
Abstract
Introduction
A validated psychosocial self-screening tool, MyHEARTSMAP, was used to screen hospitalized children, who often experience disproportionate mental health burdens. The primary objective compared the proportion of participants receiving psychosocial intervention between those with and without MyHEARTSMAP screening. Secondarily, we explored the utilization of resources at 3 months post-discharge.
Methods
This randomized control trial was conducted in an emergency department, enrolling 289 children being admitted. The intervention group completed MyHEARTSMAP, and results were shared with clinicians. The control group received standard care and completed MyHEARTSMAP following discharge. Health records were reviewed to document in-hospital management. Descriptive statistics and logistic regression modeling were used to evaluate the association between screening and intervention.
Results
Psychosocial intervention rates were higher in the intervention group (40.4%) than the control (32.9%), though this was not significant (RR = 1.28, 95% CI [0.95, 1.73], p = .109). Among those with positive screening results, the intervention group had a statistically significant higher proportion of psychosocial intervention (41.3%) than the control (25.1%) (RR = 1.60, 95% CI [1.04, 2.46], p = .0318). At 3 months post-discharge, engagement with recommended services was overall modest.
Conclusions
Universal screening can identify youth at higher risk of psychosocial burden, and MyHEARTSMAP shows promise as a low-barrier tool for addressing the psychosocial needs of children.
Plain Language Summary
Introduction
Youth mental health concerns impact everyday function, including the ability to meet milestones, form relationships, and participate in school and community activities (Bardach et al., 2014). There is a disproportionate burden of comorbid mental health concerns among hospitalized youth or those experiencing acute or chronic illness. In a large retrospective study on pediatric hospitalizations, 13.2% of admitted youth experienced a psychiatric comorbidity, which was associated with increased length of stay and hospital costs (Canada, 2015; Doupnik et al., 2016; Kang et al., 2019; Knight et al., 2014). In those with chronic health conditions, the prevalence of psychiatric disorders is greater than in the general pediatric population (Hysing et al., 2007), and up to 26% of youth hospitalized for a non-psychiatric concern have received a diagnosis for a condition affecting their emotional or behavioral health (Doupnik et al., 2017). It is important to ensure optimal health outcomes by addressing both psychiatric and medical concerns (Shafran et al., 2017).
The need for standardized universal mental health screening in hospitalized pediatric populations is widely recognized as a critical need (Garcia et al., 2018). Without routine screening, psychosocial concerns may go undetected, potentially delaying intervention and compromising care. While clinical teams are encouraged to routinely screen for mental health concerns as part of regular care for admitted patients (Suryavanshi, 2016), there is a lack of comprehensive, resource-efficient screening tools. Current tools may include family/social histories and psychosocial screening interview instruments such as H.E.A.D.S.S. (Cohen et al., 1991). However, these do not alleviate prevalent screening barriers as they necessitate personnel involvement (Waller et al., 2023), are overly time-consuming (Kazak et al., 2017), and demand resources. While instruments like the PROMIS-25/PROMIS Parent Proxy or myAssessment (Barrera et al., 2018; Bradford & Rickwood, 2015; Irwin et al., 2012) do not require personnel for assessment, they do not provide psychosocial resource recommendations for disposition planning or youth access. The absence of a systematic and resource-efficient psychosocial screening approach, coupled with reduced screening amongst youth with higher medical needs may result in certain pediatric populations falling through gaps of care.
MyHEARTSMAP is a validated psychosocial self-screening tool designed to address the screening needs of pediatric patients (Doan et al., 2020; Li et al., 2021; Virk et al., 2019). Adapted from the HEARTSMAP emergency clinician assessment (Virk et al., 2018), this tool allows children and their parents/guardians to self- and proxy-report across multiple domains of mental health. Unique to MyHEARTSMAP is the comprehensive analysis of 10 areas of wellbeing: Home, Education and activities, Alcohol and drugs, Relationships and bullying, Thoughts and anxiety, Safety and Sexual health, Mood, Abuse, and Professional resources. Using an electronic device, users answer questions encompassing these areas and select statements scored from 0 for ‘no concern’ to 3 for ‘severe concern’. Scores from each section are mapped to 1 of 4 domains: Psychiatry, Function, Social, and Youth Health. Upon completion, it produces personalized recommendations for local resources to address each concern depending on their reported severity and acuity.
This randomized trial evaluates whether universal psychosocial screening via MyHEARTSMAP influences the proportion of youth receiving psychosocial intervention during their inpatient stay and upon discharge.
