
Abstract
This longitudinal cohort study explored resilience in adolescents with and without acne regarding development of depressive symptoms and suicidal ideation, and investigated the contribution of risk/protective factors. Participants were n = 482 13- to 17-years-olds from the Lifelines Cohort Study. Data were collected at three times (2007–2023). Two group-based trajectory models were fitted. Factors across social and built environments (family functioning, parental rearing, air quality) were accounted for using regression models. All variables except air quality used self-report measures. Two trajectories of suicidal ideation were identified: ‘Low’ (n = 456); and ‘Early Adult Peak’ (n = 26). Two trajectories of depressive symptoms were identified: ‘Low’ (n = 421); and ‘Elevated’ (n = 61). Regarding risk/protective factors, higher acne severity increased odds of membership in the ‘Early Adult Peak’ trajectory. Findings suggest that severe acne exposure in adolescence may increase risks of experiencing suicidal ideation during the transition to adulthood. Implications involve treating youth with acne, particularly severe cases, with a psychodermatological approach.
Keywords
Introduction
Acne affects approximately 85% of 12- to 25-year-olds (Seattle, 2013). It is a highly stigmatised condition. For instance, Shields et al. (2024) found that adults were less comfortable hiring, dating and being friends with people with severe acne compared to those without. Moreover, people with severe acne were rated as more unhygienic, untrustworthy and unintelligent than people without (Shields et al., 2024). Stigmatisation is often experienced by young people with acne and acne-related stigma has been associated with depression in adolescents and adults (Tunca et al., 2024).
Psychodermatology focuses on interactions between the mind and skin (Jafferany, 2007). Psychophysiological conditions are exacerbated by stress (Koo and Lebwohl, 2001), which is an aggravating factor for acne (Jović et al., 2017). Psychodermatology also involves primary dermatological conditions with secondary psychiatric symptoms, creating psychological consequences for wellbeing and quality of life. Psychological comorbidities like depression combined with chronic illness can undermine medical treatment due to poor adherence (DiMatteo et al., 2000), subsequently impacting disease outcomes. This relationship between psychopathology and treatment non-compliance has been reported for acne (Alghofaili et al., 2021).
The importance of psychodermatology in clinical practice is demonstrated by the immense psychosocial burden experienced by people with skin conditions (Hughes et al., 2022). For skin conditions propagated by inflammatory pathways, including acne, increased stress can result in adverse effects (Balieva et al., 2022). The impact of acne on mental health should be considered from the outset, because disease onset can have serious impacts on those affected. Skin conditions affect many aspects of daily life, constituting a large psychological burden with documented connections with depressive symptoms and suicidality (Lukaviciute et al., 2017). Accounting for this, it is not surprising that young people with acne may experience stress and stigmatisation. People with skin conditions are at risk for developing avoidant behaviours or poor coping skills (Bewley et al., 2021). Therefore, investigating resilience, the process of adaptation and coping when exposed to adversities (Luthar et al., 2000), and factors associated with resilience which may help young people to manage and cope with exposure to acne becomes extremely important.
Acne can effect psychological wellbeing with evidence suggesting increased mental health difficulties in affected adolescents (18- to 19-years-old; Halvorsen et al., 2011). Young people have an increased risk of suicide (Ohayon, 2009), which is the 15th leading cause of death globally (World Health Organization, 2014). Suicidal ideation, which increases suicide risk (Franklin et al., 2017), involves thought processes about possible suicide. The most reliable biological indicator of suicidal behaviour is disruption in the serotonergic system, which is implicated in major depressive disorder (MDD; Mann, 2013). Cross-sectional studies report associations between acne, depressive symptoms and suicidal ideation in adolescents. For example, higher suicide risk has been linked to increasingly severe acne in 18- to 19-year-olds (Halvorsen et al., 2011). Tasneem et al. (2023) suggested an increased likelihood of depressive symptoms in adolescents and young adults with acne.
However, long-term investigation of the effects of acne on psychiatric problems is significantly limited. The available empirical landscape of longitudinal research shows mixed findings. For example, a prospective longitudinal study in New Zealand investigated whether acne preceded depression from adolescence to adulthood (data collected from 21 to 38-years-old, with acne reported retrospectively from 15). Participants with acne had a 36% higher risk for MDD than those without (Ramrakha et al., 2016). Yet, an Australian cohort study investigated acne in 14- to 17-years old and psychological morbidity at 6- and 12-month follow-up (Magin et al., 2010), and reported no associations with psychological morbidities. The role and/or nature of risk factors and mechanisms associated with psychological wellbeing and quality of life may change over time and across developmental stages. Longitudinal research could further our understanding of the temporal associations between acne and mental health as people transition from one developmental stage (adolescence) to another (adulthood). Without robust longitudinal evidence, aspects of acne management related to psychological impacts of the condition remains reactive rather than preventive. Hence, more longitudinal research is needed to better understand the risk factors and mechanisms involved, as well as the protective factors which may support resilience.
Although evidence suggests a strong relationship between depression and suicidality, suicidal ideation is the least common symptom reported by people with MDD (Zimmerman et al., 2015). Over 50% of individuals who die by suicide suffer from MDD (American Foundation for Suicide Prevention, 2016). Approximately half of those were not diagnosed with MDD, although they may have suffered other psychiatric disorders or encountered help-seeking barriers (Haavik et al., 2019). However, suicidal ideation can be experienced by people with sub-diagnostic or without depressive symptoms, therefore suicidal ideation and depression may be considered separately as presence of one does not imply the other. The evidence to date demonstrates that acne can have serious psychological impacts in adolescence and young adulthood. Increased knowledge on the impact of acne on suicidal ideation and depressive symptoms, and factors related to resilience which may protect against these outcomes, is needed.
Multisystemic resilience
Multisystemic resilience depends on interacting biological, psychological, social and ecological systems (Ungar and Theron, 2020). It involves the capacity to navigate towards resources within the environment which help sustain wellbeing (Ungar, 2011) and may act as a protective process against the development of pathological consequences of adverse events (Stainton et al., 2019) (e.g. development of suicidal ideation or depressive symptoms in individuals with acne). The multisystemic resilience model accounts for the influence of biological, psychological, social, built and natural environmental systems which interact and influence processes of recovery, adaptation and transformation when under stress (Brown, 2021). Resilience study requires accounts of multiple systems, because no single system or system factor can be fully responsible for the processes associated with resilience and its outcomes (Ungar, 2021). However, the factors within these systems which promote resilience are not fully understood.
