
Abstract
Background
Youth with chronic physical illness (YwCPI) are more vulnerable to developing psychopathology than their healthy counterparts. Families are negatively impacted by CPI diagnosis; however, research has neglected siblings. This study assessed the continuity of symptoms of psychopathology in YwCPI and siblings.
Methods
Data come from MY LIFE, a prospective study that includes five waves (T1 through T5) among 171 YwCPI and their siblings. Two cross-lagged panel models were computed to evaluate continuity of internalizing and externalizing symptoms. Autoregressive pathways measured homotypic continuity by predicting changes in the same outcome across assessments, while cross-lagged pathways appraised heterotypic continuity by testing if one symptom predicted another at later time points.
Results
Significant (p < 0.05) autoregressive paths were detected between all time points for internalizing (YwCPI: β = 0.22–0.78; sibling: β = 0.23–0.75) and externalizing (YwCPI: β = 0.40–0.75; sibling: β = 0.26–0.78) symptoms. In YwCPI, internalizing symptoms at T1 predicted externalizing symptoms at T2, while in siblings an indirect effect was observed from T1 externalizing to T2 internalizing symptoms.
Conclusion
Homotypic continuity was strong and similar for YwCPI and siblings. Patterns of heterotypic continuity were of smaller magnitude and differed between the two groups. The presence of internalizing and externalizing symptoms in YwCPI and siblings support the inclusion of siblings in family-centred care.
Plain Language Summary
Background
Youth with chronic physical illness (YwCPI) are more likely to experience mental health challenges compared to their healthy peers. While research has mostly looked at how their caregivers are affected, this study examines the mental health of both YwCPI and their siblings over time.
Method
Data was collected from 171 YwCPI and their siblings across five time points. Patterns of internalizing symptoms (such as anxiety and depression) and externalizing symptoms (such as aggression and impulsivity) were analyzed. Cross-lagged panel modelling was used to determine how these symptoms of mental illness persist or change over time, and whether one type of symptom could predict the other over time.
Results
The results showed that symptoms of internalizing and externalizing symptoms remained stable across all time points for both YwCPI and their siblings. Patterns of continuity were strong and similar for both groups. However, when assessing whether one type of symptom led to another, different patterns emerged between YwCPI and siblings. Among YwCPI, internalizing symptoms predicted externalizing symptoms at the earlier time points. In siblings the opposite was observed, where externalizing symptoms predicted internalizing symptoms at the earlier time points.
Conclusion
Overall, internalizing and externalizing symptoms were stable over time. Continuity was strong and similar for YwCPI and siblings. The presence of internalizing and externalizing symptoms in both YwCPI and their siblings support the inclusion of siblings in family-centred care approaches to support well-being.
Globally, the prevalence of psychopathology in youth is estimated to be 14% (World Health Organization, 2021). In Canada, the proportion is slightly higher at 18% (Georgiades et al., 2019). It is widely accepted that symptoms of psychopathology among adults are often preceded by a history of symptoms in earlier developmental stages (Costello et al., 2005; Jones, 2013; Kim-Cohen et al., 2003; Mulraney et al., 2021; Pine et al., 1998). An early onset of psychopathology can result in a higher reoccurrence of symptoms and poorer prognosis (Kim-Cohen et al., 2003). For many disorders, the likelihood of remission or recovery is low, resulting in the continuous presence of psychopathology (American Psychiatric Association, 2013). Research has suggested that this course is more stable from adolescence to adulthood than from childhood to adolescence (Hofstra et al., 2000). However, any history of symptoms can lead to lower levels of functioning in adulthood in outcomes related to health, socio-economic status, social relationships and criminal or self-injurious behaviour compared to adults with no history of mental illness (Copeland et al., 2014; Dooley et al., 2023).
Although the course of psychopathology is well documented, the stability of its presentation is more nuanced. When conceptualizing the stability of psychopathology, researchers often refer to homotypic and heterotypic continuity. Homotypic continuity is the progression of an illness with little change in its presentation over time (Angold et al., 1999). This pattern suggests that an observed behaviour in childhood is a predictor of itself in later developmental stages. On the other hand, heterotypic continuity refers to the perpetuation of mental illness with different manifestations over time (Angold et al., 1999). As an example, externalizing behaviours in early childhood and adolescence are associated with a higher risk of successive anxiety disorders and late externalizing disorders in early adulthood (Knappe et al., 2022).
Studies assessing continuity in psychopathology during childhood and adolescence found stronger homotypic effects compared to heterotypic effects over time (Costello et al., 2003; Ferro et al., 2024; Finsaas et al., 2018; Luby et al., 2009; Oldehinkel & Ormel, 2023). However, strong heterotypic effects among common disorders have also been reported in the literature (e.g., the cross-prediction of anxiety and depression) (Benjamin et al., 2013; Copeland et al., 2014; Costello et al., 2003). Yet, symptom-level assessment of continuity suggests that the presence of heterotypic and/or homotypic continuity may depend on the types of symptoms present. Some studies found that with age, externalizing symptoms became more stable compared to internalizing symptoms (Blok et al., 2022; Obsuth et al., 2020). Conversely, approximately half of individuals in the study by Blok et al., that presented internalizing symptoms in late childhood (9 to 12 years of age) reported no symptoms in adolescence (Blok et al., 2022). Interestingly, 91% youths who had the “dysregulation profile” (both internalizing and externalizing symptoms) in childhood remained in one of the mental illness groups into adolescence (i.e., the internalizing, externalizing, or dysregulation subgroups) (Blok et al., 2022). Furthermore, a study focusing on the transition from childhood to adolescence found evidence of heterotypic continuity, whereby externalizing disorders (e.g., attention deficit hyperactivity disorder) predicted other psychopathologies (e.g., general anxiety disorder) over time (Shevlin et al., 2017).
