
Abstract
Methods to effectively improve socio-emotional functioning by adolescents with developmental language disorders (DLD) are scarce. Current methods to improve socio-emotional functioning in adolescents with other neurobiological disorders seem less suitable, as these methods are highly language based. This study therefore examined the feasibility of the virtual reality (VR) training for socio-emotional skills: ‘InterAction’. The aims of the present study were to (1) examine whether interactive VR is a feasible training method for adolescents with DLD; (2) investigate adolescents’ appreciation of the VR training; (3) examine whether the virtual reality training facilitates the participants’ sense of presence during social practice situations in an interactive digital world; and (4) explore whether adolescents socio-emotional skills improved during the six-session training. A sample of nine adolescents (13–16 years) with DLD reported on their presence in VR contexts and their appreciation toward the VR training. They also completed weekly self-reports on their socio-emotional functioning. Results indicated that ‘InterAction’ was a feasible method to practice socio-emotional functioning with adolescents with DLD. Adolescents highly appreciated the VR training. In addition, adolescents rated the sense of presence as high in the VR training. The individual trajectories showed that improvements in the trained skills varied both between and within participants. The results were also not uniform between the specific skills trained. The findings suggest that interactive virtual reality training may be a promising tool for improving socio-emotional functioning in adolescents with DLD. Future studies should examine the positive indications of this study in a larger sample.
Keywords
Introduction
Adolescents with developmental language disorder (hereafter: DLD) are at greater risk of socio-emotional problems than typically developing (TD) peers. Adolescents with DLD often encounter socio-emotional challenges, such as increased levels of shyness and anxiety in social settings, fewer positive peer relations, and greater risk of victimization, social isolation and depression (Conti-ramsden et al., 2013; Durkin et al., 2017; Smit et al., 2019). These problems in adolescents with DLD indicate the need to improve their socio-emotional functioning. However, methods effectively training socio-emotional functioning by adolescents with DLD are scarce (Arts et al., 2022). Moreover, current methods to improve socio-emotional functioning in adolescents with other neurobiological disorders, often ask to reflect on hypothetical vignettes (Bauminger, 2002; Laugeson et al., 2012). This methods seem less suitable for youth with DLD, as these hypothetical vignettes are highly language based. This study therefore examined the feasibility of a more behaviourally focused interactive virtual reality training (i.e. InterAction). Adolescents with DLD encounter difficulties in their receptive and/or expressive language skills, with no discernible medical origin (Bishop et al., 2017). Expressive language involves the ability to vocalize and convey clear communication through speech, whereas receptive language involves the skill of comprehending and understanding spoken language (Arts et al., 2022). It is estimated that DLD has a prevalence of 5–10% (Law et al., 2000; Van Agt et al., 2011). DLD is more common in boys than girls (ratio 3:1) (Wiefferink et al., 2020).
Social and emotional functioning are closely intertwined. Emotional competence evolves through the process of emotion socialization, wherein children acquire the ability, via social interactions, to identify, comprehend, manage and convey emotions in accordance with the societal norms of their environments (Saarni, 1999). The social domain encompasses the acquisition of insights and skills that enable positive interactions with others (Vissers et al., 2021). Research indicates that in the social domain, ‘social contacts with peers’ was most frequently reported as problematic among adolescents with DLD, which was related to pragmatic language problems (Mok et al., 2014). Adolescents with DLD did not report other aspects of social functioning (e.g. prosocial behavior) as problematic (Conti-Ramsden et al., 2013).
To develop effective training for socio-emotional functioning of adolescents with DLD, it is necessary to understand the etiology of their problems with social functioning. From a neuropsychological perspective (Tomas & Vissers, 2019), the socio-emotional problems of individuals with DLD can be explained by cognitive difficulties in mentalization (Theory of Mind [ToM], Bakopoulou & Dockrell, 2016; Nilsson & de López, 2016) and self-regulation (Executive Functioning [EF], Henry et al., 2012; Sikora et al., 2019) EF can be described as the set of advanced cognitive control processes, to control human cognition and behaviour, in pursuit of specific goals (Diamond, 2013; Miyake et al., 2000). ToM encompasses the capacity to understand emotions (affective), thoughts, intentions, desires and beliefs (cognitive) of oneself (intrapersonal) and others (interpersonal) (Westby & Robinson, 2014).
There are three suggested models to explain the interplay between the language and cognitive problems. The first model proposes that cognitive factors stimulate the development of language. In this way, ToM and EF are proposed to allow children to learn new words (Vugs et al., 2015). In the second model, language facilitates the development of ToM and EF. Following this approach, EF and ToM are positively influenced by the use of self-regulatory speech and conversations about others’ thoughts, intentions and feelings (Milligan et al., 2007). The third model proposes that language and problems in EF and ToM co-occur as a product of the same underlying factors (Bishop et al., 2014).
Well-developed EF and ToM skills are indispensable to adequately interact in social situations. Individuals are expected to understand and predict others’ behaviour and to represent mental states of oneself and others (i.e. ToM) (Arts et al., 2022; Smit et al., 2019). Furthermore, adequate socio-emotional functioning relies on the presence of well-established self-control functions (Arts et al., 2022; Mcquade et al., 2013). For example, individuals need to inhibit their distractive thoughts and inappropriate behaviour (inhibition), demonstrate flexibility in varying social situations (cognitive flexibility), and cognitive capacity to process social information (working memory).
Once socio-emotional problems arise, they may activate a vicious cycle: Less frequent and efficient social dialogue can result in less sufficient social input and practice with the underlying aspects of interaction and communication, that may in turn further compromise social interactions adolescents could have learned from (Vissers et al., 2021). Indeed, by 16 years of age, nearly 40% of individuals with a history of DLD appear impaired in their interactions with peers (St Clair et al., 2011). Adolescents with DLD are more likely to experience bullying victimization and exhibit more difficulties in peer relations and friendships (Conti-Ramsden et al., 2013; Durkin & Conti-ramsden, 2010). In addition, they are less socially confident, experience higher levels of shyness, lower levels of social self-efficacy (Durkin et al., 2017), and show more withdrawal in social situations (Hart et al., 2004), again resulting in fewer learning opportunities within social interactions and socio-emotional problems.
