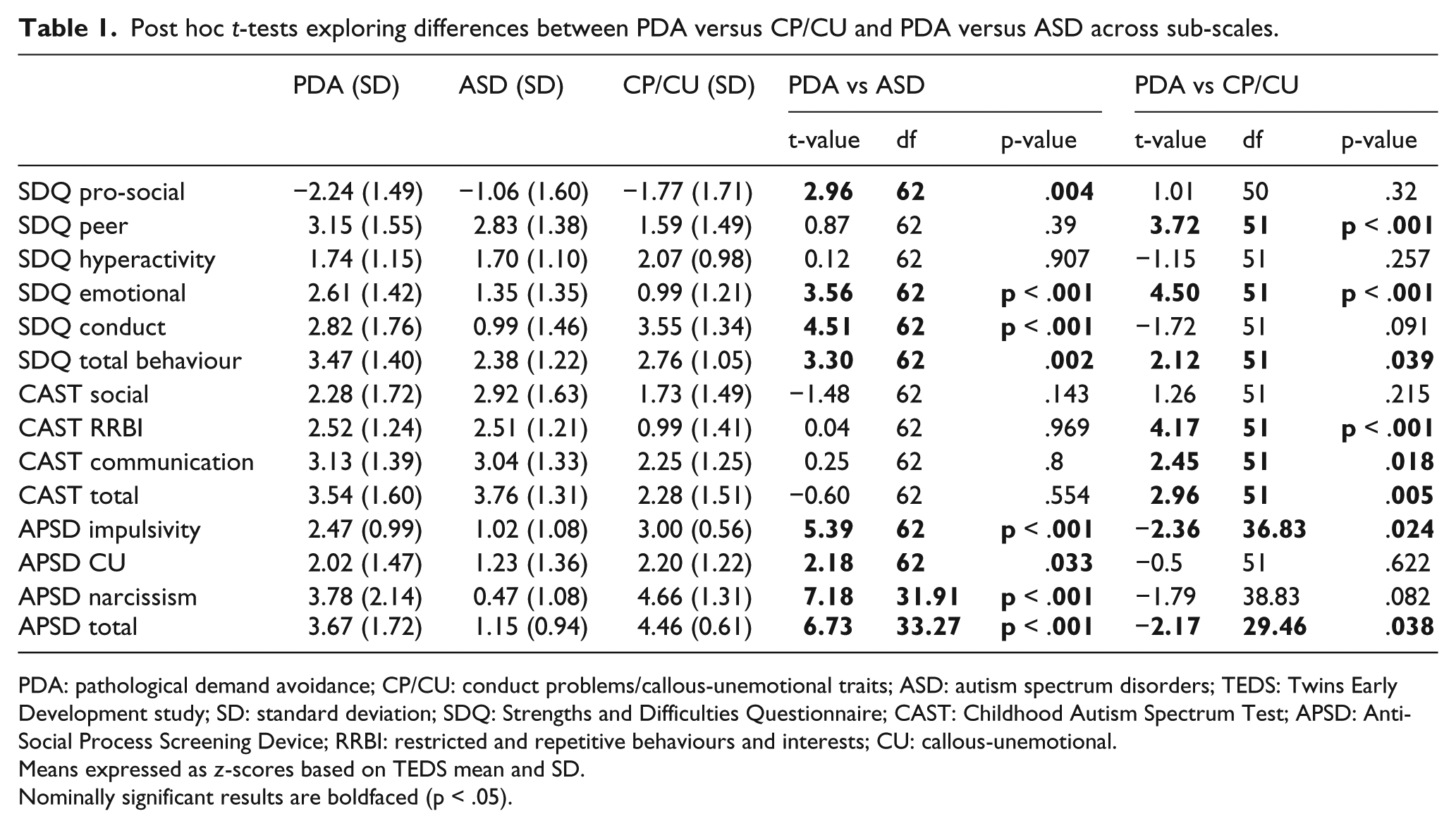
PDA: pathological demand avoidance; CP/CU: conduct problems/callous-unemotional traits; ASD: autism spectrum disorders; TEDS: Twins Early Development study; SD: standard deviation; SDQ: Strengths and Difficulties Questionnaire; CAST: Childhood Autism Spectrum Test; APSD: Anti-Social Process Screening Device; RRBI: restricted and repetitive behaviours and interests; CU: callous-unemotional.
