
Abstract
Depression and anxiety are prevalent mental health challenges experienced by youth and young adults; however, existing psychosocial interventions are not sufficiently effective. A growing body of research has examined the multiple factors that impact psychosocial treatment participation for youth with anxiety and depression. This scoping review uses the Health Belief Model (HBM) as a guiding framework to synthesize and categorize the factors that limit treatment participation (i.e., barriers) and those that are associated with greater treatment participation (i.e., facilitators) for youth aged 12–25 presenting to outpatient services for mood and anxiety difficulties. Abstracts and titles were reviewed for 5483 studies with 21 studies fitting full inclusion criteria. Most of the extracted factors fell within established HBM domains, with factors related to perceived barriers and severity most frequently reported. Relatively understudied areas included cues to action, perceived susceptibility, and self-efficacy. Also identified were multiple factors that serve as both barriers and facilitators depending on the context. The factors not captured by the HBM were socio-demographic factors and factors related to mental health service structure. Overall, this review aims to inform development of refined assessment and treatment approaches for youth with anxiety and/or depression at risk for early treatment termination.
Plain Language Summary
A Review of Studies to Identify Barriers and Facilitators of Psychosocial Treatment Participation for Youth with Depression and Anxiety: Depression and anxiety are prevalent mental health challenges experienced by youth and young adults; however, existing interventions are not sufficiently effective. A growing body of research has examined the multiple factors that impact intervention participation for youth with anxiety and depression. This study will review the literature to synthesize and categorize the factors that limit treatment participation (i.e., barriers) and those that are associated with greater treatment participation (i.e., facilitators) for youth aged 12-25 presenting to outpatient services for mood and anxiety difficulties. Abstracts and titles were reviewed for 5483 studies with 21 studies fitting full inclusion criteria. Factors related to perceived barriers and severity most frequently reported and multiple factors that serve as both barriers and facilitators depending on the context. Overall, this review aims to inform development of refined assessment and treatment approaches for youth with anxiety and/or depression at risk for early treatment termination.
Keywords
Introduction
Depression and anxiety are prevalent mental health problems, affecting 15–20% of adolescents and young adults with rates substantially increasing in recent decades (Duffy et al., 2019; Shorey et al., 2022; Starcevic, 2006). Experiencing depression or anxiety as a youth or early adult can disrupt academic, social, and emotional development with long-term difficulties in education, employment, and interpersonal relationships (Chang & Kuhlman, 2022; Clayborne et al., 2019; Essau et al., 2014; Miles et al., 2018). A meta-analysis of 31 prospective studies pooling longitudinal data across multiple cohorts showed robust associations between depression in youth and later academic and vocational disadvantages (Clayborne et al., 2019). Further, depression onset in adolescence and early adulthood has been linked to lower household incomes and reduced likelihood of getting married and having children (Chang & Kuhlman, 2022). Similarly, experiencing anxiety in adolescence and early adulthood is associated with greater difficulties at age 30, including educational underachievement, interpersonal difficulties, chronic stress, substance abuse, and life and career dissatisfaction (Essau et al., 2014; Miles et al., 2018). Taken together, this body of research demonstrates that both depression anxiety in youth and early adulthood confer risk for poor outcomes (Chang & Kuhlman, 2022; Clayborne et al., 2019; Essau et al., 2014; Miles et al., 2018).
Psychotherapy is recommended as a first line intervention to treat mild to moderate anxiety and depression, with 70% of newly diagnosed youth choosing this option (Joyce et al., 2018). However, meta-analytic findings suggest that while psychosocial interventions can reduce depression and anxiety symptom severity, not all youth experience clinically significant benefits (Baker et al., 2021; Bear et al., 2020). Current evidence-based treatments for anxiety and depression have small to moderate effect sizes (Eckshtain et al., 2020; Fluckiger et al., 2014). Further, disorder heterogeneity and individual differences also make it challenging for evidence-based treatments to be universally applicable (Parker & Fletcher, 2007), suggesting a need to refine treatments to better reflect the unique needs of those failing to sufficiently benefit.
The efficacy or effectiveness of evidence-based treatments is often limited by low participation and early termination with only one-third of youth attending eight or more sessions and many evidence-based interventions requiring about 13–16 sessions (Fluckiger et al., 2020; Miller et al., 2008). Some research has sought to improve treatment participation by examining common barriers to care, including time limitations and other responsibilities (e.g., work, school, babysitting younger siblings; O'Connor et al., 2020; Meredith et al., 2009; Seligman et al., 2020), having comorbid mental health challenges (O’Dor et al., 2021), being a racial or ethnic minority (Miranda et al., 2015; Zarger & Rich, 2016), low socioeconomic status (Zarger & Rich, 2016), and skepticism around treatment effectiveness (Mehra et al., 2021; Miranda et al., 2015; Moore et al., 2020). These barriers are associated with lower treatment utilization, engagement, and adherence (O’Connor et al., 2020; Mehra et al., 2021; Meredith et al., 2009; Miranda et al., 2015; Moore et al., 2020; Seligman et al., 2020; Zarger & Rich, 2016) and less post-treatment symptom and impairment reduction (Abbott et al., 2019). Additionally, treatment facilitators commonly reported include perception of potential benefit, therapist factors (e.g., rapport, knowledge, collaboration), and treatment availability (O'Dor et al., 2021; Upadhyay et al., 2019; Wisdom et al., 2006)). However, to date, factors that influence treatment participation for youth with depression and anxiety have not been systematically reviewed. Given the variety and range of factors studied, categorizing and consolidating the evidence is an important next step in informing opportunities for treatment innovation and further research.