This vicious cycle of deficits underscores the need for an intervention method to improve the underlying components of socio-emotional functioning in adolescents with DLD, and which provides opportunities to practice social interactions with peers.
Practicing socio-emotional functioning
While most intervention methods for individuals with DLD focus on expressive or receptive language abilities, improvement of social skills and the ability to socially interact with peers has received increased attention (Law et al., 2017). Unfortunately, very little data exists on effects of training socio-emotional functioning in adolescents with DLD (Arts et al., 2022). Despite these limited data, several suggestions for improving socio-emotional functioning in individuals with DLD have been made in the literature. First, methods should focus on the linguistic, cognitive, and social communication skills that underlie socio-emotional functioning (Vissers et al., 2015; Vissers & Koolen, 2016). For example, the ability to understand what others say and to formulate an appropriate response (linguistic skills), are necessary to participate in social interaction. Simultaneously, understanding the intentions and emotions of peers (ToM) seems equally important to adequately interact with each other (Bishop et al., 2000).
Second, it is suggested that individuals, to achieve adequate social communication skills, need to learn from many social interactions with different peers, in different situations and with different pragmatic rules (Vissers et al., 2021). Important skills of social interaction include: turn taking, repair of communication breakdowns, responding to questions, topic management skills (Gerber et al., 2012), entering peer groups, and negotiating and resolving conflicts (Timler et al., 2005). To achieve a generalization effect, intervention methods should ensure that these social communication skills are trained in meaningful, natural contexts with peers (Timler et al., 2007).
To achieve adequate cognitive skills it seems also crucial to participate in social dialog (Carpendale & Lewis, 2004; Kuhn et al., 2014). Within this social dialog, adolescents will learn about different perspectives and beliefs of others. This process will provide the basis for the capacity to further adopt and internalize perspectives of others, and thus the development of ToM (Fernyhough, 2008). Studies focusing on improving ToM in children suggest to specifically train the meaning of emotion words (Avila, 2019), to practice mental state verbs (Durrleman, 2020) and analyze video-clips of social interactions to help adolescents recognize conversational cues and perspectives in real people (Westby & Robinson, 2014). For EF, it has recently been suggested that lab-based executive-function training may not be effective, at least not to obtain far transfer to daily social life (Kassai et al., 2019). Based on these recent insights, it has been suggested to train EF in real-life, meaningful, social contexts (Diamond & Lee, 2011).
The potential benefits of VR
Since many individuals with DLD experience bullying victimization and exhibit more difficulties in peer relations and friendships (Conti-Ramsden et al., 2013; Durkin & Conti-ramsden, 2010), practice and support for social behaviour in real-life practice seems difficult to attain within practical and ethical boundaries. Fortunately, the utilization of virtual reality (VR) has been proposed as a possible way to address these problems by emerging participants in realistic social learning experiences. Recent studies showed favorable outcomes (participants and clinicians highly appreciated the VR setting; only reported minor technical issues) of using interactive VR for improving socio-emotional functioning in youth with autism (Didehbani et al., 2016; Kandalaft et al., 2013), and aggressive behaviors (Alsem et al., 2021). Based on these results, virtual reality may also be a promising technique for adolescents with DLD (Arts et al., 2022).
The use of virtual reality training has several advantages. The main advantage is that VR can offer immersive, interactive and dynamic real-life scenarios and enable social interactions remarkably similar to the real world (Veling et al., 2014). This real-world experience may increase the generalization of the practiced skills. Another attraction is that the real-world environment in VR eliminates the need for complex linguistic and mentalizing skills involved in the dialogues about hypothetical social interactions that are common in traditional treatment, so that adolescents with DLD may have more cognitive resources left at their disposal for social reflection and task attention (Brinton & Fujiki, 2006). Moreover, VR provides a safe and reliable environment: adolescents can practice without any chance of victimization, rejection, embarrassment or other risks that are associated with real-life situations (Didehbani et al., 2016). Therefore, it seems well-suited for adolescents with DLD, who have experienced negative social interactions. At the same time, VR is controllable, whereby social situations can be paused, repeated and adjusted to personalized preferences or level (Nijman et al., 2019). In the end, utilizing virtual reality for therapeutic treatment in adolescents may boost their motivation, as most adolescents are intrigued by computers, video games, and innovative technologies (Brezinka, 2014; Didehbani et al., 2016).
In contrast with the proposed benefits, it is also possible that some adolescents may not fascinated by computers and video games. Furthermore, research has historically delved into the negative facets of VR, such as cybersickness (i.e. headache, nausea, dizziness) and technological difficulties (e.g. computer errors). However, these negative symptoms were mainly prevalent during an era of slower hardware and older technology. Recent research showed that clinicians and individuals in recent studies no longer reported these adverse facets of VR (Alsem et al., 2021; Nijman et al., 2020; Verhoef et al., 2021). Nevertheless, it is possible that some individuals do continue to see certain disadvantages in using VR training.
Characteristics of virtual reality
VR is characterized by the experience of a sense of presence (i.e. the sense of being there) in an interactive digital world. The computer generates an image, which is presented to the user by means of VR glasses in a three-dimensional way (Veling et al., 2014). The movements of the user are registered by a tracker and translated into the displayed image in the VR glasses. The outcome is an immersive experience that evokes psychological an physiological responses remarkably to those in the real world (i.e. sense of presence) (Veling et al., 2014). When the possibilities of VR are used to create role-playing and naturalistic situations, it is hypothesized that VR could support generalization of trained skills to real-life contexts (Parsons & Mitchell, 2002).