Methods
Study Setting and Population
This study was conducted at a tertiary care site, where recruitment occurred in the ED from August 2021 to May 2023. We enrolled children and youth aged 7–17 years old that were local residents and admitted after ED assessment to the inpatient service of general pediatrics, cardiology, nephrology, neurology, endocrinology, gastroenterology, urology, or orthopaedic surgery. We excluded those requiring sustained critical care, presenting with primary mental health concerns, without the capacity to assent or consent, previously enrolled, or without internet access (to complete subsequent surveys). Interpreters were available to accommodate families with language barriers.
Study Design
This prospective two-arm, non-blinded randomized controlled trial evaluated the impact of psychosocial screening using the MyHEARTSMAP tool, on the proportion of those who received intervention over the hospitalization. At 3 months post-discharge, participating families completed a follow-up survey to explore their access of mental health resources. The research ethics board granted study approval (H21-01221). Informed consent was obtained from all participants. This study was published on ClinicalTrials.gov (NCT06553521).
Demographics and Randomization
We collected demographic variables, admitting diagnoses, and past medical history. Ethnicity and gender were self-reported and collected to assess for balanced randomization. Participants were randomized to the intervention or standard of care arm using REDCap (Harris et al., 2009, 2019), with an allocation ratio of 1:1. Randomization was stratified by admitting inpatient services.
Intervention Arm
Participants accessed the MyHEARTSMAP tool on a device and received the treating team’s standard psychosocial assessment. These assessments vary depending on the practice of the admitting care team, but can include evaluation of emotional well-being, coping strategies, and social supports. Participants aged 7 to 9.9 years old required parent/guardian proxy-report. Participants 10 years old and older were eligible for self-report and/or parent proxy-report. Upon completing MyHEARTSMAP, a report containing domain severity scores and personalized recommendations was generated. Reports were printed for the patient chart to be used by the treating team and provided to the families for discussion. The clinical team was informed of the report’s confidentiality and whether it was completed by the youth or parent. For youth self-reports, parents were not present unless the youth consented to their involvement. This confidentiality protocol was clearly communicated to all participating services and clinicians. If participant responses indicated acute safety concerns, providers from the treating team were notified immediately to verify the acuity and severity. Mental health management was incorporated into the care plan per their judgment.
Standard of Care Arm
Participants received only the treating team’s standard psychosocial assessment, if existent. Participants received the MyHEARTSMAP tool via email after discharge. Participant responses that indicated severe or acute safety issues were directed by the tool to crisis lines and EDs for urgent help. Automatic alerts were triggered for the research team and participants were contacted to ensure access the recommended emergency services. A physician investigator was available for further guidance and clinical consultation. If imminent threats to safety were perceived and inadequately addressed in consultation with the principal investigator, research team members would contact pertinent authorities as required.
Data Collection
Upon discharge, health records were reviewed to document if psychosocial support was requested or received. This included consultation of mental health services from psychiatry, clinical psychology, social work, or adolescent medicine. Consultation of other allied mental health services was captured separately (e.g. child life specialists). Data collection occurred through: (1) Chart review of psychosocial interventions and discharge plans; (2) Communication with families to inquire if specialists were consulted for mental health concerns or resources were discussed during discharge planning; (3) Communication with treating teams to ascertain whether any additional resources were discussed.
Parents/guardians were contacted by email at 3 months to complete a follow-up survey indicating their utilization of mental health services outlined in the disposition plan. Survey items consisted of closed-ended yes/no questions and free text responses for perceived barriers to care.
Outcome Measures
The primary outcome was measured by the proportion of participants who received mental health resources or consultation from psychiatry, clinical psychology, social work, adolescent medicine, or other allied mental health services during their in-patient stay or upon discharge planning. Secondary outcomes included the utilization and perception of recommended psychosocial resources or therapeutics by patients at 3 months post-discharge.
Sample Size
In previous studies, approximately 40% of youth who presented to the ED screened positive in at least one domain of HEARTSMAP with specific follow-up recommendations (Doan et al., 2020). We assumed that at least 80% of these would receive recommended services within their hospital stay or referrals at the time of discharge, or 30% of all participants randomized to screening with MyHEARTSMAP. To achieve a power of 80% at a significance level of 0.05 and detect an absolute difference of 15% (or relative difference of 50%) in the proportion of youth who received psychosocial interventions between study arms, we targeted 135 participants per arm.