We may ask, ‘which promotive and protective factors or processes are best for which people in which contexts at what level of risk exposure and for which outcomes?’ (Ungar, 2019: 2). Resilience varies across each aspect of this question. Psychodermatology research demonstrates close connections between acne (a biological condition) and emotional distress (a psychological outcome), and the psychophysiological nature of acne signifies that stress can exacerbate symptomology (Jović et al., 2017). Stress-flare-up cycles can create prolonged stress exposure and within the context of this adversity, resilience may protect against psychopathology (Shrivastava and Desousa, 2016). Robust evidence is required to understand how factors within multiple systems surrounding the developing young person operate and interact to promote resilience amidst this dermatological adversity.
Resilience and psychological wellbeing
The level of adversity exposure may increase the likelihood of developing psychiatric disorders and symptoms including depression and suicidality (Edward, 2005). Acne severity is positively connected to odds of depressive symptoms in 12- to 40-years-olds (Tasneem et al., 2023), suggesting that the level of acne exposure plays a role in the development of psychological symptoms. Resilience may mitigate the role of suicidal ideation (Johnson et al., 2010) and depression related to acne by diminishing symptom severity (Wingo et al., 2010). Resilience research has investigated psychiatric symptoms in youth with chronic illnesses (Kim et al., 2019), however there has been little investigation into acne. This gap in empirical evidence may reflect traditional framing of acne mostly as a physical health condition without considering its psychosocial impact, or potential factors associated with resilience in light of exposure to such impacts. Acne has been suggested as the most common chronic skin condition in young people with estimates showing it affects up to 85% of 12- to 25-years-olds (Seattle, 2013). Considering the significant comorbid mental health difficulties in youth with skin conditions including acne (Flinn et al., 2025), it is important to identify factors which serve as protective resilience agents.
In light of increasing awareness of adolescent mental health and the intensifying influence of appearance-related stressors, investigating resilience in young people with acne represents a timely and necessary extension of current psychological research.
Risk and protective factors associated with resilience
To approach resilience holistically, it is imperative to investigate factors across system levels, including the social and built environments (Ungar and Theron, 2020). The social environment involves a persons’ relationships, society and culture. In recent decades, the understanding and treatment of illness in youth has shifted towards consideration of family context (Crespo et al., 2013). The transition from adolescence to adulthood in the context of acne presents challenges for individuals, and their families. A study of personal burden of isotretinoin therapy, treatment for severe acne involving monthly clinic visits, found that 65% of children and 81% of caregivers missed school or work due to clinic visits (Mori et al., 2016). Therefore, managing severe acne in youth can have direct impacts on families. Family functioning refers to the effectiveness of family members regarding communication, emotional ties and coping with external events (Olson et al., 1983). Family functioning and context are important because they set foundations for later socialisation, developmental changes and socioemotional skills (Dworkin and Serido, 2017; Morris et al., 2007). Dysfunctional families can put youth at-risk of developing mental health difficulties, including through experiencing emotional rejection and invalidation (Kganyago Mphaphuli, 2023). Poor family functioning, including hostile and critical behaviour by parents, is demonstrated to predict depression in young adults (mean age 21 years; Yu et al., 2015), while high conflict and parental psychological control is associated with suicidal ideation and behaviour in adolescents (van Renen and Wild, 2008). In contrast, a longitudinal study in the United States following adolescents into midlife (aged 12–42 years) suggested that positive family functioning, including high cohesion and positive family relationships, was associated with fewer depressive symptoms over time (Chen and Harris, 2019). Another longitudinal study of adolescents (mean age 12 years) in China suggested that when facing adversity, family functioning predicts resilience over time (Dou et al., 2023). Family functioning is directly related to parental rearing, with parenting styles and practices forming key components of the overall functioning and emotional climate of families (Matejevic et al., 2014; Morris et al., 2007). These factors may interact to affect adolescents’ emotion regulation and adjustment (Morris et al., 2007), making them important within resilience research.
Parenting rearing encompasses care provided by parents/caregivers to their children, with theoretical models often comprising acceptance/warmth and rejection (Arrindell et al., 1999). Positive parenting styles may act as foundations for positive family functioning, with parental warmth in childhood contributing to better coping and wellbeing in adulthood (Moran et al., 2018). In contrast, parental rejection may contribute to dysfunctional family patterns including emotional dysregulation (Di Giunta et al., 2022). Parenting style is suggested to be an aetiological factor influencing vulnerability to mental illness (Arrindell et al., 1999), and positive parental rearing could mitigate manifestations of psychological disorders through resilience (Richter-Kornweitz, 2011). A study of 11- to 18-year-olds reported that parental emotional warmth was positively associated with resilience (Feng et al., 2024), whereas rejection was negatively associated. Moreover, parental rejection has been associated with depressive symptoms (Petrowski et al., 2014), and suicidality in adults (Sobrinho et al., 2016). Adolescence is a critical developmental period characterised by immense changes. Building supportive social environments through family functioning and parental rearing is particularly important during this period given their impacts on psychological wellbeing.
The built environment involves human-made conditions and structures. To date, there has been little resilience research including factors existing and operating within the built environment. Multisystemic resilience research needs research addressing multiple system levels within a single study. Psychological research to date has often focused on psychosocial approaches and explanations of resilience. However, inclusion of the built environment is important because it can have serious impacts on mental and physical health. Air pollution, for example, is a major cause of premature death, while significant disease burden could be alleviated through air pollution (World Health Organization, 2023). In Germany, Petrowski et al. (2019) demonstrated that particulate matter (PM) exposure significantly affected chronic stress, which in turn can negatively affect family functioning (Repetti et al., 2002) and the social environment. PM and nitrogen dioxide (NO2) have been associated with greater risk of in children and young adults (Buoli et al., 2018), and increased suicide attempts (Szyszkowicz et al., 2010). In fact, some researchers suggest causal pathways between air pollutants and mental disorders (e.g. Prata et al., 2017). Furthermore, air pollution has been linked to changes in biological mechanisms including inflammation and oxidative stress (Kelishadi et al., 2009), both of which are implicated in acne development (Tanghetti, 2013; Wong et al., 2016). Although air pollution poses risks to young peoples’ psychological and physical wellbeing, parental support may lessen this influence, with Feng et al. (2023) suggesting that caregivers could improve parenting styles to provide more emotional support in order to alleviate stress caused by air pollution.
