
Abstract
Many mental disorders (MD) share common etiology, fuelling debates about the specificity of clinical categories and whether the presence of specific risk factors (RF) can distinguish among them. The study of developmental language disorder (DLD), more specifically, has been further hindered by a lack of consensus regarding its definition. These limitations increase the risk of under-detection and lifelong consequences for affected children. This paper aims (1) to document which individual RF allow differentiating DLD from other MD and (2) to compare the cumulative RF between children with DLD versus other MD. This case-control design study used medical records of a psychiatric sample of 795 preschoolers (mean age 4:11, 75% boys). A logistic regression measured the predictive value of potential RF on DLD. Later first sentences, maternal immigration and family history of language delay were identified as significant in explaining 30% of the variance for DLD diagnosis. An ANCOVA revealed that children with DLD were exposed to a significantly higher number of RF than were children with other MD. Public health policies informed with the knowledge of specific RF associated with DLD, and their cumulative impact, could improve early detection and reduce the cascade of negative consequences associated with DLD.
Keywords
Introduction
Many children struggle with language development in their first years of life. While some overcome their difficulties, about 7.5% of the population will be diagnosed with a developmental language disorder (DLD; Norbury et al., 2016). DLD has repeatedly been associated with psychosocial and cognitive difficulties, which are likely to persist throughout adulthood (Conti-Ramsden et al., 2018; Parsons et al., 2011). Unfortunately, the lack of research attention and public health awareness about this phenomenon may have led to a high percentage of undetected cases of DLD among children consulting for emotional and behavioural problems (Hollo et al., 2014). This could in turn lead to an unfortunate cascade of developmental consequences for children with DLD. Improving its early detection may help ensure that children are provided with appropriate treatment and that they are oriented to language services at a time when they are most beneficial because of neural plasticity (Capone Singleton, 2018).
Mental disorders (MD) are generally characterized by a combination of abnormal thoughts, perceptions, emotions, behaviours, and relationships with others (World Health Organization, 2013). According to the World Health Organisation (2013), MD include depression, bipolar disorder, schizophrenia, dementia, as well as behavioural and developmental disorders with onset occurring in childhood. The authors of a recent meta-analysis (Vasileva et al., 2021) pointed out that while the overall MD prevalence in young children is of 20.1%, this field of research is neglected. DLD is even less known than other MD with similar prevalence, such as attention deficit/hyperactivity disorder (ADHD; Bishop et al., 2012).
Many challenges have hindered the study of DLD. First, several different terms and definitions have been used in the past to designate children with language difficulties, giving rise to significant obstacles in interpreting relevant literature, reconciling disparate results or generating conclusions. A coherent perspective on language problems is also blurred because studies have been conducted on general language development, delays or impairment. For that reason, the CATALISE project assembled an international and interdisciplinary group of 57 experts in order to reach consensus on the terminology to use. This work led to the adoption of the term developmental language disorder to designate persisting language problems that affect everyday life in the absence of biomedical conditions such as intellectual disability (ID) or autism spectrum disorder (ASD; Bishop et al., 2016). This definition will be used in the present paper.
Additionally, risk factors (RF) associated with DLD may remain misunderstood because of common precursors among childhood MD (Mash & Hayden, 2014). Shared etiology has fuelled debates about the specificity of clinical categories, and it remains unanswered whether the presence of specific RF can distinguish between MD. Identification of specific markers could allow for an earlier detection of DLD and for appropriate interventions, therefore improving later outcomes and prognosis. Unfortunately, clinical groups are generally compared to controls, rather than other clinical groups. This limits the comprehension regarding the development of specific MD, raising doubts as to the scientific validity of clinical categories (Caron & Rutter, 1991). Moreover, different MD are not only rarely compared within the same study, but studies also seldom include several RF simultaneously, notably because of insufficient sample size. Furthermore, most samples are population-based or convenience-based, raising important ecological validity issues. Studies conducted on large enough samples of consulting preschoolers are much needed to improve knowledge on MD in general and DLD more specifically.
Building on the recent CATALISE consensus, this case–control study will allow documenting individual and cumulative RF in a large sample of preschoolers referred in psychiatry to verify whether they can distinguish DLD from other MD.
Which early life risk factors are associated with Developmental language disorder?
Personal risk factors
Male gender is one of the most common RF for presenting a language deficit in early childhood in community-based and population-based samples (Brignell et al., 2018; Hammer et al., 2017), as well as for presenting many other MD, such as ADHD and depression (Cree et al., 2018; Wichstrøm et al., 2012). It remains unknown whether male gender is a specific RF for DLD or for suffering from mental health problems in general.
Perinatal difficulties have been identified as RF for language delays in early childhood in a population-based study (Putnick et al., 2017), but not for DLD in a case–control study (Diepeveen et al., 2017). Perinatal difficulties are also strongly associated with ASD and ID, which both include language delays (Schieve et al., 2015). Therefore, it is currently unknown whether this RF is associated with presenting a language delay, a vulnerability to developing a neurodevelopmental disorder in general, or a DLD specifically.
Clinicians use developmental milestones as indicators of many neurodevelopmental disorders (Bellman et al., 2013). A scoping review reports that delays in gesture production, vocabulary or word combination emerged as early predictors of DLD (Sansavini et al., 2021). Yet, other studies observed that children who suffered language or motor delays were likely to subsequently be diagnosed with ADHD (Loughan & Perna, 2013; Shephard et al., 2022). More severe neurodevelopmental disorders such as ASD (Haque et al., 2021) and Down syndrome (Locatelli et al., 2021) are also screened from developmental milestones. Again, further studies are necessary to determine if delays in the acquisition of developmental milestones have a specific predictive value for DLD.
Familial risk factors
Lower maternal education has been linked to DLD (Rudolph, 2017) and to pathological language development in several studies (Hammer et al., 2017; McKean et al., 2015; Muluk et al., 2014). Both the younger (Muluk et al., 2014) and older age of the mother (Hammer et al., 2017) have been identified as risks for language difficulties.
