
Abstract
Enteroviruses can cause severe, chronic infections in patients with primary and secondary humoral immunodeficiencies. These patients may benefit from anti-enteroviral therapy. Here, we report a patient with mantle cell lymphoma treated with chemotherapy followed by autologous stem cell transplantation and rituximab maintenance therapy, who presented with echovirus 7-associated deafness and myositis leading to severe disability. She showed marked clinical improvement and enterovirus clearance from faeces and blood after treatment with intravenous immunoglobulins (IVIgs) followed by remdesivir. We demonstrated efficacy of IVIg and remdesivir against echovirus 7 using virus neutralization and cell culture assays, which supports a potential contribution to the treatment success for both therapies.
Introduction
Enteroviruses of the Picornaviridae family are a diverse group of RNA viruses with many serotypes that commonly circulate in the population and cause a broad range of clinical syndromes. Infections in healthy individuals are generally mild and self-limiting and include respiratory infections, gastro-enteritis, hand-foot-mouth disease and meningitis. However, immunocompromised hosts and particularly those with humoral immune defects may be more severely affected, in some cases leading to a chronic infection. For example, chronic enteroviral meningoencephalitis is a well-described clinical entity in patients with X-linked agammaglobulinemia, which can be prevented with immunoglobulin replacement therapy. 1 In recent years, an increasing number of case reports have also suggested a link between the use of B-cell-depleting therapy, such as rituximab, and chronic enterovirus-associated neurological manifestations with potentially fatal outcome. 2 These patients developed fever and a variety of symptoms including headache, cognitive decline and neurological deficits like deafness and aphasia, during or even months to years after cessation of rituximab.3–5 Myositis or myofasciitis have also been described as a clinical feature of chronic enterovirus infections in immunocompromised hosts. 6
Effective treatment is urgently needed for the small group of patients with protracted, severe enterovirus infections. Sporadic cases have been treated with antiviral agents with known in vitro activity against enteroviruses like fluoxetine, pocapavir, favipiravir, nitazoxanide and ribavirin, but with variable success and without efficacy data to support treatment choices. 7 Currently investigated, novel treatment strategies include combinations of multiple antivirals or immune modulating agents that potentiate the innate immune response.8,9 In this case report, we describe an immunocompromised patient with enterovirus-associated acute deafness and myositis, who showed marked clinical improvement and viral clearance after treatment with intravenous immunoglobulins (IVIgs) followed by the broad-spectrum antiviral remdesivir.
Case report
The patient is a 70-year-old woman with a medical history of stage IV mantle cell lymphoma (MCL). For this, she was treated with rituximab/cyclophosphamide/doxorubicin/vincristine/prednisolone (R-CHOP) and rituximab/dexamethasone/cytarabine/cisplatin (R-DHAP) and subsequently with carmustine/etoposide/cytarabine/melphalan (BEAM) and autologous stem cell transplantation followed by 2-monthly rituximab maintenance treatment for a total duration of three years. Six months before hospital admission, she experienced acute bilateral perceptive hearing loss that was steroid-refractory and progressed to deafness. No tumour was found on magnetic resonance imaging (MRI) of the cerebellopontine angle. Auto-immune serology was negative. Liquor puncture revealed polyclonal pleocytosis with a positive real-time 5′UTR PCR for enterovirus (Ct value 27) and otherwise negative polymerase chain reactions (PCR) for neurotropic viruses. At that time, it was considered unlikely that the patient’s deafness was caused by enterovirus infection, because enteroviruses are highly prevalent in the population, do not commonly cause deafness and the patient tested negative by PCR on several earlier nasopharyngeal swabs obtained while she was already symptomatic.