Given the risks associated with built and social environment factors, it is important to address these systems in order to better understand how resilience operates in the context of dermatological adversity.
The present study
Longitudinal research involving youth with acne and repeated mental health assessments is needed to understand prospective associations between the mind and skin during the transition from adolescence to adulthood. There has been some investigation to date (e.g. Magin et al., 2010; Ramrakha et al., 2016), which yielded a lack of consensus on the associations between mental health and acne in adolescent cohorts.
There is also limited research on resilience in youth with acne. Existing evidence is predominantly cross-sectional and treats resilience as a singular, measurable construct. Researchers created a tool for identifying paediatric dermatology patients (including acne) requiring psychosocial support, including resilience within the psychosocial domain (Zambare et al., 2022). A study in Egypt investigated psychological impacts of acne in 16- to 19-year-olds, reporting gender differences in ‘resilience severity’ (psychometric scale; Elsadek et al., 2021). These present one-dimensional pictures of resilience and its relationships with psychopathology in the context of acne, and do not capture the complexities and multisystemic nature of resilience. To date, to our knowledge, there is no longitudinal research on multisystemic resilience in the context of acne in adolescents or young adults. Longitudinal research identifying patterns of suicidal ideation and depressive symptoms during these periods is needed to understand resilience in youth with acne.
The present study sought to longitudinally examine multisystemic resilience and trajectories (patterns of change) of suicidal ideation and depressive symptoms in adolescents with and without acne. We aimed to explore resilience regarding the development of psychopathological outcomes, and to understand the contribution of risk and protective factors across system levels. The objectives were:
To investigate resilience in adolescents with and without acne regarding the development of (i) suicidal ideation and (ii) depressive symptoms;
To examine whether risk and protective factors identified across system levels predict the development of psychopathological outcomes.
Method
We used select secondary data from the Lifelines Cohort Study. Lifelines is a multidisciplinary prospective population-based cohort study examining in a unique three-generation design the health and health-related behaviours of 167,729 persons living in the North of the Netherlands. It employs a broad range of investigative procedures in assessing the biomedical, socio-demographic, behavioural, physical and psychological factors which contribute to the health and disease of the general population, with a special focus on multi-morbidity and complex genetics. The study design, sampling procedure and cohort profile are described in full elsewhere (Scholtens et al., 2014). In short, general practitioners invited patients (25- to 50-years-old) to participate. Inhabitants of the northern provinces of the Netherlands could self-register on the Lifelines website. Participants were asked to invite family members to participate (i.e. family referral). Children and adolescents (under 18-years-old) could only take part if a parent was also participating. The Lifelines Cohort Study was approved by the medical ethical committee of the University Medical Center Groningen, The Netherlands, document number METC UMCG METc 2007/152. All participants provided informed consent prior to participation.
For our selected sample, time 1 (1A: Baseline) data were collected between April 2010 and December 2013. Time 2 (2A) data were collected between July 2014 and December 2017. Time 3 (3A) data were collected between October 2019 and November 2023.
The study procedure for the total Lifelines sample is as follows. Visit 1A involved attending a Lifelines location where a physician’s assistant performed various physical measurements, collected the general questionnaire (completed by parents) and instructed adolescent participants (13- to 17-years-old) to fill in the youth questionnaire. Visit 1A lasted 60 minutes (plus 30–45 minutes for the youth questionnaire). Visit 2A similarly involved attending a Lifelines location where physical measurements were taken. Visit 2A lasted 20 minutes (plus time for computer tests). Scheduled on-site visits for 3A were interrupted due to COVID-19 and digital questionnaires were completed at home. In-depth descriptions of each assessment period is described elsewhere (Lifelines Cohort Study, 2025b).
This study included participants aged 13- to 17-years-old at baseline, and had complete data for the selected outcome measures at 1A, 2A and 3A. Figure 1 presents the selection of the sample. All participants in our sample were recruited via family referral. For our adolescent sample, non-responders were more likely to be female, and there were no differences in age or ethnicity. Reasons for withdrawal were not available for our specific sample. Reasons for withdrawal for the total Lifelines sample included: too time-consuming, lost interest, lost trust in big data/negative media attention and moved outside the region.
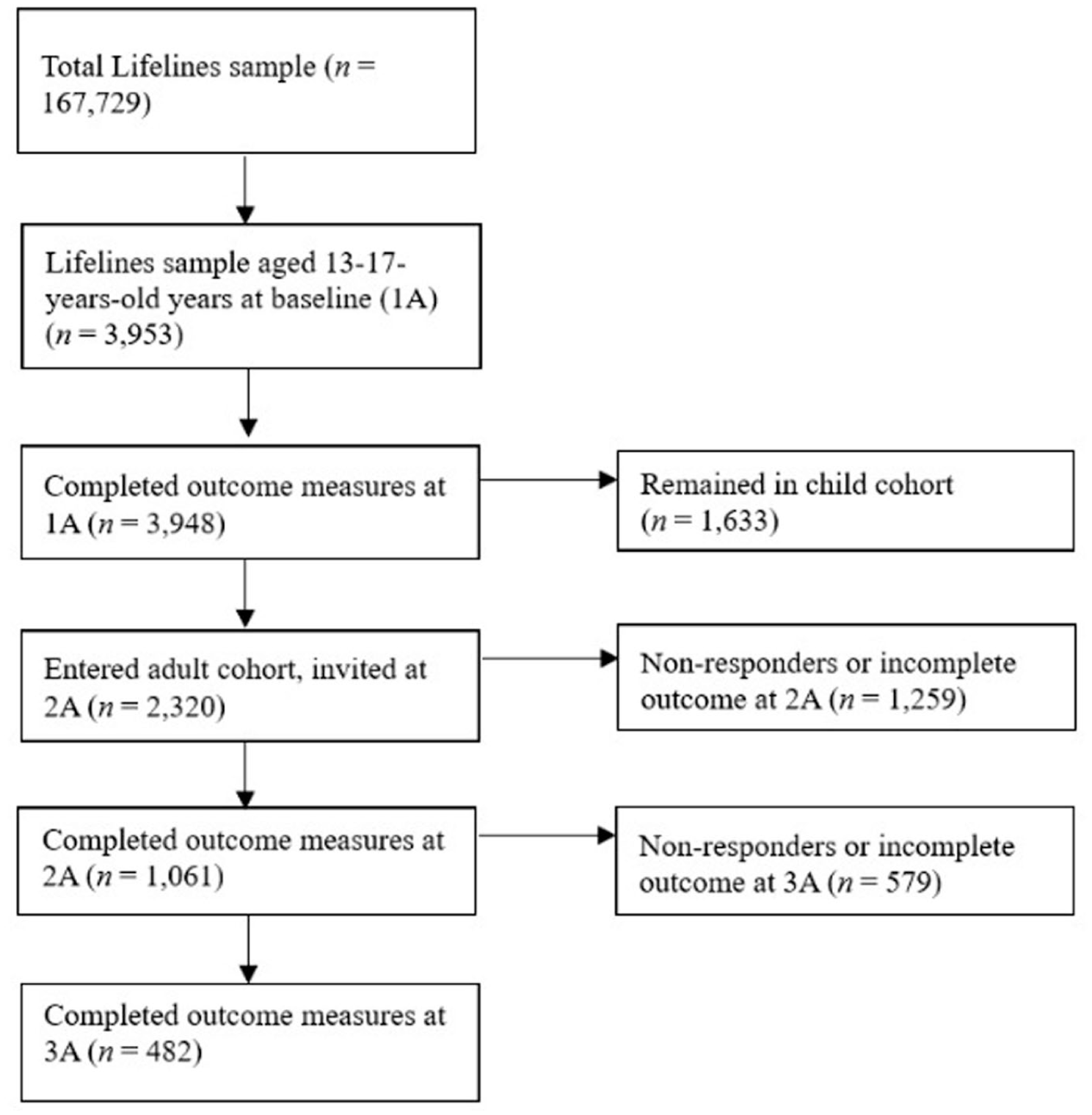
Selection of the analytical sample.