The sense of presence has usually been considered as the key element of VR (Baños et al., 2004). To achieve this sense of presence, recent studies suggest to make use of immersion and affective content (Baños et al., 2004; Gorini et al., 2011). Immersion refers to the objective description of the used technology (i.e. system resolution, software, speed of images, sound). Affective content refers to the emotional conditions (i.e. narratives, emotions/voice/sayings of the characters) that are added to the virtual environments. Thus, to achieve some feelings of presence in individuals using VR, the training must consist of a combination of adequate technology and affective content.
The present study
Given the feasibility (in other clinical populations) and potential advantages of using virtual reality, we decided to develop an individual virtual reality training to practice socio-emotional functioning. To the best of our knowledge, this is the first study examining the feasibility of a virtual reality training in adolescents with DLD. Hence, we decided to conduct a small-scale feasibility study. The aims of the present study were to (1) examine whether this interactive VR is a feasible training method for adolescents with DLD; (2) investigate adolescents’ appreciation of the VR training; (3) examine whether the virtual reality training facilitates the participants sense of presence in social practice situations; and (4) explore whether adolescents socio-emotional skills increased during the six-session training.
Method
Participants
Nine adolescents with DLD (3 girls, 6 boys), were recruited at two secondary schools for special education of children with communication problems in the Netherlands. These schools are specialized in educating children who are deaf or hard of hearing and children with DLD. All participants met the inclusion criteria for InterAction: age 12–18 years (M = 14.4), an established developmental language disorder and no history of epilepsy. To recruit these participants, all students with DLD (whose casefiles met the studies inclusion criteria and exhibited issues with socio-emotional functioning [<3.0 in at least one category of the IKAN] see Appendix B, Table B1) received an invitation letter to participate in the study. This allowed selected adolescents to voluntarily enroll in the research (i.e. voluntary sampling). Adolescents were recruited until the predetermined sample size was reached. Written informed consent was obtained from 9, out of a total of 15 approached participants and their parents/caregivers (60%). Participation was voluntary and adolescents and parents were assured of confidential use of their data.
Diagnosis
All adolescents were indicated as having DLD by a multidisciplinary team at an audiological center. To obtain a diagnosis of DLD, adolescents had to have (1) no severe hearing problems, as assessed by an audiologist; (2) typical nonverbal intelligence, as assessed by a psychologist; (3) no neurological problems; and (4) severe and persistent language difficulties, impacting communicative efficacy (SIAC, 2023). To determine the severity and content (domains: speech, grammar, semantics, pragmatics) of language problems, a speech-language therapist at the audiological center used the Clinical Evaluation of Language Fundamentals (CELF-5; Wiig et al., 2019), The Schlichting Test for Language Comprehension (Schlichting et al., 2010a), the Schilting Test for Language Production (Schlichting et al., 2010b) and the Peabody Picture Vocabulary Test (PPVT; Schlichting, 2005). Language problems were only ‘severe’ enough for a DLD diagnosis, when individuals (1) score ≤2 SD below average in one of the four language domains, or (2) score ≤1.5 SD below average in two of the four language domains, or (3) score ≤ −1 SD below average in three of the four language domains. This deviation must be demonstrated with at least two language tests.
Procedure
Each participant completed one session, 50 minutes, once a week, for six weeks. Every week, approximately 5 minutes were used to fill in the weekly questionnaire of socio-emotional functioning (see below), 5 minutes to rate how much they appreciated the training and how immersive the training was, and 40 minutes for the InterAction training itself. The InterAction training was performed in a small classroom, at their own schools, during class time, with a table for the complete VR system, where the participant could walk around freely while wearing the VR glasses.
InterAction training
InterAction is a newly developed training method to improve socio-emotional functioning with interactive virtual reality. InterAction consists of six weekly, individual sessions of approximately 40 minutes. All sessions were conducted by the same experimenter. The experimenter has an background in education and behavioral sciences. The experimenter underwent a comprehensive full-day training on the VR technology used in InterAction. The training was facilitated by CleVR (the software company of InterAction).
