
Abstract
Objective
Our objective was to explore clinicians’ views on the MyHEARTSMAP screening report; whether this report has impacted their patient care, and if so, how. MyHEARTSMAP is a psychosocial self-screening tool for youth to identify mental health concerns.
Methods
We conducted a cross-sectional study as a sub-study of the MyHEARTSMAP In-Patient randomized control trial. Eligible clinicians (nurses and physicians who have cared for patients in one of our partnered specialties and have seen a MyHEARTSMAP report in their patients’ charts) provided their perceptions of the screening report through a survey.
Results
Sixty-five clinicians were enrolled; 60 (92.3%; 95% CI 85.8–98.8%) believe psychosocial screening is beneficial, with many finding it helpful for building rapport with patients/families and providing additional mental health information. Thirty-seven clinicians (56.9%; 95% CI 44.9–69%) had previously read or used the MyHEARTSMAP report, and 31 (83.8%; 95% CI 71.9–95.7%) of these clinicians found the report helpful. Clinicians specifically found the report helpful for communicating with the patient, and guiding patient-centered care.
Conclusion
Clinicians’ perceptions towards the MyHEARTSMAP report were positive amongst those who had previously encountered it. While clinicians believe psychosocial screening is beneficial, exploring options for better accessibility to the screening results is necessary to increase utilization.
Plain Language Summary
Understanding Clinicians’ Views on Mental Health Screening, Hospital Care, and Discharge Planning: In this study, we asked clinicians about their thoughts on the MyHEARTSMAP screening report and how it affects their patient care. MyHEARTSMAP is a tool that helps identify mental health issues in youth who are hospitalized. Once the youth completes the tool, the results are printed and placed in the patients’ physical chart so that their care team can assess it. We found that most clinicians believe overall screening for mental health concerns (not specific to MyHEARTSMAP) is useful for building relationships with patients and families, and it provides them with new information about their patients' mental health. When clinicians used the MyHEARTSMAP report, they found it specifically helpful for communicating with patients/families and helpful for allowing the patient to have a platform to provide their own input into their care plans. Overall, clinicians had positive views about the MyHEARTSMAP screening report, but we need to make it easier for them to access the results of the screenings.
Keywords
Introduction
Among hospitalized pediatric patients, the co-existence of medical and psychiatric conditions is a frequently encountered phenomenon (Bardach et al., 2014; Chavira et al., 2008; Pinquart & Shen, 2011). A retrospective analysis conducted on 670,161 pediatric hospitalizations found that 13.2% of admitted youth experienced psychiatric comorbidities (Doupnik et al., 2016). Coexisting psychiatric illnesses among medical pediatric admissions can increase length of stay and contribute up to $90 million in yearly hospital expenditure (Doupnik et al., 2016). Typically, care for hospitalized youth focuses on the physical concerns that lead to hospitalization, often neglecting the synergistic relationship between physical and mental health. To provide holistic care and to optimize patient recovery, screening and addressing co-existing mental health concerns when managing physical ailments is essential (Poulsen et al., 2016; Shafran et al., 2017). Screening instruments that assess both psychological and social (psychosocial) factors enables identification and management of mental health issues (Lee et al., 2019; Monohan et al., 2022), potentially improving longer term health outcomes, treatment efficacy, and health-related quality of life (Iragorri & Spackman, 2018). However, limited data exists on how clinicians across diverse inpatient specialties perceive and act on findings from psychosocial screening tools implemented in clinical settings. Further research is needed to explore the usability of psychosocial screening outputs in pediatric patient care, their implementation potential, and whether screening prompts or informs clinicians’ delivery of patient care (Battista, 2015).
MyHEARTSMAP is a digital, self-administered psychosocial screening instrument that allows patients and families to identify youths’ mental health needs in the pediatric emergency department (ED). MyHEARTSMAP evaluates 10 psychosocial areas:
The current investigation is a sub-study nested within the larger randomized control trial, with the objective to gauge how inpatient clinicians involved in the care of the trial participants perceive the utility of psychosocial screening results (i.e., the MyHEARTSMAP report) in delivering patient care.
Methods
Study design
We conducted a cross-sectional survey study nested within a randomized control trial of inpatient pediatric patients at a Western Canadian children’s hospital, specifically surveying clinicians who previously cared for the patients in the trial. Our approach to survey design and administration was informed by the Dillman’s Tailored Design Method. (Stern et al., 2014) Following a preliminary item generation based on study objectives, the survey underwent multiple iterations of review and modification by two of our team members, who are experts in methodology with extensive clinical experience. The survey was digitally hosted and administered over the secure web-based program, Research Electronic Data Capture (REDCap) platform (Harris, 2008, 2019). Ethics approval was obtained by our institution’s clinical research ethics board. All participants provided informed consent prior to survey completion.