Statistical Analysis
We used descriptive statistics to summarize patients by treatment arm and ordinal logistic regression models to assess the prevalence of psychosocial issues between study arms with the expectation that rates would be similar between arms (as this was a baseline measure).
Logistic regression modeling evaluated the effect of screening on receiving psychosocial interventions as part of their in-patient care or discharge planning, adjusted for age, sex, and current general and mental health status. We reported marginal risk ratios and differences, and corresponding 95% confidence intervals with standard errors estimated by the delta-method (Naimi & Whitcomb, 2020). Effect modification of the intervention was assessed by type of admission specialty and illness chronicity by including interactions within the treatment arm in our logistic regression models. The primary analysis was repeated in the subgroup that screened positive for any psychiatric, social, youth health, function, or abuse concern identified by MyHEARTSMAP. As child life services provide both procedural support and psychosocial intervention, we conducted sensitivity analyses that excluded child-life intervention unrelated to mental health concerns and all child-life specialist intervention.
We used descriptive statistics to summarize 3-month outcomes with mental health support service recommendations and perceived barriers of accessing mental health services by patients lacking support. All analyses were conducted using R statistical software version 4.0.4.
Results
Between August 2021 to May 2023, 3,131 patients being considered for admission were screened and 2,429 of those patients were excluded for not meeting the inclusion criteria or meeting the exclusion criteria. Of the remaining 702 patients eligible for recruitment, 289 were consented and randomized: 145 to the standard of care arm and 144 to the MyHEARTSMAP intervention arm. The final analysis population included 143 patients in the standard of care arm and 141 in the intervention arm (Figure 1). CONSORT diagram.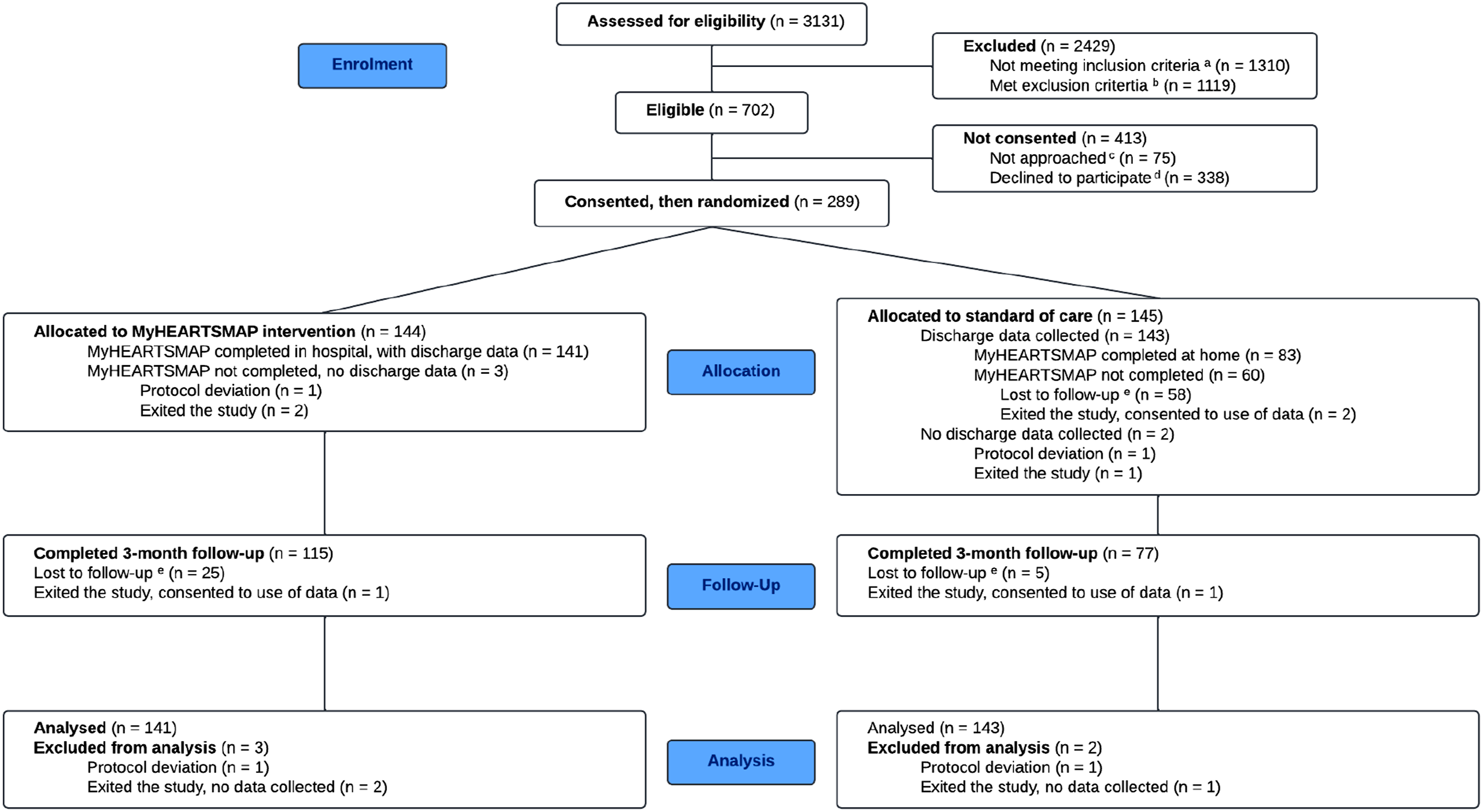
Demographic and Clinical Characteristics of Enrolled Youth by Trial Arm
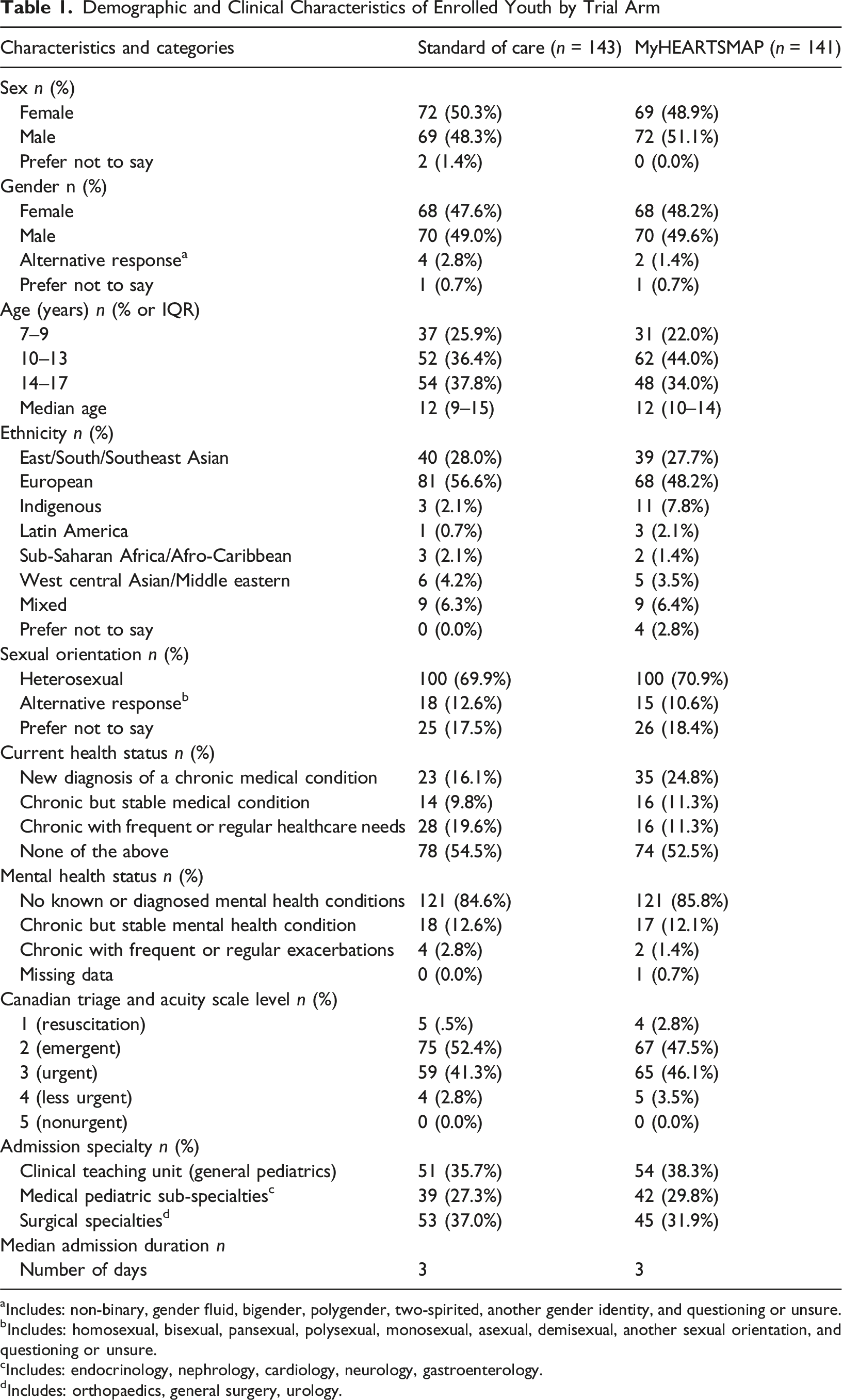
aIncludes: non-binary, gender fluid, bigender, polygender, two-spirited, another gender identity, and questioning or unsure.