Health Belief Model
Psychosocial treatment barriers and facilitators may be understood within the Health Belief Model (HBM), which was initially developed to categorize treatment seeking behaviour for physical health conditions but has also been used in a mental health context (Nobiling & Maykrantz, 2017; Smith, 2009) and with a range of age groups, including adolescents and young adults (Rickwood et al., 2005). The HBM proposes six domains that influence treatment participation: perceived susceptibility, perceived severity, self-efficacy, perceived benefits, perceived barriers, and cues to action (Nobiling & Maykrantz, 2017).
Perceived susceptibility refers to how vulnerable an individual believes they are to a health problem and is predictive of help seeking intentions (Connor et al., 2014; Kim & Zane, 2016). Failing to recognize treatment need increases the time between symptom onset and disorder recognition, with research demonstrating an average delay of 8 years in diagnosing mood or anxiety disorders and an additional one-year delay to seek treatment (Thompson et al., 2008).
Perceived severity refers to how much an individual believes symptoms have serious functional consequences (Kim & Zane, 2015), and is a robust predictor of treatment seeking and engagement (Abbott et al., 2019; Lilly et al., 2020; O’Dor et al., 2021). In some contexts, less severe symptoms promote treatment engagement and benefit with more severe symptoms predicting lower treatment engagement and poorer clinical outcomes (e.g., O’Dor et al., 2021; Seligman et al., 2020). Further, symptom severity is associated with negative self-talk and hopelessness, which may reduce understanding and application of intervention components (Abbott et al., 2019; O'Dor et al., 2021). However, the literature is mixed, with other studies indicating that higher severity promotes engagement and improved clinical outcomes, possibly through better recognition of treatment necessity and increased motivation for change (e.g., Li et al., 2019; Wu et al., 2001).
The next component of the HBM is self-efficacy, which is the belief in one’s ability to promote change (Nobiling & Maykrantz, 2017). Some research has shown that higher self-efficacy is a treatment facilitator associated with greater treatment utilization and positive outcomes in young adults with depression (Lilly et al., 2020). However, findings are inconsistent, with lower self-efficacy at times facilitating treatment participation through its association with greater perceived symptom severity and uncertainty regarding independent symptom management (Andersson et al., 2014; Keeling et al., 2020).
Perceived benefits refer to a person’s belief in the effectiveness of the treatment and its potential to reduce distress (Kim & Zane, 2016; Lilly et al., 2020). Benefits may include expected improvements in emotional functioning, coping with stress, processing past experiences, handling current stress, and reducing problematic thinking and behaviours (Mehra et al., 2021). In contrast, skepticism suggests low perceived benefit and is a barrier to engagement (Mehra et al., 2021; Meredith et al., 2009; Miranda et al., 2015; Moore et al., 2020; Stafford & Draucker, 2020). Of note, some research indicates that racial minorities perceive fewer psychosocial treatment benefits, which can worsen treatment participation within marginalized communities (Kim & Zane, 2016).
Perceived barriers are a next domain of the HBM and robust cross-cultural predictors of treatment participation in anxious adolescents and young adults (Kim & Zane, 2016; O’Connor et al., 2020). Many youth perceive barriers to attending treatment such as time constraints, transportation challenges, and financial limitations (Mehra et al., 2021; Moore et al., 2020). These barriers have a particularly adverse effect on treatment outcomes for at-risk populations (Golberstein et al., 2019; Miranda et al., 2015; Zarger & Rich, 2016).
Finally, cues to action refer to proximal drivers of treatment participation that increase motivation to participate in an intervention (Dillon et al., 2020). Cues to action may be internal (e.g., thoughts about treatment, realization of problem severity) or external (e.g., advertisement, recent referral to treatment program, interpersonal experiences, personal crises) (Castonguay et al., 2016; Daud et al., 2020; Lilly et al., 2020; Nobiling & Maykrantz, 2017).
Current Study
The objective of this scoping review is to synthesize and categorize findings from empirical studies that have identified barriers and facilitators that influence psychosocial treatment participation in youth aged 12–25 presenting to outpatient mental health services for mood and anxiety difficulties. Barriers and facilitators will be described, categorized, and charted within the HBM framework adapted for mental health. Factors that do not fit within the original HBM will be analyzed thematically as possible extensions of the HBM. As the HBM was initially developed to understand medical treatment seeking behaviour, a review of the mental health literature may reveal important gaps in the HBM with proposed extensions to better capture help-seeking behaviour in mental health contexts. Additionally, this study is expected to increase understanding of common barriers and facilitators to mental health care, ultimately generating knowledge that may inform future studies and potential modifications for psychosocial treatment for youth with depression or anxiety.
Methodology
Study methodology was informed by the Preferred Reporting Items for Systematic Reviews and Meta-Analysis extension for scoping reviews (PRISMA-ScR) (Tricco et al., 2018). Articles published in print or online from January 2000 to May 2022 were identified through systematic searches in Medline (Ovid), Embase (Ovid), APA PsycInfo (Ovid), and CINAHL (EBSCO). The search strategy was first drafted in Medline by a health sciences librarian (TR) and refined through team discussions. The final search strategy (Supplemental Table 1) was then translated and executed in the four selected databases on May 27, 2022. All strategies used database-specific subject headings, keywords in natural language, and advanced search operators to capture and combine multiple concepts. This multi-stranded approach was needed to identify articles that might meet the complex set of eligibility criteria, which included individual factors, treatment factors, participation, and outcomes. Final search results were imported into online review software Covidence, which automatically removed duplicates. Year limit was 2000 to date of search. No language or study type limits were applied. Conference abstracts and dissertations were removed when possible.
