
Abstract
Objectives
Adolescents with a chronic medical condition (CMC) are at greater risk of mental health difficulties, but demographic factors and subjective health may confound this relationship.
Design
Using data from a nationally representative adolescent sample from Northern Ireland (N = 1,299), we examined whether three CMC categories were associated with symptoms of depression, anxiety, posttraumatic stress disorder, and with suicidal thoughts or plans, and attempts.
Methods
Hierarchical multiple regression analyses were conducted to test whether the CMC classifications explained a significant proportion of the variance across the mental health variables, while controlling for age, sex, and subjective health. A multinomial logistic regression analysis was conducted to test whether the CMC classifications were associated with suicidality.
Results
CMC categories explained a small but statistically significant proportion of variance in mental health. Age was associated with suicidal thoughts or plans, and suicide attempts. Subjective health emerged as the factor most strongly linked to all criterion variables except suicidality.
Conclusions
Subjective health may be more strongly related to adolescent mental health than previously identified. Future research could explore potential psychosocial factors associated with these CMC classifications to clarify the links between CMCs and mental health.
Plain Language Summary
The relationship between having a chronic medical condition, mental health problems, and thinking about, planning, or attempting suicide: Teenagers with long-term physical health conditions are more likely to experience mental health difficulties, but this link may be explained by age, sex, and how healthy young people feel overall. This study used data from a large representative sample of teenagers in Northern Ireland to explore whether different types of chronic conditions were linked to depression, anxiety, post-traumatic stress disorder, and suicidal thoughts, plans, or attempts. Chronic medical conditions were linked to slightly higher levels of mental health symptoms overall. Older teenagers were more likely to report suicidal thoughts, plans, or attempts. How healthy teenagers felt was the factor most strongly related to mental health, except for suicidal thoughts, plans, or attempts. Teenagers’ own perspectives of their health may be more important for mental health than previously recognised. Future research could explore the social and psychological factors linked with chronic conditions to better understand how physical health and mental health are connected.
The peak age of onset for most mental health disorders occurs during late adolescence (Luo et al., 2024; Pfeifer & Allen, 2020). Depression and anxiety are common issues among adolescents with approximately 10.0% diagnosed with major depressive disorder, and 6.5% diagnosed with an anxiety disorder (Liu et al., 2024) - at least twice as many experience ‘sub-syndromal’ levels of depression and anxiety – and these mental health problems are associated with an increased risk of suicidality (Horn et al., 2021; Noyes et al., 2022). Over 700,000 people die by suicide every year, ranking as the third leading cause of death among adolescents (World Health Organization [WHO], 2025b). Northern Ireland has the highest rate of suicide among young people aged 15–24 in the United Kingdom at 17.8 per 100,000 people (Royal College of Pediatrics and Child Health, 2020).
One group who may be particularly at risk of these mental health and suicide sequelae are adolescents with a chronic medical condition (CMC). Globally, 20–30% of adolescents have CMC, with asthma being the most common (Asher & Pearce, 2014; Russo, 2022). CMCs in adolescence often co-occur with depression and anxiety (Brady et al., 2017; Cobham et al., 2018; Dudeney et al., 2024). Being diagnosed with a CMC, receiving invasive treatments, and managing chronic pain can be experienced as traumatizing for adolescents (Meentken et al., 2017; Pinquart, 2018), and higher rates of post-traumatic stress disorder (PTSD) have also been reported in adolescents with a CMC (Eskander et al., 2020; Pinquart, 2018).
There is also evidence that having a CMC is associated with a higher risk of suicidality in adolescence – defined by the American Psychological Association (APA) as the risk of suicide indicated by suicidal ideation, intent, or plans (APA, 2018; Heynemann et al., 2021; Underner et al., 2022; Zhang et al., 2019). Adolescents with a CMC can endure persistent pain, social stigma, social isolation, and impaired daily functioning, all of which can increase the likelihood of suicidality (Iannucci & Nierenberg, 2021). Ideation-to-action frameworks, such as the Interpersonal Theory of Suicide (Van Orden et al., 2010), Integrated Motivational-Volitional theory (O’Connor, 2011), and 3 Step Theory (Klonsky & May, 2015), posit that extreme physical or psychological pain, perceiving oneself as a burden, and thwarted belongingness or connectedness, are key facilitators for suicide ideation and attempts. These risk factors can be experienced as a direct consequence of having a CMC (Miao et al., 2024).
The strength of association between CMCs, mental health problems, and suicidality varies considerably across the literature (Ferro et al., 2017). Such variation may be accounted for by differences in measurement. While many studies account for the physical impacts of CMCs, they differ in how health is measured – some rely on objective indicators like patient health records, while others rely on subjective self-reports. Though not a direct measure, subjective health correlates with objective health status (Wuorela et al., 2020), and many studies support the reliability and validity of subjective health (Postigo-Zegarra et al., 2024). Obtaining subjective health reports of adolescents is increasingly prioritized in clinical practice, as they offer a broad understanding of how adolescents are affected across life domains including mobility, sleep quality, and independence (Dalgleish et al., 2020). Adolescents with good physical functioning are up to fifteen times more likely to report better subjective health scores than those with poor subjective health, and almost 80% less likely to report depressive symptoms (Shi et al., 2022). Regarding the onset of mental health difficulties, older adolescents who identify as female are typically much more prone to internalizing and have a higher risk of suicidal ideation and attempts (Levkovich et al., 2025; Miranda-Mendizabal et al., 2019).