Having a single parent was identified as a RF for language impairment (Brignell et al., 2018), and for other MD in the preschool years (Wichstrøm et al., 2012). As for family rank, being a younger sibling was associated with DLD (Diepeveen et al., 2017). Family history of language problems has often been documented as a major RF for DLD, which was confirmed in a recent scoping review (Sansavini et al., 2021). Yet, this RF also predicts child language development in general (AlHammadi, 2017) which can be delayed in other MD such as ID or ASD.
Foreign language spoken at home has been identified as a RF for language impairment (McKean et al., 2015), but links between multilingual environment and language development are complex to interpret (Andersson et al., 2019).
Figure 1 summarizes the RF associated with DLD and/or with other clinical presentations. The poor convergence in data underlines the importance of clearly defining the type of language pathology studied to generate more specific conclusions. Maternal education, child’s birth order, family history of language difficulties and later acquisition of language milestones have been identified as RF for DLD. Most of these results were obtained in community-based and population-based samples in which comparison between diagnoses are not considered. Thus, it is unclear whether these RF predict DLD specifically, since none of these studies compared clinical groups within their study design. Venn diagram of shared and individual risk factors for developmental language disorder, general language difficulties and other mental disorders.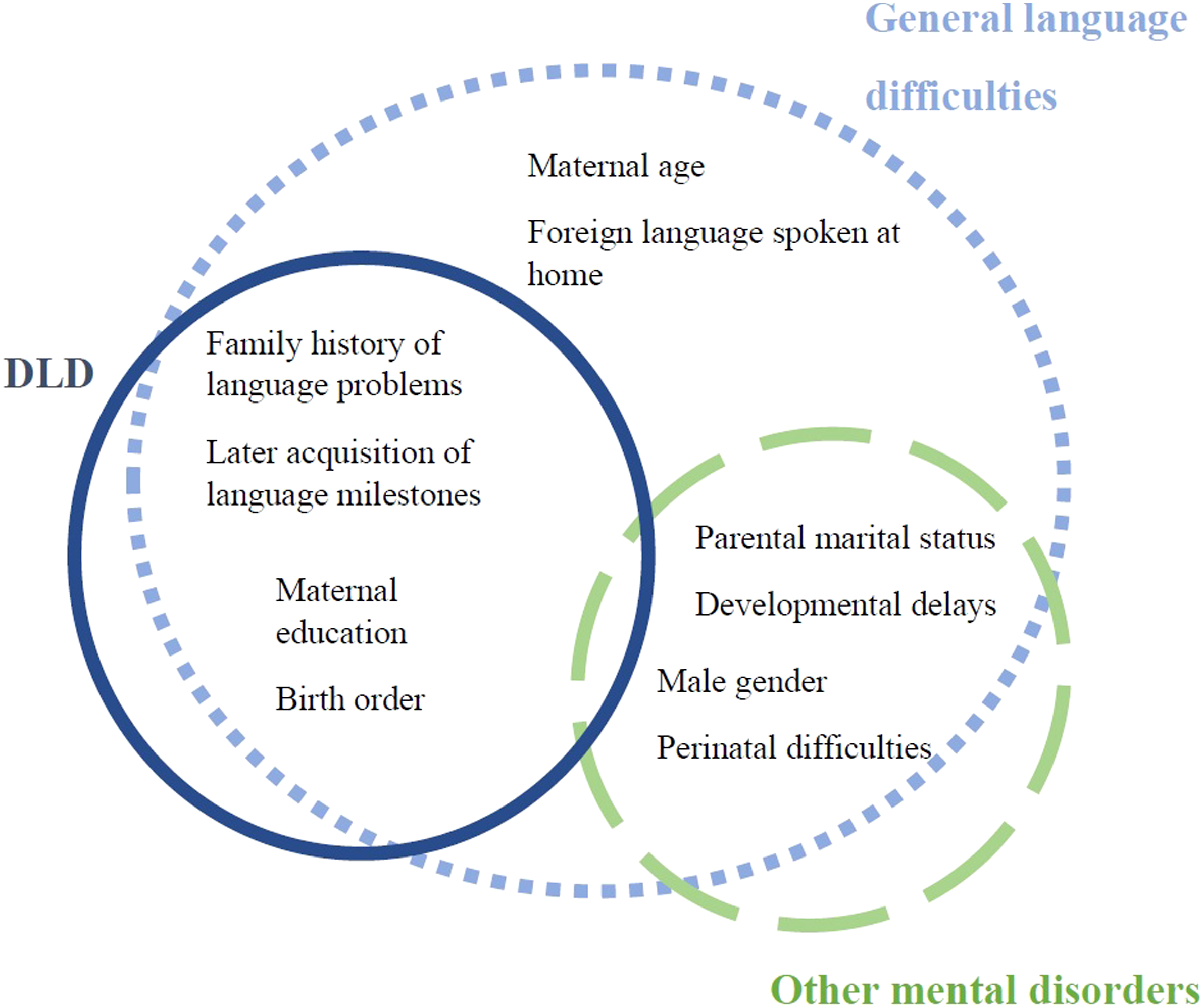
What about cumulative exposure to risk?
Robust findings suggest that exposure to a higher number of risks is associated with worse developmental consequences than the exposure to a fewer number of risks (Sameroff, 2006). According to the neurophysiological model of allostatic load (McEwen & Stellar, 1993), having to deal with several RF undermines a system, which must adapt on several fronts. Multiple risk exposure was associated with language pathological development in infants from a predominantly low socioeconomic status population (Stanton-Chapman et al., 2004). However, the cumulative risk model of development has not yet been applied to the study of DLD. The present study will therefore include a cumulative risk index to verify whether clinical children diagnosed with DLD show more adversity than other clinical children.