Outcome measures
Our primary outcome was to explore the clinician-perceived impact psychosocial screening reports had on patient care. Clinicians self-reported their perceived utility of psychosocial screening for hospitalized patients (beneficial, no impact, or harmful) and perceived helpfulness of the MyHEARTSMAP report using 5-point Likert scales (very helpful to very unhelpful). Text boxes were provided for qualitative responses. As a secondary outcome, we gauged how the MyHEARTSMAP report impacted several dimensions of patient care: clinician-patient communication, patient and family involvement in the care process, and the context of care delivery. (Kitson et al., 2013) These were self-reported through closed ended yes/no questions, followed by text boxes to contextualize survey responses.
Study setting and population
This study was conducted in an inpatient setting in a pediatric quaternary care hospital between December 2022 and April 2023. The randomized control trial, MyHEARTSMAP Inpatient, included participants hospitalized under one of our partnered pediatric inpatient services: general paediatrics, cardiology, nephrology, neurology, endocrinology, gastroenterology, orthopaedic surgery, urology, and general surgery. Participants were randomized to receive the intervention or standard of care. In the intervention arm, participants (n = 142) completed MyHEARTSMAP once their hospitalization was confirmed, while still in the emergency department. The completed MyHEARTSMAP tool generates a report with recommendations for psychosocial services based on self-scoring and a validated algorithm (Virk et al., 2019). This report is placed in the patient’s chart, where it is accessible to members of their clinical care team. Standard of care participants (n = 143) completed the MyHEARTSMAP tool post-hospital discharge, to ensure screening results did not impact in-hospital care management, but families were sent the report for personal use. For this current study, clinicians (nurses, resident and attending physicians) who have previously cared for patients screened with MyHEARTSMAP during admission and were aware of the screening report in their patients’ chart were invited to participate. These inclusion criteria were verified through the eligibility survey all participants had to complete prior to study enrolment. The study setting reflects a collaborative environment where various clinician roles (nurses coordinating daily care, resident physicians managing immediate medical decisions, and attending physicians overseeing care plans) work together to deliver patient care. As the study population includes clinicians from across various pediatric services, it provides a comprehensive perspective on how MyHEARTSMAP influences clinical practice.
Study recruitment and procedures
Study invitations were regularly shared through emails, meetings, and clinician rounds and study flyers were placed in the inpatient wards in staff-only areas. Clinicians were approached in person on the inpatient wards on a rolling basis at varying days and times of the week. It was clearly communicated to clinicians who were approached that this was a voluntary study, and they had the freedom to decline participation or withdraw at any stage of the study (if enrolled) without facing consequences. Snowball sampling was used to encourage clinicians who completed the study to spread the word amongst their colleagues. Prior to study enrolment, participants completed an online eligibility survey and e-consent process if eligible. Consenting clinicians were directed to the demographic and main study survey, which took 10–15 minutes to complete. The demographics survey included items regarding participants’ gender, race, and occupation (including current position, and number of years in clinical practice). The main study survey sought information on participants’ perceived utility of psychosocial screening on hospitalized patients, and perceived helpfulness of the MyHEARTSMAP report in their patient care. The main survey items were self-reported using Likert scales and closed-ended questions, followed by text boxes where qualitative responses were collected to contextualize participants’ close-ended responses.
Analytic approach
For survey items assessing the screening report’s helpfulness, a quantitative approach was utilized to summarize clinicians’ Likert responses. Proportions and 95% confidence intervals were used for each degree of perceived utility of psychosocial assessments and helpfulness of MyHEARTSMAP. Demographic variables were descriptively reported. We conducted a qualitative analysis of clinicians’ open-text responses using Braun and Clarke’s thematic approach (Braun & Clarke, 2006) for each survey question. This aimed to identify emerging themes pertaining to clinician perceptions of psychosocial screening tool utility, their perceived helpfulness towards the MyHEARTSMAP tool report, and opportunities for improvement. Coding categories were refined iteratively with input from the study team. Representative quotes are provided for each open-ended item, followed by an identifying number for the participant (e.g., ID 1). All data analysis (including organization and coding) was completed in Microsoft Excel. The research materials related to this paper, including data and analysis, are available upon request from the corresponding author.