Two months later, she was re-admitted to the hospital for progressive clinical deterioration with severe limb girdle weakness, episodic fever, weight loss and pancytopenia. An 18F-fluorodeoxyglucose positron emission tomography-computed tomography (PET-CT), bone marrow biopsy and repeated MRI of brain and spine did not demonstrate MCL recurrence nor hemophagocytosis. We refrained from a new lumbar puncture because asymptomatic hygromas were detected and a suboccipital liquor puncture was considered too risky. Serum creatine phosphokinase (CPK) was normal, but MRI of the large muscle groups of all extremities showed extensive oedema. Antinuclear antibodies (ANA) and myositis immunoblots were negative. A MRI-guided skin-muscle-fascia biopsy demonstrated a myositis with lymphocytic cellular infiltrate and striking mitochondrial abnormalities. Myxoma resistance protein 1 (Mxa) staining on muscle tissue was positive in addition to a strong interferon type 1 signature in the circulation and upregulation of Interleukin-18, suggestive of a chronic viral infection. Infectious work-up showed a positive PCR for enterovirus (Ct value 34) on feces, in absence of diarrhoea or abdominal complaints. Enterovirus PCRs on muscle tissue as well as on EDTA plasma were also found positive (Ct value 28 and 35, respectively), but again negative on a nasopharyngeal swab. The enterovirus initially found in the cerebrospinal fluid was typed as echovirus 7 (E7) by genotyping of a 350–400 bp sequence fragment of the viral capsid protein (VP)1 gene. 10 We diagnosed this immunocompromised patient with enterovirus-associated deafness and myositis. We started treatment with IVIg of 2 mg/kg body weight divided in 5 daily dosages of 30 g. After completion of IVIg, no significant clinical improvement was observed and enterovirus PCR on EDTA plasma remained positive (Ct value 38). One week later, we also started remdesivir (a loading dose of 200 mg, followed by 100 mg once daily, for 5 days in total). On week 2 of treatment, we noted a significant clinical and neurological improvement and enterovirus PCR was negative on blood and feces. After rehabilitation, she regained the ability to walk unsupported, although some balance issues remained. Deafness also persisted, for which she received a cochlear implant. She continued on maintenance IVIg every 3 weeks and enterovirus remained undetectable by PCR in blood and feces. We discontinued rituximab maintenance treatment for MCL.
We tested the in vitro efficacy of IVIg and remdesivir against E7. For details on the materials and methods, we refer to the Supplemental materials. Attempts to isolate the virus strain from the patient failed, most likely due to relatively low virus loads. Instead, we cultured four previously stored E7 clinical isolates. We also included echovirus 30 (E30), enterovirus A71 (EV-A71, both known to circulate in the Netherlands
11
) and echovirus 1 (E1, known not to circulate in the Netherlands
12
) as controls. Neutralizing antibody (nAb) titers were determined in the IVIg batch from the patient, three additional IVIg batches, and six available sera from the patient before and during the infection. The nAb titers were determined in duplicate using a virus neutralization assay
13
based on the cytopathogenic effect (CPE) and reported as the reciprocal of the dilution where 50% viral neutralization was observed. nAb titers ≥16 and ≥32 were considered positive and protective, respectively.