The present study used data from the Northern Ireland Youth Wellbeing Prevalence Survey (Bunting et al., 2022) to examine whether adolescents with a CMC had higher levels of depression, anxiety, and PTSD, and whether they were more likely to have had suicidal thoughts or plans, and to have attempted suicide, whilst controlling for age, gender, and subjective health. Based on the existing evidence, we hypothesized that adolescents with a CMC, irrespective of gender, age, and subjective health status, would report higher levels of depression, anxiety, and PTSD (Brady et al., 2017; Pinquart, 2018), and would be more likely to have had suicidal ideation or plans, and to have attempted suicide (Ferro et al., 2017).
Methods
Participants and Procedures
This study used data collected from the Youth Wellbeing in Northern Ireland Prevalence Study (Bunting et al., 2022). The data comprised a nationally representative sample (N = 3,074) of children, adolescents, and young adults aged 2–19 years. Ethical approval for the original data collection was obtained from the relevant institutional ethics committee, and informed consent was obtained from both parents and participants. Between June 2019 and March 2020, a large representative sample of households in Northern Ireland was randomly drawn using the Pointer database. A total of 21,730 addresses were randomly selected for inclusion. Data collection was funded by the Department of Health Northern Ireland and commissioned by the Health and Social Care Borad in Northern Ireland.
Inclusion Criteria for the Analytic Sample
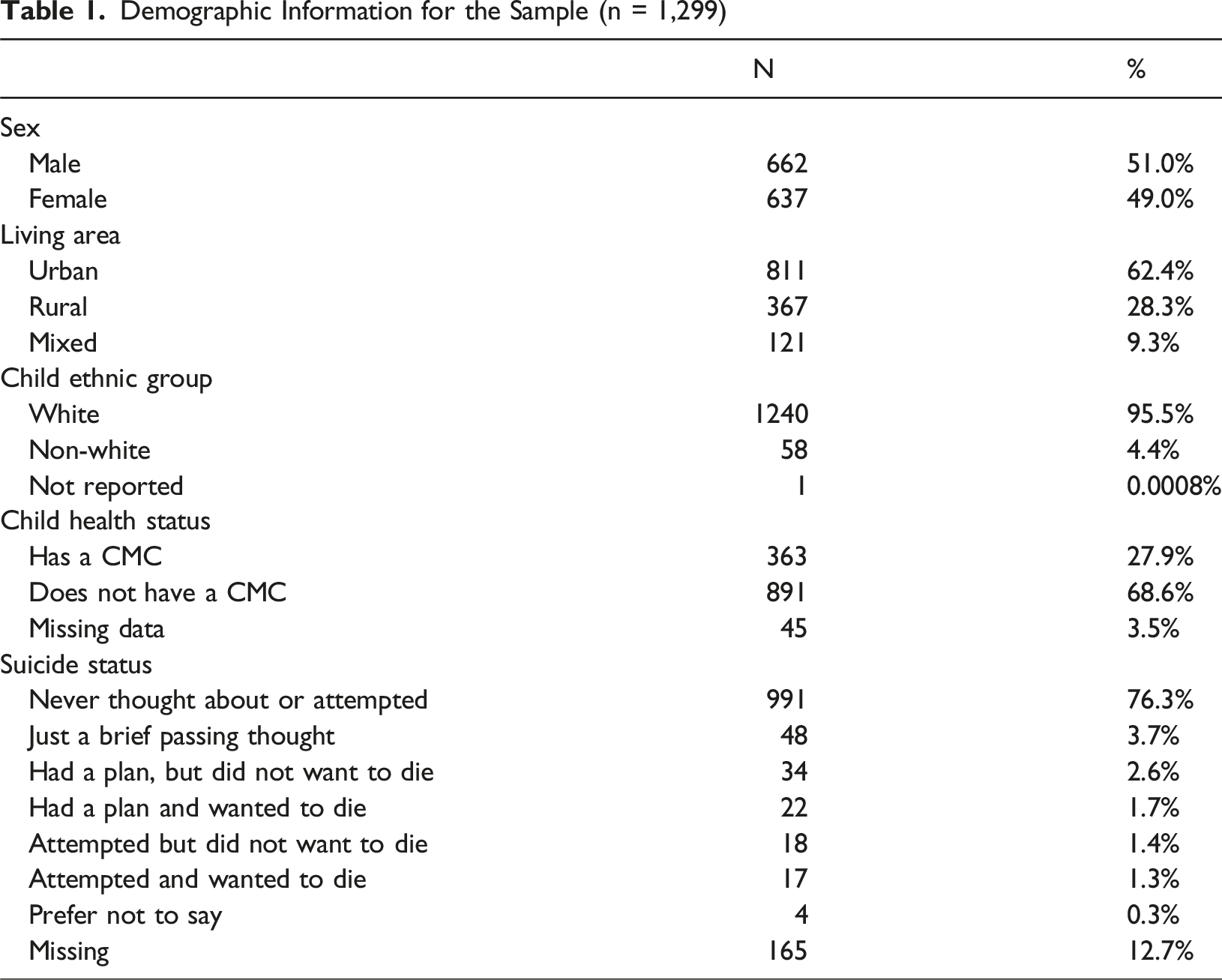
Demographic Information for the Sample (n = 1,299)
Measures
Diagnosis of a CMC
Frequency of Chronic Conditions Present in the Sample (n = 1,299)
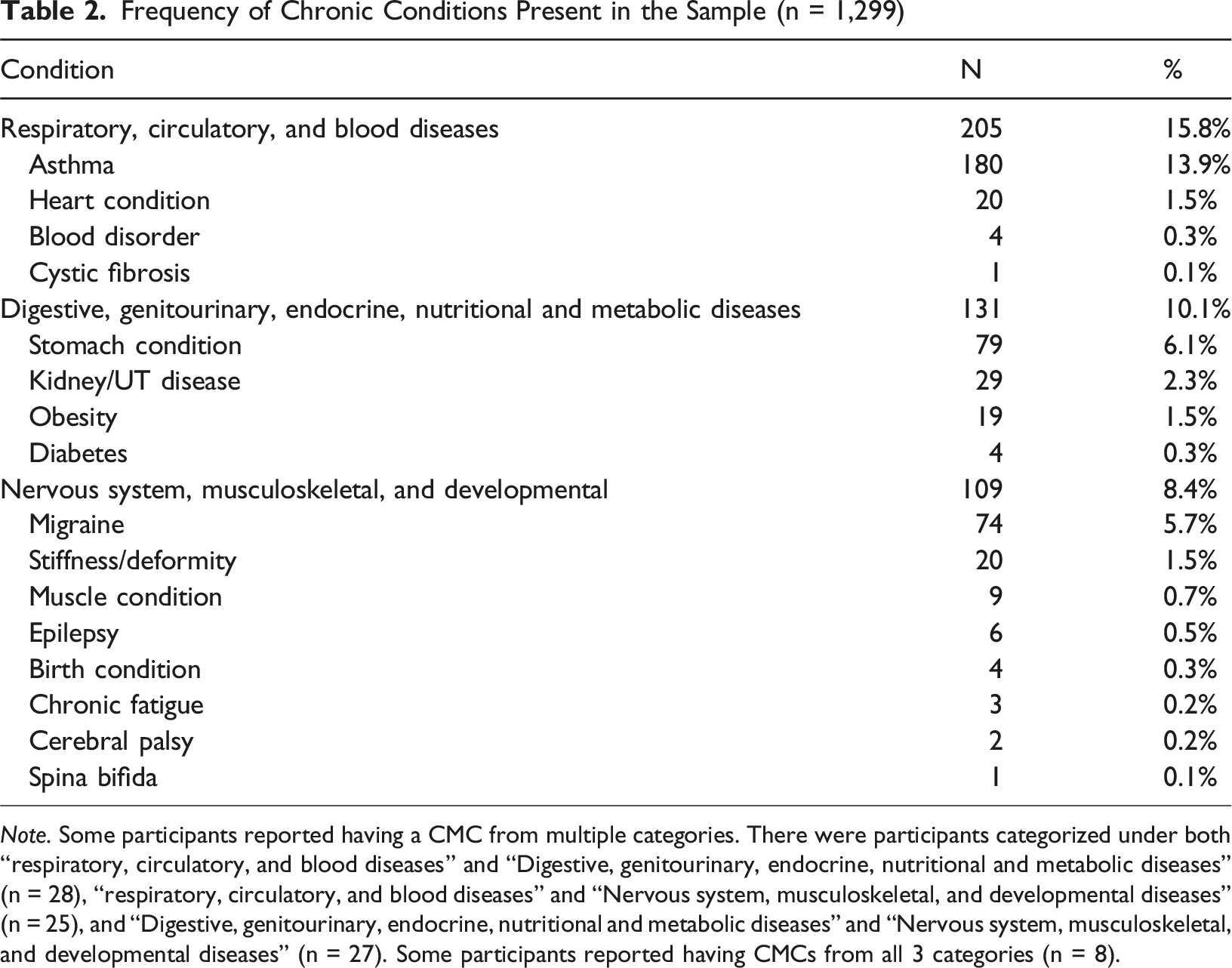
Note. Some participants reported having a CMC from multiple categories. There were participants categorized under both “respiratory, circulatory, and blood diseases” and “Digestive, genitourinary, endocrine, nutritional and metabolic diseases” (n = 28), “respiratory, circulatory, and blood diseases” and “Nervous system, musculoskeletal, and developmental diseases” (n = 25), and “Digestive, genitourinary, endocrine, nutritional and metabolic diseases” and “Nervous system, musculoskeletal, and developmental diseases” (n = 27). Some participants reported having CMCs from all 3 categories (n = 8).