Inclusion criteria were: (1) participants aged 12–25 and/or their parents/caregivers; (2) youth presenting for and/or engaging in psychosocial treatments for a mood and/or anxiety disorder; (3) inclusion of a measure and/or report of a barrier and/or facilitator associated with psychosocial treatment participation and/or outcomes; (4) English publication; (5) peer-reviewed publication; (6) outpatient psychosocial treatment; and (7) North American samples. The decision to restrict to North American samples ensured a focused synthesis with contextual comparability across health systems and cultural frameworks, whereas including global literature would have introduced substantial variability that could obscure patterns relevant to clinical practice in North America.
Exclusion criteria were: (1) the majority of study participants fell outside the age range of 12–25 years; (2) participants seeking or in treatment for autism, schizophrenia, psychotic disorders, or other mental disorders; (3) study did not include a measure and/or report of a barrier and/or facilitator; (4) published in languages other than English; (5) non-peer-reviewed publications (e.g., grey literature, theses), review papers, commentaries, case studies, or study protocols; (6) did not include outpatient treatment; (7) participants resided outside of North America. Articles were included if most data met inclusion requirements (e.g., if the majority of sample fell within the age range) or if exclusion conditions were analyzed additionally or separately (e.g., separate analyses for psychopharmacological and psychotherapy treatment conditions).