bIncludes: homosexual, bisexual, pansexual, polysexual, monosexual, asexual, demisexual, another sexual orientation, and questioning or unsure.
cIncludes: endocrinology, nephrology, cardiology, neurology, gastroenterology.
dIncludes: orthopaedics, general surgery, urology.
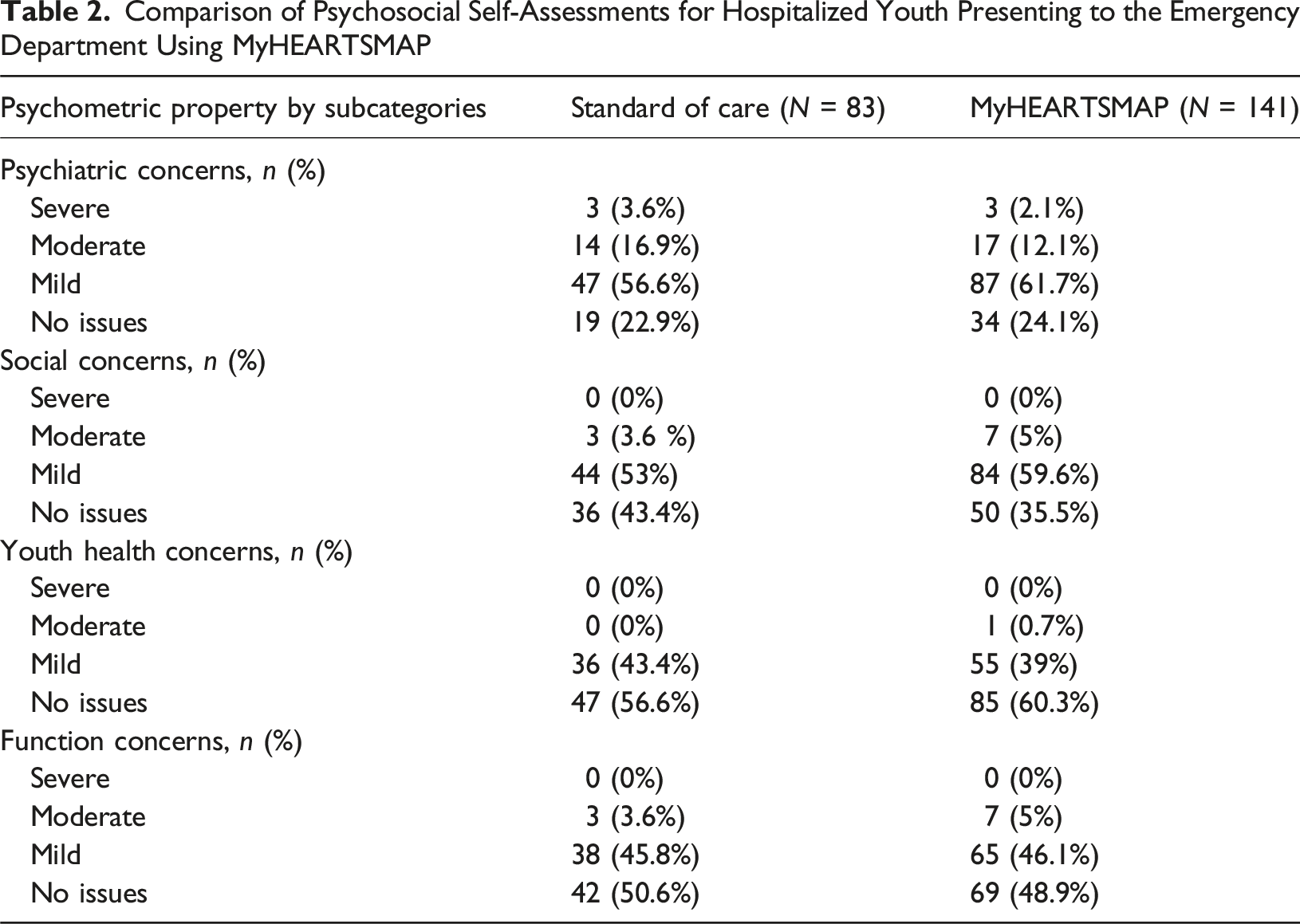
Comparison of Psychosocial Self-Assessments for Hospitalized Youth Presenting to the Emergency Department Using MyHEARTSMAP