Content of the interaction training sessions.
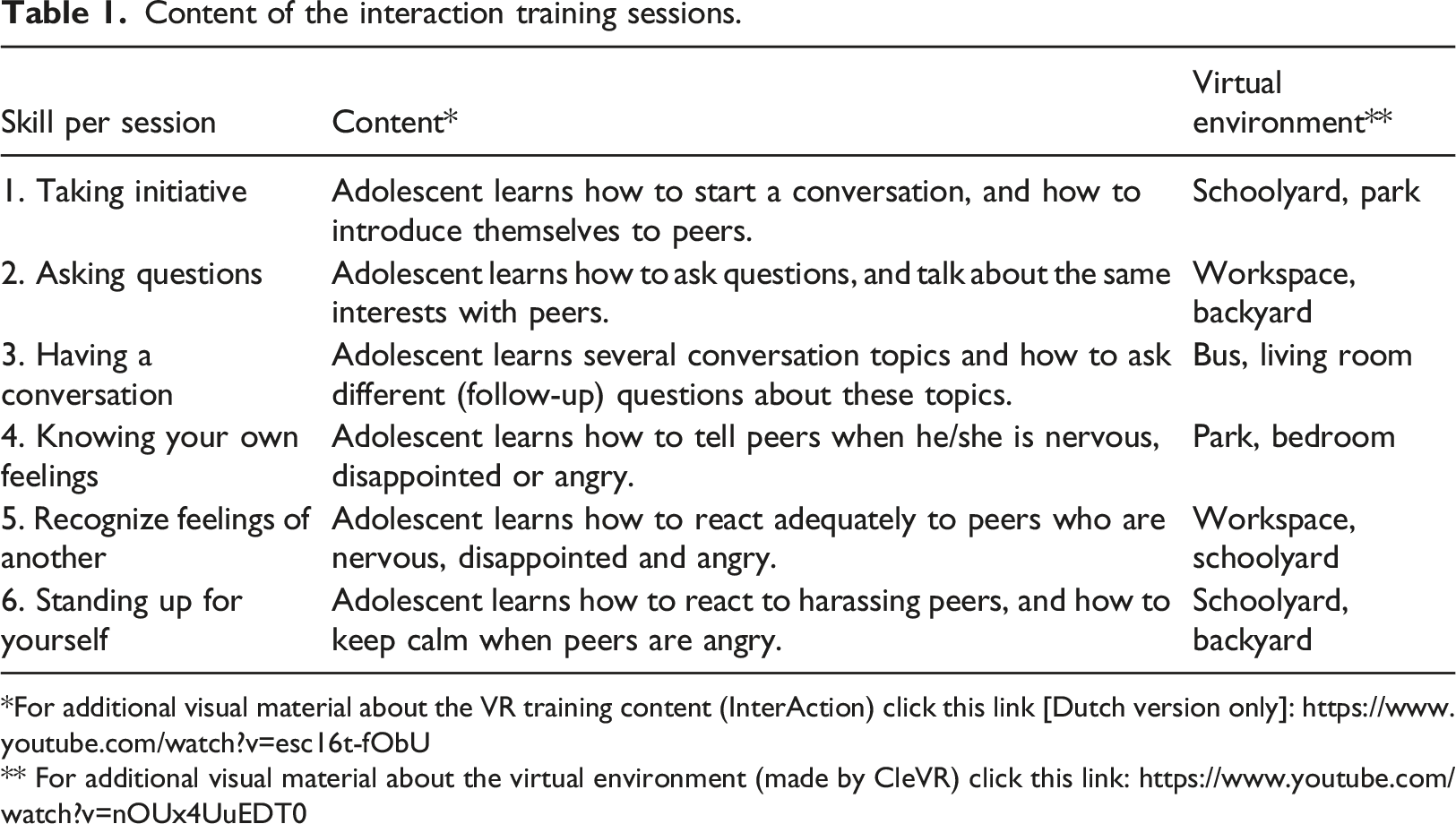
*For additional visual material about the VR training content (InterAction) click this link [Dutch version only]: https://www.youtube.com/watch?v=esc16t-fObU
** For additional visual material about the virtual environment (made by CleVR) click this link: https://www.youtube.com/watch?v=nOUx4UuEDT0
Interactive virtual reality
The content of the VR scenarios and interactive peer interaction was based on several conversations with teachers, speech therapists, psychologist and adolescents with DLD. The InterAction VR environment consisted of a workspace, a schoolyard, a park, a bus and a house (see Figure 1). Within these various environments, adolescents had the opportunity to communicate with digital peers. The VR software was developed by CleVR BV (https://clevr.net). Participants wore an Oculus Rift S (designed by Facebook Technologies and Lenovo), with a resolution of 1280 × 1440 per-eye, with an approximate diagonal field of view of 115. To hear sounds and voices in the VR, participants wore a headphone (3M Peltor WorkTunes Pro). Head tracking was realized by the built-in-sensors (6DOF inside-out tracking through 5 built-in cameras) of the Head Mounted Display (HMD). Virtual reality workspace, backyard, living room, park, bus, and schoolyard.
The VR training world included eight virtual peers, that differed in their haircut, skin color, faces, height, and clothes. All virtual peers were provided with a name and a short narrative about their identity/life (i.e. family, hobby’s). The verbal responses and movements of virtual peers were controlled by the experimenter. We did not script the social interactions, to provide the spontaneity of natural communication (Didehbani et al., 2016). The voice of the experimenter was, via the microphone (using the program MorphVox), transformed into teenage voices of the characters, so the experimenter could spontaneously adapt all characters’ behaviors to the participant’s behavior. The emotions of the characters, during the social interactions, were controlled by the experimenter. Present emotions in the VR were: sad, angry, happy, scared and disgust. By adding names, teenage voices, emotions and narratives about the characters identity/life, we tried to add affective content to the VR training, and thus maximize the sense of presence in participants. During the sessions, adolescents practiced the session’s skill in different digital environments, with different digital characters and different peer emotions. By varying these parameters adolescents may develop flexibility in their thinking (i.e. understand why a social strategy that might work in one situation may not work in another), thus promoting far transfer (Westby & Robinson, 2014).
Measures
The feasibility of InterAction was assessed by investigating several topics, such as: training implementation and suitability, appreciation of the training and preliminary participant results (Orsmond & Cohn, 2015). Specifically for the efficacy of the VR, we also monitored participants sense of presence within the virtual environment.
Training implementation and suitability
The first topic, training implementation, included the usability of the used technology and the occurrence of any technical issues (e.g. tracking problems, difficulties with headset/microphone, computer errors or other unforeseen problems) regarding the VR system. In addition this topic included, suitability, related to training duration, practice time in VR, and the fact if adolescents experienced any negative effects of VR (e.g. cybersickness). To investigate this topic, the experimenter was asked qualitative questions about his/her experience after each training session (e.g. “Have there been any unexpected technical issues? If so, which ones? Can the training sessions be conducted in an ethical manner (e.g. cybersickness) If not, what ethical issues occurred?”).
Appreciation of the training
To measure the second topic, appreciation of the training, the adolescents completed a weekly (self-designed) assessment. Adolescents assessed (paper-and-pencil) their appreciation of the training on two items (i.e. “I liked today’s training” and “I’m looking forward to the next training”) on a 3-point Likert scale (“not – a little bit – yes”). Ratings were averaged over both items.
Sense of presence
Adolescents rated (paper-and-pencil) their sense of presence on three items (i.e. “the VR world is realistic”, “the contact with the VR peers feels realistic”, “During the VR, the exercise had my full attention”) on a 3-point Likert scale (“not – a little bit – yes”). Ratings were averaged for all three items.