A group particularly vulnerable to psychopathology are youth with chronic physical illness (YwCPI). Cross-sectionally, YwCPI were found to have a 51% greater risk of mental illness, compared to youth with no physical illness; older youth were more likely to develop internalizing disorders, while externalizing behaviours were more likely to be present in younger youth (Adams et al., 2019). Prevalence of chronic physical illness (CPI) during childhood (such as, allergies, arthritis, epilepsy, etc.), is estimated to be between 30% and 50% (L. C. Jones et al., 2017; Van Cleave et al., 2010; van der Lee et al., 2007), and high comorbidity between CPI and psychopathology have been reported. Estimates ranged from 20% to 35% in youth population studies (Ferro et al., 2022; Tegethoff et al., 2015; Wisk & Sharma, 2025), and over 50% in clinical samples (Butler et al., 2018; Canning et al., 1992; Leyenaar et al., 2024). Of the few studies that have assessed the continuity of psychopathology in YwCPI, homotypic continuity has been found for both internalizing and externalizing disorders (Ferro et al., 2024; Reaume & Ferro, 2019). Heterotypic effects were also reported; for instance, behavioural disorders at baseline were associated with attention-deficit hyperactivity disorder, mood disorders, and anxiety disorders over a 24-months follow-up (Ferro et al., 2024). Notably, both studies assessing continuity of psychopathology in YwCPI used a structured interview to indicate the presence of mental illness and on account of their relative lack of sensitivity, such interviews may not be useful for understanding burden of psychopathology (Boyle et al., 2017). Assessing the presence of mental illness using structured interviews typically does not capture subclinical symptoms, which have been shown to impact youth (Crockett et al., 2020; Roberts et al., 2015). Instead, using self-reported checklists to measure symptoms of psychopathology (versus categorical diagnoses), allows for a more nuanced understanding of mental health and changes in psychopathology over time. Evidence suggests that the prevalence of youth, including those with CPI, presenting subclinical symptoms of psychopathology is high and these youth often have compromised functioning and high levels of unmet needs (Burstein et al., 2014; Crockett et al., 2020; Roberts et al., 2015).
The experience of CPI does not impact a child in isolation. Despite calls from researchers to consider sibling outcomes, most research on the impact of CPI on the family unit has only focused on parent outcomes. The scarce research on siblings of chronically ill youth has found that CPI negatively impacted the mental and physical health of siblings (Barlow & Ellard, 2006; Dinleyici et al., 2020). Specifically, siblings of YwCPI were at higher risk for both internalizing and externalizing symptoms compared to population norms and siblings of youth without CPI (Vermaes et al., 2012). In a sample composed of YwCPI and their siblings, the mental health of siblings was either better or worse than the chronically ill child depending on the presence of multimorbidity—the co-occurrence of mental and physical illness (Qureshi et al., 2022). Initial evidence suggests that siblings of YwCPI had lower scores for emotional problems, hyperactivity/inattention, and prosocial behaviours than their chronically ill sibling (Qureshi et al., 2022). However, these findings were not replicated when siblings were compared to youth with multimorbidity, where the siblings had significantly better mental health scores (Qureshi et al., 2022). Furthermore, while siblings of youth with multimorbidity had worse mental health compared to siblings of YwCPI, these effects were negated once family environment factors were incorporated into the model (Qureshi et al., 2022).
Exploring homotypic and heterotypic patterns of continuity in internalizing and externalizing symptoms of psychopathology improves our understanding of symptom pathways by providing further insight on predictors of future symptoms. This enables earlier identification of symptoms of psychopathology, and the adoption of more targeted and proactive approaches to interventions. Although previous studies have assessed the continuity of psychopathology over time, gaps in the literature remain. Firstly, studies assessing the continuity of psychopathology have often included few assessments (Blok et al., 2022; Obsuth et al., 2020; Shevlin et al., 2017), minimizing opportunities to understand patterns of mental illness. To discern the potential nuances in the continuity of psychopathology, multiple assessments over longer periods is needed, especially following significant life events, such as the onset of a CPI (Butwicka et al., 2015; Christiansen & Stenager, 2012). Secondly, only a small number of studies have assessed continuity in YwCPI (Adams et al., 2019; Ferro et al., 2024; Reaume & Ferro, 2019), and fewer studies include siblings (Qureshi et al., 2022), limiting the extent to which risk factors are specific to each of these populations. YwCPI and their siblings have unique vulnerabilities, such as the burden of illness management and worry surrounding prognosis, that may impact the progression of their specific mental health outcomes. Given the daily companionship of siblings and their impact on development, there is growing call to include them in research and family-centered treatment plans (Feinberg et al., 2012). To address gaps in the current literature, the objective of this study was to assess homotypic and heterotypic continuity of mental illness in YwCPI and their siblings over a 48-months period.