Outcomes
Suicidal ideation
At 1A, a single binary item from the Youth Self Report (YSR; Achenbach et al., 2001) was used. The YSR is designed for 11- to 17-year-olds. Responses refer to symptoms experienced in the preceding 6 months. At visits 2A and 3A, a single binary item from the Mini-International Neuropsychiatric Interview (MINI; Sheehan et al., 1998) was used. Responses refer to symptoms experienced in the past 2 weeks. Items were self-reported by adolescents.
Depressive symptoms
At 1A, the Diagnostic and Statistical Manual of Mental Disorders (DSM) Affective Problems subscale of the YSR was used. Clinical depressive symptoms were classified according to Achenbach (2013) and Achenbach et al. (2001). The scale comprises Dysthymia and MDD and has acceptable diagnostic power for DSM-IV disorders (Lacalle et al., 2012). Reliability was acceptable (α = 0.72; Ω = 0.73). At 2A and 3A the MINI was used. Symptoms of MDD and Dysthymia were used to classify participants into categories of elevated depressive symptoms, according to the DSM-IV (American Psychiatric Association, 2000). Reliability was good at 2A (α = 0.80; Ω = 0.80), and acceptable at 3A (α = 0.79; Ω = 0.80). Items were self-reported by adolescents.
Acne exposure
Acne was measured at 1A using the item, ‘Acne/can you indicate how much you suffered from this problem in the past year?’. Response options were: not at all; a little; a lot; and extremely. Higher scores indicated higher acne severity. This was self-reported by adolescents.
Factors associated with resilience
Family functioning
Family functioning was measured at 1A using the general family functioning subscale of the McMaster Family Assessment Device (Epstein et al., 1983), assessing overall family functioning. Items were reported by parents. Items were rated on a 4-point Likert scale (1 = Strongly Disagree, 4 = Strongly Agree). Higher scores indicated healthier family functioning. The subscale showed very good internal consistency (α = 0.90; ω = 0.90).
Rearing style
Two subscales (Emotional Warmth; Rejection) from the Short Egna Minnen Betraffande Uppfostran for Adolescents (Arrindell et al., 1999) measured parental rearing at 1A. Items were rated on a 4-point Likert scale (1 = No, never to 4 = Yes, almost always). Higher scores indicated higher emotional warmth and rejection respectively. The Emotional Warmth and Rejections subscales respectively showed very good (α = 0.89; ω = 0.88) and good internal consistency (α = 0.80; ω = 0.78). Items were self-reported by adolescents.
Air pollution
Annual mean exposures to NO2 and particulate matter with aerodynamic diameter less than 2.5 μm (PM2.5) were estimated using linked data from the Effects of Low-Level Air Pollution: A Study in Europe project (ELAPSE; Strak et al., 2021). In short, the home addresses of participants were collected at 1A and linked to air pollution data from ELAPSE. Annual mean exposures to NO2 and PM2.5 were estimated using land-use regression models, which are commonly used in epidemiological and environmental studies to estimate air pollution exposures in urban areas. Detailed information is presented elsewhere (de Hoogh et al., 2016, 2018).
Statistical analyses
Group-based trajectory modelling (GBTM; Jones and Nagin, 2007) was applied to examine suicidal ideation and depressive symptoms from adolescence into adulthood. GBTM is a specialised application of finite mixture modelling, assuming multiple groups within a population with different trajectories over time (Nagin and Odgers, 2010). Two GBTMs were estimated: (i) suicidal ideation, age; and (ii) depressive symptoms, age. The trajectory models were built using a stepwise approach.
Step 1: The basic models were built with three repeated measures of (i) suicidal ideation and (ii) depressive symptoms, using binary logit models (1A, 2A, 3A). Selection of the number of groups was based on two aspects: first, the optimal number of groups (two to four groups) were compared using Bayesian information criterion (BIC; Schwarz, 1978) and Akaike’s information criterion (AIC; Dziak et al., 2019). Second, the optimal shape of trajectories were explored by varying growth terms and evaluated based on: (i) the average posterior probabilities (APP) exceeding 0.7; (ii) the odds of correct classification exceeding 5.0; (iii) close correspondence between the probability of group membership and the posterior probability of group membership; and (iv) each group comprising >5% of the sample (Nagin, 2005; Nagin and Odgers, 2010). Lastly, groups were assigned nominal labels.
Step 2: To analyse determinants of trajectories, multivariable binomial logistic regression analyses were performed. These estimated associations between risk factors and trajectory group assignment. Logistic regression models were fitted in steps in terms of predictors: Model 1: acne and gender (male, female); model 2: Model 1 plus social environment factors; and model 3: Model 1 plus built environment factors. This was repeated for each outcome (i.e. depressive symptoms, suicidal ideation).