Due to an under-representation of many diseases, we combined several diagnostic classifications to allow for more stable estimation of associations between CMCs and mental health variables, maintain distinctions between disease classes, and potentially identify disease classifications that are more burdensome for adolescents. These classifications were combined based on broad physiological system overlap and general patterns of disease burdens: 1. Respiratory, Circulatory, and Blood Diseases (n = 197) were grouped based on their co-occurrence and shared links to systemic infection; 2. Digestive, Genitourinary, Endocrine, Nutritional, and Metabolic Diseases (n = 126) were grouped based on their roles in metabolic functioning; and 3. Nervous System Diseases, Musculoskeletal Diseases, and Developmental Anomalies (n = 109) were combined due to their early-life onset, chronic progression, and impact on developmental functioning (note: Neoplasms and External Causes of Mortality were excluded from analyses as these were under-represented and could not meaningfully be combined with other classifications).
Depression and Anxiety Symptoms
Participants completed the full 47-item version of the Revised Children’s Anxiety and Depression Scale (RCADS) (Chorpita et al., 2000). While the RCADS assesses subdomains of anxiety such as generalized anxiety, social phobia, separation anxiety, obsessive-compulsive disorder, and panic disorder, total anxiety scores are obtainable by summing scores across the anxiety subscales. In the present dataset, participants reported how often they experienced each symptom using a 4-point Likert scale (“Never” = 0, “Sometimes” = 1, “Often” = 2, “Always” = 3). The RCADS does not provide participants with a timeframe on which to base their responses. The depression subscale comprises 10 items, and the anxiety subscale comprises 37 items. Depression scores range from 0 to 30, and anxiety scores range from 0 to 104, and in both cases, higher scores indicate higher symptom scores. The internal reliability scores for the depression (Cronbach’s α = 0.90) and anxiety (Cronbach’s α = 0.96) scales in this sample were high.
PTSD Symptoms
Participants completed the International Trauma Questionnaire – Child and Adolescent version (ITQ-CA) (Cloitre et al., 2018), which is a self-report measure of ICD-11 PTSD and Complex PTSD symptoms. The PTSD subscale is comprised of six indicators and participants report how often they experienced each symptom over the last month on a scale of 0–4 (0 = “never,” 1 = “a little bit,” 2 = “sometimes,” 3 = “a lot,” 4 = “almost always”). PTSD scores range from 0–24, with higher scores indicating higher levels of PTSD. Previous studies have found support for the psychometric properties of the ITQ-CA (Ho et al., 2022). The internal reliability of the PTSD scale scores in this sample was satisfactory (Cronbach’s α = 0.88).
Indicators of Suicidality
Participants were asked, “Have you ever thought about or attempted to kill yourself?,” which is an item taken from the Suicide Behaviors Questionnaire (SBQ-R) (Osman et al., 2001). Response options were: 1 = “never,” 2 = “it was just a brief passing thought,” 3 = “I have had a plan at least once to kill myself but did not try to do it,” 4 = “I have had a plan at least once to kill myself and really wanted to do it,” 5 = “I have had attempted to kill myself, but did not want to die,” and 6 = “I have attempted to kill myself, and really hoped to die.” Owing to low frequencies across the categories (i.e., response option 5, n = 18; response option 6, n = 17), and recognizing important differences between suicidal ideation and suicidal behavior (Klonsky et al., 2021), responses were recoded into three categories representing ‘no suicidal thoughts or attempts’ (i.e., original response option of 1, n = 991), ‘suicidal thoughts or plans’ (i.e., original response options 2, 3, 4, n = 104), and ‘suicide attempt’ (i.e., original response options 5 and 6, n = 35). Frequencies for each recoded response are presented in Table 1.
Subjective Health Status
Participants reported their general health on a 5-point Likert scale using the following prompt: “How is your health in general?” The scale was coded 1 (very bad) to 5 (very good). Participants were not provided with a timeframe. While full scales designed to assess subjective health exist and have proven reliable (Bart et al., 2018), the single item above is widely used across large epidemiological studies like the Canadian Health Survey on Children and Youth, which utilized a scale from 1 (poor) to 5 (excellent) (Wang et al., 2023). Subjective health measures like this have consistently been shown to be as reliable and valid as objective measures of health (Hamplová et al., 2022).
Data Analysis
Descriptive statistics were used to summarize scores on the measures of depression, anxiety, and PTSD. Data distributions were inspected for normality to ensure the data were suitable for analyses. Given that assumptions of linearity between independent variables and the dependent variables, multicollinearity across independent variables, and homoscedasticity were met, three hierarchical multiple regression analyses were employed to determine unique associations with each mental health variable (i.e., depression, anxiety, and PTSD). In step 1 of each model, age, sex, and subjective health were entered, while at step two, the three CMC classifications (i.e., Respiratory, Circulatory, and Blood Diseases; Digestive, Genitourinary, Endocrine, Nutritional, and Metabolic Diseases; and Nervous System Diseases, Musculoskeletal Diseases, and Developmental Anomalies) were entered as dummy variables. This ordering tests if each CMC class is uniquely associated with mental health problems, above and beyond the influence of known risk factors for mental health problems. The suicide variable was recoded to include three categories (0 = no suicidal thoughts or behavior, 1 = suicidal thoughts or plans, and 2 = suicidal attempt) so a multinomial logistic regression was conducted to test how age, sex, subjective health, and CMCs classes were related to suicidal thoughts or plans, and suicidal attempt. All analyses were conducted in IBM SPSS version 30.