Two reviewers (ADS and EN) independently screened titles and abstracts for primary inclusion. Conflicts were resolved in team discussions with senior co-authors (ACB, JK, BA). Full texts of eligible articles were obtained and rescreened by the two reviewers (ADS, EN). Conflicts were again resolved through team discussions with senior co-authors (ACB, JK, BA). A data extraction form was created and included fields for the following: basic article information (e.g., authors, publication year, study location); participant demographics (e.g., age, gender, socioeconomic status, ethnicity); informant (e.g., parent or youth); sample size; study design; disorder type; psychosocial intervention type; treatment setting; timing of data collection (e.g., before, during, or after treatment); types of barriers and/or facilitators; and relevant measures of identified barriers and/or facilitators. Two reviewers (ADS and EN) independently charted the data.
The raw data derived from the extraction form was reviewed by co-authors and reduced to reflect the most relevant information organized alphabetically by author. All identified barriers and facilitators were then categorized according to the domains of the HBM. Treatment barriers and facilitators that best fit proposed additions of the HBM specific for mental health (e.g., service structure factors, socio-demographic factors) were also included.
Results
Study Selection
The PRISMA flow diagram (Figure 1) outlines the number of articles included and excluded at each stage of the review, resulting in a final total of 21 articles that were included. PRISMA flow diagram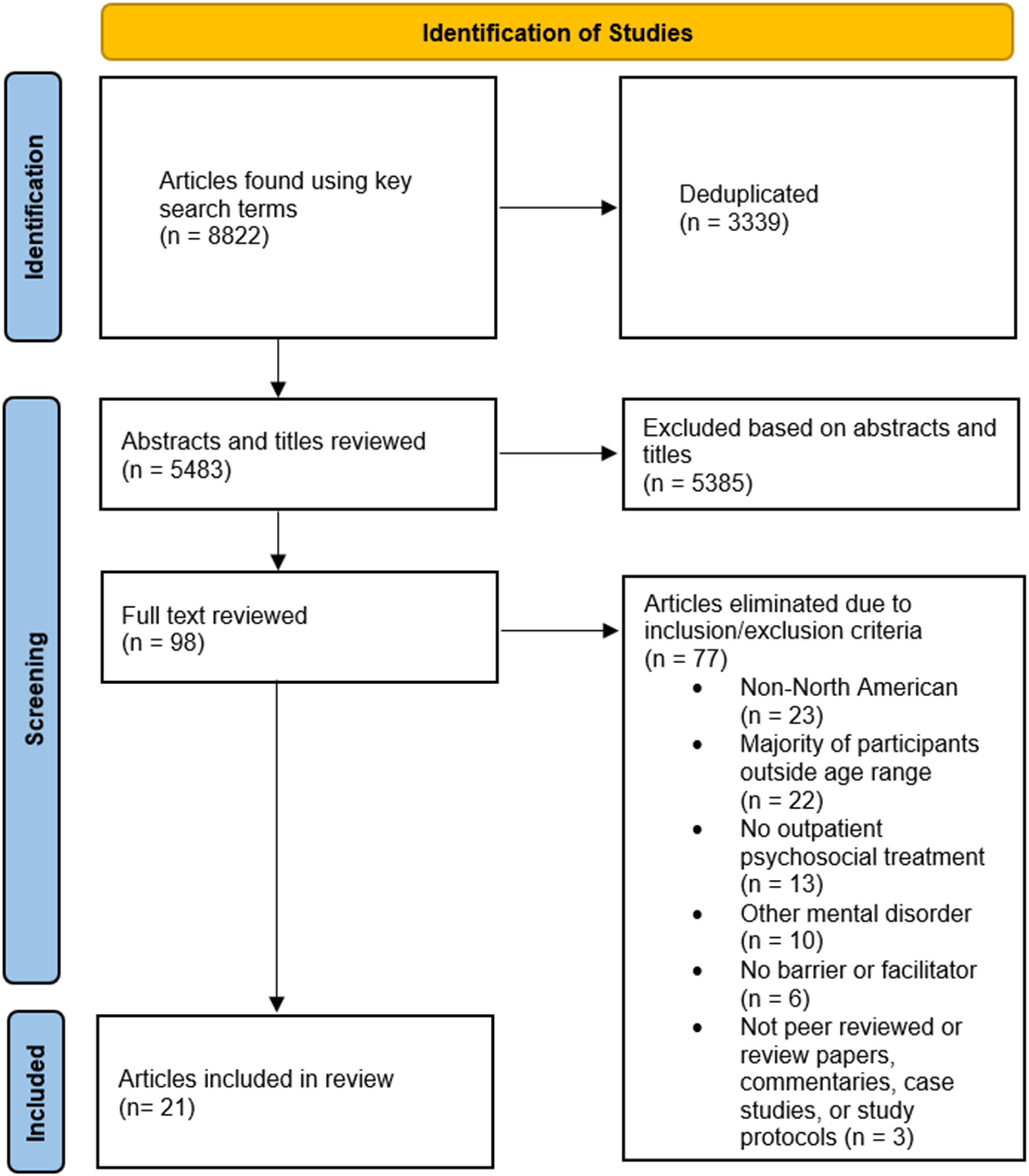