Step 3: The group-based models of (i) suicidal ideation and (ii) depressive symptoms were re-estimated with risk factors, allowing for evaluation of the influence of risk factors on the probability of trajectory membership.
Results
Table 1 presents baseline (1A) sample characteristics. Participants (67% female) were 13- to 17-years-old (M = 15.7; SD = 1.04) at baseline, 18- to 23-years-old (M = 19.3; SD = 1.01) at 2A, and 23- to 30-years-old (M = 25.4; SD = 1.41) at 3A. Most (>95%) of the sample were ‘White/East and West European’ and born in the Netherlands.
Baseline characteristics of all participants and classified trajectory groups. Percentages, means and standard deviations are presented to prevent traceability of participants.
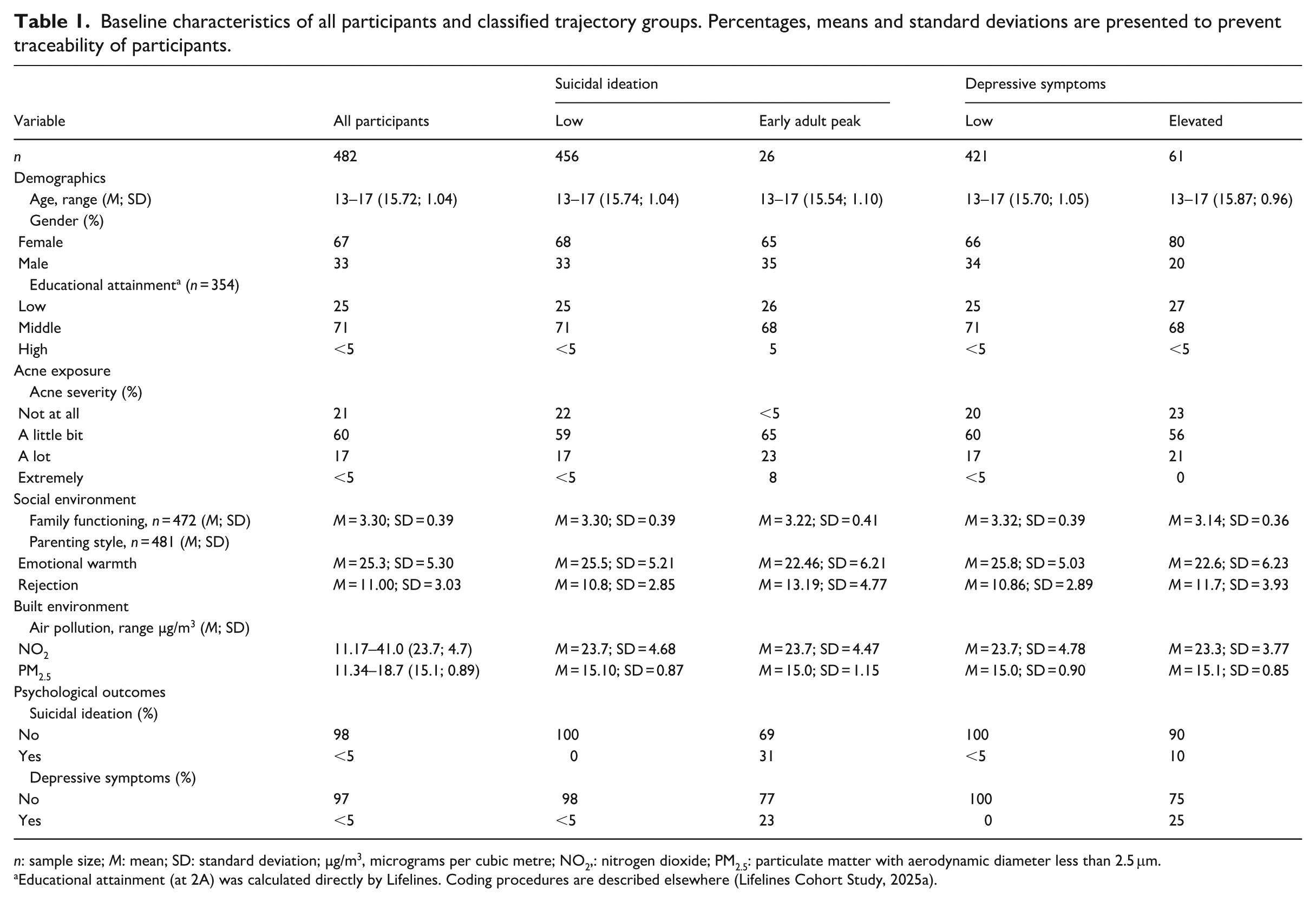
n: sample size; M: mean; SD: standard deviation; µg/m3, micrograms per cubic metre; NO2,: nitrogen dioxide; PM2.5: particulate matter with aerodynamic diameter less than 2.5 μm.
Educational attainment (at 2A) was calculated directly by Lifelines. Coding procedures are described elsewhere (Lifelines Cohort Study, 2025a).
Suicidal ideation trajectories
Multiple group-based trajectory models (two to four groups) were fitted. The two-group model showed the best-fit according to BIC, AIC and APP values. Participants exhibited two trajectories of suicidal ideation which were assigned nominal labels (Figure 2). A large majority (92%) showed consistently low suicidal ideation (‘Low’). Remaining participants (8%) showed elevated suicidal ideation, increasing into young adulthood, then returning to baseline levels (‘Early Adult Peak’).