Results
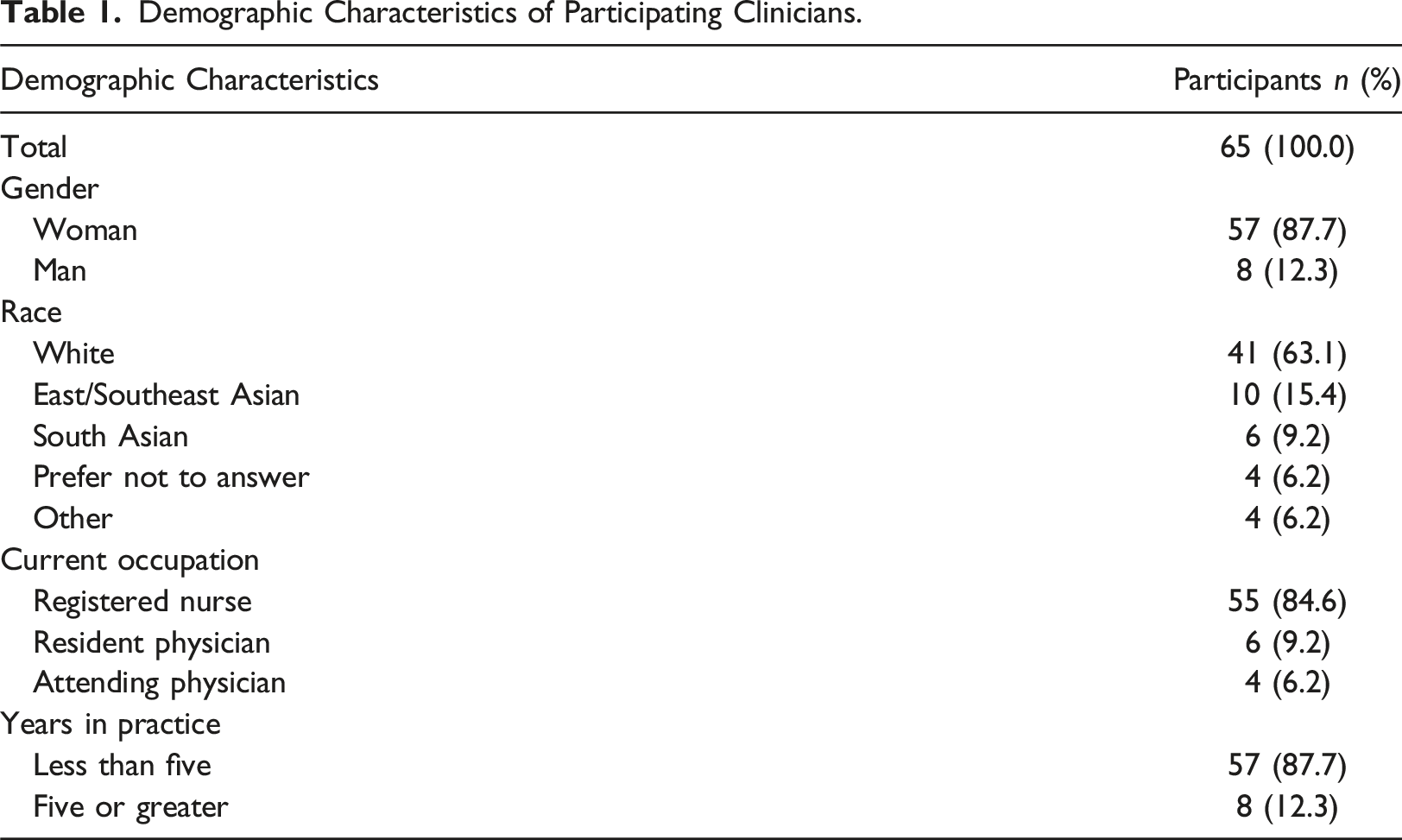
Demographic Characteristics of Participating Clinicians.
Participant Responses for Survey Items.