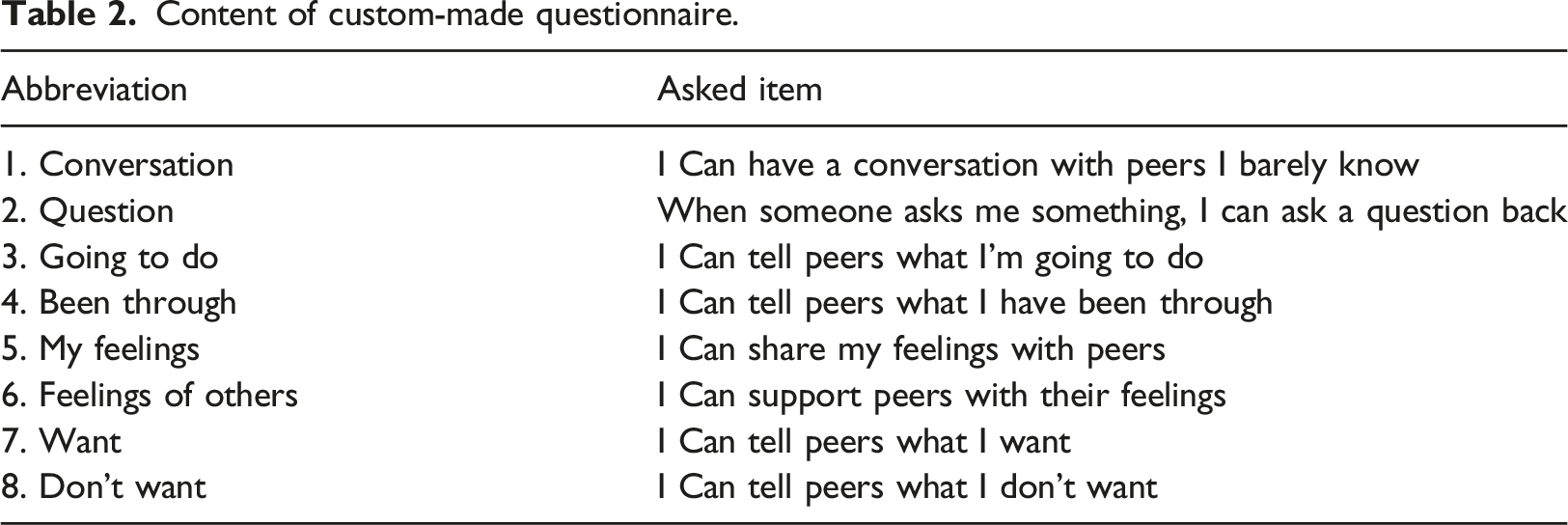
Preliminary participant results
Content of custom-made questionnaire.
Analyses
To describe feasibility, training appreciation, and sense of presence, we used descriptive statistics. To explore training effects on socio-emotional functioning, we evaluated plots of within-person change over time. As our small-sample study was not designed to examine statistical significance of changes over time at the group level, no statistical tests were conducted.
Results
Training implementation and suitability
Within the area of training implementation, the experimenter reported minor technical issues regarding the VR technology (i.e. three sound- and tracking issues; were resolved after restarting the system). These issues could (according to the experimenter) be prevented by starting the VR system before the participants are present; this increases the implementation of the training. In addition, findings reveal that the VR training was suitable for adolescents with DLD in school setting. The experimenter did not report any negative effects of the VR on the participants. Moreover, no uncertainties were reported regarding the assignments in the InterAction workbook. The assignments in the workbook clarified the expectations for the adolescents in the virtual environment (experimenter’s report). During the 40 minutes training sessions, participants practiced an average of 8 minutes and 57 seconds per session in the VR environment with a total average of 52 minutes and 42 seconds per participant over the 6 weeks of training. Finally, the experimenter expressed that a more extended training duration (50 minutes per session) results in more practice time in VR (i.e. the experimenter had to frequently end the virtual conversation due to the training time reached).
Appreciation of the training
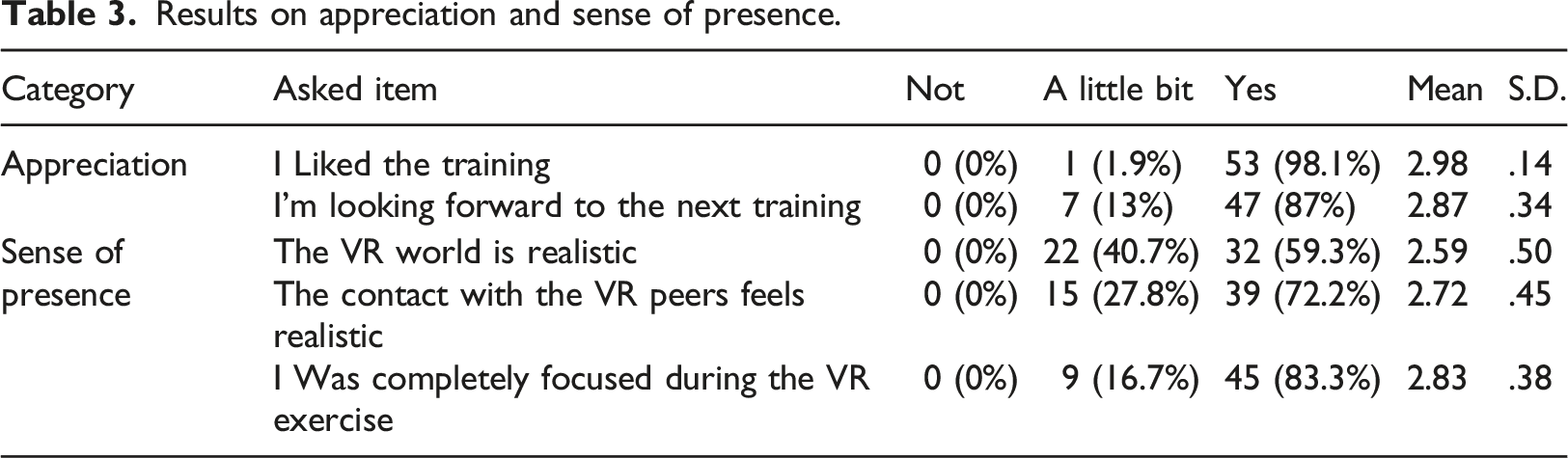
Results on appreciation and sense of presence.