The current study
This case-control study has two purposes: it aims to verify, within the medical records of a psychiatric clinic-referred sample of preschoolers, (1) which risk factors (RF) allow distinguishing between DLD and other mental disorders MD, and (2) if children diagnosed with a developmental language disorder (DLD) are exposed to a higher number of RF in comparison to children with other MD.
For the first objective, the respective prediction of personal and familial RF will be verified. Child’s personal RF considered are gender, perinatal conditions (childbirth difficulties and gestational age) and age of acquisition of developmental milestones (acquisition of first words, first sentences, first steps, independent eating, and toilet training). Familial RF are maternal education, maternal age, maternal country of birth, foreign language spoken at home, parental marital status, family history of language delays, and child’s birth order. Across these fifteen factors, only five were previously documented to be specifically associated with DLD. Thus, we hypothesize that these characteristics will predict DLD diagnosis in our clinical sample. Therefore, it is expected that (1) later birth order (2) lower maternal education, (3) presence of family history of language delay and later acquisition of (4) first words and (5) first sentences will distinguish children diagnosed with DLD from children with other diagnoses in our clinical sample.
Regarding the second objective, in accordance with previous findings regarding multiple risk exposures and language pathological development, we hypothesize that the number of RF will be higher in children diagnosed with DLD than those with other MD.
Methods
Participants
Data was extracted from the information available in the medical records of children who consulted at an early childhood psychiatric clinic in a large metropolitan area (Montreal, Quebec, Canada). That clinic was responsible for providing services to all children referred for any developmental, emotional, and behavioral difficulties not primarily related to an ASD diagnosis. The institution’s Research Ethics Board authorized access to the clinical records of all 931 patients assessed between 2000 and 2016. Medical files were reviewed by research assistants to extract psychiatric diagnoses as well as personal and familial characteristics. Children with no psychiatric assessment (n = 38) were excluded from the sample. Participants were then grouped into two categories according to the