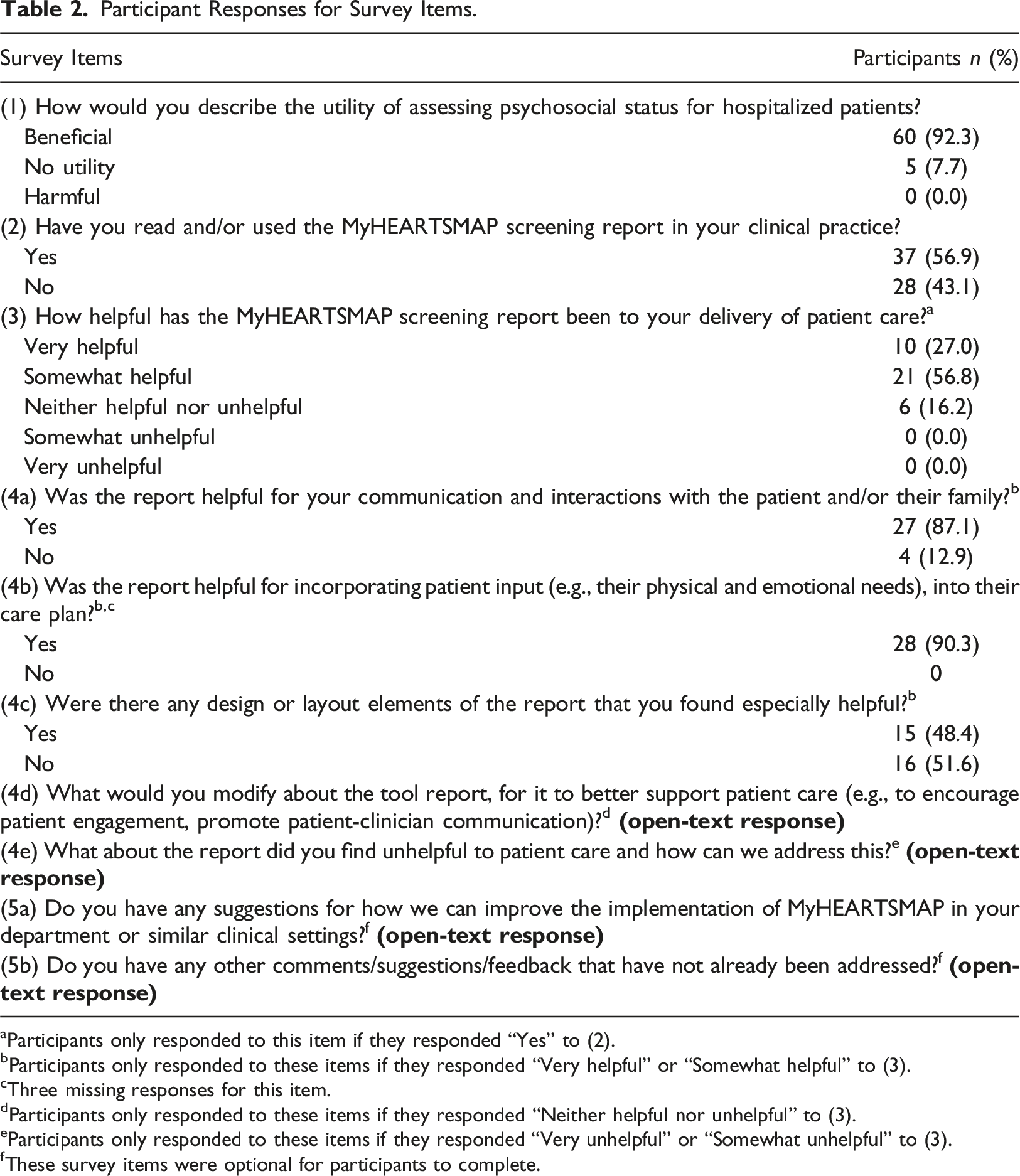
aParticipants only responded to this item if they responded “Yes” to (2).
bParticipants only responded to these items if they responded “Very helpful” or “Somewhat helpful” to (3).
cThree missing responses for this item.
dParticipants only responded to these items if they responded “Neither helpful nor unhelpful” to (3).
eParticipants only responded to these items if they responded “Very unhelpful” or “Somewhat unhelpful” to (3).
fThese survey items were optional for participants to complete.
High-level perspectives of psychosocial screening in the inpatient setting
Among all survey respondents, 60 (92%) believed that assessing psychosocial status for hospitalized patients is beneficial. These respondents described psychosocial screening tools as useful in helping establish patient-clinician relationships and providing additional information about the patient’s mental health. One clinician described that: “[I] think it’s hard to tell sometimes when patients are having difficulties or struggling, it sometimes is hidden or not brought up and we don’t automatically ask every patient. [I] think it would be helpful to identify patients who need some help and be recommended resources that we can share.” (Registered nurse, ID:9)
Conversely, 16% of clinicians saw no utility in universal psychosocial screening. Lack of education and inadequate patient responses on the tool were cited responses that contributed to the shortfall of utility. One clinician reported that specific to MyHEARSTMAP, they “personally haven’t researched or seen the result of this – maybe there is follow up [they’re] not personally aware of.” From a safety perspective, no participating clinician endorsed potential harms associated with psychosocial screening.