Sense of presence
Adolescents rated the sense of presence in the VR environment relatively high. The scores of the adolescents are presented in Table 3.
Preliminary participant results
We created plots to explore within-person change in the eight assessed socio-emotional skills over the six training weeks, based on adolescent reports (see Figure 2). These plots demonstrate that improvements in the trained skills were not uniform between and within participants. Some participants showed clear change – other patterns were less convincing. For example, the trendlines of adolescent 7 showed an increase over time in only three trained skills, compared to the increased trendlines of adolescent 8 on seven socio-emotional skills. In addition to between-person differences, the results also show within-person differences. For example, the trendlines of adolescent 6 indicated an increase on six trained socio-emotional skills. In contrast, the linear trendlines of the other two skills suggested a decrease in socio-emotional skills over time. This phenomenon occurred for all participating adolescents. Socio-emotional functioning reported by adolescents over weeks. Dots reflect reported scores, and solid lines reflect linear trendlines.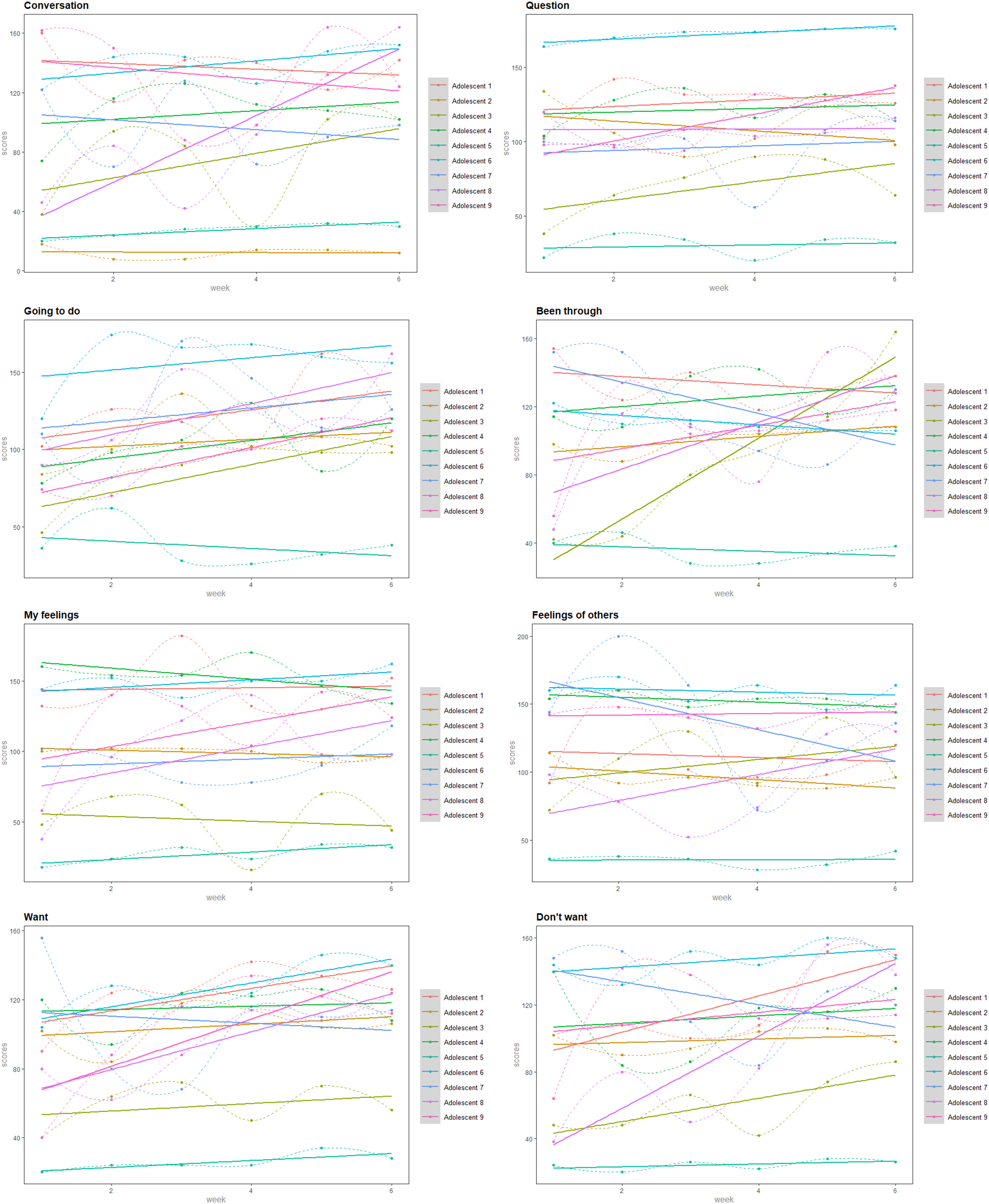
The results of the study were also not uniform per trained skill. This is also visually illustrated in Figure 2. For example, the linear trendlines of eight adolescents showed improvements on the trained skill ‘telling what I’m going to do’. However, the trendline of one participant showed a decrease on this trained skill. This heterogeneity applies to all trained skills.
Discussion
This study assessed the feasibility of an interactive virtual reality training to improve socio- emotional functioning in adolescents with DLD. The first aim of the study was to examine whether interactive virtual reality is a feasible treatment method for adolescents with DLD. Results of this study showed that VR seems a feasible method since (1) adolescents with DLD reported no negative effects over six weeks of training, and (2) there were no technical issues noted during preparation and implementation of the VR sessions. The second aim was to investigate adolescents’ appreciation of the VR training. Results showed that adolescents’ training appreciation was very high, with maximum scores for all sessions by almost all participants. The third aim was to examine whether the virtual reality training facilitates the participants’ sense of presence in social situations. Results indicate that adolescents rated the aspects of the VR as realistic, and that they felt themselves mentally involved in practice moments, contributing to a high sense of presence. The fourth aim was to explore whether adolescents’ socio-emotional functioning improved during the six-session training. Weekly training progress based on self-reports showed that improvements in the trained skills did occur, but were not uniform between and within participant, nor per trained skill.