presence or absence of a DLD diagnosis in their clinical records. The DLD group included 504 preschoolers and the MD group included the remaining 291 children. Following the CATALISE criteria (Bishop et al., 2017), children who were also diagnosed with ID, ASD, hearing impairment, or biomedical problems such as epilepsy or cerebral palsy (n = 76) were excluded from the DLD group, as were children with a speech disorder (n = 22). Figure 2 illustrates the constitution of the final sample of 795 participants. Participants were on average 4:11 years of age (SD 1:6 years) and the sex ratio was of 3 boys:1 girl. Flowchart illustrating the configuration of the final sample.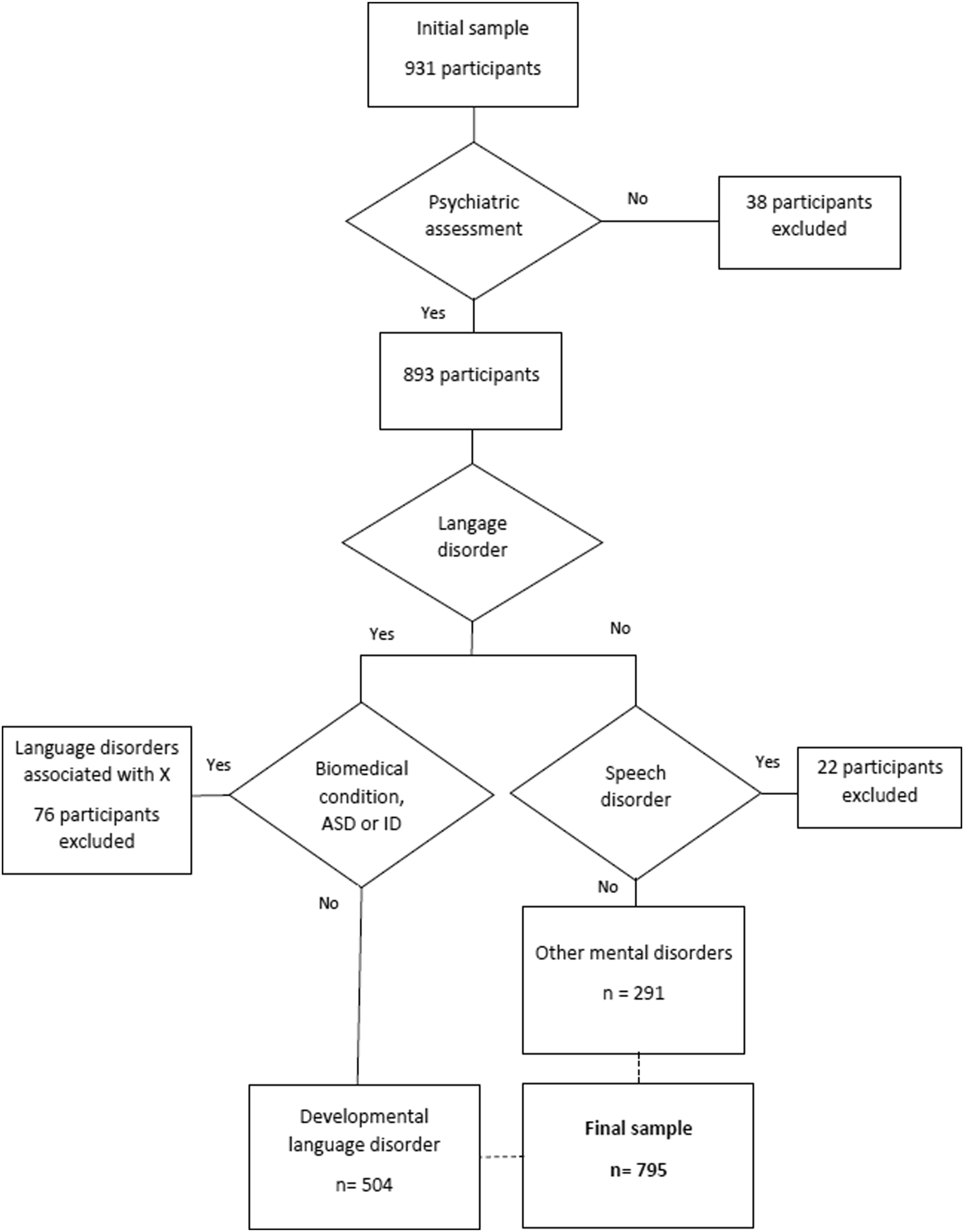
Measures
Psychiatric diagnoses
Accompanied by their parents, children met a psychiatrist who was assisted by another health professional specialized in mental health (i.e., a nurse). Diagnoses issued following a psychiatrist assessment were organized into disorders defined by the DSM-IV-TR’s structure, which was the valid system at the time. Figure 3 illustrates the distribution of disorders according to DLD or other MD status. Some diagnoses were overrepresented in the DLD group. For example, 82% of children in the DLD group also had a developmental coordination disorder (DCD). As a result of the DLD definition, 0% of the children in the DLD group had an ASD, ID or biomedical problems. Bar graph of the diagnosis distribution within developmental language disorder and other mental disorders categories. Note. Eating disorder, sleep disorders, hearing impairment, learning disorder, tic disorders, central auditory processing disorder, sensory modulation impairment and stuttering were not included in the histogram because of their low prevalence in both groups (<5%).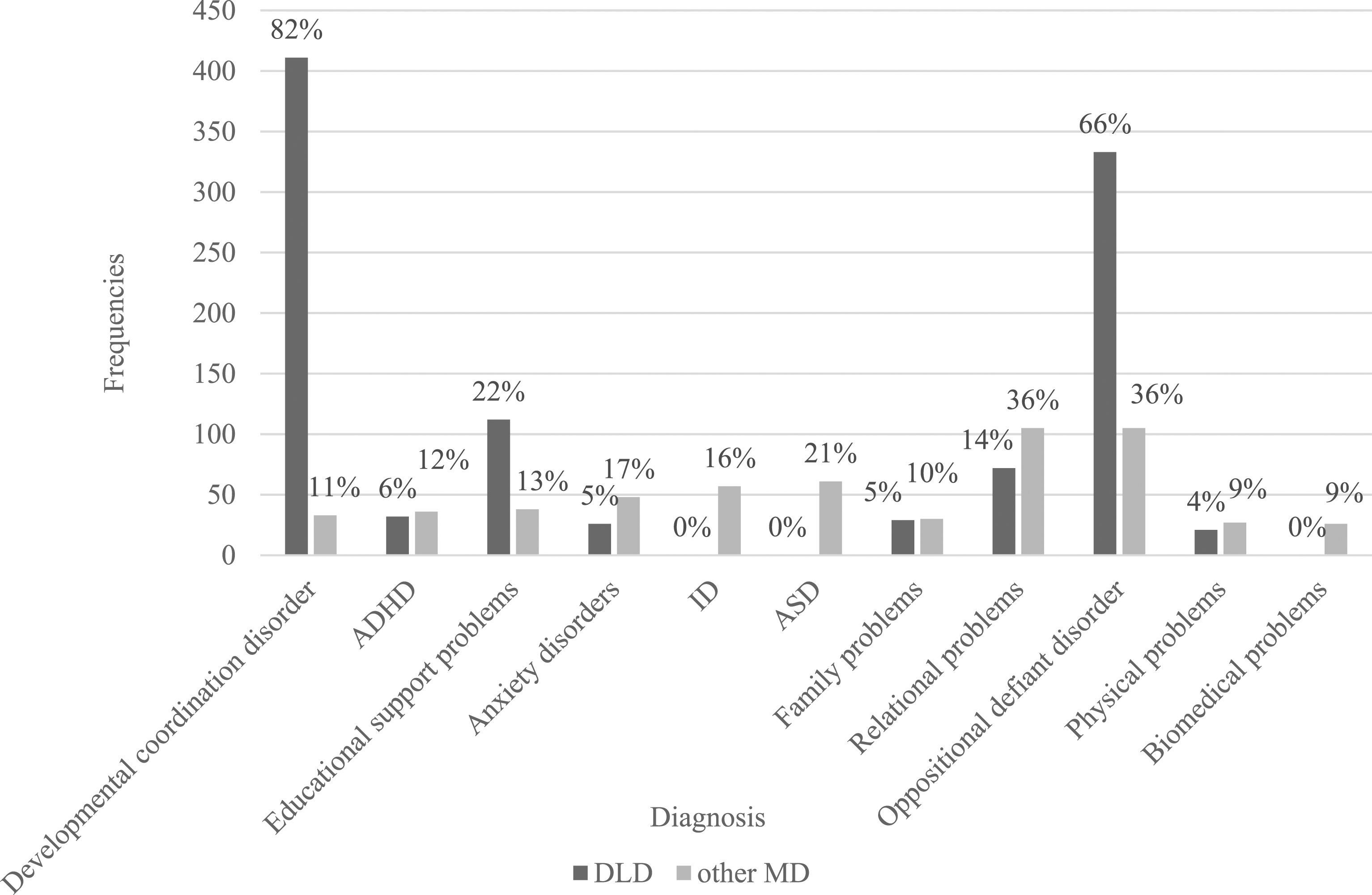
Personal and familial risk factors
The clinical preregistration questionnaire was sent routinely to parents of prospective patients. Information gathered included: child’s sex, child and maternal age, maternal education, maternal country of birth, birth order, parents’ marital status, family history of language delays as well as the child age of acquisition of the following developmental milestones: first words, first sentences, first steps, toilet training, eating independently.
Information about perinatal conditions (gestational age and childbirth difficulties) was obtained from the birth hospital medical records. The percentages of missing values varied from 0% to 45.7% depending on the RF.