Method
Sample
Data comes from the Multimorbidity in Children and Youth across the Life-course (MY LIFE) study (Ferro et al., 2019, 2021). This ongoing prospective study includes five waves of data collection [baseline (T1) and follow-ups at 6-months (T2), 12-months (T3), 24-months (T4), and 48-months (T5)] using self-reported questionnaires and structured interviews from 263 youth and their primary caregiver from outpatient clinics at McMaster Children’s Hospital (Ontario, Canada) (39). At baseline, 171 (65%) youth had an age-matched (±3 years) sibling who was also eligible to participate in MY LIFE. The analysis was conducted using data from the 171 sibling dyads. Youth between the ages of 2 and 16 years with a physician-diagnosed CPI were eligible to participate in MY LIFE. A CPI was defined as one that would last ≥12 months. Furthermore, the illness needed to result in one of the following: functional limitations, dependencies due to their limitations, and/or additional healthcare (Ferro et al., 2019). Youth were not included in the study if they were diagnosed with multiple CPIs or if they or their caregivers were not proficient in English.
Procedure
Eligible families were identified and recruited from the following outpatient clinics: dermatology, endocrinology, gastroenterology, haemophilia, immunology, neurology, respirology and rheumatology. During their visit with a physician, a nurse presented the study to the families and invited them to speak with a research assistant. Once the study was described and they agreed to participate, written permission was provided by the families to be contacted by the research team (Ferro et al., 2019). Research staff conducted interviews at families’ homes or the hospital. In some cases, study packages were sent via mail. In March 2020, all questionnaires were completed via mail and interviews were conducted by telephone due to the public health guidelines in response to the COVID-19 pandemic. Informed written consent was obtained before the initial study visit by the caregivers and children aged ≥16 years, and written assent was obtained for children between the ages of 7 and 15 years. Oral assent was obtained for the children under the age of 7 (Ferro et al., 2019). For the current study, all measures were completed by the primary caregiver.
Measures
Mental Health
The Emotional Behavioural Scale (EBS) measures symptoms of psychopathology based on the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) (Duncan et al., 2019). The scale includes items that measure symptoms of the seven most common psychopathologies among youth, which were grouped into an internalizing and externalizing scale. The internalizing scale includes 27 items that measure symptoms of major depressive disorder, generalized anxiety disorder, separation anxiety, and social anxiety disorder (social phobias). Twenty-five items are included in the externalizing scale, which assesses symptoms of attention-deficit hyperactivity disorder, conduct disorder, and oppositional defiant disorder. Caregivers are asked to evaluate items on a three-point scale (0 = ‘never or not true’, 1 = ‘sometimes or somewhat true’, and 2 = ‘often or very true’) over the last six months. The raw scores of each subscale are summed to describe frequency of internalizing and externalizing symptoms. Plausible scores range from 0 to 54 for the internalizing scale, and from 0 to 50 for the externalizing scale. A higher score corresponds to a greater presence of symptoms. The EBS has good internal consistency among YwCPI (internalizing: α = 0.92, externalizing: α = 0.90) and siblings (internalizing: α = 0.92, externalizing: α = 0.91) in the MY LIFE study.
Data Analysis
A cross-lagged panel analysis (CLPM) was used to assess the continuity of internalizing and externalizing symptoms in YwCPI and their siblings over 48 months using Mplus 8.8 (Muthén & Muthén, 1998). This approach uses a structural equation modelling framework, which feature a combination of techniques that include factor analysis and multiple regression analysis to assess associations between observed variables (Kline, 2016). Maximum likelihood estimation was used to generate unbiased estimates under the assumption of data missing at random.
As recommended, model fit was assessed using comparative fit index (CFI), root mean square error of approximation (RMSEA), and standardized root mean squared residual (SRMR) (Kline, 2016). Acceptable fit was determined based on the following values: CFI ≥0.90, RMSEA ≤0.08, SRMR <0.08 (Brown & Little, 2015; Hu & Bentler, 1999).
Autoregressive pathways were computed to assess homotypic continuity as they predict change in the same outcome over time, while adjusting for previous symptoms of mental illness (Obsuth et al., 2020). The change in behaviour is represented by a coefficient that estimates the direct effect of the predictor on itself (Kline, 2016). To assess heterotypic continuity, cross-lagged pathways were conducted to evaluate the association between a given symptom score (internalizing or externalizing) at earlier and later time points (Obsuth et al., 2020). Auto-regressive paths were included for all available timepoints (e.g. T1–T2, T1–T3, T2–T4, etc.), whereas cross-lagged paths were specified only between adjacent time points (e.g. T1–T2, T2–T3, etc.). Initial models included all cross-lagged paths; however, these paths were not significant and did not improve model fit. Consequently, they were removed from the final models in favour of model parsimony. The same procedure was used to assess continuity of psychopathology in YwCPI and their siblings. Both models controlled for age and sex, and time since diagnosis at baseline, and standardized estimates are reported. Item-level missingness on the EBS was <5% at each time point. Item-level mean imputation was used to compute internalizing and externalizing scale scores. A critique of CLPM is that it conflates between- and within-person effects (Hamaker et al., 2015), consequently, random intercept-CLPM is often preferred. However, CLPM is used in the present study to assess continuity in psychopathology as it is a relatively parsimonious approach, well suited for smaller samples, and are simpler to estimate and interpret. Furthermore, random intercept-CLPM could not be estimated given the sample size.
