
Abstract
Purpose: This study aimed to examine whether the visibility of dermatological conditions differed with distinct trajectories of psychopathological symptoms before and after dermatological treatment. Methods: In total, 162 adults aged 18–35 years participated in the study. A prospective, controlled design was employed, comparing two dermatological patient groups (Group A, n = 54: visible facial acne, and Group B, n = 54: non-visible psoriasis/eczema) with a healthy control group (Group C, n = 54) across two assessment points, using a battery of questionnaires. Results: While both dermatological patient groups exhibited elevated psychopathology compared to controls at both time points, patients with visible acne demonstrated a distinct post-treatment exacerbation of specific psychopathological dimensions (Somatization, OCD, Anxiety, and Paranoid Ideation). Conclusions: Findings suggest that dermatological treatment alone may be insufficient to alleviate psychological distress, particularly when the skin condition is visibly located. Therefore, a combination of dermatological and psychological treatments is recommended.
Keywords
Introduction
The way in which the presence of psychopathology may affect how a dermatological disorder is experienced has not been adequately investigated (Jowett and Ryan, 1985; Kent, 2000). Likewise, there is a dearth of studies assessing the impact of skin conditions on the development of psychopathological symptoms. Since any skin disorder also affects an individual’s overall well-being, including their feelings, thoughts, and general behavior (Fried and Wechsler, 2006; Gupta and Gupta, 1998; Koo, 1995; Koo et al., 2000; Morrison et al., 2010), the investigation of the psychological factors implicated in the experience of living with a skin disorder becomes important both for the management and the prevention of secondary difficulties in dermatological disorders.
Research findings are contradictory regarding the severity of the skin condition and the psychopathology among dermatological patients. Few findings suggest that the emotional difficulties of dermatological patients are not always related to the clinical severity of the skin disorder (Hahm et al., 2009; Kokandi, 2010; Mulder et al., 2001; Ogedegbe and Henshaw, 2014; Schroeder et al., 2012). It was shown that young patients with severe acne manifestations appear to have high levels of emotional and behavioral difficulties in comparison with adolescents with milder acne manifestations. Other studies report that acne patients exhibit high levels of depression (Khan et al., 2001), obsessive compulsive symptoms (Yesilova et al., 2012), social phobia and anger (Rapp et al., 2004). Taken together, prior findings suggest that psychological distress in dermatological patients may arise both independently of and in interaction with clinical severity. While some studies emphasize subjective perception and psychosocial appraisal as key determinants of distress, others demonstrate that increasing dermatological severity can exacerbate specific psychopathological symptoms. These mixed findings highlight the need for designs that can disentangle severity, visibility, and temporal change.
Similarly, chronic dermatological disorders such as psoriasis or eczema can lead to increased levels of psychopathology, especially if they have an early developmental onset (Gupta et al., 1987). More specifically, it is reported that children with psoriasis or eczema are often characterized by introversion and experience mood swings (Koblenzer and Koblenzer, 1988; Williams, 1951). According to some researchers, the psychological difficulties that frequently occur in patients with psoriasis or eczema often constitute somatosensory manifestations of anxiety and depression (Laihinen, 1987; Remröd et al., 2013), hypochondriac symptoms and anger difficulties (Ginsburg and Link, 1989).
It is considered that basic dermatological care can bring out just as many positive results as the care provided by mental health professionals for patients with acne-related mental disorders, due to the resulting skin disfigurement (Capoore et al., 1998; Kish and Lansdown, 2000). Prior research in a sample of patients with signs of discomfort due to acne suggested that there was a significant improvement in their mental state, such as a decrease in anxiety and depression symptoms, when treated with dermatological medications such as erythromycin 1 and isotretinoin 2 (Marron et al., 2013; Rubinow et al., 1987). However, no similar findings have been observed by other researchers (Hull and D’Arcy, 2003; McGrath et al., 2010). For example, in a study by Kellett and Gawkrodger’s (1999), it was found that despite the significant decrease in the clinical severity of acne in their sample, no improvement in patients’ emotional state was observed. More precisely, while emotional symptom scores tended to decrease following treatment, these improvements did not reach statistical significance, suggesting that clinical improvement does not necessarily translate into meaningful psychological change (Kellett and Gawkrodger, 1999). Lastly, other researchers view patients’ psychopathological symptoms as an idiosyncratic response to the use of isotretinoin (Ng et al., 2002). Importantly, these authors do not support a general causal relationship between isotretinoin and psychopathology but rather describe rare and unpredictable adverse reactions in vulnerable individuals.