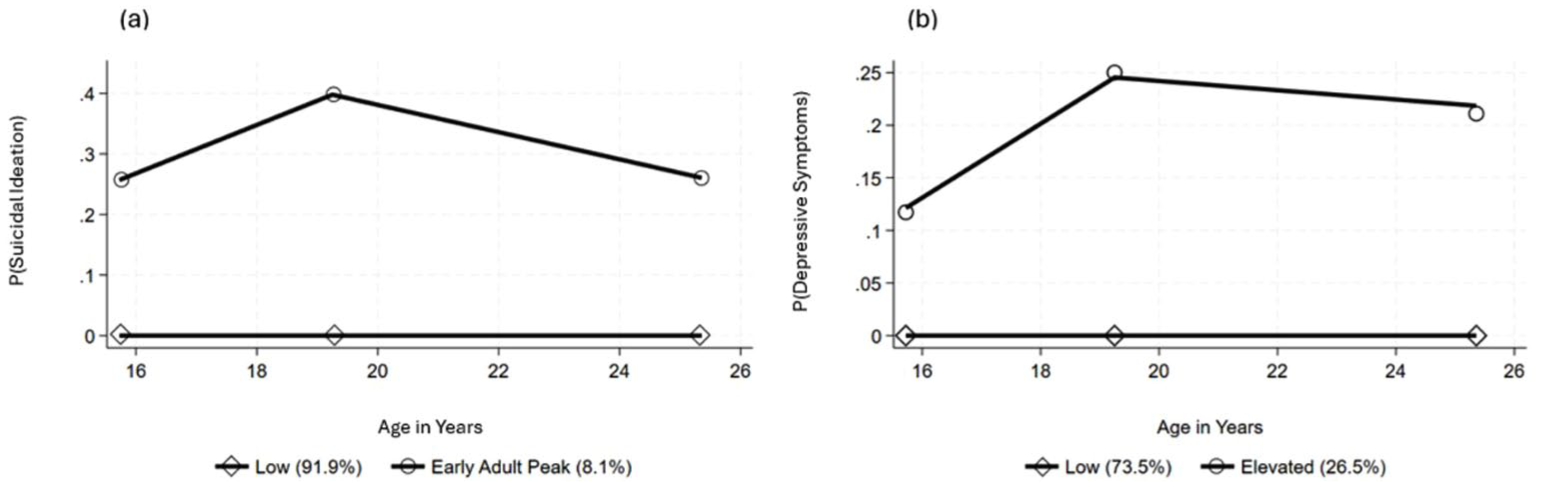
Distinctive trajectory models of (a) suicidal ideation and (b) depressive symptoms. The predicted probability of (a) suicidal ideation and (b) depressive symptoms for each trajectory group is plotted.
Depressive symptoms trajectories
Multiple group-based trajectory models (two to four groups) were. A two-group model showed the best fit according to BIC, AIC and APP values. Participants exhibited two depressive symptom trajectories which were assigned nominal labels (Figure 2). Almost three-quarters (73.5%) exhibited consistently low depressive symptoms (‘Low’). The remainder (26.5%) exhibited elevated, increasing depressive symptoms into adulthood, which subsequently reduced but did not return to baseline levels (‘Elevated’).
Factors associated with resilience: Trajectory group determinants
Suicidal ideation
Table 2 presents multivariate logistic regression analyses for suicidal ideation group membership probabilities. Acne severity increased membership probability in the ‘Early Adult Peak’ group relative to the ‘Low’ group in all models. Gender did not predict group membership in any model. Social and built environment factors did not predict group membership.
Regression estimates (odds ratios) of ‘Early Adult Peak’ suicidal ideation trajectory group relative to ‘Low’ suicidal ideation group.
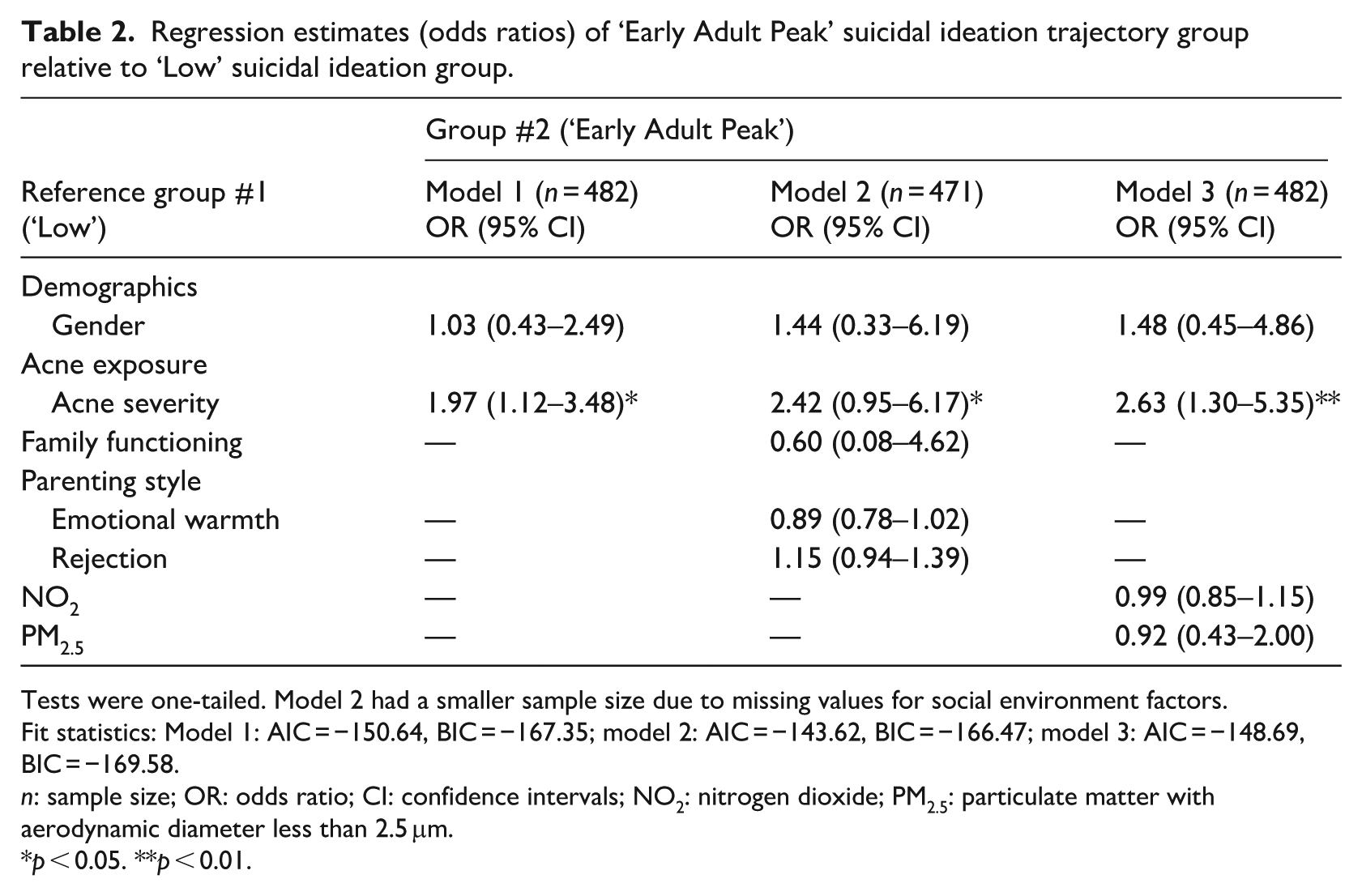
Tests were one-tailed. Model 2 had a smaller sample size due to missing values for social environment factors.