Study characteristics and key findings related to treatment barriers and facilitators can be found in Supplemental Table 2. Included articles used American (n = 16) and Canadian (n = 5) samples with individuals with depression (n = 12), anxiety (n = 5), or both (n = 4). Sample sizes ranged from N = 22 to N = 9896, and the majority of samples were predominantly white (67%) and female (81%). Most studies employed quantitative analyses (n = 15); others used mixed methods (n = 4) or qualitative (n = 2) approaches.
Study Categorization
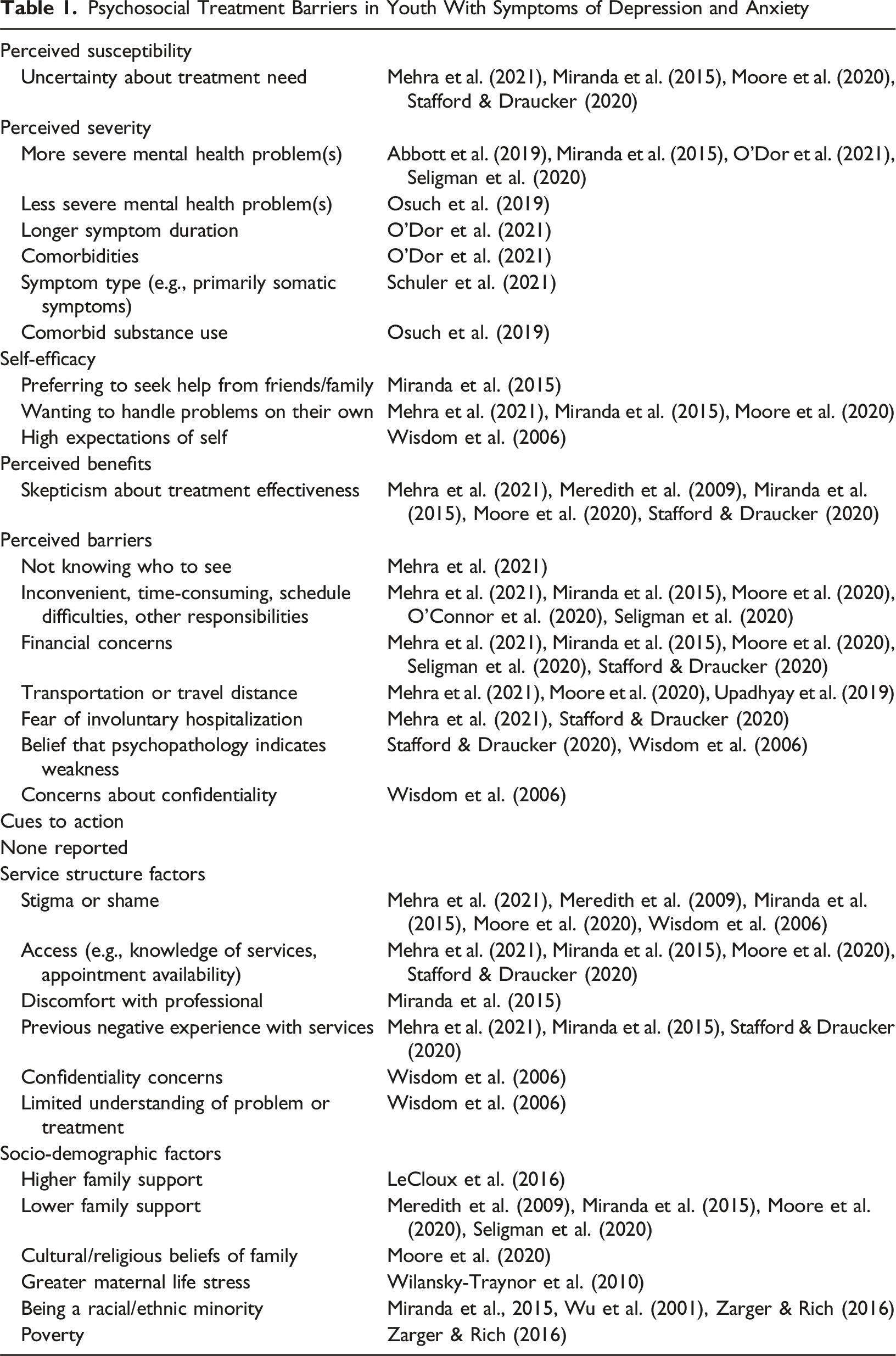
Psychosocial Treatment Barriers in Youth With Symptoms of Depression and Anxiety
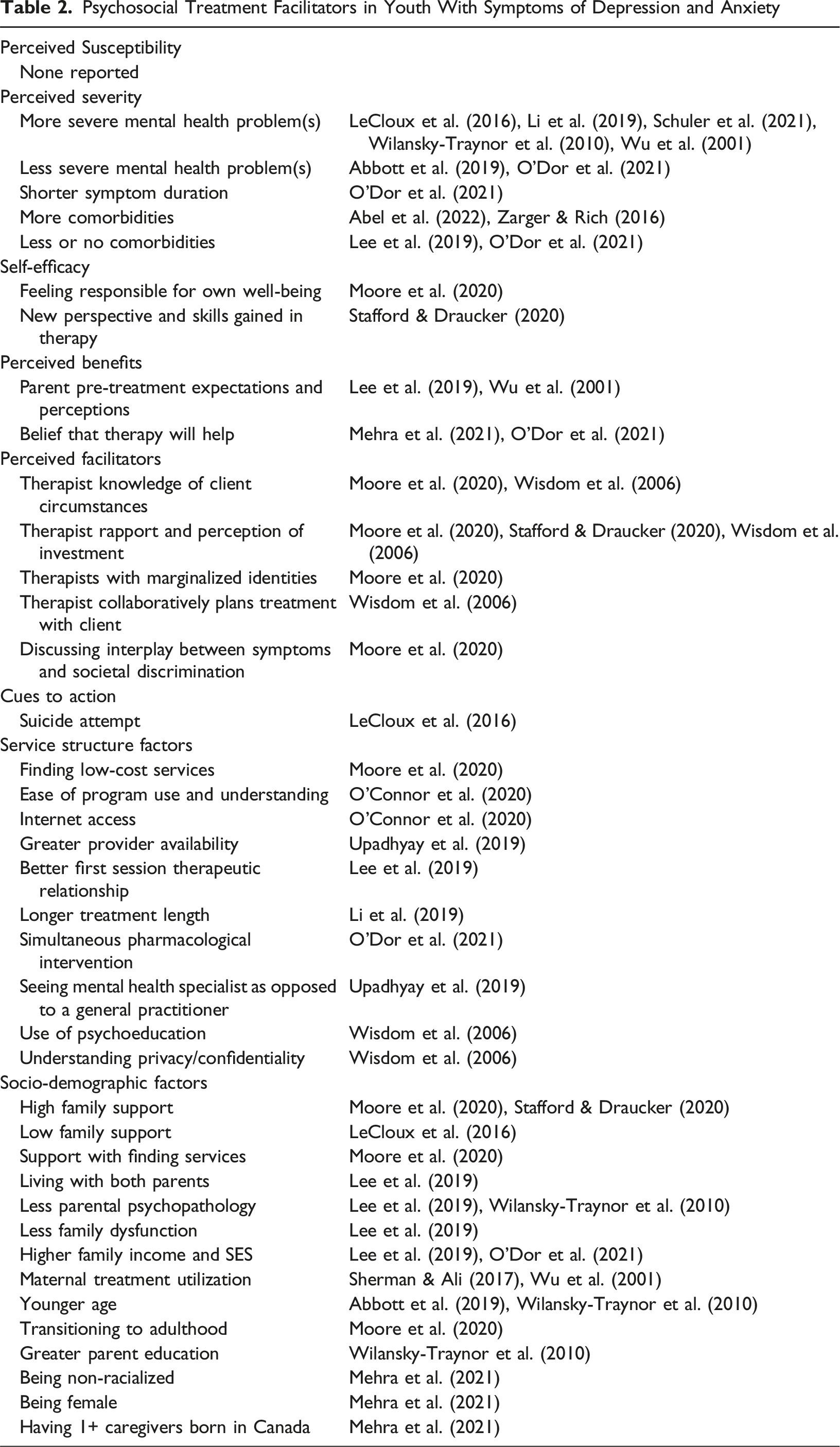
Psychosocial Treatment Facilitators in Youth With Symptoms of Depression and Anxiety
Study Findings within the HBM Framework
Uncertainty about treatment need was a treatment barrier related to the perception of susceptibility and was reported in four studies (Mehra et al., 2021; Miranda et al., 2015; Moore et al., 2020; Stafford & Draucker, 2020). No facilitators related to perceived susceptibility were identified.
Mental health problem severity findings were mixed, with greater severity being both a barrier (Abbott et al., 2019; Miranda et al., 2015; O'Dor et al., 2021) and a facilitator (LeCloux et al., 2016; Li et al., 2019; Schuler et al., 2021; Wilansky-Traynor et al., 2010; Wu et al., 2001). Interestingly, lower severity of mental health problems was also both a barrier (Osuch et al., 2019) and a facilitator (Abbott et al., 2019; O'Dor et al., 2021). Findings were also mixed with comorbidities being both a treatment barrier (Lee et al., 2019; O'Dor et al., 2021; Osuch et al., 2019) and a facilitator (Abel et al., 2022; Zarger & Rich, 2016). Symptom duration findings showed longer duration being a barrier and shorter duration being a facilitator of better treatment outcomes; however, this was found in just one study (O'Dor et al., 2021).