Means expressed as z-scores based on TEDS mean and SD.
Nominally significant results are boldfaced (p < .05).
On the CAST (measuring autistic traits), 72% of the PDA group met the ‘at-risk’ cut off for ASD (a raw score > 14), compared to 79% of the ASD group and 39% of the CP/CU group. The z-scores indicated that the means of PDA and ASD groups were in the most affected 1% of the population sample for CAST total score. Analyses of CAST sub-scales indicated a main effect of group across sub-scales (F(2, 89) = 10.00, p < .001), but the group × sub-scale interaction failed to reach significance (F(4, 178) = 2.18, p = .074; Pillai’s trace). There were no group differences between total or sub-scale scores for PDA and ASD. PDA scored significantly higher than CP/CU on total CAST score and non-social and RRBI sub-scales (Figure 1(a) and Table 1).
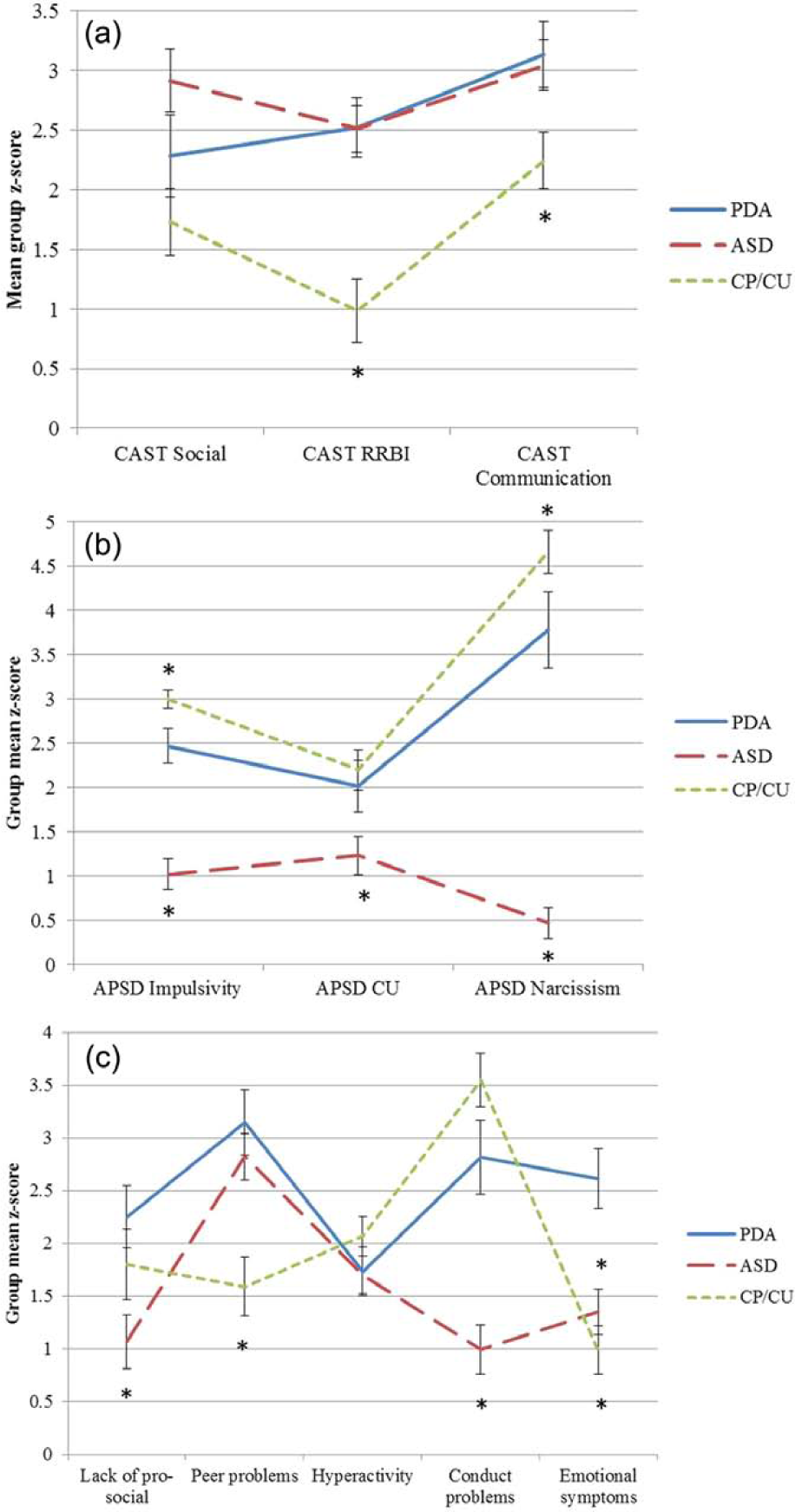
(a) Mean group z-scores for CAST sub-scales by group. (b) Mean group z-scores for APSD sub-scales by group. (c) Mean group z-scores for SDQ sub-scales by group.