Furthermore, there is a dearth of research investigating levels of psychopathology in patients with acne, psoriasis, and eczema before and after dermatological treatment phase. This may be happening because most studies involving dermatological patients employ different experimental designs. For example, a majority of studies compare the results collected from one group of dermatological patients, before and after the completion of the dermatological treatment, in the absence of a control group (Hahm et al., 2009; Jick et al., 2000; Karadag et al., 2013; Yesilova et al., 2012); other studies might compare the results from a group of dermatological patients with a control group, at one specific period of time (Gül and Çölgeçen, 2015). Moreover, other studies compare the results from two groups of patients who share the same dermatological disorder but follow different pharmacological treatments (Bremner et al., 2005; Chia et al., 2005; Jick et al., 2000). Lastly, several studies compare different groups of dermatological disorders, without pre-interventional and post- interventional design, by excluding the use of a control group (Friedman et al., 2006; Gupta and Gupta, 1998).
Present study
Based on the literature, findings on psychopathology levels in dermatological patients are contradictory, largely due to the experimental designs of individual studies and the absence of a holistic psychopathology assessment tool. The present study addresses this gap by comparing results from two groups of dermatological patients (Group A: acne; Group B: psoriasis/eczema) with a control group (Group C) at two time points (before and after completion of the dermatological treatment). To understand the psychological problems of dermatological patients, a clinical tool that explores various aspects of psychopathology was used. The central hypothesis of the current study is that patients with severe visible facial cystic acne (Group A), as well as patients with psoriasis and eczema localized elsewhere on the body (with no visible localization; Group B), exhibit higher levels of psychopathology compared to the control group. In addition, patients with acne (Group A), whose skin condition is visible, exhibit higher levels of psychopathology at both phases of the study, before and after dermatological treatment, compared to patients with psoriasis and eczema (Group B), whose skin condition is not visible.
Methods
Study design
A 6-month longitudinal study was conducted in two cities in Cyprus (Paphos and Limassol), assessing psychopathology levels in dermatological patients at two phases: before and after dermatological treatment, compared to a control group. The first phase involved referring patients to dermatologists for their skin conditions. The second phase was conducted 6 months later, after the prescribed dermatological treatment was completed. All skin diagnoses were confirmed exclusively by dermatologists. Group A (n = 54) consisted of patients with severe facial cystic acne who were treated with oral retinoids and antibiotics. Group B (n = 54) included patients with psoriasis or eczema managed with oral corticosteroids, antibiotics, and topical therapies (creams, salicylic acid, shampoos). Group C (n = 54), the control group without skin conditions, was included to compare the distress levels of dermatological patients with those in the general population. Participants were excluded if they had medical conditions that affected their body image or appearance satisfaction, were pregnant, had physical disabilities, or faced challenges with the Greek language. Group-specific criteria included: for Group A, exclusion of individuals with additional dermatological conditions; for Group B, exclusion of those with visible skin symptoms.
Ethical considerations
The study was approved by the Cyprus National Bioethics Committee (EEBK EΠ 2015.01.103).
Study population: Recruitment and screening
Participants across all groups were recruited between February 2015 and July 2015. Participants in Groups A and B were diagnosed by their dermatologists, who informed them about the study and provided consent forms. The researcher arranged individual telephone meetings in their private office, ensuring participants understood the study’s purpose, confidentiality protocol, and the 6-month follow-up phase. Eligibility was confirmed through a brief interview assessing demographic details and skin condition characteristics, followed by participants completing the Symptom Checklist 90 Revised (SCL-90-R). Group C (the control group) was recruited through snowball sampling. The SCL-90-R was re-administered to all participants 6 months after their initial assessment. Participants were informed of their right to withdraw at any time.
Study variables: Sociodemographic questionnaire and skin disorder characteristics
A custom-designed questionnaire, administered as a brief interview, collected closed-ended information on participants’ age, gender, and educational background, as well as the onset, nature, and anatomical localization of their skin condition. Patients also confirmed impending pharmacological treatment.