Perceived utility of MyHEARTSMAP in the inpatient setting
Overall helpfulness
Of the 65 participants, 37 (57%) had directly interacted with the MyHEARTSMAP report during their patient care duties at least once, while 28 (43%) had seen the MyHEARTSMAP reports in their patients’ charts and were aware of them but had not read any. Among the 37 participants who had engaged with the MyHEARTSMAP report, 31 (84%) found it helpful to their patient care, while the remainder found it neither helpful nor unhelpful.
Clinicians found that the report helped them guide and provide holistic care, gain information about the patient’s mental state, and aided the patient in self-identifying their psychosocial status. The screening report was described as helpful for investigating the “many aspects of social factors that impact the patient and the family”. Another clinician expressed that: “[They] just feel that knowing that extra bit about the child that they have shared truly allows [them] to gain perspective on what might work or not work for them and what their strengths are to achieve certain goals like discharge.” (Registered nurse, ID: 33)
Those who found the screening report neither helpful nor unhelpful (16%) cited reasons related to accessing resources. One clinician stated that “[They] think the barrier to helping these patients…[is] resources outside of [their] control.” There is also uncertainty regarding how to apply psychosocial screening results in their practice due to lack of training or comfort with mental health management. A clinician suggested more efforts directed towards “education for nurses regarding the purpose of the tool/how to integrate it into our practice.” Of note, no clinicians who had previously read/used the report found it unhelpful. Clinician responses to the utility and perceived helpfulness of the MyHEARTSMAP screening report is summarized in Figure 1. Consenting clinicians and the proportions who reported using MyHEARTSMAP in-practice and found the instrument helpful to patient care.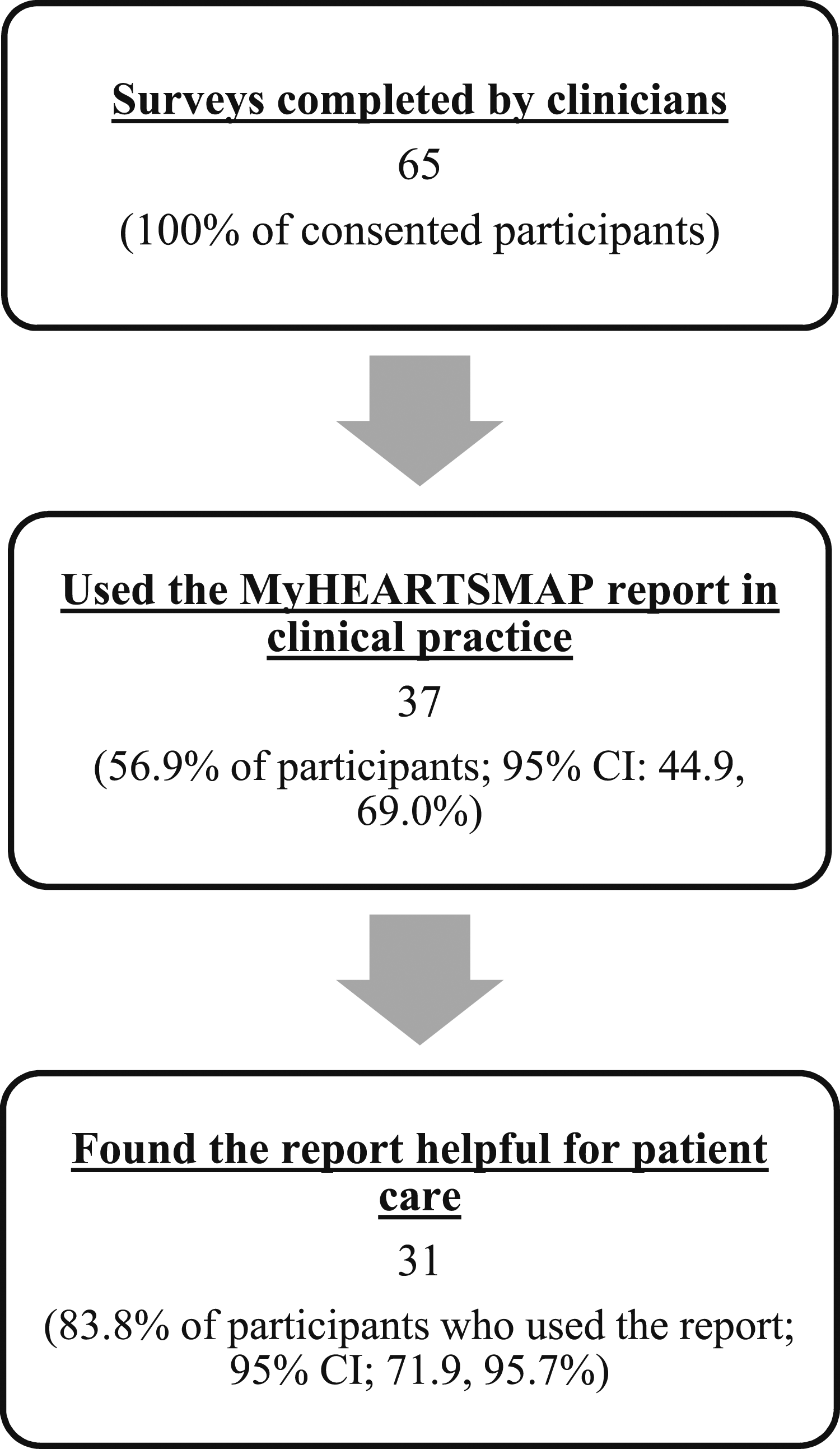
Communication
Twenty-seven (87%) of the 31 participants who found the MyHEARTSMAP screening report helpful, found it specifically helpful in improving communication/interactions with patients and their families. The respondents expressed that the report made it easier to initiate conversations, as it contained prompts that were used “to follow as a guideline”. The screening report provided background information on patients which saved time by eliminating redundant questioning and helped personalize their approaches.