Fit statistics: Model 1: AIC = −150.64, BIC = −167.35; model 2: AIC = −143.62, BIC = −166.47; model 3: AIC = −148.69, BIC = −169.58.
n: sample size; OR: odds ratio; CI: confidence intervals; NO2: nitrogen dioxide; PM2.5: particulate matter with aerodynamic diameter less than 2.5 μm.
p < 0.05. **p < 0.01.
Depressive symptoms
Table 3 presents multivariate logistic regression analyses for depressive symptom group membership probabilities. Female gender increased membership probability in the ‘Elevated’ group relative to the ‘Low’ group in models 1 and 3, but not model 2. Acne severity did not predict group membership in any model. Social and built environment factors did not predict group membership.
Regression estimates (odds ratios) of ‘Elevated’ depressive symptom trajectory group compared to ‘Low’ depressive symptom group.
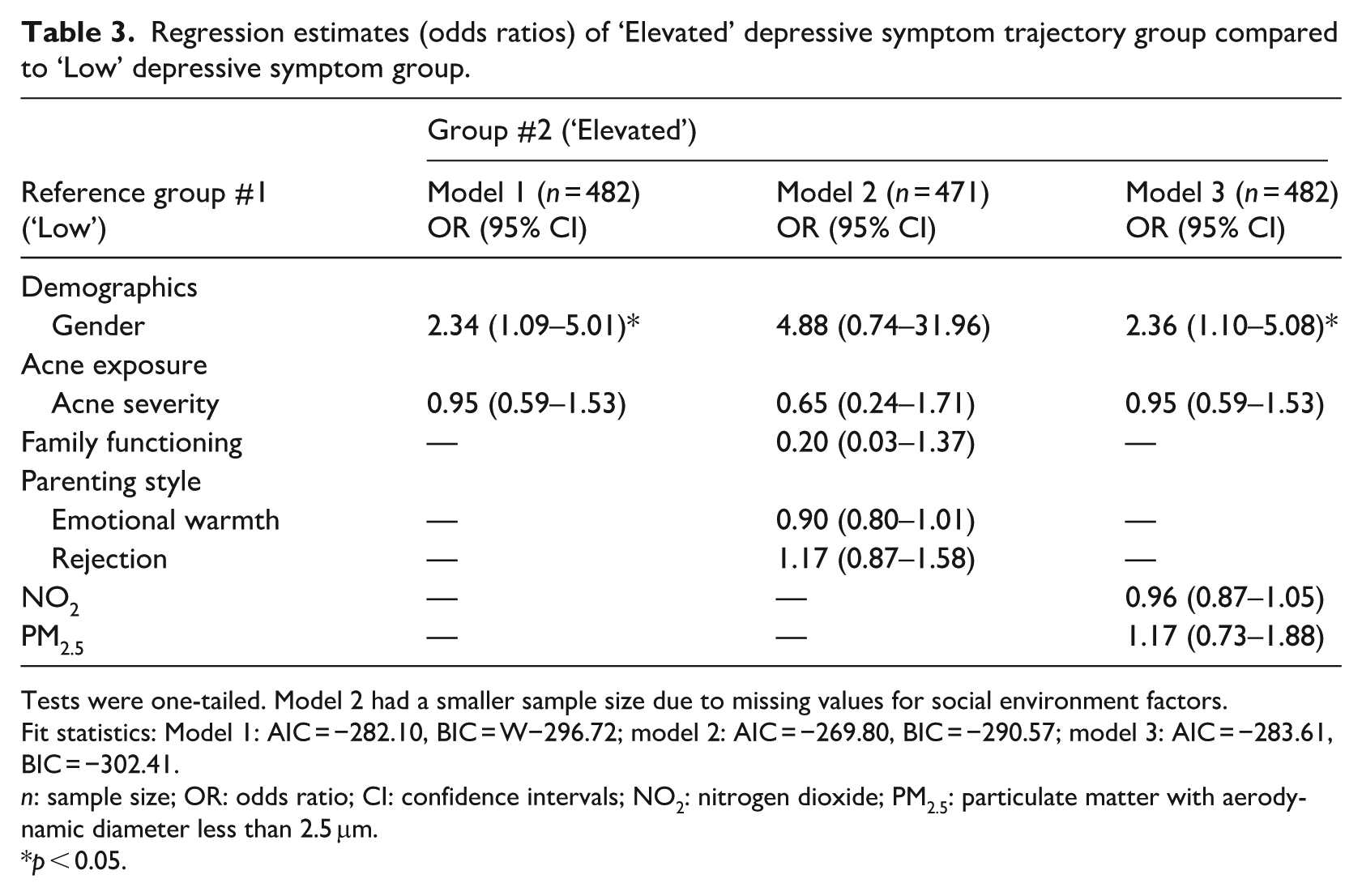
Tests were one-tailed. Model 2 had a smaller sample size due to missing values for social environment factors.
Fit statistics: Model 1: AIC = −282.10, BIC = W−296.72; model 2: AIC = −269.80, BIC = −290.57; model 3: AIC = −283.61, BIC = −302.41.
n: sample size; OR: odds ratio; CI: confidence intervals; NO2: nitrogen dioxide; PM2.5: particulate matter with aerodynamic diameter less than 2.5 μm.
p < 0.05.
Discussion
This longitudinal, population cohort study provides a novel investigation of multisystemic resilience using psychological outcomes, depressive symptoms and suicidal ideation, in the context of acne. Approximately 8% of participants displayed an increased probability of experiencing suicidal ideation. Late adolescence and early adulthood involve changes including leaving home, pursuing education, and entering the workforce. Disruption during these transitions can lead to social isolation (Eckhard, 2018) subsequently increasing suicidal ideation risk (Calati et al., 2019). The ‘Elevated’ depressive symptom trajectory group provides further evidence for psychosocial challenges during this period. Findings reinforce our knowledge that, even without acne, this transition period is associated with vulnerability regarding suicidal ideation and depressive symptoms.