The method of variance estimate recovery was used to assess how the patterns of continuity of psychopathology for YwCPI differ from their sibling. This approach uses the confidence intervals of parameter estimates from both models and constructs new confidence intervals around parameter differences between the two models (Donner & Zou, 2012).
Results
Sample Characteristics
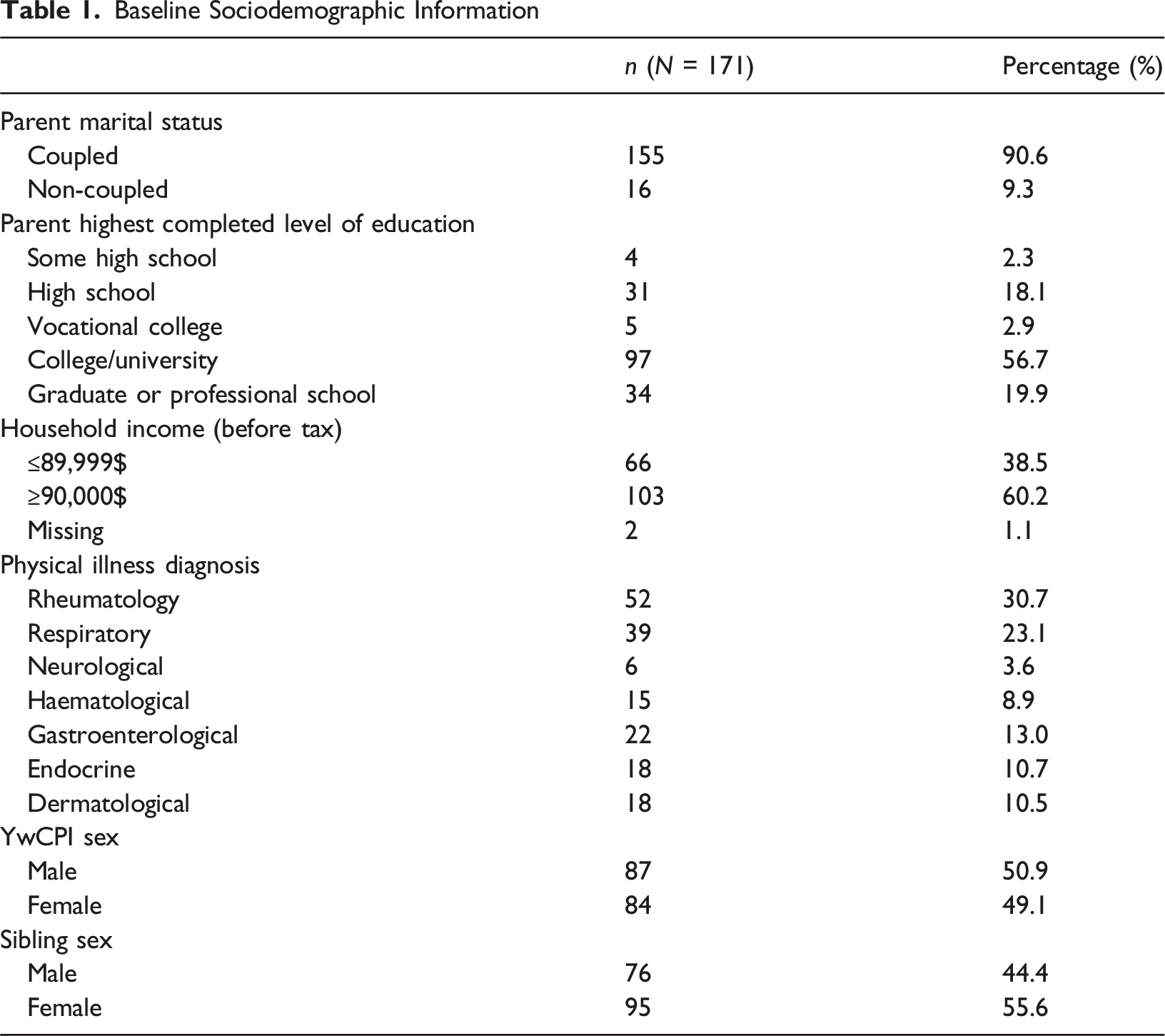
Baseline Sociodemographic Information
Bivariate Correlations for all Study Variables
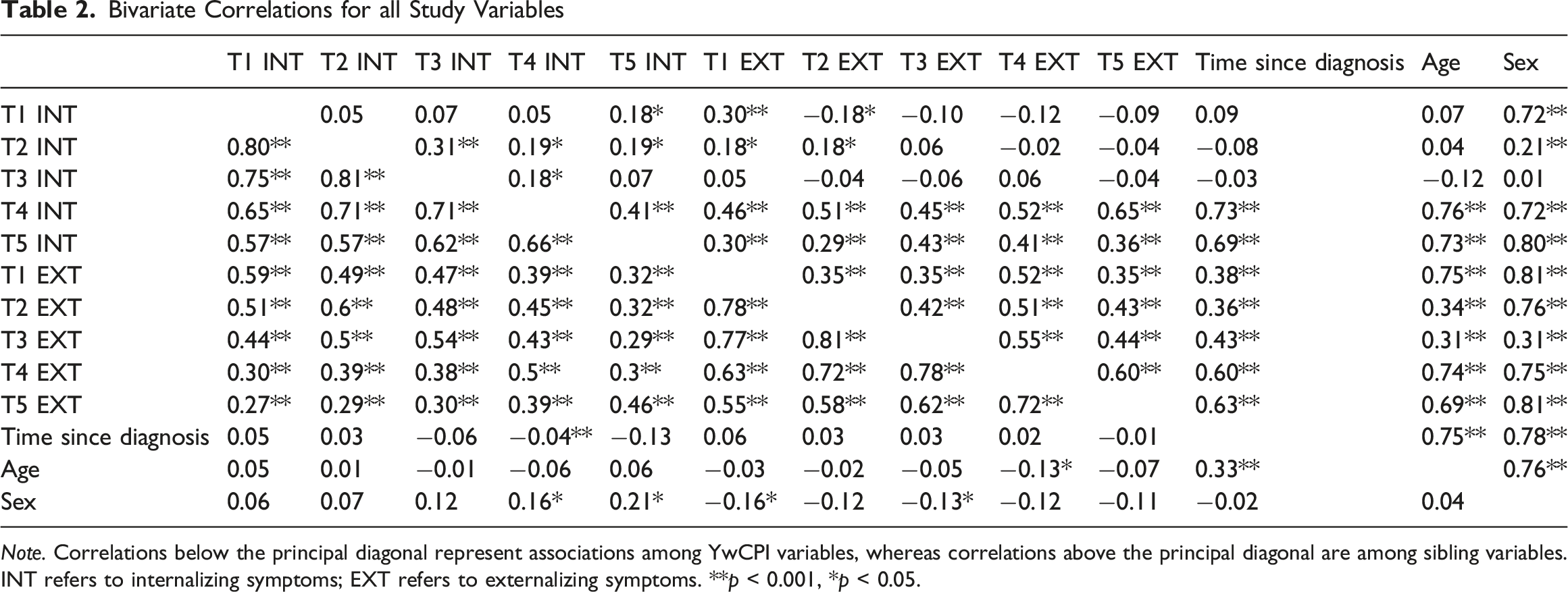
Note. Correlations below the principal diagonal represent associations among YwCPI variables, whereas correlations above the principal diagonal are among sibling variables.
INT refers to internalizing symptoms; EXT refers to externalizing symptoms. **p < 0.001, *p < 0.05.
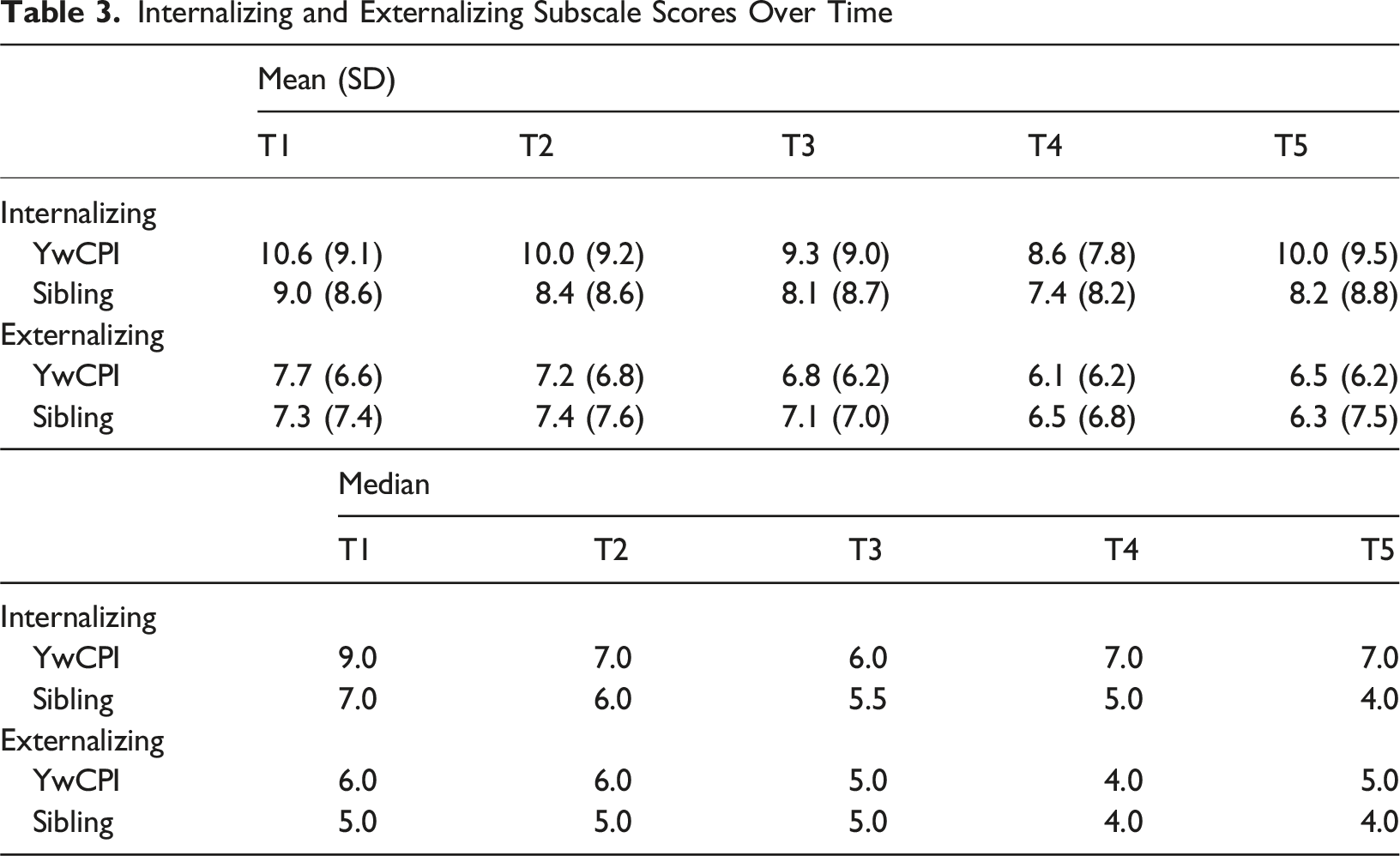
Internalizing and Externalizing Subscale Scores Over Time
Continuity of Psychopathology
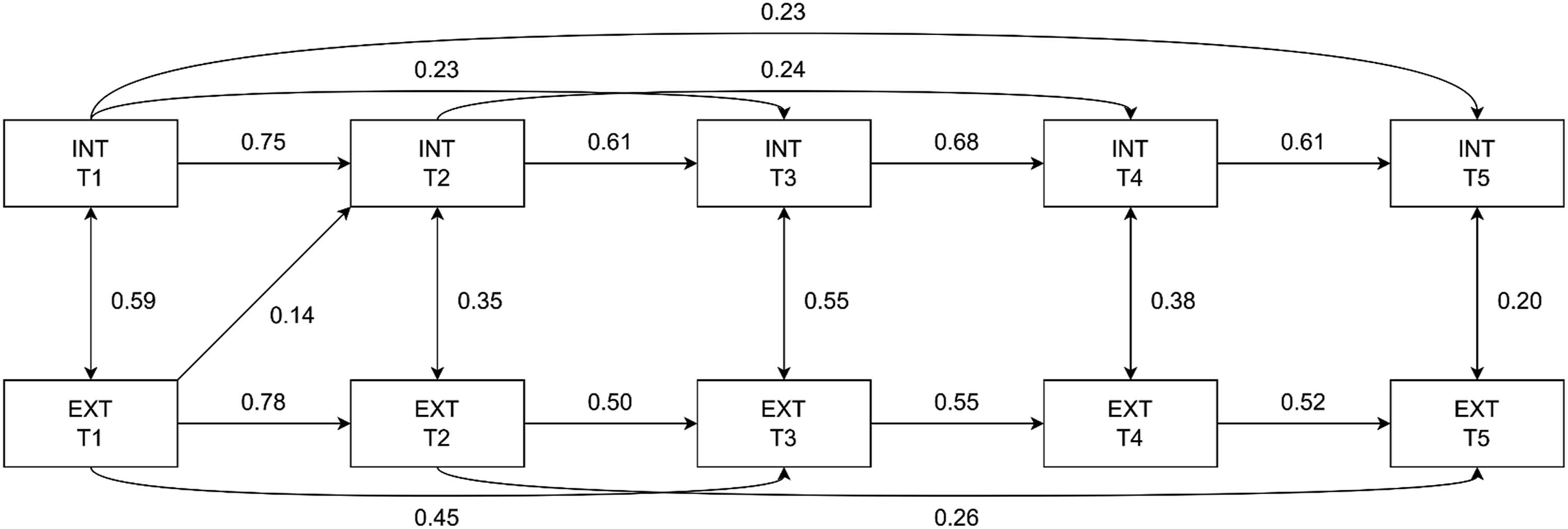
For both models, fit indices meet the threshold for acceptable fit (YwCPI: RMSEA = 0.07; 95% CI, 0.01–0.11; CFI = 0.99; SRMR = 0.02; sibling: RMSEA = 0.06; 95% CI, 0.00–0.09; CFI = 0.99; SRMR = 0.04). Figures 1 and 2 presents all statistically significant (p = 0.05) paths for YwCPI, and siblings, respectively. At each time point, internalizing and externalizing symptoms were positively correlated in both models, with the strongest correlation at T1. Although all correlation