The 4 (13%) participants who did not find the MyHEARTSMAP report specifically helpful for patient/family communication cited inadequate patient responses to the tool being the most significant factor. As one clinician reported, “the one [report they’ve] seen so far was not very helpful as the patient did not identify any issues and selected N/A for most answers.”. Another clinician expressed that “it could be more helpful depending on a patient’s answers”.
Patient-centered care
A large proportion (90%) of participants that found the MyHEARTSMAP report helpful found it useful for incorporating patient input into their care plan. Emerging themes showed the MyHEARTSMAP report was supportive in personalizing clinicians’ practices, providing a platform for patient input, and helping them better understand the patient, as the report “provides more knowledge of the patients’ needs as it has guided questions/prompts for the provider to use that we may have not thought to ask”. Another clinician reported that: “Because the patient fills out the booklet, it gives them a voice to communicate to us how to best decrease the stressors involved in hospitalization.” (Registered nurse, ID:7)
Tool interface
Less than half (48%) of the participants identified specific elements of the report that made it helpful stating that it was straightforward and concise and was “comprehensive of most mental health categories”. Other respondents that did not specifically find the report’s design or layout elements helpful expressed that nothing from the report “stood out” to them.
Challenges and opportunities for the MyHEARTSMAP report
Many clinicians expressed accessibility concerns regarding the paper MyHEARTSMAP report, mentioning that they would prefer to have the report uploaded on to CST Cerner (electronic medical record), the system used at our site. One clinician suggested that: “Since we have fewer reasons to review the paper chart on patients, now that most information is on-line in CST, it is easy to miss these reports. It would be nice to have some alert or indicator in CST…” (Attending physician, ID:70)
Additionally, participants conveyed that because the MyHEARTSMAP reports are placed in physical charts, it would be beneficial to have the report in a more “visible place” as the report is often “buried in the chartlet”, or to use markers such as “flash stickers or tags”, for increased visibility, as proposed by a clinician.