Symptom checklist 90 revised (SCL-90-R)
This validated self-report instrument, an updated version of the Hopkins Symptom Checklist (Derogatis et al., 1974), assesses 10 psychopathology dimensions: somatization, obsessive-compulsive disorder, interpersonal sensitivity, depression, anxiety, anger/hostility, phobic anxiety, paranoid ideation, and psychoticism. Comprising 90 items scored on a 5-point scale (0 = not at all to 4 = extremely), the total score ranges from 0 to 360. The Global Severity Index (GSI), derived from the mean of all subscales, indicates overall psychological distress. The Greek translation, previously validated (Donias et al., 1991), was used in this study. The internal reliability of the scales ranged from 0.74 to 0.90. The SCL-90-R was administered both before and after the dermatological treatment for all groups.
Statistical analysis
To test our hypotheses, we used SPSS 22 for Windows. Specifically, the sample distribution was tested for normality using the Kolmogorov-Smirnov test (D(162) = 0.11, p > 0.05), indicating that the distribution was normal. Therefore, t-tests and ANOVA were considered appropriate for analyzing the current sample. A factorial mixed ANOVA was conducted to examine differences in psychopathology scales between the study groups, both before and after dermatological treatment. Additionally, post hoc comparisons were performed to identify specific differences in psychopathological difficulties between Group A and Group B. A Bonferroni correction with p < 0.001 was used to minimize Type I errors.
Results
Sample characteristics
The study sample comprised 162 participants, divided into three groups: patients with acne (Group A, n = 54), patients with psoriasis or eczema (Group B, n = 54), and a Control group (n = 54). Participants ranged in age from 18 to 35 years (76 males; Mage = 24.94 years). Demographic details are presented in Figure 1. No statistically significant differences in age or gender distribution were observed between the three groups.
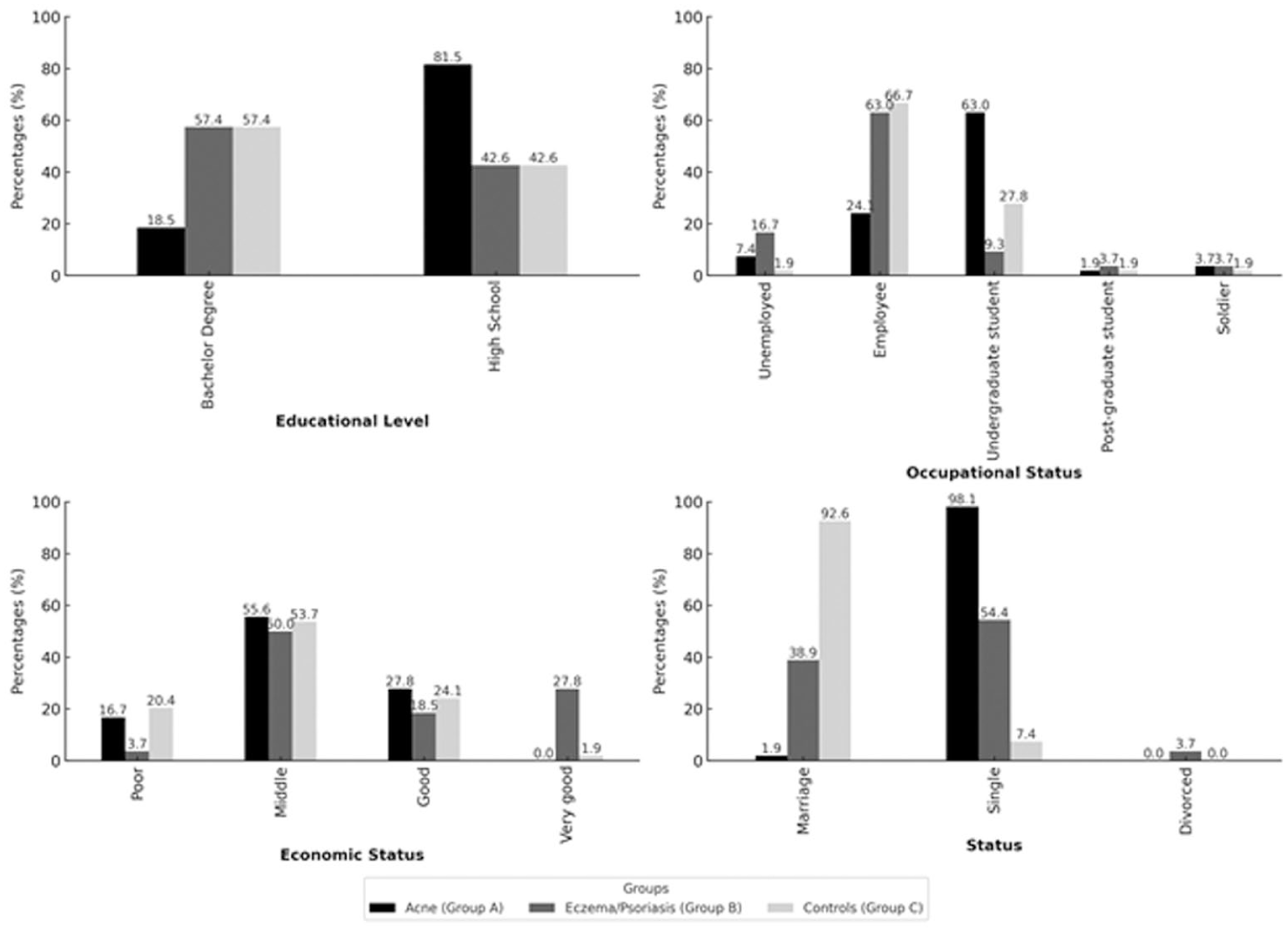
Percentages for demographic characteristics of the sample (N = 162).