We assume that the variability in change on the trained skills reflects the complex nature of factors underlying socio-emotional functioning, and associated developmental profiles in adolescents with DLD. DLD is a heterogeneous category that encompasses a wide range of problems and may be associated with very different social problems in different clients (Bishop et al., 2017). The difference in the problems experienced during social situations may contribute to the varying results. Given the diagnostic heterogeneity and complexity of DLD, it seems an important step, for future studies, to focus on individuals in their unique contexts (e.g. measure improvements of individuals, tailored training, personal treatment goals). This can be achieved, for example, by having the adolescents indicate up to 5 problems in socio-emotional functioning that they are concerned about (Chiu et al., 2022). Based on these individually formulated problems, weekly measurements can be used to determine whether the adolescents experience progress on these goals.
In addition, it was notable that the scores within adolescents did not improve or decrease consistently, but fluctuated over the training period. We tentatively suggest that this fluctuation of scores may have been influenced by the experience of positive and negative events in adolescents’ daily lives (e.g. illness). To avoid excessive influence of such fluctuations on evaluations, future studies could add more measurement occasions in both the baseline and intervention period. By adding these datapoints, one specific event will have less influence on the whole pattern of change.
The weekly indicators of social functioning were self-reports of socio-emotional functioning by adolescents with DLD. Since these self-reports were the only measurement technique in this study, interpreting the results warrant caution. It has been suggested that self-appraisal is dependent upon frontal lobe development, which may continue to mature into early adulthood (Hughes et al., 2009). Hence, it is possible that the self-report measure of socio-emotional functioning was not as representative of actual behaviour as observational measures would have been. Indeed, a recent study in adolescents with DLD showed that adolescents rated themselves more positively than did their parents (Hughes et al., 2009). In conclusion, weekly self-reports may not be as valid for measuring social-emotional functioning. Future studies are recommended to add measurements from multiple perspectives (parents/teachers), to gain a more accurate reflection of socio-emotional functioning.
Limitations and recommendations
It is worth re-emphasizing at this point that this is not an efficacy study. Limitations of design (i.e. absence of baseline period or control group) and small sample size limit the generalization of findings. Future studies aiming to evaluate the effects of VR-based training for socio-emotional functioning should examine its impact with a larger sample of adolescents with DLD. Second, because the study lacked a control condition, it is uncertain whether changes in socio-emotional functioning were an actual effect of the training. To determine this, future studies could use control groups or use single-case data that include a control phase (i.e. baseline period) to examine training effects. Moreover, more datapoints obtained during both baseline and intervention periods would minimize the influences of incidental life events on the pattern self-reported functioning over time A third limitation is that the current study utilized self-reports of adolescents with DLD as primary outcome measures. Additional measurements from another perspective (i.e. parents/teachers) are recommended in future studies. Additionally, we did not use a standardized measures to assess presence and socio-emotional functioning, because we were interested in elements specific to our intervention. Furthermore, the items in these questionnaires are not formulated to capture short term changes (as they typically ask for the past year or months). Thus, while our custom surveys were informative for further development of the VR training, it cannot be directly compared with previous research. To evaluate the training outcomes, we recommend future studies to use psychometrically established assessment measures. Finally, the relatively short training period may influenced the outcome of the VR training on socio-emotional functioning. Studies indicate that in the context of cognitive training, increased treatment intensity could lead to more favorable outcomes (Choi & Medalia, 2005). Future studies may extend the training time per participant.
Conclusions
In conclusion, the results suggest that interactive virtual reality is a feasible method for training socio-emotional functioning, that is highly appreciated by participating youth. In addition, VR training meets the need for an interactive training method for youth with DLD. However, as an uncontrolled feasibility study, the results of this study lack statistical power and methodological rigor to draw conclusions concerning the efficacy of InterAction. Given the feasibility and high appreciation of the VR training, a next logical step would be to examine the positive indications of this study in a larger sample, with more tailoring of training to individual needs, a longer period of training, and the addition of a baseline control phase to evaluate effectiveness.
Supplemental Material
Supplemental Material - Interactive virtual reality training to improve socio-emotional functioning in adolescents with developmental language disorders: A feasibility study
Supplemental Material for Interactive virtual reality training to improve socio-emotional functioning in adolescents with developmental language disorders: A feasibility study by Elke Arts, Bram O De Castro, Ellen Luteijn, Ben Elsendoorn and Constance TWM Vissers in Clinical Child Psychology and Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Nederlandse Organisatie voor Wetenschappelijk Onderzoek (4O.5.19630.066).