Results
Descriptive Statistics
Descriptive Statistics for Continuous Variables
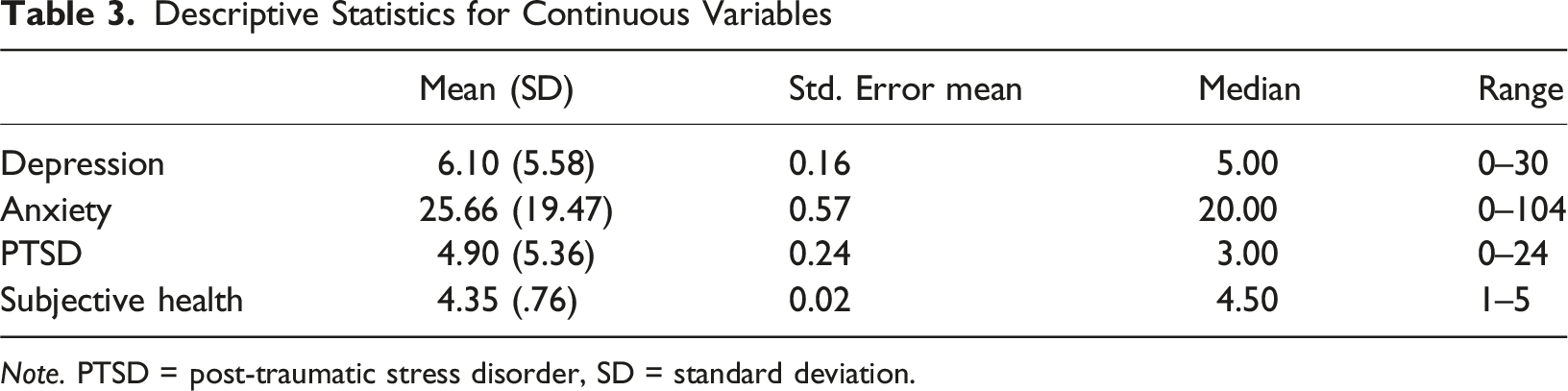
Note. PTSD = post-traumatic stress disorder, SD = standard deviation.
Hierarchical Multiple Regression Models of Depression, Anxiety, and PTSD
Hierarchical Multiple Regression Models of Depression, Anxiety, and PTSD
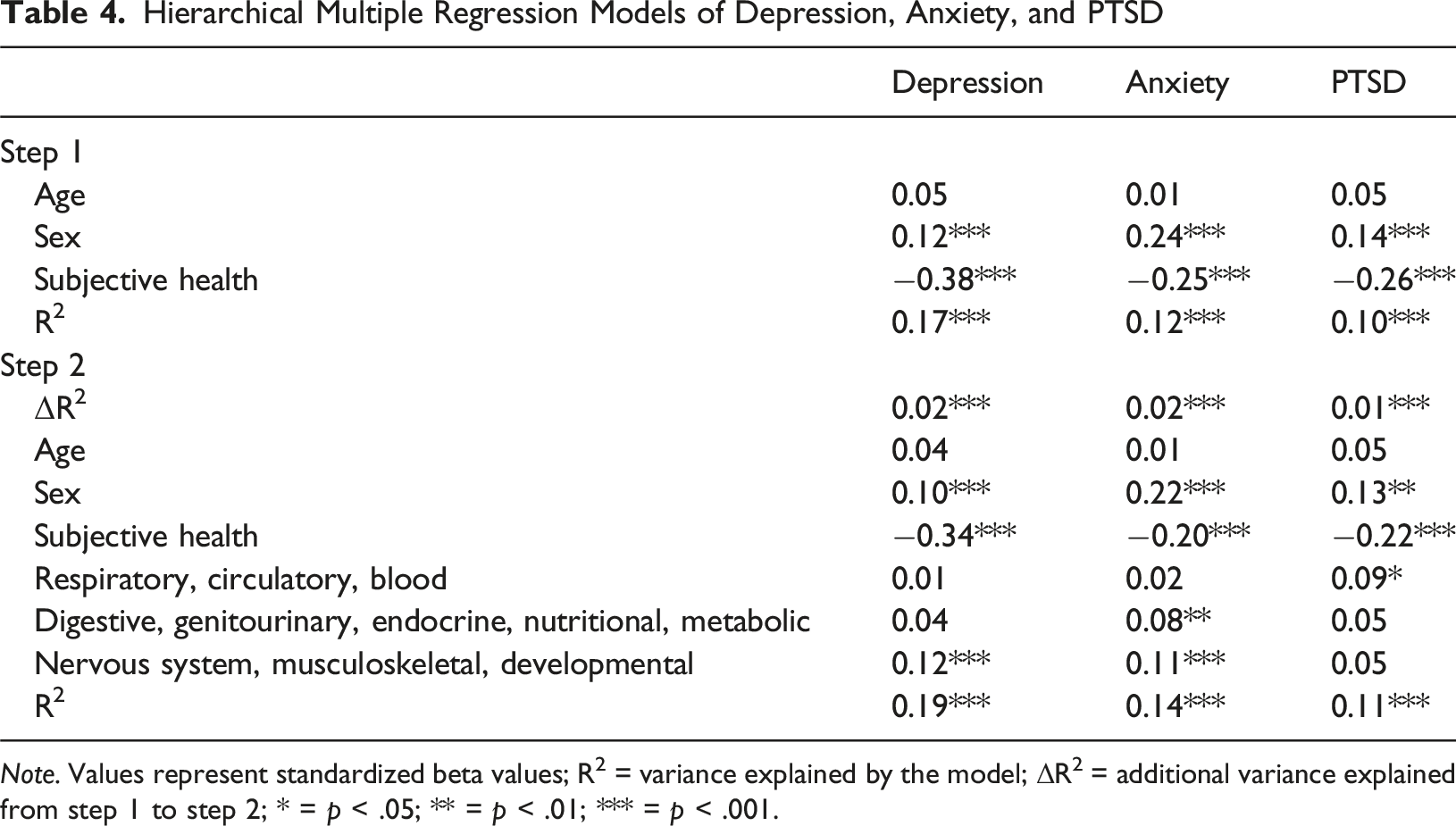
Note. Values represent standardized beta values; R2 = variance explained by the model; ΔR2 = additional variance explained from step 1 to step 2; * = p < .05; ** = p < .01; *** = p < .001.
In Step 1, age, sex and subjective health status explained 17%, 12%, and 10% of the variance in depression, anxiety, and PTSD scores, respectively. In Step 2, the addition of the CMC classifications explained a small but statistically significant proportion of variance in depression (R2 change = 0.02, p < .001), anxiety (R2 change = 0.02, p < .001), and PTSD (R2 change = 0.01, p < .001) scores.
Nervous System, Musculoskeletal, and Developmental Diseases were significantly associated with higher levels of depression (β = 0.12, p < .001) and anxiety (β = 0.11, p < .001); Digestive, Genitourinary, Endocrine, and Metabolic Diseases were associated with higher levels of anxiety (β = 0.08, p = .004); and Respiratory, Circulatory and Blood Diseases were associated with higher levels of PTSD (β = 0.09, p = .041). Of the covariates in the model, being female was associated with higher levels of depression (β = 0.10, p < .001), anxiety (β = .22, p < .001), and PTSD (β = 0.13, p = .003). Better subjective health status was associated with lower levels of depression (β = −0.34, p < .001), anxiety (β = −0.20, p < .001), and PTSD (β = −0.22, p < .001).
Multinomial Logistic Regression Model of Suicide Status