Proportion of Patients Receiving Psychosocial Intervention Over the In-Patient Stay by Category Type
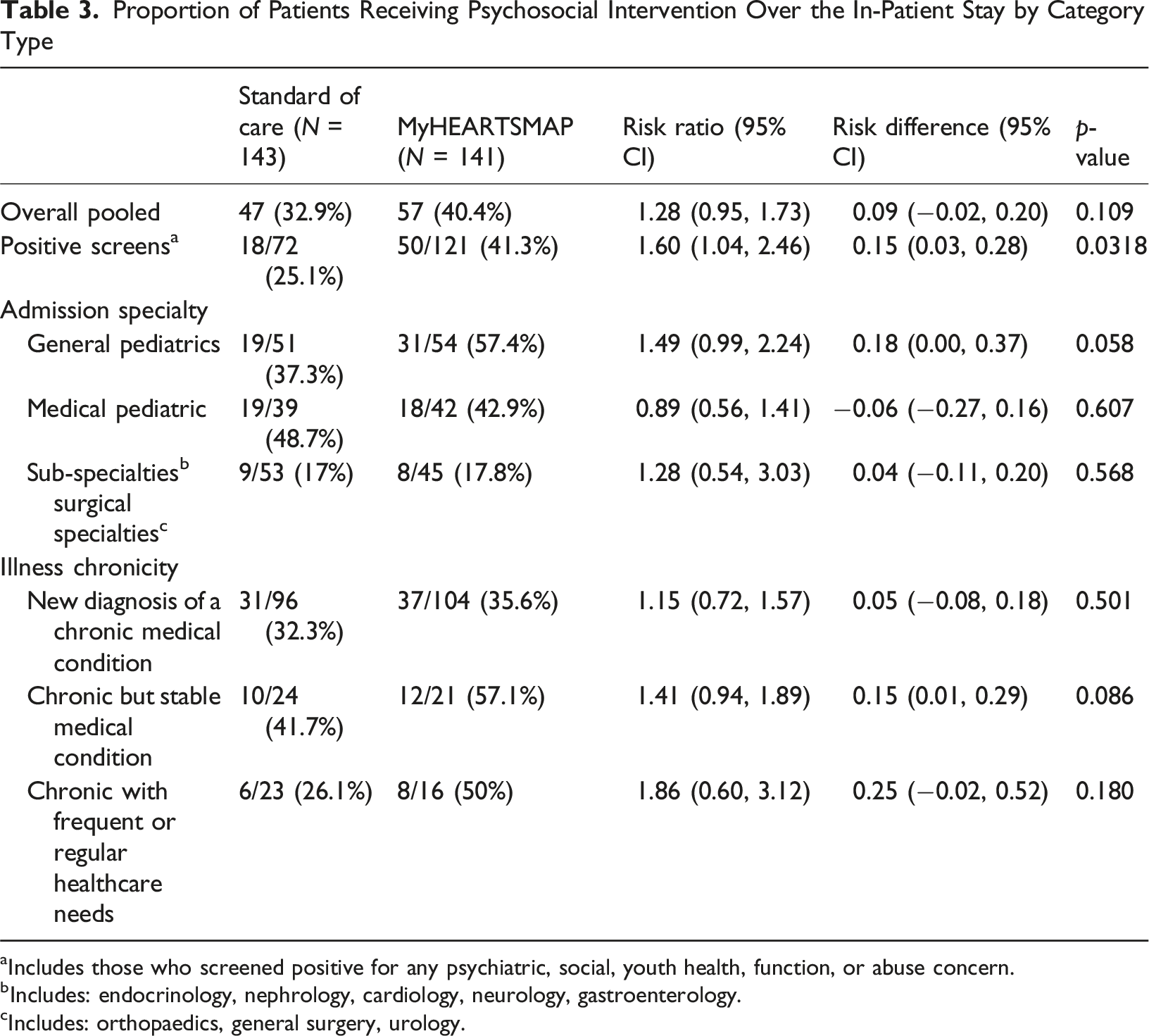
aIncludes those who screened positive for any psychiatric, social, youth health, function, or abuse concern.
bIncludes: endocrinology, nephrology, cardiology, neurology, gastroenterology.
cIncludes: orthopaedics, general surgery, urology.