11
Duplicate measurements never differed more than one twofold dilution step. All IVIg batches contained protective nAb titers ranging from 181 to 1448 against all E7 strains as well as against the E30 and EV-A71, but not against E1 (Figure 1(a)). As expected, the patient sera did not contain nAb titers against any of the enteroviruses. Next, we assessed remdesivir efficacy against E7, E30 and EV-A71 by antiviral testing. Results indicate that 4 µM remdesivir completely inhibited replication of E7 (strain 3) and E30 at the highest viral load of 10−1 after 24 h, while enterovirus A71 was not inhibited (Figure 1(b)). E7 strains 1 and 2 were also completely inhibited by 4 µM remdesivir at viral load 10−1, while strain 4 was inhibited from a viral load of 10−3 (data not shown). In conclusion, both IVIg and remdesivir showed in vitro inhibition of E7 strains. Efficacy of IVIg and remdesivir against clinical enterovirus isolates. (a) Neutralizing antibody (nAb) titers against echovirus 1 (E1), echovirus 30 (E30) and four strains of echovirus 7 (E7) in IVIg from four different batches (shades of purple), including the one that the patient received (IVIg patient), and in six sera (S, shades of green) from the patient before (S1, obtained in 2022) and during the infection (S2-6, obtained between April and July 2024). nAb titers are averages of duplicate measurements, calculated using the Reed Muench method. nAb titers ≥16 and ≥32 were considered positive and protective, respectively. (b) Enterovirus A71 (EV-A71), E7 (3) and E30 cytopathogenic effect (CPE) in single measurements on RD cells after 24, 48 and 72 h of incubation without (shades of red) and with (shades of blue) 4 μM remdesivir (REM). Lower CPE indicates stronger inhibition of the virus.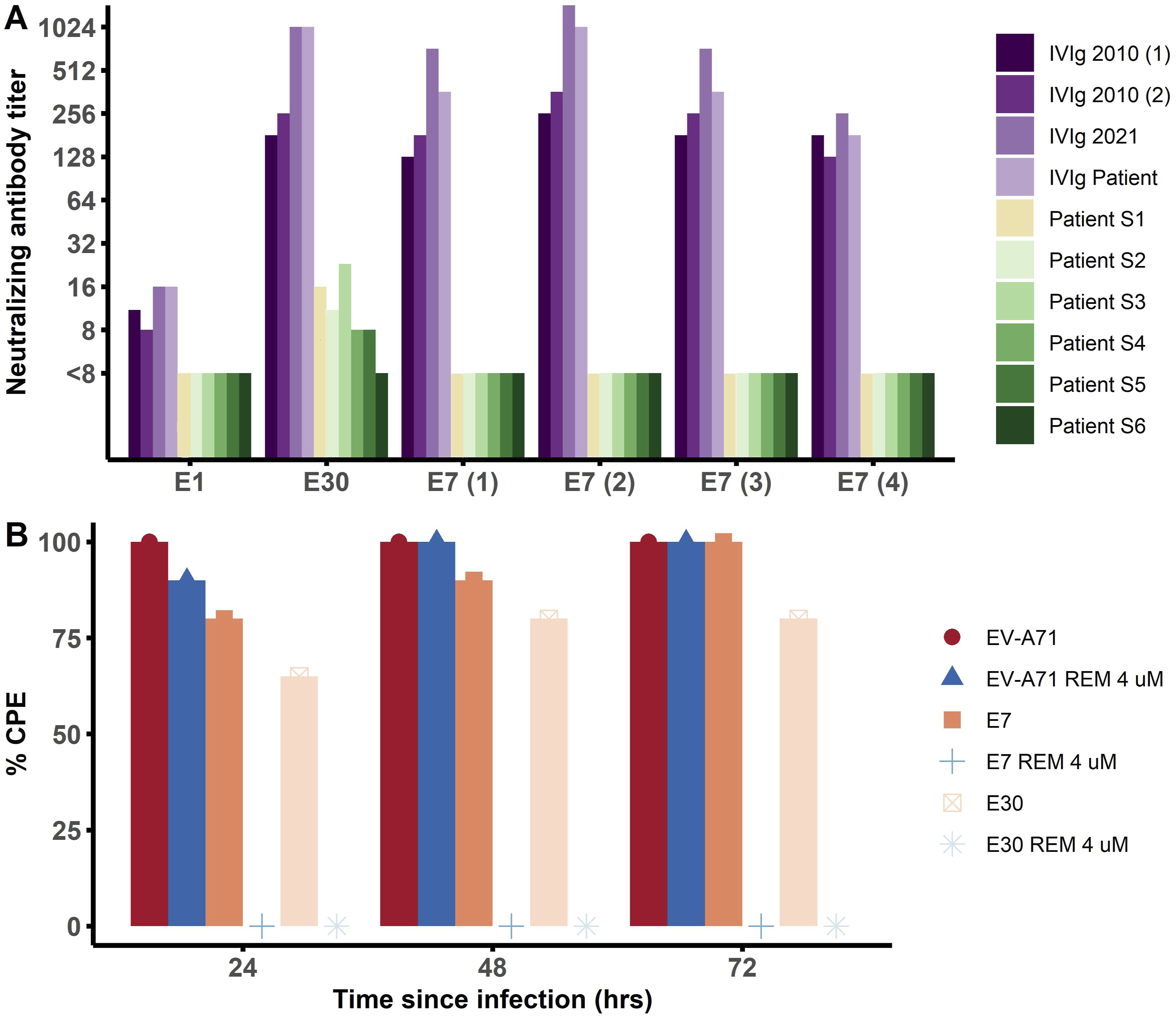
Discussion
This case report demonstrates clinical and virological success of an experimental therapy combining high dose IVIg with the broad-spectrum antiviral remdesivir in an immunocompromised patient with enterovirus-associated deafness and myositis following rituximab. Although these symptoms are not classically attributed to enterovirus infection, similar cases with deafness and/or myositis as presenting symptom have been described previously.2,14,15 In particular, we found one case report of a 67-year-old female on maintenance rituximab therapy for MCL, who presented with hepatitis, bilateral hearing loss and myalgias and had enterovirus (serotype unknown) detected in cerebrospinal fluid by PCR. 4 She was treated with IVIg and showed clinical improvement after the first infusion, though deafness persisted. 4 In our patient, timing of clinical improvement and virus clearance from blood and feces only after starting remdesivir suggests that the antiviral was an important component of the treatment. Nonetheless, we demonstrated in vitro efficacy of both IVIg and remdesivir against replication of E7, so both therapeutic modalities may have contributed to the treatment success. IVIg is a rational treatment option for patients with a- or hypogammaglobulinemia and infection burden, but has shown inconsistent results in severe enterovirus infections.2,5 Remdesivir has known activity against a wide spectrum of RNA viruses, including enteroviruses. 16 Clearance of a long-lasting infection with vaccine-derived poliovirus after treatment with remdesivir for an intercurrent SARS-CoV-2 infection underlined the potential of remdesivir against chronic enterovirus infections. 