Multinomial Logistic Regression Model of Suicide Categories
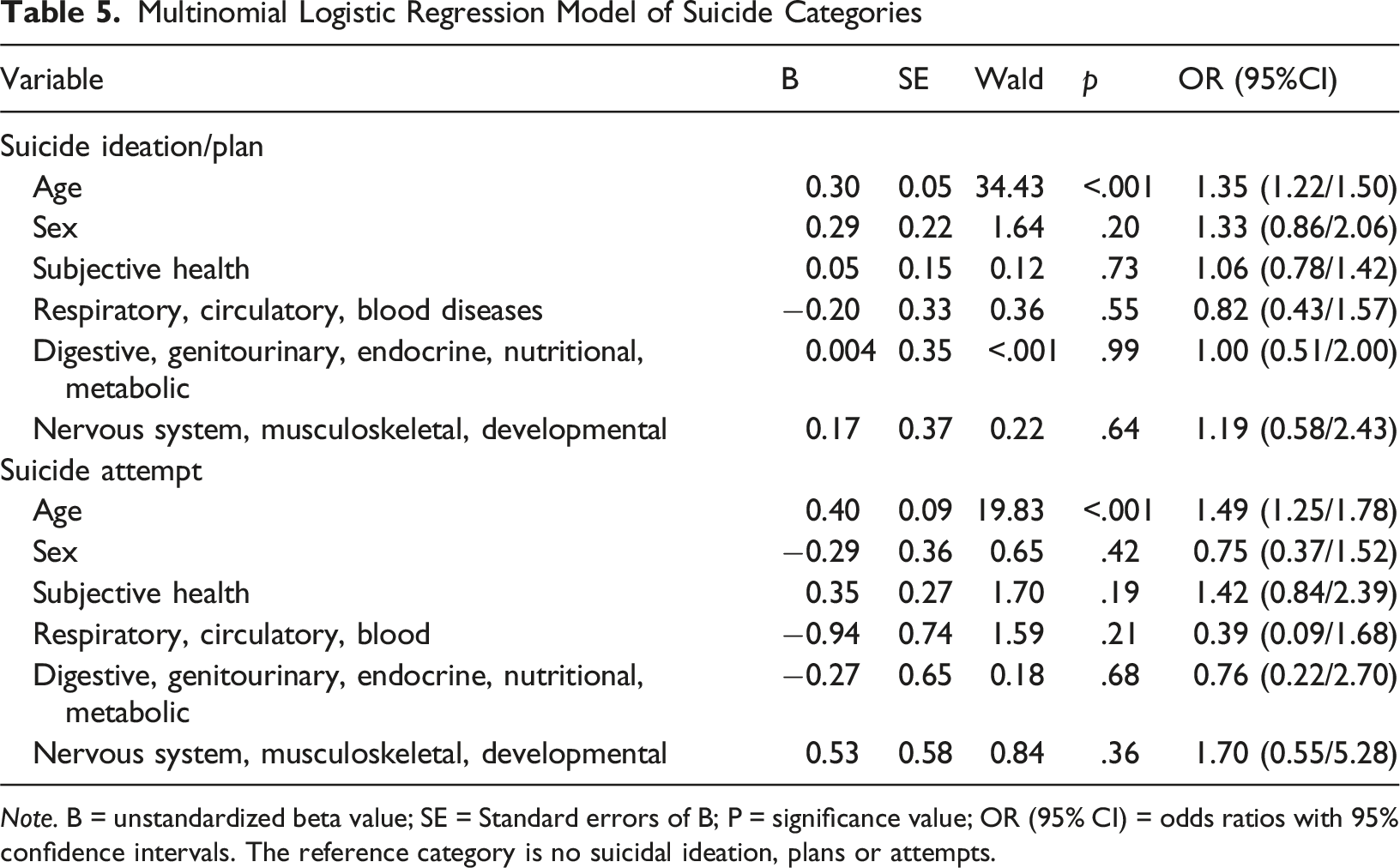
Note. B = unstandardized beta value; SE = Standard errors of B; P = significance value; OR (95% CI) = odds ratios with 95% confidence intervals. The reference category is no suicidal ideation, plans or attempts.
Discussion
The present study used a nationally representative sample of adolescents aged 11–19 living in Northern Ireland to investigate whether having a CMC was associated with higher levels of depression, anxiety, and PTSD, as well as well as having had suicidal thoughts and plans, and having made a suicide attempt, above and beyond the influence of age, sex, and subjective health status. Just over one-quarter of participants (28%) had a CMC, positioning our findings at the upper end of global estimates, which vary between 20% and 30% (WHO, 2025a). Asthma was the most common CMC among participants, with a prevalence of 13.9%. This is slightly above the global estimate of approximately 11% (Yuan et al., 2025). Previous research has found that the Republic of Ireland and Northern Ireland have some of the highest prevalence rates of asthma in the world, where approximately 1 in 12 people suffer with asthma (Asthma Society of Ireland, 2024; Carthy et al., 2020). Given this context, the elevated proportion of those with a CMC in our sample is unsurprising, as asthma alone constituted almost 50% of all reported CMCs. A complex influence of gene-environment factors and interactions likely contributes to the development of asthma (Ogeyingbo et al., 2021), through air pollution, which is relatively poor in Ireland compared to most EU nations, has been hypothesized to contribute to asthma prevalence rates (Tang et al., 2020; Tiotiu et al., 2020).