Cumulative risk index
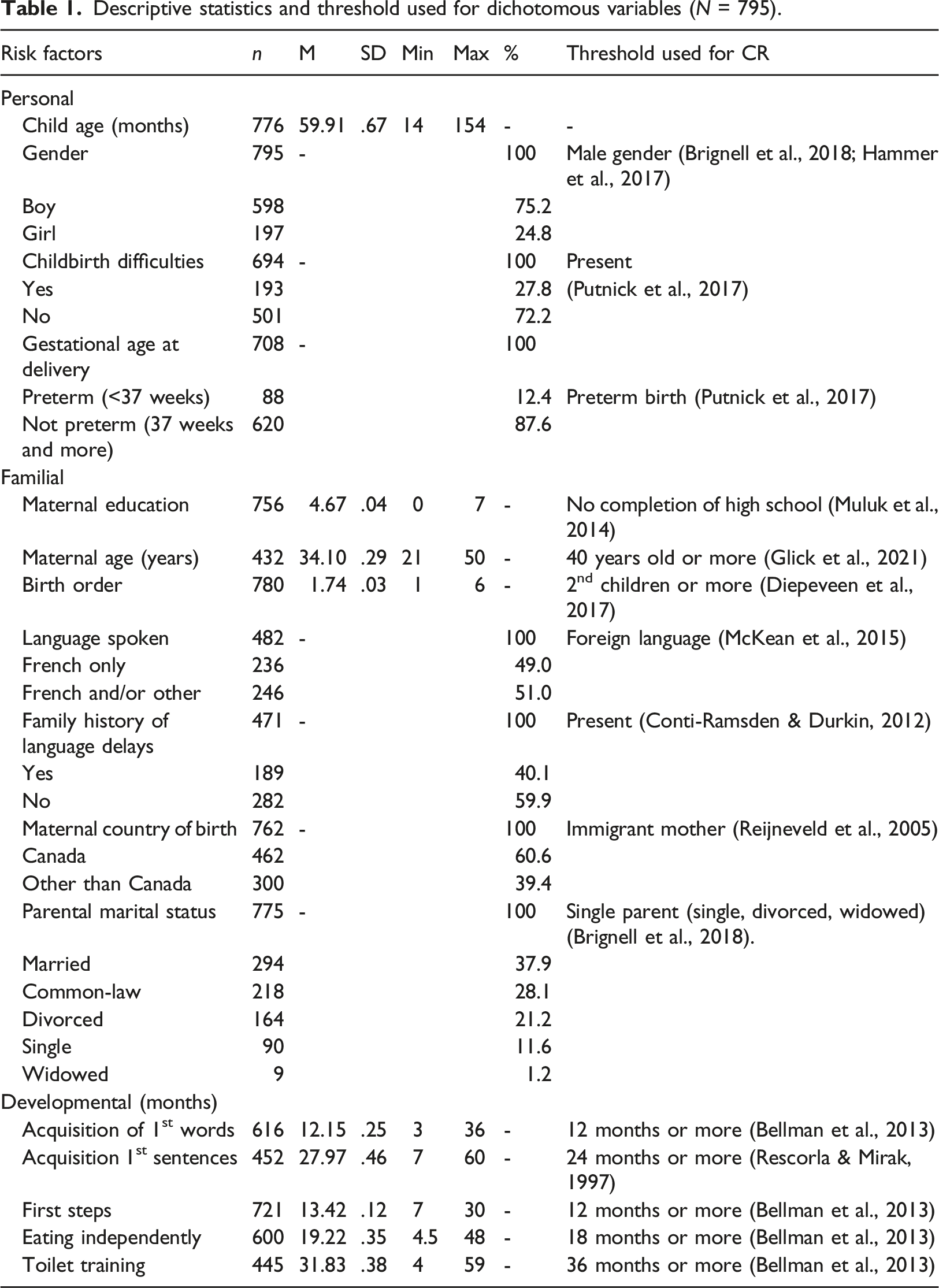
Descriptive statistics and threshold used for dichotomous variables (N = 795).
Data analyses
Analyses were conducted in IBM SPSS Statistics version 27.0. Descriptive statistics were used to analyze individual, familial, and diagnoses variables. Variance inflation factors values indicated no collinearity issues.
According to Field’s (2013) recommended selection procedure, the relationships between RF and type of diagnosis were examined using stepwise backwards logistic regression with elimination of variables that did not significantly contribute to the statistical model (elimination criterion of p-value > 0.1). At each step, the variable that had the lowest correlation with DLD was removed from the model. The final logistic regression (Enter method) measured the predicting value of the remaining RF, with child age as a control variable. Explained variance was measured using Nagelkerke pseudo-R2.
An analysis of covariance (ANCOVA) compared the average number of cumulative risk (CR) exposure between children with DLD and other MD while controlling for the number of diagnoses. Explained variance was measured with partial eta squared.
Results
Descriptive statistics
A total of 63% (504 out of 795) preschoolers were diagnosed with a developmental language disorder (DLD). Table 1 presents the descriptive statistics of the risk factors (RF) and the threshold used to create the dichotomous variable for total cumulative risk (CR).
Logistic regression analyses
Risk factors selection procedure
Stepwise backwards logistic regression reduced the initial 15 RF to six, which were included in the final model: (1) family history of language delay, (2) maternal immigration, (3) child gender, (4) first sentences after 24 months, (5) toilet training after 36 months and (6) independent eating after 18 months.
Final regression model
Logistic regression examining risk factors predicting developmental language disorder (n = 121).