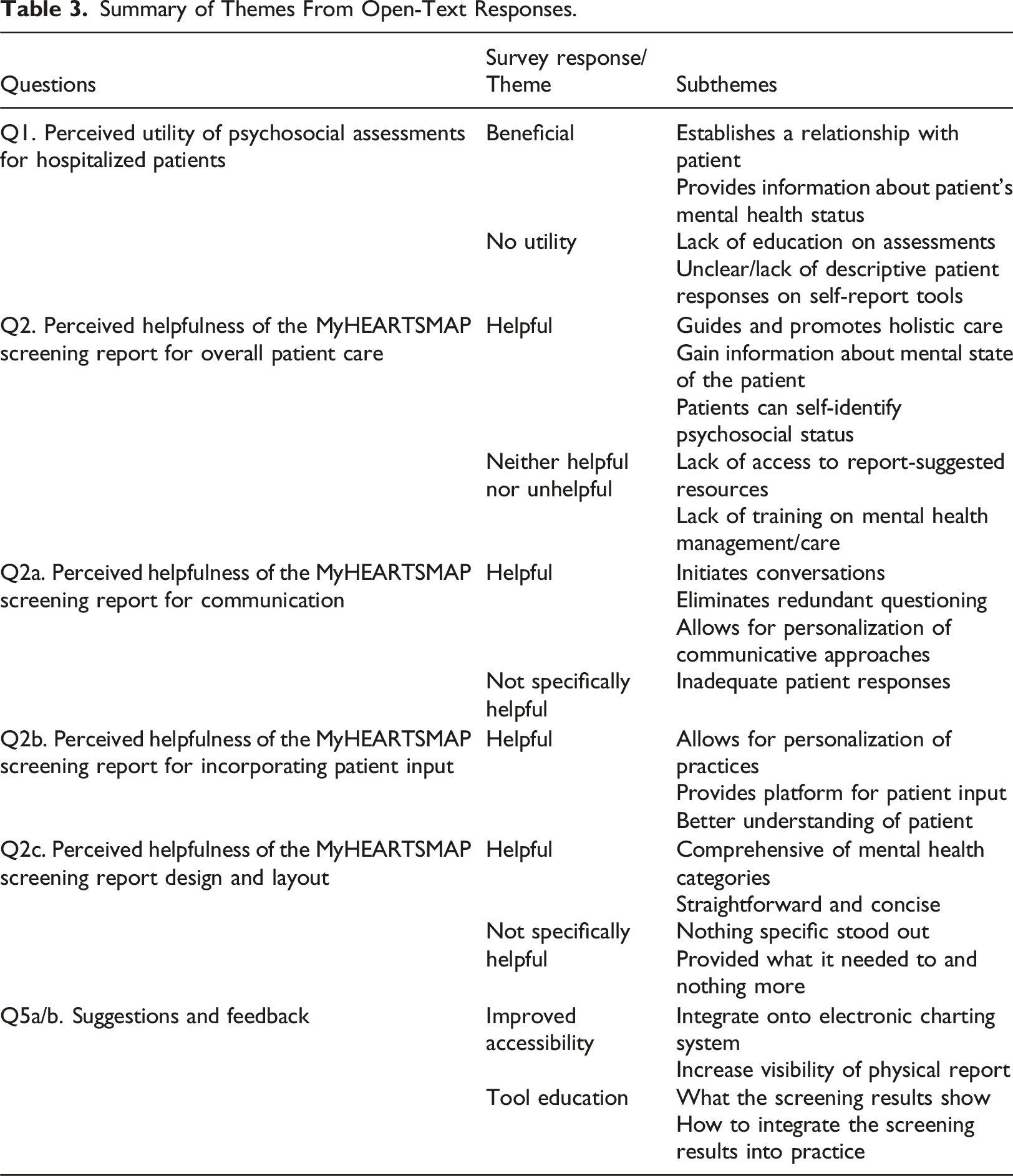
Summary of Themes From Open-Text Responses.
Discussion
This study describes clinicians’ perspectives around psychosocial screening and the use of MyHEARTSMAP for hospitalized children. Most participating clinicians showed positive attitudes towards the utility of psychosocial screening for hospitalized patients, finding it specifically helpful for establishing patient-clinician relationships, incorporating patient input into care plans, providing additional information about the patient’s mental health, and for improving communication. Some clinicians found limitations in the MyHEARTSMAP screening report as it relies on the richness of patients’ responses, particularly when explanation for self-reported scores were not provided.
Our outcomes are consistent with a study on perceptions of healthcare providers on psychosocial screening in a pediatric oncology setting. Their perceived benefits of psychosocial screening included providing concise documentation, aiding in initiating conversations, and directing families towards any necessary psychosocial services (Barrera et al., 2018). Like our study, respondents expressed unfamiliarity with handling psychosocial information provided by the screening, suggesting the need for standardized training in psychosocial care. In another study by Bradford and Rickwood (2015), clinician acceptability was explored for myAssessment, an electronic assessment of psychosocial status for youth. Their findings, in alignment with outs, showed that clinicians thought the assessment summary provided information about the patient’s psychosocial status and mental state (Bradford & Rickwood, 2015). Few other reports of clinician experience with psychosocial screening in other pediatric settings exist. However, in a study exploring clinician perspectives (n = 14) on the Genetic Psychosocial Risk Instrument (GPRI) for adult patients, similar results were found. Clinicians believed that the GPRI helped identify patient needs, improved clinician-patient communication, and improved patient care (Monohan et al., 2022).