At the 3-month follow-up, 192/224 participants (85.7%) completed the follow-up survey with comparable completion rates between study arms for recall of recommended services, agreement with screening results, and follow-through with recommendations (Figure 2). In addition to those introduced to psychosocial resources during their hospitalization, 9.4% (18/192) of those with service recommendations engaged with these resources after discharge, and 13.0% (25/192) involved their family physician or pediatrician. (Figure 2). Barriers to accessing mental health support included financial burden, lack of transportation, waitlist times, personal availability, and lack of knowledge in accessing these services (Table S3). 3-Month referral outcome comparison between study group participants with MH support service recommendations
Discussion
Our study assessed the association between psychosocial screening upon admission with MyHEARTSMAP and the proportion of those who received psychosocial intervention during hospitalization and discharge planning. While receiving mental health screening upon admission was not significantly associated with increased psychosocial intervention when assessing the overall pooled sample of participants, the intervention group had a significantly higher rate of psychosocial intervention compared to the control group when limiting the analyses to only those who screened positive for any psychosocial concern. At 3 months post-discharge, we observed comparable recall rates for recommended psychosocial services between study groups, with modest engagement with mental health services or involvement of primary care providers. Cited barriers to accessing mental health services included financial constraints, transportation, wait times, patient availability, and limited resource knowledge.
Over 76% of youth in our sample reported psychosocial concerns, emphasizing the importance of universal screening as part of the admission process. Knight et al. (2014) also reported a large proportion of those who screen positive for mental health concerns in hospital settings have never been previously identified. In DeVylder et al.’s (2019) study comparing universal screening to selective screening for suicidal risk, patient benefit from risk detection was greater if universal screening was applied. Screening irrespective of the specificity resulted in improved risk detection compared to the standard of care, underscoring the importance of universal screening regardless of presenting chief complaint.
Youth with chronic illnesses are at risk for under-screening of mental health concerns and have a higher incidence of anxiety and depression (Orth & van Wyk, 2021; Santos et al., 2015). Universal psychosocial screening is essential to address the needs of these populations. In a randomized control trial by Barrera et al. (2020), the effect of psychosocial screening on caregivers’ mental health in pediatric cancer was investigated. In their study, both arms completed a psychosocial assessment at time of diagnosis and 6 months later, but only the intervention arm had their screening information provided to treating teams (Barrera et al., 2020). At 6 months, there was no significant difference in outcomes when assessing the pooled sample of depression and anxiety symptoms. However, when considering the intervention effect relative to psychosocial risk, caregivers in the “high-risk” subgroup in the intervention group had significantly lower depression scores than “high-risk” controls at 6 months (Ms 6.68 vs. 9.76). Similar trends were seen with anxiety scores between the intervention and control (Ms 9.36 vs. 11.34) (Barrera et al., 2020). Our study observed possible increased benefit of intervention in those at higher risk for psychosocial ailments, such as children with stable chronic illness or chronic illness with frequent healthcare needs. However, the confidence intervals included null values (RR = 1.86, 95% CI [0.60, 3.12] and RR = 1.41, 95% CI [0.94, 1.89] respectively), indicating statistical insignificance. The observed direction of these effects is consistent with early screening and communication of results being beneficial for high-risk populations, but these findings are exploratory and require confirmation in larger studies.
Less than 10% of participants engaged with recommended resources from psychosocial screening when surveyed at the 3-month follow-up. This pattern is consistent with the findings of Marshall et al.’s (2024) systematic review, where despite high uptake of psychosocial screening, under 40% of children who were identified as high-risk engaged with recommended psychosocial resources. Similarly, a cross-sectional study by Sheridan et al. (2021) examined patients discharged from the pediatric ED with mental health complaints and found that 10% of these patients were unable to establish outpatient follow-up care six months post-discharge, primarily due to concerns about provider availability. Our study identified additional barriers, including costs of services and lack of knowledge about mental health services, which were echoed by Collopy et al.’s (2021) interviews with pediatric patients with cardiovascular diseases and comorbid mental health issues. These findings highlight significant challenges in the follow-up and utilization of recommended mental health services, emphasizing the need to address these barriers to improve care continuity and access. Possible pathways for follow-up could be improved by offering virtual or low-cost options, brief automated check-ins, and access to a social worker or care coordinator to help families schedule appointments and navigate services. MyHEARTSMAP can also serve as a tool to improve mental health literacy, helping families understand their child’s needs and the available resources. Together, these steps can bridge the gap between screening and service use, improving continuity of care for children with identified psychosocial needs.