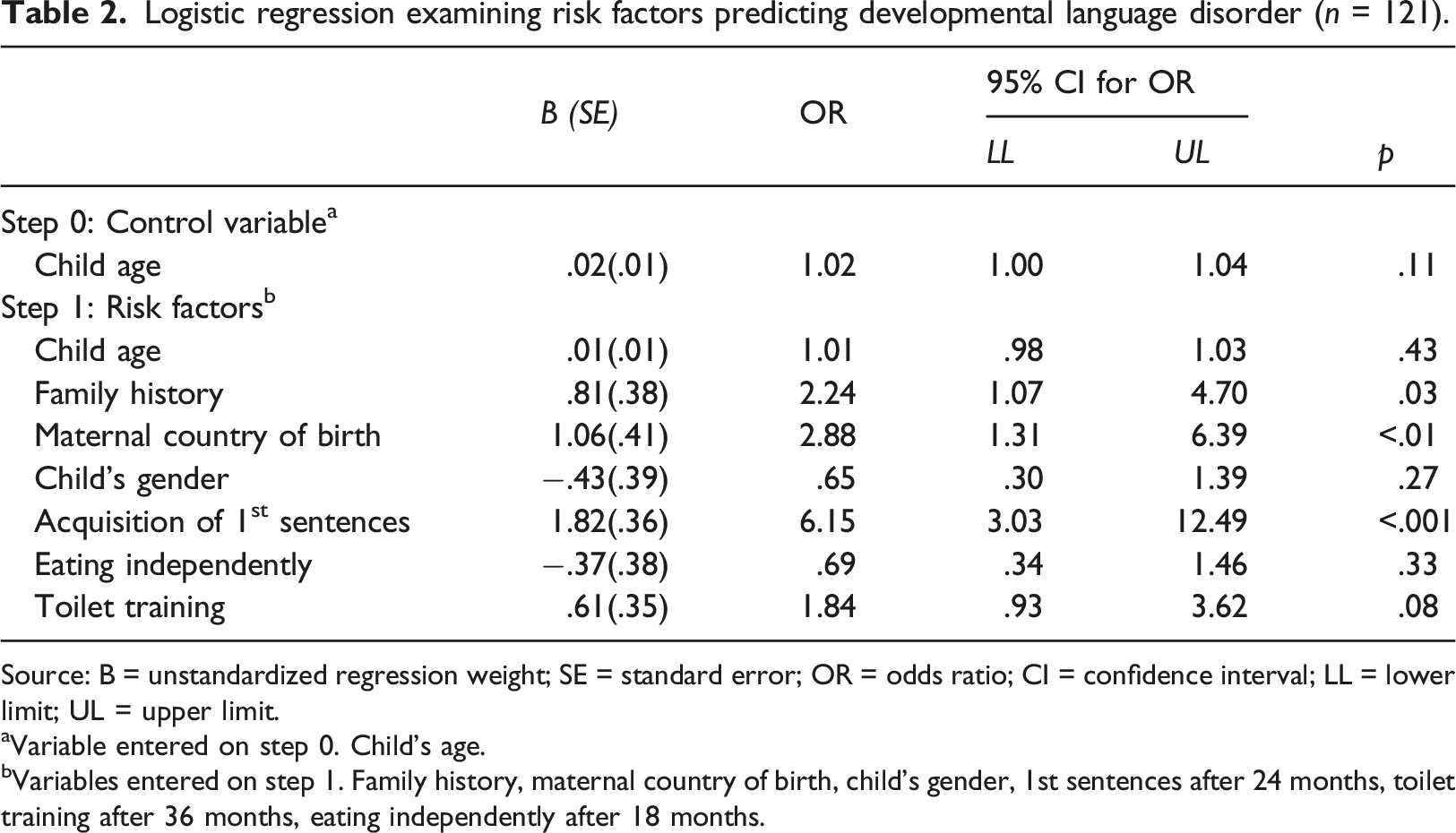
Source: B = unstandardized regression weight; SE = standard error; OR = odds ratio; CI = confidence interval; LL = lower limit; UL = upper limit.
aVariable entered on step 0. Child’s age.
bVariables entered on step 1. Family history, maternal country of birth, child’s gender, 1st sentences after 24 months, toilet training after 36 months, eating independently after 18 months.
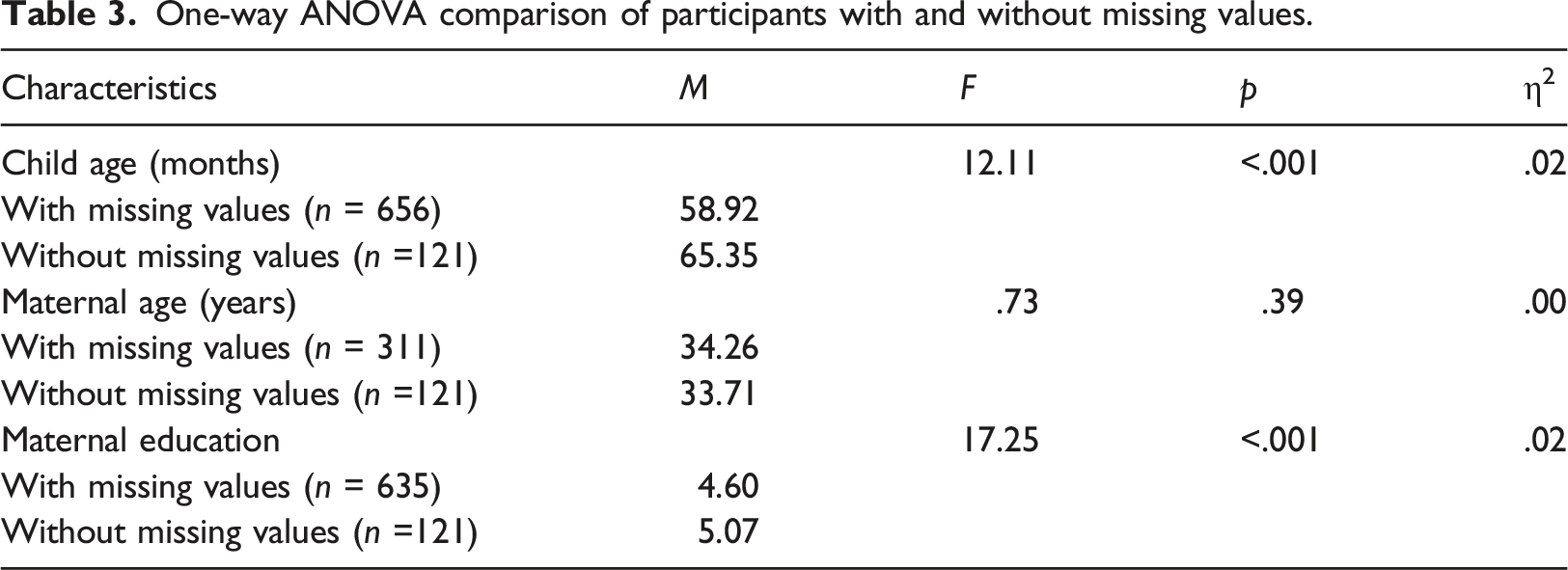
Treatment of missing values
One-way ANOVA comparison of participants with and without missing values.