Previous evidence suggests that acne exposes young people to additional adversity through physical and psychosocial difficulties (Hazarika and Archana, 2016). Increased acne severity increased membership odds in the ‘Early Adult Peak’ suicidal ideation group relative to the ‘Low’ group, aligning with evidence that suicidal ideation is reported more often by 18- to 19-year-olds with increasingly severe acne (Halvorsen et al., 2011). While many factors may contribute to associations between suicidal ideation and severe acne, we can consider that acne may affect social functioning due to its highly visible nature (Halvorsen et al., 2011) and stigmatisation (Shields et al., 2024). Acne in youth may put people at risk regarding poor self-image, bullying, stigmatisation and suicidal behaviour (Kelly et al., 2021). In the present study, acne severity did not predict membership in depressive symptom trajectories, contradicting evidence suggesting positive connections between acne severity and depressive symptoms (Lukaviciute et al., 2017). Although there was, overall, a high prevalence of any acne symptoms in our sample (80%), three-quarters of participants with acne reported mild levels, possibly suggesting that mild acne is considered a normative experience by some people during this period. Milder acne may not be a risk factor, however more severe acne exposure is. Severe acne can have painful, uncomfortable symptoms (Hazarika and Archana, 2016), challenging medical treatments including isotretinoin therapy, and increased stigma (Shields et al., 2024). Therefore, exposure to severe acne in youth creates adversity which may affect the development of certain psychological outcomes including suicidal ideation. There are, though, many protective factors at multiple system levels which are likely operating for young people who experience less severe dermatological adversity.
Accounting for acne, female gender increased membership probability in the ‘Elevated’ depressive symptom trajectory (>130% greater odds) in models 1 (acne, gender) and 3 (model 1 plus built environment factors), but not model 2 (model 1 plus social environment factors). Females may be more psychologically affected by acne than males (Tan et al., 2008) even without differences in pain and discomfort (Hassan et al., 2009). Aesthetic ideals regarding clear, blemish-free skin are held by males and females (Magin et al., 2011a), however females may feel greater social pressure to experience such ideals (Samson et al., 2010). Aligning with this notion, when accounting for factors in the social environment, female gender was no longer a risk factor. Overall, our sample demonstrated positive family functioning. Accounting for this may help young females exposed to acne to sustain psychological functioning amidst societal ideals regarding blemish-free skin. Although female gender may impede resilience and contribute to depressive symptoms, the mechanism by which this occurs is not suicidal ideation. This reinforces our rationale for modelling both psychopathological outcomes, demonstrating that identifying risk factors for one outcome does not imply they will act similarly for another related, but distinct outcome.
Although previous research suggested connections between parental rejection and suicidality (Sobrinho et al., 2016), our findings indicate that when accounting for acne exposure, people who perceive parental rejection are not necessarily more vulnerable to suicidal ideation or depressive symptoms. This finding may only be relevant to youth who experience extreme forms of parental rejection. Our sample demonstrated low parental rejection, possibly creating a social environment which enabled participants to sustain psychological functioning when exposed to acne during adolescence.
Air pollution did not predict membership in the ‘Early Adult Peak’ suicidal ideation or ‘Elevated’ depressive symptom trajectories, contradicting evidence suggesting negative relationships between NO2 and PM2.5 and mental wellbeing (Buoli et al., 2018). The air pollutant concentrations observed fell far below air quality regulations (European Union, 2015; The National Archives, 2010). We may consider that the air quality in our sample did not create an environment of risk; rather it provided resources within the built environment which facilitated the maintenance of psychological functioning in the context of acne.
In the context of mild acne exposure in youth, social environment factors related to upbringing including low parental rejection and positive family functioning, as well as built environment factors like healthy air quality, may help to sustain psychological functioning over time. Understanding how these factors operate in the context of acne exposure has important implications for the wellbeing of young people with acne.
Practical implications
This study provides a novel exploration of multisystemic resilience in people with and without acne from adolescence into adulthood. Individuals experiencing suicidal ideation may not present with clinical depressive symptoms, and those with depressive symptoms may be overlooked should they not meet diagnostic criteria. However, suicidality and depressive symptoms pose serious threats to wellbeing. Adolescents with milder acne may be better able to adapt, whereas those with more severe exposure must cope with higher risk of suicidal ideation, and greater psychosocial challenges. Mental health practitioners working with young people should be aware of skin-specific challenges that acne presents, be prepared to discuss acne and its impacts, and integrate associated challenges into care. For example, cognitive stress management techniques can improve perceived stress and negative affect in females aged 18- to 40-years-old with acne (Chatzikonstantinou et al., 2019).
Limitations and future research
The self-assessment of acne may have created reliability problems. Although evidence demonstrates correlations between self-assessed and physician-assessed acne (Magin et al., 2011b), future research would benefit from including more objective measures of acne severity (e.g. dermatologist assessment). There was an overrepresentation of participants who were female, ‘White/West and East European’ and born in the Netherlands. Future research could seek to involve a more diverse sample.
The missing data methods employed may have excluded participants who screened positively for psychopathology. However, when large amounts of data are missing, the probability of estimating missing data precisely decreases, and risks of false positive effects increase (Hardt et al., 2013). Nonetheless, findings should be interpreted with caution.
Although this study provides a multisystemic approach to resilience in the context of dermatological adversity, there were various factors which may impact the development of acne, depressive symptoms and suicidal ideation (e.g. hormone levels, nutrition, body mass index) which were not investigated in order to provide a focused study and parsimonious statistical model. Future research could explore the impacts of such factors on resilience and the development of psychological outcomes.
Footnotes
Acknowledgements
The authors wish to acknowledge the services of the Lifelines Cohort Study, the contributing research centres delivering data to Lifelines, and all the study participants.
Ethical considerations
The Lifelines study is approved by the medical ethical committee of the University Medical Center Groningen, The Netherlands, document number METC UMCG METc 2007/152.
Consent to participate
All Lifelines participants provided consent to participate.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data.
Author contributions
Conceptualisation and design of work: CF, FN; data analysis and interpretation: CF, FN, SD, MU; writing – original draft: CF, FN; writing – review and editing: CF, FN, SD, MU.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Ad Astra Fellow Studentship programme at University College Dublin. The Lifelines initiative has been made possible by subsidy from the Dutch Ministry of Health, Welfare and Sport, the Dutch Ministry of Economic Affairs, the University Medical Center Groningen (UMCG), Groningen University and the Provinces in the North of the Netherlands (Drenthe, Friesland, Groningen).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data may be obtained from a third party and are not publicly available. Researchers can apply to use the Lifelines data used in this study. More information about how to request Lifelines data and the conditions of use can be found on their website.