coefficients were significant, the magnitudes of the association were mostly small or moderate. Significant autoregressive paths were detected between all time points for internalizing (YwCPI: β = 0.22–0.78; sibling: β = 0.23–0.75 and externalizing (YwCPI: β = 0.40–0.75; sibling: β = 0.26–0.78) symptoms. Few cross-lagged paths were significant. In the YwCPI model, internalizing symptoms at T1 were positively associated with externalizing symptoms at T2 (β = 0.12, p = 0.02). As for the sibling model, a significant indirect path was found between externalizing symptoms at T1 and internalizing symptoms at T2 (β = 0.14, p = 0.01). The magnitudes of these indirect paths between T1 and T2 in both models were small. Comparing the paths in the YwCPI and the sibling model, the method of recovery estimate showed no significant difference in the magnitude of parameter estimates between any of the paths. Cross-lagged panel model for YwCPI. INT = internalizing symptoms; EXT = externalizing symptoms. Standardized estimates of the significant paths (p ≤ 0.05) are presented Cross-lagged panel model for siblings. INT = internalizing symptoms; EXT = externalizing symptoms. Standardized estimates of the significant paths (p ≤ 0.05) are presented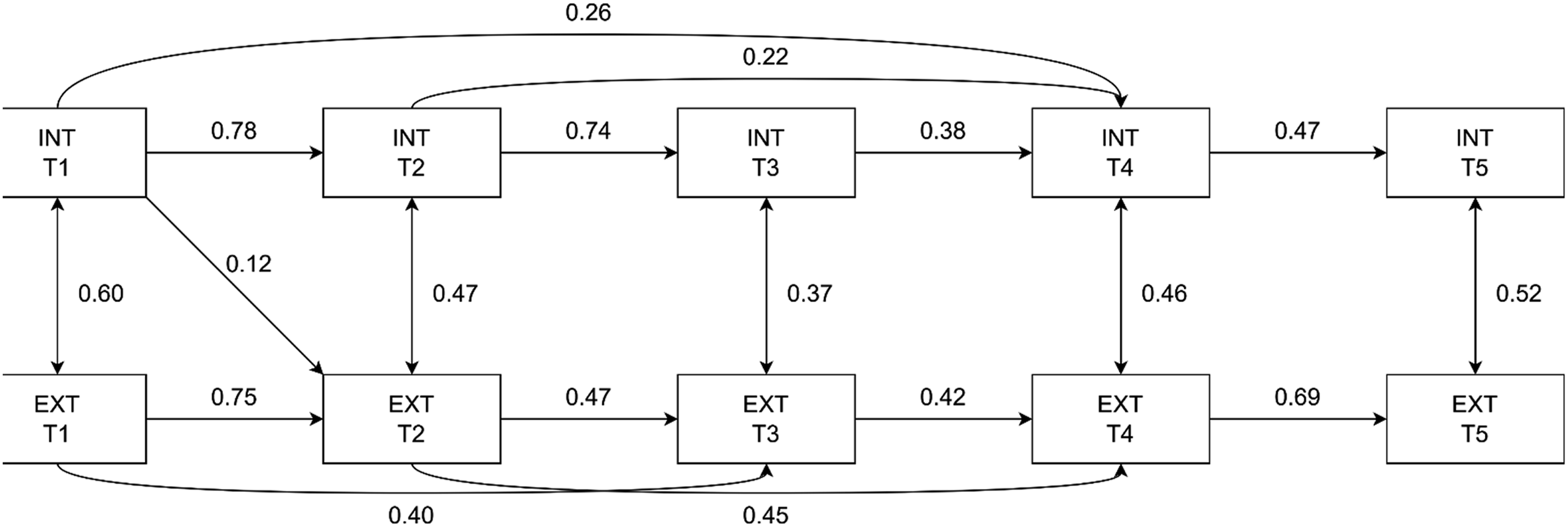
Discussion