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
: Example of the training session (InterAction)
Step-by-step explanation of session 3 ‘Having a conversation’.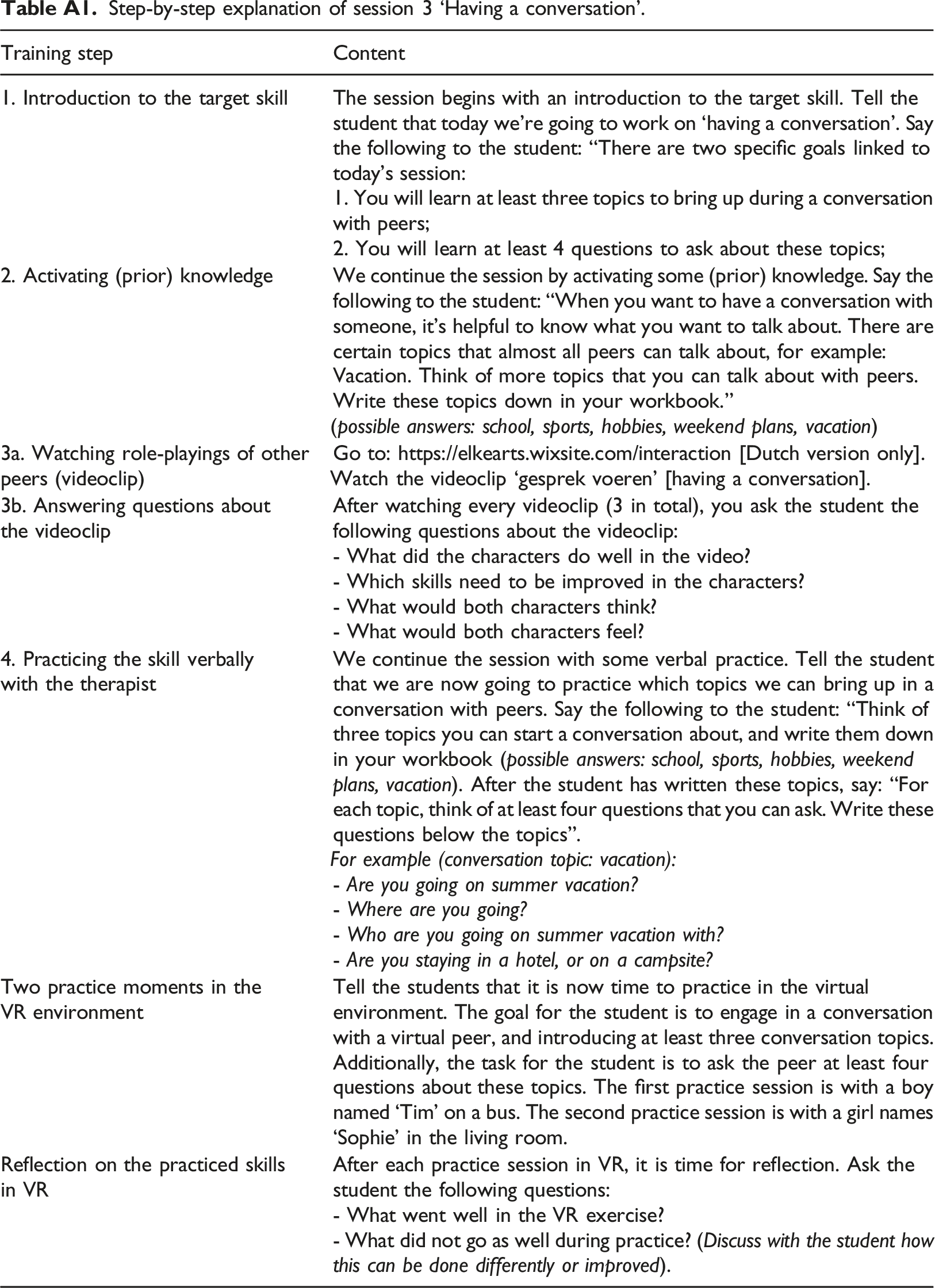
Training step
Content
1. Introduction to the target skill
The session begins with an introduction to the target skill. Tell the student that today we’re going to work on ‘having a conversation’. Say the following to the student: “There are two specific goals linked to today’s session:
1. You will learn at least three topics to bring up during a conversation with peers;
2. You will learn at least 4 questions to ask about these topics;
2. Activating (prior) knowledge
We continue the session by activating some (prior) knowledge. Say the following to the student: “When you want to have a conversation with someone, it’s helpful to know what you want to talk about. There are certain topics that almost all peers can talk about, for example: Vacation. Think of more topics that you can talk about with peers. Write these topics down in your workbook.”
(possible answers: school, sports, hobbies, weekend plans, vacation)
3a. Watching role-playings of other peers (videoclip)
Go to: https://elkearts.wixsite.com/interaction [Dutch version only].
Watch the videoclip ‘gesprek voeren’ [having a conversation].
3b. Answering questions about the videoclip
After watching every videoclip (3 in total), you ask the student the following questions about the videoclip:
- What did the characters do well in the video?
- Which skills need to be improved in the characters?
- What would both characters think?
- What would both characters feel?
4. Practicing the skill verbally with the therapist
We continue the session with some verbal practice. Tell the student that we are now going to practice which topics we can bring up in a conversation with peers. Say the following to the student: “Think of three topics you can start a conversation about, and write them down in your workbook (possible answers: school, sports, hobbies, weekend plans, vacation). After the student has written these topics, say: “For each topic, think of at least four questions that you can ask. Write these questions below the topics”.
For example (conversation topic: vacation):
- Are you going on summer vacation?
- Where are you going?
- Who are you going on summer vacation with?
- Are you staying in a hotel, or on a campsite?
Two practice moments in the VR environment
Tell the students that it is now time to practice in the virtual environment. The goal for the student is to engage in a conversation with a virtual peer, and introducing at least three conversation topics. Additionally, the task for the student is to ask the peer at least four questions about these topics. The first practice session is with a boy named ‘Tim’ on a bus. The second practice session is with a girl names ‘Sophie’ in the living room.
Reflection on the practiced skills in VR
After each practice session in VR, it is time for reflection. Ask the student the following questions:
- What went well in the VR exercise?
- What did not go as well during practice? (Discuss with the student how this can be done differently or improved).
Appendix B: Me-and-the-other-list [IKAN]
To assess the inclusion criteria ‘problems in social communication’ we used the annual school questionnaire [IKAN] (van Hoof et al., 2023), completed by the teachers of the adolescents. This questionnaire consist of 8 categories, with a total of 34 questions. For this study, we used the results of the 4 categories of social communication. Teachers rated each item on a 4-point Likert scale (1 = the student cannot do this yet, 2 = the student can do this with the help of an adult, 3 = the students can do this independently with helpful tools [timer, step-by-step plan], 4 = the student can do this completely independently). Ratings were averaged for all 4 categories. To participate in the VR study, students had to score below the set school norm (<3), in at least one of these categories.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.