Higher self-efficacy was a treatment facilitator as indexed by feeling responsible for one’s own well-being and developing new skills and perspectives over the course of therapy (Moore et al., 2020; Stafford & Draucker, 2020). However, when individuals had high expectations of self and preferred to handle challenges independently or with social support, this type of increased self-efficacy was reported as being a treatment barrier (Mehra et al., 2021; Miranda et al., 2015; Moore et al., 2020; Wisdom et al., 2006). When parents had higher pre-treatment expectations, and clients believed therapy would help, participation was greater (Lee et al., 2019; Mehra et al., 2021; O'Dor et al., 2021; Wu et al., 2001). Conversely, when skepticism was high and treatment benefits were unclear, there was a greater likelihood of treatment disengagement and drop-out (Mehra et al., 2021; Meredith et al., 2009; Miranda et al., 2015; Moore et al., 2020; Stafford & Draucker, 2020).
There were many perceived logistical barriers to treatment participation reported by parents and youth, including not knowing who to see, time constraints, financial concerns, transportation challenges, and other responsibilities (Mehra et al., 2021; Miranda et al., 2015; Moore et al., 2020; O'Connor et al., 2020; Seligman et al., 2020; Stafford & Draucker, 2020). Also reported, and maybe somewhat unique to mental health care, were concerns about confidentiality, the possibility of involuntary hospitalization, and whether psychopathology indicates weakness (Mehra et al., 2021; Stafford & Draucker, 2020; Wisdom et al., 2006).
On the other hand, studies also reported several perceived facilitators of treatment participation including therapist knowledge of circumstances, therapist-client rapport, client perception of therapist’s investment in their care, and degree of collaborative treatment planning (Moore et al., 2020; Stafford & Draucker, 2020; Wisdom et al., 2006). Further, in one study clients with marginalized identities, such as racial or sexual minorities, engaged better with therapists with similar identities (Moore et al., 2020).
Cues to action are proximal precipitants of treatment seeking behaviour, such as suicidal behaviour prompting an individual to engage in treatment to reduce distressing and impairing symptoms (LeCloux et al., 2016). Cues to action were less relevant as treatment barriers, with none reported in the reviewed studies. Attempted suicide was a cue to action that facilitated treatment-seeking behaviour (LeCloux et al., 2016).
Emergent Domains Beyond the HBM
A service structure factors category was created, because factors specific to mental health service use were not adequately captured by the HBM. Barriers to treatment classified within this category include stigma or shame (Mehra et al., 2021; Meredith et al., 2009; Miranda et al., 2015; Moore et al., 2020; Wisdom et al., 2006), client discomfort after poor treatment experiences (Mehra et al., 2021; Miranda et al., 2015; Stafford & Draucker, 2020), and clients not understanding their symptoms and treatment options (Wisdom et al., 2006). There were also facilitators related to service structure such as the use of psychoeducation, collaborative treatment planning, and explanations of confidentiality (O'Connor et al., 2020; Wisdom et al., 2006). Clients also participated more when services were low cost (Moore et al., 2020), there was greater provider availability, and the provider was a mental health specialist as opposed to a general practitioner (Upadhyay et al., 2019). When treatments were virtual, other factors such as internet access became important (O’Connor et al., 2020). Treatment-related factors (e.g., early therapeutic rapport, longer treatment length, simultaneous pharmacological treatment) also facilitated treatment participation (Lee et al., 2019; Li et al., 2019; O'Dor et al., 2021).
The reviewed studies identified several socio-demographic factors related to treatment participation. Findings were mixed with regards to family support, with one study reporting it as a barrier (LeCloux et al., 2016) Formatting… and five studies identifying it as a facilitator (Meredith et al., 2009; Miranda et al., 2015; Moore et al., 2020; Seligman et al., 2020; Stafford & Draucker, 2020). Other family factors such as family cultural and religious beliefs, worse family functioning, and parental psychopathology also predicted less treatment participation (Lee et al., 2019; Moore et al., 2020; Wilansky-Traynor et al., 2010). Further, two studies found that when mothers had previous therapeutic experiences, their adolescents were more likely to participate in treatment (Sherman & Ali, 2017; Wu et al., 2001).
Demographic barriers to treatment participation included being racialized or low-income (Lee et al., 2019; Miranda et al., 2015; O'Dor et al., 2021; Wilansky-Traynor et al., 2010; Wu et al., 2001; Zarger & Rich, 2016). Demographic facilitators included younger age (Abbott et al., 2019; Wilansky-Traynor et al., 2010); emerging adulthood (Moore et al., 2020), greater parent education (Wilansky-Traynor et al., 2010), being female (Mehra et al., 2021), living with both parents (Lee et al., 2019), and having multiple caregivers born in Canada (Mehra et al., 2021).