On the APSD (measuring anti-social and CU traits), 44% of the PDA group met the ‘atypical’ threshold (a score of 25 or above), compared to 100% in the CP/CU group (selected on the basis that they scored above this threshold), and 0% of the ASD group (the four ASD individuals who scored above threshold were not included in the analysis). The z-scores indicated that for the APSD total score, the PDA and CP/CU group means were in the most affected 1% of the population sample. Analyses of APSD sub-scales revealed a significant main effect of group (F(2, 89) = 73.31, p < .001) and a group × sub-scale, interaction (F(4, 178) = 11.55, p < .001; Pillai’s trace). PDA scored significantly higher than ASD on total score and all sub-scales, but significantly lower than CP/CU for total score and the impulsivity sub-scale. There were no differences between PDA and CP/CU for narcissism and CU traits (Figure 1(b) and Table 1).
On the SDQ (measuring child behaviour problems), the PDA group mean was in the most affected 3% of the population sample for lack of pro-social behaviour, and the most affected 1% for emotional symptoms, peer problems (as were the ASD group) and conduct problems (as were the CP/CU group). Analyses of SDQ sub-scales indicated a main effect of group (F(2, 88) = 9.22, p < .001) and a group × sub-scale interaction (pro-social scale reverse coded) (F(8, 172) = 12.59, p < .001; Pillai’s trace). The PDA group scored significantly higher than ASD for conduct problems and lack of pro-social behaviour, and significantly higher than CP/CU for peer problems (Figure 1(c) and Table 1). The PDA group scored significantly higher than both comparison groups for emotional symptoms and total behavioural problems. All three groups had similarly high levels of hyperactivity (in the most affected 5% or higher relative to the population cohort).
Discussion
This study is the first to use standardized measures to explore the behavioural profile in children receiving the increasingly used label PDA. It represents the first clear evidence that children fitting the PDA description display severe impairments across multiple domains. Comparisons between behaviour in PDA and two putatively overlapping groups, ASD and CP/CU, revealed levels of peer problems and autistic-like traits in PDA comparable to ASD. In addition, levels of anti-social traits and lack of pro-social behaviour in PDA were comparable to those in CP/CU. Notably, the PDA group had significantly higher levels of SDQ-rated emotional symptoms (anxiety/internalizing problems) than either the ASD or CP/CU group.
Consistent with the observation that individuals with PDA often come to the attention of ASD services, CAST scores (measuring autistic traits) resembled ASD across all sub-scales. However, this apparent similarity may reflect endorsement of questionnaire items for different reasons in PDA and ASD groups. For example, endorsement of the CAST item ‘imposes routines on oneself or on others’ may reflect need for sameness in ASD but a need to control interactions in PDA. Research using neurocognitive tasks is needed to explore whether apparent behavioural overlap reflects similar or separable underlying social processing difficulties.