Differences in psychopathology scales of the SCL-90-R questionnaire between groups, before and after dermatological treatment
Factorial Mix ANOVA measures were used, with each scale of the SCL-90-R questionnaire serving as the dependent variable (Somatization, Obsessive-Compulsive Disorder, OCD, Interpersonal Sensitivity, Depression, Anger/Hostility, Paranoid Ideation, Psychoticism, and Global Severity Index). The Time factor (before and after dermatological treatment) was used as a within-subjects factor, and the Group as a Between-subjects factor. Group × Time interaction effects were interpreted as indicating differential trajectories of psychopathological symptoms across study groups. Table 1 presents the mean values for each psychopathology scale before and after dermatological treatment.
Mean values of the psychopathology scale of SCL-90-R questionnaire before and treatment phases.
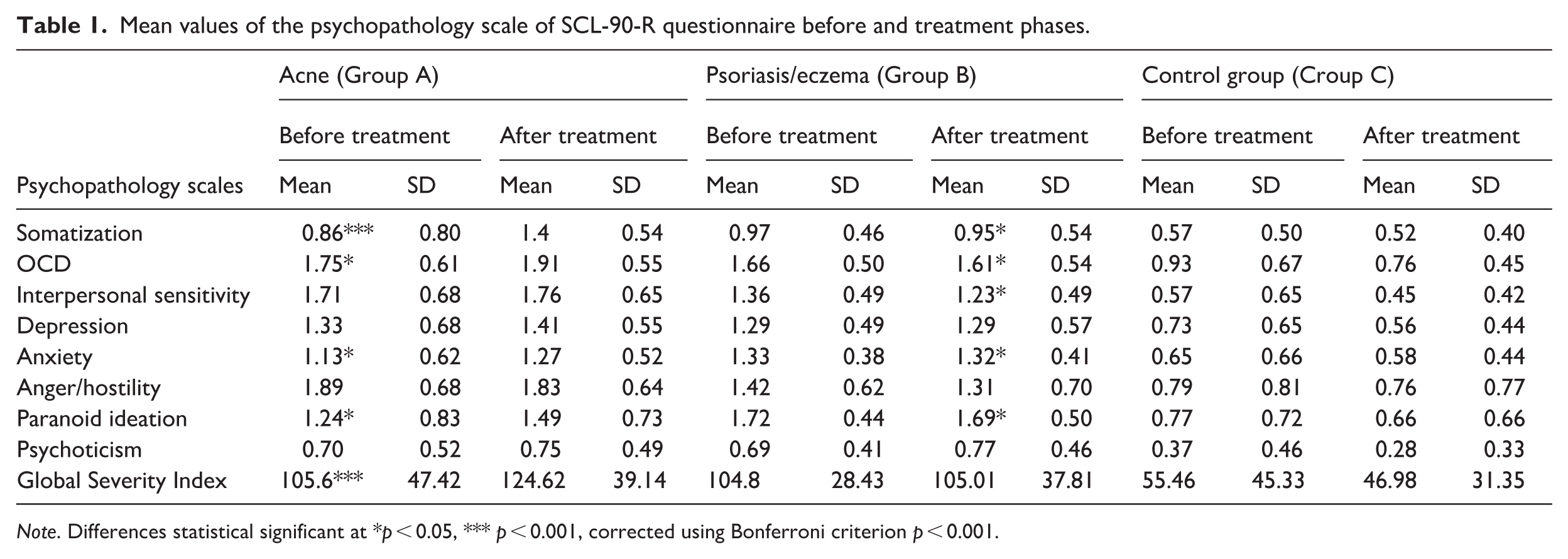
Note. Differences statistical significant at *p < 0.05, *** p < 0.001, corrected using Bonferroni criterion p < 0.001.