Chi-square test of independence comparison of participants with and without missing values.

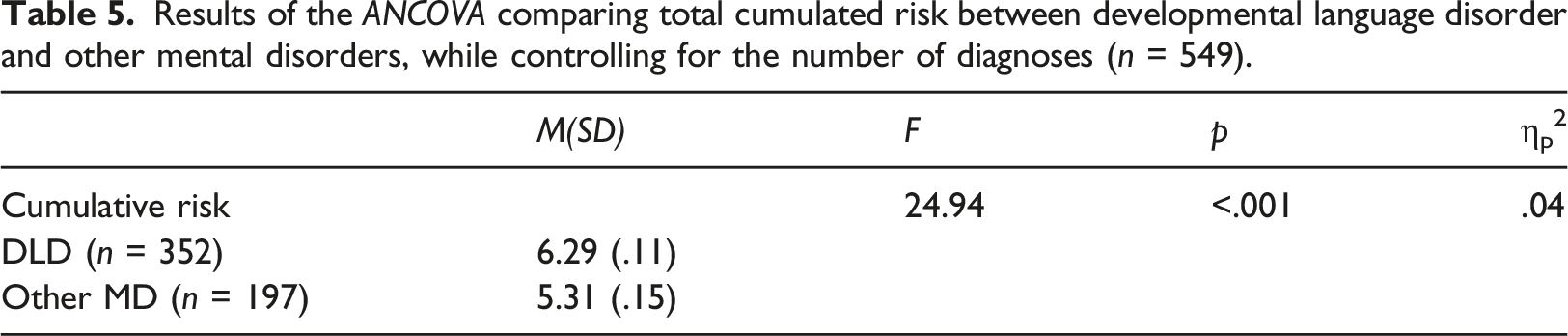
Cumulative risk
Results of the ANCOVA comparing total cumulated risk between developmental language disorder and other mental disorders, while controlling for the number of diagnoses (n = 549).
Discussion
This large case–control study aimed to identify risk factors (RF) that distinguish DLD from various mental disorders (MD) in a clinical cohort of 795 preschoolers.
Developmental language disorder prevalence in this clinical cohort was 63%, which corresponds to the high rate of language disorder previously reported among clinical children (71%; Benner et al., 2002). Developmental coordination disorder (DCD) and oppositional defiant disorder (ODD) were overrepresented in the DLD group, which is congruent with the high rates of comorbidity recently reported in other studies (ODD: Chow & Wehby, 2018; DCD: Flapper & Schoemaker, 2013). Our results do not allow to discriminate the influence of these disorders on DLD, yet they underline the importance of better documenting their co-occurrence with DLD by comparing clinical groups in future studies.
Individual risk factors
The first objective of the present study was to evaluate which RF allowed to distinguish between DLD and other MD. In line with the literature, we hypothesized that (1) later birth order (2) lower maternal education, (3) presence of family history of language delay and later acquisition of (4) first words and (5) first sentences would predict DLD in our clinical sample. This was partially confirmed. The final regression model showed that two of those predictors, later acquisition of first sentences and family history of language delay, represented significantly greater risks for a DLD diagnosis than for other MD. Maternal immigration appeared as the third significant RF for DLD, which was an unexpected result.
Backwards selection procedure did not find perinatal conditions (gestational age and childbirth difficulties), age of acquisition of first steps, maternal education, maternal age, marital status, and foreign language spoken at home to be significant predictors for DLD status. Child gender, later toilet training and later independent eating were retained to be integrated in the final model but were not significant predictors in the final model. Although these RF might play a role in the development of DLD, this suggests that they may be markers for psychopathology more generally, but this hypothesis needs to be verified in future studies.
Acquisition of first sentences was the strongest predictor of DLD status among clinical preschoolers. This finding is consistent with a landmark study of Rescorla (1989), which noted that the absence of word combinations at 24 months was an indicator of persistent language deficits. Thus, age of first sentences merits special attention in the assessment of preschoolers and for referral to specialized language services.
Consulting children whose mother was born in another country and with a reported family history of language delay were respectively 2.88 and 2.24 times more likely to be diagnosed with a DLD when compared to children diagnosed with other MD.
Neither multilingualism at home nor maternal level of education predicted DLD diagnoses within this clinical sample. Lindsay et al. (2016) also reported that children with speech, language and communication needs were overrepresented in ethnic groups at school age. Since the present study cannot explain this overrepresentation, further studies are needed to understand the possible impact of immigration as a factor to consider in the early identification of DLD. Future studies about multilingual family environment should document maternal immigration as a potential confounding variable when studying the relation between multilingualism and language development.
It was expected that family history of language delays would predict DLD diagnosis, since this RF is robustly documented (Conti-Ramsden & Durkin, 2017). The present study replicated this finding even if the comparison group included other diagnoses with a strong language delay component such as ID and ASD.