Discussion
This study aimed to systematically review studies that identified barriers and facilitators related to psychosocial treatment participation for youth aged 12–25 with depression and/or anxiety. Identified barriers and facilitators were then classified within the domains of the HBM, which has been widely used to understand participation in healthcare (Nobiling & Maykrantz, 2017). Although this model captured the majority of identified psychosocial treatment barriers and facilitators, two categories were added that may be key within mental health contexts: service structure and socio-demographic factors. Overall, the most studied factors fell within the domains of perceived severity, perceived barriers, service structure factors, and socio-demographic factors. Relatively understudied domains included cues to action, perceived susceptibility, and self-efficacy. There were also mixed findings within many domains, with multiple factors that serve as either barriers or facilitators depending on the context.
Perceived severity was a highly studied domain of the HBM with inconsistent findings; it was identified as both a barrier and a facilitator of treatment participation (Abbott et al., 2019; LeCloux et al., 2016; Li et al., 2019; Miranda et al., 2015; O'Dor et al., 2021; Osuch et al., 2019; Schuler et al., 2021; Wilansky-Traynor et al., 2010; Wu et al., 2001). For example, in two studies high anxiety severity was associated with increased avoidance of anxiety-provoking stimuli encountered in aversion to the therapeutic process, and reduced participation in treatment (Lehrbach et al., 2023; Lorian & Grisham, 2011). In contrast, other studies identified higher severity and longer symptom duration as motivators (facilitators) of treatment participation (Buckman et al., 2021; Klein et al., 2011). One explanation was that better treatment response may be achieved in cases of higher severity because there is more room for improvement compared to individuals with lower severity (Elices et al., 2022). Indeed, youth with more complex concerns, greater severity of psychopathology, and comorbid diagnoses may require more intensive and long-term treatment (Delgadillo et al., 2017).
It appears that the role of severity as a treatment barrier or facilitator was dependent on how it was operationalized, with some research suggesting that severity defined in terms of functional impairments was more limiting than severity indicated by increased symptomatology although additional research is needed in this area (O'Dor et al., 2021). In one study, higher initial severity was both a barrier associated with less symptom improvement and a facilitator associated with more rapid change, depending on how outcomes were defined (Stochl et al., 2022). Overall, although a preponderance of research has examined the role of perceived severity in treatment participation, findings remain mixed, and further research is needed to better understand how severity-related predictors interact to influence treatment participation in youth and young adults with depression and anxiety.
Another domain of the HBM that was highly researched was perceived barriers, which included logistical barriers (e.g., time constraints, transportation challenges) and other beliefs (e.g., involuntary hospitalization, being seen as weak); this was consistent with prior research showing that perceived barriers predicted treatment participation over and above demographic factors, symptom severity, and stressful life events (Goetter et al., 2020; Kazdin et al., 1997). The most identified facilitators of treatment participation were factors related to the therapist or the therapeutic process, such as a strong therapist-client bond (i.e., therapeutic alliance) and collaborative goal setting (Moore et al., 2020; Stafford & Draucker, 2020; Wisdom et al., 2006). These factors were identified repeatedly across the reviewed studies, suggesting that they may be important during the course of treatment. However, their relative importance or impact on client treatment participation has not yet been studied systematically.
Within the HBM, few studies identified cues to action, which are proximal treatment-facilitating factors that drive service seeking behaviours (Nobiling & Maykrantz, 2017). Cues to action were relatively understudied predictors of treatment participation (LeCloux et al., 2016; Monti et al., 2003). Suicidal behaviour emerged as an important cue to action in depressed adolescents (LeCloux et al., 2016), which was consistent with other research findings indicating that 68% of suicide attempters were in treatment one-month post-attempt and 62% at three months post-attempt (Monti et al., 2003). Suicidal behaviour can be a signal that urgent intervention is needed (LeCloux et al., 2016; Lizardi & Stanley, 2010). However, more research is needed to elucidate additional cues to action that predict participation in youth with mood and anxiety difficulties. These may include factors such as physician referrals or targeted advertisements (Nobiling & Maykrantz, 2017).
Perceived susceptibility, a pre-treatment mindset regarding a disorder, is believed to impact treatment participation (Nobiling & Maykrantz, 2017). Within the reviewed literature, only one barrier fit within the perceived susceptibility domain: uncertainty about treatment need (Mehra et al., 2021; Miranda et al., 2015; Moore et al., 2020; Stafford & Draucker, 2020). No facilitators were classified within the perceived susceptibility domain. However, four of the twenty-one reviewed studies (19%) identified uncertainty about treatment need as an important factor that is frequently reported in youth seeking treatment for mood and anxiety disorders.
Barriers and facilitators related to self-efficacy were also relatively understudied with inconsistent findings. Theories of motivation have highlighted the importance of self-efficacy, positing that individuals put forth more effort when they believe in their ability to achieve goals (Eccles & Wigfield, 2002). Bandura (1997) suggested that approaching and coping with previously avoided stimuli increases self-efficacy, with such strategies often employed in interventions such as Cognitive Behavioural Therapy (CBT). Subsequent research has extended this finding, demonstrating that self-efficacy improves with other treatment modalities (e.g., Acceptance and Commitment Therapy, Dialectical Behaviour Therapy) and with a variety of anxiety disorders (e.g., panic disorder, post-traumatic stress disorder, social anxiety disorder) and other mental health challenges (e.g., eating disorders) (Brown et al., 2014; Keshen et al., 2017). Similarly, in a sample of individuals with Generalized Anxiety Disorder, as CBT progressed, self-efficacy improved, and severity of anxious and depressive symptoms decreased (Visla et al., 2023). Self-efficacy was reported as a treatment facilitator with individuals developing new skills and positive perspectives over the course of therapy (Stafford & Draucker, 2020). However, high self-efficacy was a barrier when high expectations led to individuals wanting to solve problems independently or with family support rather than seek formalized treatment (Mehra et al., 2021; Miranda et al., 2015; Moore et al., 2020; Wisdom et al., 2006). Further, when self-efficacy was higher, it resulted in unrealistic treatment expectations (Visla et al., 2023) or increased worrying and negative emotionality as participants “prepared” themselves to face challenges (Newman & Llera, 2011; Visla et al., 2023). This could suggest a nonlinear association or a “Goldilocks effect” in which a moderate degree of self-efficacy might be most beneficial for optimal treatment participation (McCarthy et al., 2016)(). The influence of self-efficacy on treatment participation requires further nuanced study to unpack when and how it facilitates or negatively influences treatment participation.