This study is among the first to examine the continuity of internalizing and externalizing symptoms of psychopathology over a four-year period, utilizing five waves of data collection in YwCPI and their siblings. Evidence of continuity of symptoms of psychopathology was found in both YwCPI and siblings over the 48-months, aligning with previous findings in the general child population and samples of youth with chronic illness (Costello et al., 2003; Ferro et al., 2024; L. C. Jones et al., 2017; Reaume & Ferro, 2019). Internalizing and externalizing symptoms were mostly stable, although they showed a slight ascending trend over. Relatively large standard deviations of EBS scores over time suggest that internalizing and externalizing symptoms experienced by YwCPI and siblings are heterogeneous. The continued presentation of these symptoms in YwCPI could be due to illness-related factors such as unknown prognosis and perceived illness stigma, which have been shown to influence psychopathology (Ferro et al., 2024). For siblings, factors such as the uncertainty surrounding outcomes for their chronically ill sibling, family functioning, taking on caregiving roles and parental differential treatment could negatively impact their mental health (Ferro & Boyle, 2015; Sharpe & Rossiter, 2002). The small increase in internalizing and externalizing from T4 to T5 symptoms coincided with public health ordinances such as school closures during the COVID-19 pandemic. Evidence suggested that families with a YwCPI may have been particularly vulnerable to the psychological impact of the pandemic (Samji et al., 2022).
Estimates of homotypic continuity were strong and similar for YwCPI and their siblings (Costello et al., 2003; Finsaas et al., 2018; Luby et al., 2009; Oldehinkel & Ormel, 2023). Paths were significant between all adjacent time points, and early internalizing and externalizing symptoms (T1 and T2) predicted symptoms at later time points (T3, T4, T5) in both models. Previous evidence from MY LIFE found that over 50% of YwCPI with anxiety disorders had clinical symptoms that persisted over 24 months (Ferro et al., 2024). Therefore, the stability in internalizing symptoms found in the current study may be driven by symptoms of anxiety. Among YwCPI, factors such as the unpredictable course of the illness, illness severity, family functioning, and stigma could have contributed to the stable presentation of symptoms over time. Given their shared environment, these factors may have also contributed to the stability in internalizing symptoms in siblings. The magnitude of this effect in externalizing symptoms could be due to the nature of the symptoms present. Most of the externalizing symptoms in the sample are associated with ADHD. Homotypic continuity is expected in ADHD as it is classified as a chronic neurodevelopmental disorder which has a strong genetic etiology (Bélanger et al., 2018). The similarity in findings on externalizing symptoms between siblings could be explained by the heritability of ADHD and its significant genetic component (Balogh et al., 2022).