The findings that clinicians believed the MyHEARTSMAP report supported families’ involvement into their child’s care planning is particularly important as Edbrooke-Childs et al. (n = 177) determined that child and parent inclusion in decision making in healthcare, based on patients’ self-reported psychosocial status, can lead to enhanced treatment outcomes. By including service users in the decision-making process, it allows them to understand the intended outcomes of their treatment plan, and provides an opportunity for personal input or to discuss any concerns they may have (Edbrooke-Childs et al., 2016). This, in turn, has the potential to increase the patient’s quality of life and satisfaction with their ongoing management.
Our study findings align with previous research, highlighting that system-level barriers such as staffing shortages, funding challenges, and resource limitations hinder the connection of families with necessary resources following psychosocial screening (O’Brien et al., 2016). There is also a systemic ceiling - the effectiveness of psychosocial screening tools is limited by available resources in the healthcare network in which the report is being used. Lee et al. (2022) evaluated wait-times for 123 community-based, child and adolescent mental health services. It was found that 60% of psychiatric programs, 35.5% of youth health-related (sexual health and substance-related resources) programs and 30% of social programs reported having wait times greater than one month, showing a substantial barrier for accessing these resources (Lee et al., 2022).
Limitations of this study include limited physician perspectives on the MyHEARTSMAP screening report, given that most study participants were nurses. Without further exploring physician perspectives, it is unclear how physicians view psychosocial screening, but as nurses frequently interact with patients, and often already include psychosocial screening as apart of standard practices, the screening report would be most utilized by them. This study also had a small sample size in consideration to the total number of MyHEARTSMAP screening reports available to clinicians through the randomized control trial. Lastly, by looking at survey data retrospectively, we were unable to probe further on responses or ask for clarification, whereas using interviews would permit this. However, our open text responses and qualitative data reached saturation, thus our findings are likely representative of the users’ experience. While this study focuses on clinician perspectives towards the MyHEARTSMAP screening results, it did not explore broader factors such as burnout, institutional pressures, or clinician hesitancy when addressing psychosocial concerns. These areas remain important for future research to better understand the challenges clincians face when engaging with psychosocial aspects of patient care.
Conclusion
Hospital-based pediatric clinicians perceived psychosocial assessment results to have utility in clinical management planning and interacting with patients and families. Integrating psychosocial assessment tools into inpatient hospital settings may facilitate greater clinical attention to providing holistic care, in addition to approaching patients’ acute medical concerns. Next steps prior to implementation should consider providing training on the effective use of psychosocial tools, ensuring that all members a patient’s clinical team are familiar with how to interpret and utilize screening tools and reports in their daily practice. Additionally, improving the accessibility of these tools within electronic medical records could further streamline their use, making it easier for clinicians to incorporate psychosocial information into patient care plans.
Footnotes
Acknowledgements
We would like to acknowledge Kathryn Armstrong, MD, Robert Baird, MSc, MDCM, Matthew Carwana, MD, Anthony Cooper, FRCSC, Michelle Demos, MD, FRCSC, Janis Dionne, MD, FRCSC, Alice Foster, MD, Soojin Kim, MD, and Constadina Panagiotopoulos, MD, FRCSC for their partnership critical to participant recruitment. We would also like to acknowledge Karly Stillwell, BSc, whose exceptional administrative support was instrumental throughout the study.
Author contributions
Ms. Chong conceptualized and designed the study; developed the data collection tool; recruited participants; led data collection, analysis, and interpretation; drafted the initial manuscript; reviewed and revised the manuscript; and approved the final manuscript as submitted. Dr. Virk conceptualized and designed the study; supervised the development of the data collection tool; oversaw data collection, analysis, and interpretation; critically reviewed and revised the manuscript; and approved the final manuscript as submitted. Dr. Doan supervised the conceptualization and design of the study; supervised the development of the data collection tool; supervised data collection, analysis, and interpretation; critically reviewed and revised the manuscript; and approved the final manuscript as submitted.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the BCCHRI Research Leadership Council Award at BC Children’s Hospital Research Institute. This work was completed in partial fulfillment of Ms. Alyssa Chong’s Bachelor of Science degree in Integrated Sciences. This work utilized REDCap (Research Electronic Data Capture) database, which was made available through BC Children’s Hospital Research Institute (F17-03510).
Appendix
Author biographies