It should be noted that 23% of children and adolescents living in Northern Ireland live in poverty, compared to 19% in the United Kingdom, and research indicates that poverty-driven health inequalities may be contributing to the higher prevalence of CMCs among youth (Royal College of Paediatrics and Child Health, 2020). It is well-established that adolescents who live in poverty are more likely to experience developmental delays, injuries, malnourishment, acute physical illnesses, and poor mental health, all of which can increase the likelihood of developing a CMC (Adjei, 2021). Northern Ireland also has the highest prevalence of mental disorders in the United Kingdom, which researchers partly attribute to a 30-year political conflict known as the Troubles (O’Neill & Rooney, 2018). Direct and familial experiences of this conflict have been shown to contribute to elevated levels of depression and PTSD in the Northern Irish general population (McLafferty et al., 2018).
Nevertheless, mean levels of depression and anxiety were low in the current sample and reflective of similar research in the general adolescent population in Europe and the United Kingdom (Baron et al., 2021; McKenzie et al., 2018). The mean PTSD score in our sample was low and indicative of mild PTSD symptom severity, based on qualitative descriptors of the ITQ-CA scoring system provided by Baker et al. (2025). Just under 8% of adolescents in this sample had thought about, planned, or attempted suicide. This frequency is lower than estimates from large-scale epidemiological studies, which report ranges from 10% to 20% for suicidal thoughts or plans, and from 4.6% to 16% for suicide attempts depending on the measurement methods employed and study setting (Van Meter et al., 2022; Zygo et al. (2018).