Differences in the somatization scale between groups, before and after dermatological treatment
Analysis revealed a significant interaction effect between Group and Time, F(2,159) = 22.12, p < 0.001, η2 = 0.22. Moreover, the dermatological patient groups displayed higher levels of somatization than the control group before and after dermatological treatment (p < 0.001). The two groups of dermatological patients had no significant differences in the pre-intervention phase. Follow-up pairwise comparisons reflected that in the Control group the level of somatization did not change significantly from the pre-treatment phase (M = 0.57, SD = 0.50) to the post treatment phase (M = 0.52, SD = 0.40), p > 0.05. However, for Group A the levels of somatization were significantly increased before (M = 0.86, SD = 0.80), p = < 0.001, and after treatment (M = 1.40, SD = 0.54), p < 0.001 (see Figure 2). This pattern indicates a post-treatment escalation of somatic symptom reporting among acne patients.
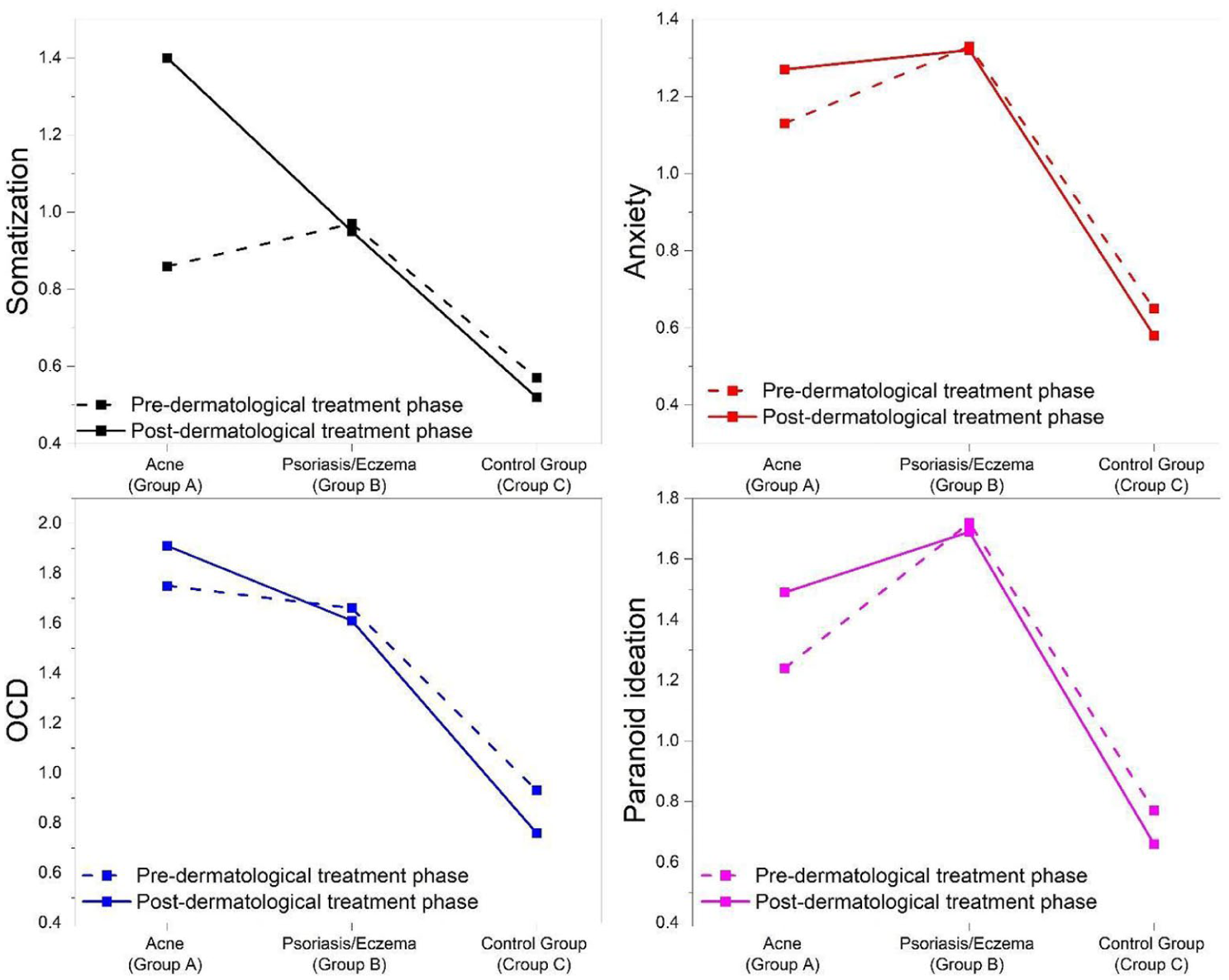
Changes in the somatization, OCD, anxiety, and paranoid ideation scales among the groups, before and after treatment.