Therefore, consulting preschoolers who express their first sentence after 24 months, whose mother was born in another country or for whom there is a family history of language delay, are more likely to be diagnosed with a DLD than any other MD. Even though male gender, later independent eating and later toilet training were not significant predictors of DLD in our final model, it remained important to simultaneously measure several RF to identify which are really discriminating or which have a more indirect effect. These RF are documented in the literature but are not specific to DLD among a group of clinical children. Other studies should compare clinical groups to better understand which RF are specifically associated with distinct MD and which are associated with psychopathology in general.
Cumulative risk factors
The second objective was to determine if the number of RF, regardless of the nature of the risk, distinguished DLD diagnosis form other MD in our clinical sample. In accordance with our hypothesis, we found that children with DLD were exposed to a significantly higher number of RF than those with other MD, even when controlling for the number of diagnoses. In other words, identifying specific characteristics appears necessary but insufficient to target at-risk children for DLD in a clinical sample; the exposition to multiple risks must also be considered. The results translate the higher level of adversity that children with DLD are susceptible to have been exposed to. This is the first study to document CR in DLD and future studies are necessary to explain the intensity of risk exposition in this population. In sum, from a prevention perspective, it is important to consider that the effect of some stressors might not be detectable unless they are present in conjunction with other RF. Considering the poor outcomes resulting from DLD (Schoon et al., 2010), the severity of the problems associated with this disorder should not be underestimated.
Limitations and strengths of the study
The current study has limitations, several resulting from relying on data extraction from clinical archives. This method allowed to access an entire cohort of preschoolers who had consulted in psychiatry without attrition but resulted in a high rate of missing values. Representativeness of results was verified by comparing socio-demographic characteristics of participants with and without missing values. Participants of both groups presented similar characteristics, except that children with missing values were almost 7 months older and had mothers with lower education. The missing data could have contributed to the loss of variance in maternal education and maternal age, which could have an impact on their lack of statistical association with the DLD diagnosis. Further studies comparing groups of clinical children could verify if maternal education is a general risk factor in many diagnoses or distinguishes between diagnoses. This exploratory study should be replicated in other clinical settings to verify the generalisation of the results to other samples composed of children with DLD as well as other MD.
The heterogeneity of the difficulties experienced by the children between and within the two groups (DLD and other MD) reduced the possibility to distinguish the effect of RF on other specific disorders. Failure to identify participants’ comorbidities is a very common limitation among studies (Vasileva et al., 2021; Wallisch et al., 2020). Our study is the first to properly document all diagnoses presented by patients in child psychiatry, which better reflects the complexity of this clinical population. More studies that consider comorbid disorders are needed to develop a better understanding of MD and their associated factors.
Finally, to emphasize the dynamic aspect of psychopathology, future research should include both risk and protective factors. Proximal factors could be measured, such as quality of parent-child interactions or daycare attendance. Future studies could also use a transversal criterion, such as the level of language deficit, regardless of the disorder, rather than relying on categories, to verify if similar results are observed.
Despite these limitations, a major strength of our study lies in its ecological validity due to its clinical sample. The sample size and the width of our database allowed to identify many potential RF for DLD in early childhood psychiatry. It also improves our current understanding of DLD by comparing it with other disorders. The integrative and wider perspective about MD proposed in this paper is innovative and allowed to demonstrate that some RF do discriminate among clinical groups, which cannot be verified when no clinical comparison groups are included.
Clinical implications
Better knowledge on specific RF that distinguish among MD can guide clinicians and health agencies in their identification strategies and assessment algorithms in order to improve early detection of DLD. The present study found that speaking first sentences after 24 months old, family history of language delay and maternal immigration, not only distinguish DLD from other MD but account for 30% of explained variance among preschoolers consulting in a psychiatric clinic. Given the strong evidence regarding speaking first sentences after 24 months, which by itself multiplies by six the probability of belonging to the DLD group, clinicians and frontline professionals (i.e. pediatricians, developmental nurses) should systematically document this milestone. In addition, children who have a family history of language delay and who have an immigrant mother should be referred directly for a DLD assessment, instead of waiting for a potential recovery from their difficulties. This contribution is even more important considering that DLD is largely under-identified among clinical populations consulting for emotional and behavioral problems (Hollo et al., 2014). Adding these criteria to the decision-making process would make it easier to identify and allocate services to those children in need of early intervention. In our study, children with DLD were almost 5 years old in average at the time of the assessment. This implies that they spent 3 years with significant language difficulties and without a diagnosis, which can have a dramatic impact in terms of prognosis. Children who start school with this great delay are highly likely to have difficulty catching up (Capone Singleton, 2018). First-line language stimulation programs should be offered to these children earlier, especially since language delay at 24 months increases the risk of low school readiness at 60 months (Hammer et al., 2017). Finally, early detection is critical considering that DLD seems to be itself an important risk factor for presenting other severe mental disorders later in childhood or in adulthood, such as schizophrenia (Mouridsen & Hauschild, 2008). A better understanding of DLD could therefore help prevent other severe mental disorders.
Another important message of this paper is that children with DLD face a high level of adversity and need to adapt on several fronts, which compromise their development. Cumulative risk measures might be another strategy to integrate in DLD early detection programs to help reduce the effects of various RF that cumulatively affect children’s experience (Sameroff, 2006). This area of research needs to be a priority given the poor outcomes for children with a DLD. In conclusion, informing public health policies with the knowledge of specific RF associated with DLD, and the cumulative impact of various RF on affected children, could improve early detection and reduce the cascade of negative consequences associated with DLD.
Footnotes
Acknowledgements
We wish to acknowledge the Hôpital en Santé Mentale Rivière-des-Prairies’ (CIUSSS du Nord-de-l’île-de-Montréal) support in the development and operation of this clinical research study. We address a special thanks to Nicole Smolla PhD for her contribution to the development of the initial phase of this project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Social Sciences and Humanities Research Council of Canada and the Fonds de Recherche du Québec – Société et Culture.