We hypothesized that all chronic illness classifications would be associated with poorer mental health and an increased risk of suicidal thoughts and plans, and attempts. Being female and having lower subjective health ratings were associated with higher levels of depression, anxiety, and PTSD, though age was not. Most of the variances in depression, anxiety, and PTSD were explained by the covariates, with CMC classifications only explaining 1–2% of additional variance in these scores. Subjective health was the variable most strongly associated with mental health difficulties, indicating that it is the perceived impacts on one’s health that are more problematic for adolescent wellbeing than the medical diagnoses themselves. This mirrors previous findings among adolescents (Balázs et al., 2018; Hetlevik et al., 2020), who reported diminished, but significant, effect sizes from CMCs when controlling for subjective health, and stronger effects for subjective health than CMCs. However, we observed several cases, particularly for depression and PTSD, where the effects of CMCs on mental health were rendered statistically non-significant. To our knowledge, no existing study has demonstrated this degree of attenuation of the effect of CMCs among adolescents, though the literature is sparse. Our findings suggest that subjective health may exert a stronger influence on adolescent mental health than previously recognized, at least across the CMC categories used in this study.
Notably, depression and anxiety were weakly associated with Nervous System, Musculoskeletal, and Developmental Diseases, as well as Digestive, Genitourinary, Endocrine, Nutritional, and Metabolic Diseases when controlling for subjective health, and PTSD was associated with Respiratory, Circulatory, and Blood Diseases. The effects we observed between these CMC classifications, depression, anxiety, and PTSD were small – smaller than in existing studies, although effects vary depending on sample, setting, and CMC diagnosis (Eckhoff et al., 2017; Marcev et al., 2024; Quek et al., 2017). These small effects of CMC on mental health variable, which persisted after age, sex, and subjective health were controlled for, may reflect the psychological burden of having a CMC, or they may reflect other mechanisms we did not control for in the current study. For instance, some research suggests that low self-esteem, peer exclusion, and perceived stigma act as mediators between depression and anxiety in adolescents with a CMC (Lacomba-Trejo et al., 2020). Future research could explore these mechanisms in more detail.
In contrast to the above, thinking about suicide or having a plan, and attempting suicide were only associated with increased age. Our findings contradict substantial existing evidence, which consistently identifies adolescents with CMCs as being significantly more likely to experience suicidal thoughts and attempts, and that CMCs constitute an independent risk factor for suicide completion (Iannucci & Nierenberg, 2021). Adolescents with co-occurring mental health difficulties and at least one CMC are considered to be especially vulnerable to suicide (Iannucci & Nierenberg, 2021; Stone et al., 2018). Nevertheless, our findings are consistent with a large body of research that has identified older adolescents as being particularly vulnerable to suicidal thoughts and attempts, with suicide mortality being at least 5 times greater among adolescents than pre-pubescent children (Hua et al., 2023). Ideation-to-action frameworks of suicide explain the transition from suicidal thoughts to attempts in a multistage process that is mediated through exposure to risk factors. These comprise victimization, negative perceptions of identity, thwarted sense of belonging or connectedness, suicide capability, and access to means (Kirshenbaum et al., 2024; Okado et al., 2021), factors we did not account for, but that those with a CMC have been identified as experiencing (Gamwell et al., 2018). Thinking about suicide or having a plan and having attempted suicide were most prevalent among those aged 16–19 years in this study (See supplementary materials for the distribution of suicidality across age).
The present study is not without limitations. Firstly, though the insights provided by the results are valuable for improving the understanding of the psychological difficulties experienced by a general population cohort of adolescents, they may not reflect clinical samples. Secondly, owing to the cross-sectional nature of the data, we cannot infer causality between variables or test mediation chains that may better explain the variances in the mental health variables and suicidality. Third, the short list of covariates included across each analysis means that potentially valuable contextual or individual-level factors were not accounted for. Finally, a methodological limitation of the Northern Ireland Youth Wellbeing study is that it excluded adolescents not living in non-private households (Bunting et al., 2022), for example, those who are homeless or in secure care. Findings do not generalize to these individuals.
Overall, the present study adds to the existing literature by identifying key factors associated with mental health difficulties and suicidality in adolescents. We demonstrated that subjective health showed stronger associations with depression, anxiety, and PTSD than diagnostic classifications of CMCs, with effect sizes stronger than previously identified across the literature. We also identified key CMC classifications that remained associated with depression and anxiety when controlling for subjective health status; these were “Digestive, genitourinary, endocrine, nutritional, and metabolic diseases” and “Nervous system, musculoskeletal, and developmental diseases.” PTSD was also associated with “Respiratory, circulatory, and blood diseases.” Thinking about suicide or having a plan, and having attempted suicide, were both associated with older age. Future research may wish to explore the potential psychosocial consequences associated with these CMC classifications that extend beyond subjective health status to better understand the links between CMCs and poorer mental health.
Footnotes
Ethical Considerations
No ethical approval was required for this study as it included data from previously published studies. No informed consent was needed as this study included data from participants who granted their informed consent.
Author Contributions
IM, PH, and JMP conceived and designed the research and analytic plan. PH sourced the dataset from the original investigators. IM conducted the statistical analyses. IM wrote the manuscript. PH and JMP revised the manuscript and made redrafts. JMP conducted the final review of the manuscript. All authors read and approved the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data available upon request from the corresponding author.