Differences in the obsessive-compulsive scale between groups, before and after dermatological treatment
Analysis revealed a significant interaction effect between Group and Time, F(2,159) = 6.57, p < 0.002, η2 = 0.76. Furthermore, it was found that the groups of dermatological patients appeared to have higher obsessive-compulsive levels compared to the control group, at both prior to and post- dermatological treatment phases (p < 0.05), whilst the two groups did not differ significantly at the before treatment phase. Obsessive compulsive symptomatology showed persistence and amplification over time in the acne group, before (M = 1.75, SD = 0.61), p < 0.001, and after treatment (M = 1.91, SD = 0.55), p < 0.001 (see Figure 2).
Differences in the anxiety scale between groups, before and after dermatological treatment
Results showed a significant interaction between Group and Time, F(2,159) = 5.51, p < 0.05, η2 = 0.065. Furthermore, it was observed that the groups of dermatological patients had higher anxiety levels compared to the control group, before and after dermatological treatment (p < 0.001). Anxiety levels increased over time exclusively in the acne group, prior to (M = 1.13, SD = 0.62), p = < 0.05, to post-treatment phase (M = 1.27, SD = 0.52, p < 0.05 (see Figure 2).
Differences in the paranoid ideation scale between groups, before and after dermatological treatment
Findings indicated a significant interaction effect between Group and Time, F(2,159) = 5.93, p < 0.003, η2 = 0.069. Moreover, the two groups of dermatological patients appeared to have higher levels of paranoid ideation compared to the control group, both at the prior to and post- dermatological treatment phase (p < 0.000). More specifically, the levels of paranoid ideation of patients with acne were significantly increased from prior to (M = 1.24, SD = 0.83), p = < 0.05, to post treatment phase (M = 1.49, SD = 0.73), p = < 0.05 (see Figure 2). This increase suggests heightened suspiciousness over time among acne patients.
Differences in the Global Severity Index scale between groups, before and after dermatological treatment
There was a significant interaction effect between Group and Time, F(2,159) = 10.32, p < 0.001, η2 = 0.12. Specifically, the groups of dermatological patients exhibited higher scores on the Global Severity Index scale, compared to the control group, at both the pre- and post-dermatological treatment phases (p < 0.000). However, for Group A, the scores on the Global Severity Index were increased considerably from prior to (M = 105.59, SD = 47.42), p = < 0.001, to post-treatment phase (M = 124.62, SD = 39.14), p = < 0.001. This indicates an overall worsening of psychological distress in the acne group following treatment.
In addition, for the other scales of the SCL-90-R questionnaire: interpersonal sensitivity (p = 0.08), anger/hostility (p = 0.56), depression (p = 0.35), and psychoticism (p = 0.07), there was no statistical main effect of Time, neither interaction between Time and Group.
Discussion
The present study is among the first to compare psychopathology levels across two groups of dermatological patients, those with acne and those with psoriasis/eczema, compared to a control group, both before and after receiving pharmacological treatment for their dermatological conditions. Previous research with longitudinal designs has generally focused on a single dermatological condition (e.g. Hahm et al., 2009; Jick et al., 2000; Karadag et al., 2013; Marron et al., 2013; Ng et al., 2002; Yesilova et al., 2012), thereby limiting understanding of differences between visible dermatological disorders (e.g. acne) and concealable dermatological disorders (e.g. psoriasis/eczema). By directly comparing visible and non-visible dermatological conditions within the same longitudinal framework, the present study allows for a more nuanced examination of how visibility, in addition to disease presence, may shape psychopathological trajectories over time.