Limitations
This study sample was drawn from a single tertiary pediatric health center, which may limit the generalizability of the findings to broader pediatric populations. The study’s extended duration also presented challenges, particularly due to a transition from paper charts to electronic medical records about one-third of the way through the study. During this transition, MyHEARTSMAP reports, which were printed on paper, were not always readily accessible to physicians as they transitioned to the new electronic medical record system (Chong et al., 2024). To address this, trained research assistants ensured that treating teams were aware of and reviewed the MyHEARTSMAP reports.
The study period included the COVID-19 pandemic period and public health protocols restricted non-essential allied mental health services, such as child life, until mid-2022. To address this limitation, sensitivity analyses were conducted to assess the impact of child life services on the intervention’s outcomes (Table S2). Finally, under 60% of participants in the standard of care arm completed the MyHEARTSMAP tool post-discharge. Given the similar prevalence of psychosocial concerns in the standard of care and intervention groups, we trust that the observed difference in receiving psychosocial resources among those who screened positive is attributable to exposure to the intervention, as randomized.
Conclusion
This study’s findings demonstrate that universal mental health screening can help identify those placed at higher risk of mental health burden, prompting the treating team to request psychosocial services as needed. MyHEARTSMAP demonstrates potential as a low-barrier tool for clinicians of varying backgrounds to address both physical and mental health needs, promoting holistic care of pediatric patients in a hospital setting.
Supplemental Material
Supplemental Material - Universal Psychosocial Screening in Hospitalized Pediatric Patients: A Randomized Control Trial
Supplemental Material for Universal Psychosocial Screening in Hospitalized Pediatric Patients: A Randomized Control Trial by Rebecca Liu, Alyssa Chong, Jeffrey Bone, Ian Pierce, Sydney Sparanese, Tanner March, Kathryn Armstrong, Robert Baird, Anthony Cooper, Michelle Demos, Janis Dionne, Alice Foster, Soojin Kim, Constadina Panagiotopoulos, Quynh Doan in Clinical Child Psychology and Psychiatry
Footnotes
Acknowledgements
We would like to acknowledge the START research team for their support with data collection and Ms. Karly Stillwell, BSc, whose administrative support was instrumental for the completion of this study.
Ethical Considerations
This study was approved by the University of British Columbia Research Ethics Board on July 26, 2021 (approval #H21-01221).
Consent to Participate
Written informed consent was obtained from all participants.
Consent for Publication
Informed consent for publication was provided by all participants.
Author Contributions
All authors approve of the final manuscript as submitted and agree to be accountable for it.
Rebecca Liu designed data collection instruments, collected data, carried out data analysis, drafted the initial manuscript, and critically reviewed/revised the manuscript.
Alyssa Chong collected data, drafted the initial manuscript, and critically revised the manuscript.
Dr. Jeffrey N. Bone assisted with study design, carried out data analysis, drafted the initial manuscript, and critically reviewed/revised the manuscript.
Dr. Ian Pierce collected data, carried out data analysis, and critically reviewed/revised the manuscript.
Dr. Sydney Sparanese assisted with study design, designed data collection instruments, collected data, and critically reviewed/revised the manuscript.
Tanner March liaised with nursing staff regarding study related training, collected data, and critically reviewed/revised the manuscript.
Drs. Kathryn Armstrong, Robert Baird, Anthony Cooper, Michelle Demos, Janis Dionne, Alice Foster, Soojin Kim, and Constadina Panagiotopoulos assisted with study design revisions, coordinated study participation within their respective divisions, and critically reviewed/revised the manuscript.
Dr. Quynh Doan conceptualized and designed the study, coordinated and supervised data collection, and critically reviewed and revised the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This This work was supported by a project grant from the Canadian Institutes of Health Research (sponsor identifier: PJT-152997). The Canadian Institutes of Health Research had no role in the design and conduct of the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and analyzed during the current study will not be made available due to the sensitive nature of data collected regarding mental health.
Clinical Trial Registration
Clinicaltrials.gov, MyHEARTSMAP In-Patient Study, NCT06553521, https://clinicaltrials.gov/study/NCT06553521?term=NCT06553521&rank=1
Supplemental Material
Supplemental material for this article is available online.