Unlike the previous research that suggests strong heterotypic continuity (Benjamin et al., 2013; Copeland et al., 2014; Costello et al., 2003), we found minimal heterotypic effects. Previous reports on continuity have typically assessed specific disorders via categorical diagnostic tools. Instead, we used a dimensional tool to measure symptoms of psychopathology. Categorical assessments often lack the ability to robustly discriminate between distinct disorders, which some researchers argue partially explains the high rates of psychological comorbidity (Dalgleish et al., 2020). Furthermore, changes in symptomatology over time may be indicative of the developmental progression of psychopathology, rather than the recovery of one disorder and onset of another (Oldehinkel & Ormel, 2023). This is relevant because cross-prediction of disorders is not observed when dimensional measures are used which group symptoms into broader internalizing or externalizing scales. Use of dimensional measures is advantageous because they are not limited by thresholds imposed on categorical measures for the presence (or absence) of a disorder (Chmura Kraemer et al., 2004; Duncan et al., 2019). Dimensional measures also allow for the estimation of subclinical symptoms of psychopathology, the prevalence of which is high among youth, including those with CPI, and can cause substantial impairment and subsequent onset of mental disorder (Burstein et al., 2014; Crockett et al., 2020; Roberts et al., 2015; Shorey et al., 2022).
Few differences were observed between YwCPI and sibling models, likely a function of shared family-level effects on YwCPI and their siblings, as well as the relatively long duration since CPI onset, allowing family members time to adapt to a new normal in which a child has a CPI. The only observed differences between the models occurred from T1 to T2, where internalizing symptoms predicted externalizing symptoms in YwCPI, while externalizing symptoms predicted internalizing symptoms in siblings. The heterotypic effect could be a result of using a caregiver-proxy measure for symptoms of psychopathology. A study assessing the use of caregiver-reported psychopathology in YwCPI found evidence of response shift in parent reports of externalizing symptoms using the EBS (Sajobi et al., 2023). In the sibling model, the shift from externalizing symptoms shift to internalizing symptoms could be explained by the tendency of siblings to develop internalizing symptoms as a result of not wanting to place an additional burden on their parents. This inference is speculative and requires further investigation.
There are few limitations that should be considered when interpreting the findings from this study. First, measures were based on caregiver proxy-reports which tend to have low youth-caregiver agreement and negatively bias child psychosocial outcomes (Cleridou et al., 2017; Oltean & Ferro, 2019; Popp et al., 2017; Salbach-Andrae et al., 2009). However, in the context of having a child with CPI, these caregivers may be more attuned in recognizing symptoms of psychopathology in their children. This hypothesis is speculative, but recent evidence suggests that agreement between parents and YwCPI in assessing child psychopathology improves over time (Parks & Ferro, 2025), thus minimizing potential informant bias. Second, the sample was recruited from a single children’s hospital, was relatively small, and moderately sociodemographically homogeneous. As a result, the generalizability of the findings may be limited. Thirdly, the inclusion of a control group was not possible as the implication of the YwCPI’s health on the family caregiver would remain. Fourth, there is a need to utilize a random intercept-CLPM in future studies as it would provide more robust insights on the longitudinal pathways of internalizing and externalizing symptoms. By disentangling within-person change from between-person differences, this method would allow the identification of both group-level trends and individual-level dynamics, providing a deeper understanding of the continuity on psychopathology over time. The sample size in this study was insufficient to detect effects in a random intercept-CLPM. Finally, future research should investigate how the course of psychopathology differs between siblings in models stratified by birth order (older vs. younger). Older siblings are more likely to take on caretaking roles which can impact family dynamics and their psychosocial outcomes (Kelada et al., 2022).
Conclusion
Findings demonstrated the stability of symptoms of internalizing and externalizing disorders over time. Homotypic continuity was strong and similar in magnitude between YwCPI and their siblings, which support the inclusion of siblings as targets for intervention in family-centred care for YwCPI. Given the persistence of symptomatology, health services should promote early and routine mental health screening for YwCPI and their siblings. Further longitudinal research is needed to assess familial factors, such as family functioning, parental stress and differential parenting in the context of childhood CPI to identify at-risk families and opportunities for intervention that promote the best possible mental health outcomes for all family members.
Footnotes
Acknowledgements
The authors gratefully acknowledge the families, research staff, and hospital staff at McMaster Children’s Hospital who participate in the MY LIFE study. Without their participation this study would not be possible.
Ethical Considerations
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008, and was approved by the University of Waterloo Human Research Ethics Board (#31010).
Consent to Participate
Informed written consent was obtained by all caregiver and children aged ≥16 years prior to the participating. Written assent was obtained for children between the ages of 7 and 15 years, and oral assent was obtained for the children under the age of 7.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The MY LIFE study is funded by Canadian Institutes of Health Research grant (PJT-148602). Mark A. Ferro is supported by the Canada Research Chair Program.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.