While PDA has historically been thought of in connection with ASD, the current data suggest that children receiving the PDA label show manipulative behaviour similar to that seen in CP/CU; 44% of the PDA group scored in the ‘atypical’ range on the APSD measure. Indeed, very high levels of manipulative or controlling behaviour and lack of remorse evident in descriptions of PDA are similar to the CP/CU profile (Newson et al., 2003). Discrepant between the descriptions is the elicitation of these behaviours in response to demands, obsessive need for control and lack of social constraint, despite social insight sufficient to render them able to manipulate. Very low levels of SDQ-rated pro-social behaviour in PDA are consistent with reported lack of concern for socially appropriate behaviour and poor sense of responsibility towards others. Whether disruptive behaviour in PDA and CP/CU is underpinned by different underlying motivations or neurocognitive deficits remains to be tested.
High levels of SDQ-rated peer problems (comparable to ASD) fit reports of difficulties interacting with peers and poor peer relationships resulting from unpredictable, domineering or socially shocking behaviour in PDA. Significantly higher levels of internalizing symptoms show an additional facet that appears to differentiate PDA from both comparison groups. This could be consistent with the hypothesis that individuals with PDA find demands affectively aversive, or seek to control because of high anxiety.
In sum, the findings suggest that individuals identified as having PDA differ on parent-report measures from two established diagnostic groups with overlapping features: individuals with ASD and individuals with CP/CU. This is consistent with the suggested separation of PDA from usual presentations of ASD, but clearly much further investigation is required.
Despite being the first systematic study of PDA and comparison groups using standardized measures, some limitations of the current study should be noted. Given the absence of a diagnostic algorithm for PDA, the basis on which the label was applied may have differed across participants. Development and refinement of a diagnostic algorithm for PDA based on Newson’s criteria will be an important step in facilitating future research studies and designating boundaries with other constructs. The absence of comparable information about ability level across the groups should be addressed in future studies.
A further limitation is the differing recruitment methods used across participant groups, with the CP/CU and ASD groups coming from a population cohort, and the PDA group partially from clinic referrals, which could have rendered the PDA group a more affected case group. Of note however, the cut off used to identify the CP/CU cohort suggests ‘atypical’ levels of anti-social traits (e.g. Budhani and Blair 2005), and this group included the 28 most affected cases out of a sample of over 5000, indicative of a particularly severe profile. Indeed, levels of anti-social traits were higher in the non-referred CP/CU sample than those in the PDA sample, and levels of hyperactivity were similar across the three groups.
An additional limitation was the use of the APSD to identify both a comparison participant group (the CP/CU group) and as a dependent variable. However, as the focus of interest in this study was the PDA group, it was useful to identify the severity of anti-social traits in PDA, as well as comparing PDA to individuals with atypical levels of anti-social traits on the other measures. Future research should include multiple informants and a wider range of measures including objective clinical measures to interrogate group differences. Given the small sample size, and in particular the small number of girls, these findings should be considered preliminary until they are replicated in a larger group. However, group-level behavioural differences indicate further investigation of this profile is warranted.
While these findings could indicate that the PDA group has an ASD with co-morbid conduct problems, plus additional extreme emotional symptoms, this does not fully accommodate the main difficulties in PDA as outlined in the ‘Introduction’. Specifically, poor social cognition associated with autism appears inconsistent with instrumental use of social manipulation. Impoverished imagination in autism is inconsistent with role play and excessive fantasy engagement in PDA (e.g. taking on the role of a teacher when interacting with peers and telling tall tales). While children with conduct problems may resist complying in order to pursue their own interests – for example, to avoid a task they dislike – obsessive avoidance of even simple requests, regardless of the personal consequences, goes beyond this.
PDA may represent a subset of those who tick boxes for ASD, conduct problems and emotional symptoms, with these additional very characteristic problematic features. However, current educational or therapeutic provision for ASD children with conduct problems does not seem to suit those described as having PDA. The term may well reflect disturbances in more circumscribed socio-cognitive pathways associated with social reciprocity or processing of incoming social cues. These hypotheses must be explored using cognitive-level paradigms. Elucidating the neurocognitive basis of this profile, and possible interventions, remain key issues for future research.
Footnotes
Acknowledgements
We are extremely grateful to Phil Christie, Rukhsana Mehereli, Dorinda Miller, Jacqueline Morgan and Margaret Duncan and to the parents who participated in this study.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
The Twins Early Development study was supported by the United Kingdom Medical Research Council (G0500079). Elizabeth O’Nions was supported by a PhD studentship from the Economic & Social Research Council.