While the majority of identified treatment barriers and facilitators fit within the HBM framework, two domains were created to capture additional treatment barriers and facilitators that were identified: sociodemographic factors and factors related to mental health service structure. Identified service structure barriers included youth perceptions of stigma and shame, which may be particularly relevant in mental health disorders and treatments (Wisdom et al., 2006). The reviewed articles also identified therapeutic alliance as a service structure facilitator, which was consistent with research linking therapeutic alliance to better treatment outcomes when compared to demographic factors, pre-treatment psychopathology, treatment modality, and setting (Barnicot et al., 2011; Steuwe et al., 2023). Logistical service structure factors identified in this review (e.g., costs, time constraints, provider availability, other responsibilities) also aligned with those reported in other research studies (Goetter et al., 2020; Kazdin et al., 1997).
Although demographic factors were reported as treatment barriers or facilitators in many studies, these findings should be interpreted with caution as meta-analytic findings have shown no robust demographic predictors of treatment participation (Barnicot et al., 2011; Cougle & Grubaugh, 2022). More research is needed to examine the interplay between racial factors, gender and sexuality factors, and social determinants of health (Barnicot et al., 2011; Cougle & Grubaugh, 2022). The Contact Hypothesis offers one possible explanation, as the treatment-seeking decisions of youth are likely influenced by relational dynamics such as trust and equity (Kennedy et al., 2021). Future research could test interventions that operationalize this theory, such as pairing youth with culturally competent providers or implementing structured trust-building strategies early in treatment.
Social support emerged as another predictor of treatment participation, with some studies suggesting higher support was better (Meredith et al., 2009; Miranda et al., 2015; Moore et al., 2020; Seligman et al., 2020; Stafford & Draucker, 2020) and one study suggesting that lower support facilitated participation (LeCloux et al., 2016). Two models might explain this discrepancy: the “deficit model” suggests that psychotherapy is utilized more when external support is limited, and the “competence model” posits that greater social support reflects well-developed skills needed to participate in treatment (Herrle & Angermeyer, 1997). More recent research has reasoned that lower support predicts increased psychosocial treatment utilization as some seek treatment to improve social relationships and family functioning (Graziano & Elbogen, 2017; Jaffe et al., 2023). Due to these complexities, the role of social support as a treatment barrier or facilitator should be individually assessed during intake or early in treatment.
Limitations
This study is limited in that the reviewed articles utilized a variety of incomparable methodologies, and many had insufficient data to support quantitative analyses. Further, study design rigor was variable and often dictated by feasibility within the research setting. However, including articles with a range of methodologies provided better ecological validity with data representative of real-world mental health contexts. Another challenge of this study was establishing search terms as there is no clearly established terminology to define the constructs of interest. For instance, treatment participation may be described in terms of attendance, engagement/disengagement, drop out, retention, attrition, discontinuation, or early termination. To manage this challenge, a research librarian (TR) developed and refined the search strategy (Supplemental Table 1) through an iterative process with senior co-authors until the search strategy was determined to capture the most relevant articles.
Another limitation was that most studies included a predominantly white and female sample, with racially, ethnically, and gender-diverse populations underrepresented in included studies. Additionally, this review examined only North American research in order to maintain feasibility and maximize contextual comparability across studies, as initial searches indicated that global literature produced a large body of research with substantial variation in health systems and cultural frameworks. Although restricting to North American research allowed for a more focused synthesis, there is a need for future research to include diverse samples and examine whether findings are replicable cross-culturally.
Conclusions
Overall, this review highlights that deciding to engage in psychosocial treatment is a complex process influenced by several factors across a variety of domains. This may guide clinical decision-making through refined assessment approaches and treatment adaptations that consider barriers to and facilitators of mental health care. This review also provides insight into both the relatively understudied factors that impact treatment participation and the factors that have been examined more frequently. Ultimately, this review hopes to spur subsequent research to inform tailored service provision for youth with anxiety and depression.
Supplemental Material
Supplemental Material - Barriers and Facilitators of Psychosocial Treatment Participation for Youth With Depression and Anxiety: A Scoping Review
Supplemental Material for Barriers and Facilitators of Psychosocial Treatment Participation for Youth With Depression and Anxiety: A Scoping Review by Anneesa D. Singh, Anne-Claude V. Bedard, Terri Rodak, Elida Nexha, John Krzeczkowski, André Plamondon, and Brendan F. Andrade in Clinical Child Psychology and Psychiatry
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ontario Graduate Scholarship.
Declaration of Conflicting Interests
The authors report there are no competing interests to declare.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.