Our findings demonstrate that dermatological patients exhibit significantly higher levels of psychopathology than healthy controls, both before and following treatment. Specifically, dermatological patients reported elevated levels of somatization, obsessive–compulsive symptoms, anxiety, paranoid ideation, and overall psychological distress, as measured by the Global Severity Index. These findings are consistent with the broader psychodermatology literature suggesting that dermatological disorders constitute a chronic psychological stressor, irrespective of clinical improvement.
Furthermore, patients with acne, a visible dermatological condition, showed higher levels of various psychopathology symptoms compared to patients with eczema or psoriasis. Our findings underscore the substantial negative impact of dermatological disorders on mental health, particularly for patients with visible conditions like acne, which appears to heighten the risk of psychopathology. This study not only highlights the coexistence of diverse psychopathological symptoms with skin disorders but also elucidates differences between visible and concealable dermatological conditions, compared to a control group. Visibility may therefore act as a psychosocial amplifier of distress, intensifying self-monitoring, perceived social evaluation, and emotional reactivity. This is consistent with prior research (Frances, 2004; Kent, 2000; Kish and Lansdown, 2000; Macgregor, 1990; Sreedhar, 2009), the visible anatomical localization of skin disorders (e.g. the face) emerges as a risk factor for psychopathological manifestations. Further research is warranted to identify specific risk factors contributing to certain psychopathology symptoms in dermatological patients.
The current findings indicate that dermatological treatment has variable effects on psychological symptoms. This post-treatment exacerbation suggests that clinical improvement of the skin condition does not necessarily translate into psychological relief and may, in some cases, coincide with heightened psychological vulnerability. This worsening among acne patients might be connected to isotretinoin treatment, which has been linked to emotional instability in vulnerable individuals and heightened physical discomfort (Bremner et al., 2005; Mufaddel et al., 2017; Wysowski and Swartz, 2005). However, existing evidence does not support a general causal relationship between isotretinoin and psychopathology, suggesting that adverse psychological reactions may be rare, idiosyncratic, and contingent on individual vulnerability. Additionally, increased physical discomfort can reinforce patients’ preoccupation with their body and the skin, which in turn results in improved patients’ anxiety and rumination, and makes them more self-conscious and susceptible to developing a distorted body image. Such processes may be particularly pronounced in facial acne, where visibility intensifies social self-awareness and perceived scrutiny.
Another factor that seems to contribute to the continued heightened psychopathology levels even in post-treatment phase for patients with acne, is the visible localization of their skin condition (i.e. the face), as well as the high levels of shame, embarrassment, humiliation, and anger, which are often reported by patients as experiences during their social exposure (Babayan et al., 2008; Chernyshov, 2016; Ersin Aydin et al., 2017; Ginsburg and Link, 1989; Rapp et al., 2004; van Cranenburgh et al., 2013; Vardy et al., 2002). Recent evidence further suggests that stigmatization plays a central role in mediating the relationship between visible skin conditions and psychological distress, with higher perceived stigma associated with increased anxiety, depression, and reduced quality of life (Tunca et al., 2025). The exacerbation of psychopathological symptoms observed among acne patients may be more strongly driven by visibility-related psychosocial mechanisms. Facial acne increases social salience and exposure to stigmatization, shame, and negative self-evaluation (Tunca et al., 2025). These results underscore the importance of close collaboration between dermatologists and mental health professionals, including routine psychological screening and the provision of accessible, supportive interventions for patients with acne, particularly those undergoing isotretinoin therapy.
Moreover, it is evident that the difficulties faced by patients with psoriasis and eczema are related to inflammation and the immune system. Chronic inflammatory processes and immune dysregulation characteristics have been linked to sustained activation of pro-inflammatory cytokines, which are increasingly associated with psychological distress. These mechanisms may contribute to the persistence of elevated psychopathology scores even after dermatological improvement (Dhabale and Nagpure, 2022).