17 In recent years, a small but growing number of patients received a combination of IVIg and experimental anti-enteroviral agents with known in vitro activity. For example, eight patients in a case series received either fluoxetine, favipiravir, nitazoxanide, pocapavir, ribavirin or a combination next to IVIg, and those who received antiviral therapy early had the most favourable clinical outcomes. 7 In another case study, echovirus 13 persisted in cerebrospinal fluid despite six months of IVIg treatment every four weeks, but the virus was only cleared after the patient started fluoxetine, providing virological evidence that the antiviral therapy was benificial. 14 Because severe enterovirus infections are rare, it is not feasible to obtain robust clinical evidence and establish a unified treatment protocol. We show that additional in vitro testing can provide valuable information to personalize anti-enteroviral therapy. Intestinal organoid models could further elucidate antiviral therapy, as they allow for assessing an agent’s efficacy in a more relevant context. This was demonstrated in a recent case report where failure of remdesivir to eliminate coxsackievirus A1 infection was corroborated in intestinal organoids, whereas virus neutralization assays on monolayers of cells showed sensitivity of the virus to remdesivir. 18 Antiviral efficacy testing requires highly specialized laboratory facilities and skills, so referral of these patients to tertiary healthcare centres with specific virological expertise is recommended. Treatment options can then be offered to the limited number of heavily immunocompromised patients who experience debilitating symptoms from a chronic enterovirus infection.
Supplemental Material
Supplemental Material - Enterovirus-associated deafness and myositis in an immunocompromised patient with in vivo and in vitro efficacy of intravenous immunoglobulins and remdesivir: Case report
Supplemental Material for Enterovirus-associated deafness and myositis in an immunocompromised patient with in vivo and in vitro efficacy of intravenous immunoglobulins and remdesivir: Case report by Emma M. de Koff, Harmen van Andel, Hanna K. de Jong, Anneke J. van der Kooi, Carlemi Calitz, Gerrit Koen, Arjan J. Kwakernaak, and Katja C. Wolthers in Antiviral Therapy.
Footnotes
Ethical considerations
We comply to practice guidelines on research integrity and publishing ethics and the committee on Publication Ethics.
Consent for publication
Patient provided written informed consent for participation in this study and publication of this case.
Author contributions
EdK wrote the manuscript together with AJK and KCW. AJK also provided clinical immunology care of the patient at the in- and outpatient clinic. HvA, HKdJ and AJvdK provided haematological, infectious disease and neurology consultation, respectively. EdK and KCW provided virological consultation. CC and GK performed laboratory investigations under the supervision of KCW. The manuscript was revised and approved by all authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the European Union’s Horizon 2020 Research and Innovation 362 Programme under the grant agreement GUTVIBRATIONS [grant number 953201 to KCW and CC].
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data available on request from the authors.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.