Our study extends the findings of Gül and Çölgeçen (2015) and Gupta and Gupta (1998) by confirming persistent elevations in Global Severity Index (GSI) scores, somatization, depression, and anxiety in dermatological patients at post-treatment phase, showing that undergoing dermatological treatment does not protect against experiencing mental distress associated with the skin condition. Present findings further suggest that psychological distress may persist even in the absence of ongoing dermatological severity. Also, our study identifies additional psychopathological symptoms (e.g. obsessive-compulsive disorder and paranoid ideation) which were not assessed previously.
Moreover, our study corroborates the findings of Karadag et al. (2013), confirming increased OCD and anxiety symptoms in acne patients following completion of isotretinoin treatment. The existing results further suggest that isotretinoin may not only fail to reduce pre-existing psychopathological symptoms but may also exacerbate anxiety and obsessive–compulsive symptomatology after treatment. These findings highlight the need for careful psychological monitoring rather than assumptions of mental health improvement following dermatological treatment.
In contrast to some studies reporting a reduction in depressive symptoms following isotretinoin treatment (Hahm et al., 2009; Jick et al., 2000), the present research observed no significant improvement in depressive symptoms, alongside elevated anxiety and obsessive–compulsive symptoms in acne patients. Methodological differences, including the inclusion of a second dermatological group and a healthy control group, may partly account for these discrepancies.
Taken together, these findings indicate that dermatological patients exhibit higher levels of psychopathology compared to healthy controls, underscoring the adverse psychological burden of skin disorders. Moreover, the observation that acne patients (whose condition is prominently localized on the face) present with higher psychopathology levels than patients with psoriasis/eczema suggests that the visible anatomical localization of dermatological disorders may further aggravate psychological distress and hinder adaptation. Visibility thus emerges as a key variable shaping psychopathological outcomes in dermatological populations.
Limitations and strengths
The findings of the present study should be interpreted in light of certain limitations. First, the sample size was relatively small, limiting the generalization of the findings. Second, psychopathology was assessed exclusively through self-report measures, which may be influenced by response bias or social desirability. Third, the study did not include clinical interviews to confirm psychiatric diagnoses. Despite these limitations, the study has several strengths, including its prospective design, the inclusion of both visible and non-visible dermatological conditions, and the use of a healthy control group, which allowed for meaningful comparative analyses across groups and time.
Clinical implications and future research directions
The findings of this study highlight the importance of addressing psychological factors in dermatological care. Given the persistence and, in some cases, worsening of psychopathological symptoms following dermatological treatment, particularly among patients with acne, there is a clear need for early identification of psychological distress. Routine psychological screening within dermatology settings may facilitate timely referral to mental health services, especially for patients with visible conditions who appear particularly vulnerable to post-treatment psychological deterioration.
Moreover, dermatologists should be aware that improvement in skin symptoms does not necessarily correspond to improvement in mental health, and that patients may require additional psychosocial support even after successful dermatological treatment. Interventions targeting stigma, body image disturbance, and maladaptive cognitive patterns may be especially beneficial for patients with facial acne.
Future research should employ larger samples and include multiple follow-up assessments to better capture the trajectory of psychological symptoms over time. Additionally, future studies should consider incorporating biological markers of inflammation and immune activity to further elucidate the mechanisms linking dermatological conditions and psychopathology. Integrating psychoneuroimmunological measures may help clarify whether persistent psychological distress in psoriasis and eczema is partly mediated by chronic inflammatory processes.
Conclusion
The present study provides evidence that dermatological conditions are associated with elevated levels of psychopathology both before and after treatment. Importantly, the visibility of the skin disorder appears to play a critical role in shaping psychological outcomes, with patients with acne exhibiting greater post-treatment psychological vulnerability compared to patients with psoriasis or eczema. These findings highlight the need for integrated dermatological and psychological care models that address both the physical and emotional dimensions of skin disease.
Footnotes
Acknowledgements
We express our gratitude to the participants for their time and valuable contributions. We also acknowledge the dermatologists for their assistance in facilitating participant recruitment.
Ethical considerations
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Cyprus National Bioethics Committee (EEBK EΠ 2015.01.103, approved on 10 December 2015). Ethical approval was received in order to conduct the study.
Consent to participate
For inclusion of each participant in this study, a written informed consent was obtained.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data
Author contributions
Study conceptualization—C.C.; design and protocol development—C.C.; data collection—C.C.; data analysis—C.C. and M.P.; writing the manuscript—C.C. and M.P.; proofreading—C.C. and M.P. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Our research data are available upon request.