
Abstract
Background
There is growing interest in the use of virtual reality environments (VREs) in psychological treatment and assessment. Most research has focused on the application of VREs in adult psychological disorders with fewer studies focusing on its applicability with children and adolescents. A systematic scoping review was undertaken of research assessing how VREs have been used in the treatment and assessment of childhood mental health disorders to provide an overview of the current state of the literature and identify future research directions.
Method
Systematic searches of online databases were conducted in PsycInfo, PubMed, Embase, Scopus, and Web of Science.
Results
Eleven studies met eligibility criteria and were included in this review, with the majority focusing on VRE interventions for anxiety-related disorders. There is also emerging support for VRE deep breathing training for anxiety, VRE assisted treatment of internet gaming disorder and anorexia nervosa, and VRE assessment of body image evaluation in anorexia nervosa. Most studies were pilot and feasibility studies with only three randomised-controlled trials (RCT).
Conclusions
The current literature shows some promise for the use of VRE assessments and interventions of childhood mental health problems, particularly for anxiety-related disorders such as social anxiety and specific phobias. However, high-quality RCTs are now needed to establish effectiveness of VREs in this population, and how it compares to existing evidence-based approaches, given its promise to improve both engagement and outcomes.
Introduction
Mental health problems in childhood and adolescence are prevalent, with up to half of young people not accessing treatment, and for the majority of those that do, not maintaining contact for the duration required for standard treatment (Sawyer et al., 2019). As such, it is important to continue to develop effective, therapeutically engaging, accessible assessment and treatment and virtual reality environments (VRE) have the potential to contribute to all of these areas. Advances in VRE technology have led to increased interest in its use across a range of conditions, including mental health.
VRE refers to a computer-generated simulation of a three-dimensional environment that is experienced through sensory stimuli. Facilitated via the use of tracking technologies, physical user movements are replicated within the simulated environment to provide user perspective within the virtual space, thus providing a sense of presence and embodiment. VRE is most commonly experienced through head-mounted displays (HMDs) and cave automatic virtual environment (CAVE) systems. HMD based VREs differ to that of CAVE systems, in that HMDs often provide increased interpupillary distance (IPD) customisation and higher capable screen refresh rates. This is due to CAVE VREs being projected onto the walls of a room and consumed using 3D glasses, whereas HMD VREs are visualised using small screens and lenses within the device itself.
This VRE technology present an opportunity to expose children to simulated scenarios in a controlled clinical setting, where clinicians can assess behaviour and guide desired behavioural responses. Another potential benefit of VREs is the accessibility clinicians could have to various simulated environments that would mitigate difficulties with conducting in vivo observations and therapy. Responding to this potential, there is emerging evidence for the efficacy of using VREs in the treatment of psychological disorders. Recent reviews demonstrate most research in this field has focused on the assessment and treatment of adult anxiety-related disorders, (Cieślik et al., 2020; Freeman et al., 2017). Ceislik et al. concluded that VRE tools were generally used as an add-on to therapy rather than a replacement stand-alone intervention. Reviews reported similar effectiveness to treatment as usual and to conventional interventions (e.g., Cieslik et al., 2020) or active controls (e.g., for PTSD, Kothgassner et al., 2019). Other reviews report research into VREs in populations with neurodevelopmental disorders, such as autism spectrum disorder (ASD) and attention deficit hyperactivity disorder (ADHD), eating disorders, psychotic disorders, depressive disorders, and substance use disorders (Carl et al., 2019; Cieślik et al., 2020; Clus et al., 2018; Freeman et al., 2017; Maples-Keller et al., 2017; Valmaggia et al., 2016). These report an emerging evidence base supporting the efficacy of VREs in assessment and treatment.
While research on VREs in adult mental health disorders is advancing, there is less research evaluating whether VREs can be similarly applied to child and adolescent populations. Sharar et al. (2007) suggest children experience VREs more vividly and perceive it as more real compared to adults. This suggests that VREs could elicit responses from children that are similar to their usual response to a situation, and prove useful for assessing symptomatic behaviour and practising adaptive behaviour. The limited literature on VREs in psychological assessment and intervention with children has focused on neurodevelopmental disorders and procedural anxiety. Emerging evidence suggests that the use of VREs as a distraction tool can be effective in preventing and reducing procedural distress (Eijlers et al., 2019). In childhood ADHD most research has sought to validate the use of virtual environments for the assessment of attention (Parsons et al., 2019; Romero-Ayuso et al., 2021). Recent reviews examined VRE interventions in children with ASD, concluding that VREs can be effective in improving cognitive and emotional processing, social communication and attention (Bailey et al., 2021; Mesa-Gresa et al., 2018).
Beyond procedural anxiety and neurodevelopmental disorders, limited research has been conducted with children and adolescents. Bouchard (2011) summarised early work in the area of anxiety disorders noting encouraging findings for simple phobias. A systematic review of both VREs and applied games (digital games that aim to educate and/or change patterns of experience or behaviour) interventions for childhood mental health disorders, only included three VRE studies (Halldorsson et al., 2021). While these studies indicated that there may be potential for the use of VREs as a tool in the treatment of anxiety-related disorders, no further conclusions could be reached (Halldorsson et al., 2021). Similarly, in a review of VR exposure therapy for anxiety disorders in children, Kothgassner and Felnhofer (2021) found only four published trials, concluding that findings suggest VR exposure therapy may be an effective treatment, but more research was needed.
As such, this review sought to broaden the scope to include both assessment and treatment of all DSM/ICD mental health disorders in children and adolescents. The review aimed to establish
Method
This scoping review was conducted in accordance with PRISMA-ScR (Tricco et al., 2018) and the protocol was registered (https://osf.io/gafh8). ICD mental health disorders were added to inclusion criteria after protocol registration to include internet gaming disorder which is in the “conditions for further research” section of the DSM-5 (American Psychiatric Association, 2013) but listed as a disorder in ICD-11 (World Health Organisation, 2019).
Eligibility criteria
Eligibility criteria were refined during the review to be consistent with the study aim. Studies were eligible for inclusion if: 1. They were published in peer-reviewed journals in English. 2. They reported primary data (not reviews). 3. Participants were 18 years or younger, or if average age of participants in the study was less than 18 years. 4. The VRE was deemed an immersive, interactive 3D technology (HMDs/CAVE system). 5. VRE was used to contribute to the diagnostic assessment or the measure of symptom severity, or treatment of a diagnosed DSM/ICD mental health disorder or elevated symptoms of a mental health disorder. After preregistration the decision to exclude participants with neurodevelopmental disorders or procedural anxiety was made as recent systematic reviews are available, except when the target of intervention or assessment in children/adolescents with neurodevelopmental disorders was mental health. 6. They reported any of the following: a) The outcome of VRE interventions using a diagnostic measure or measure of symptoms of a DSM/ICD mental health disorder (this is a refinement of the preregistration criteria to include studies with mental health disorder symptom measures, as elevated symptoms indicate likely presence of the disorder) b) The effectiveness or validity of VRE for diagnostic assessment or measurement of symptom severity of a DSM/ICD mental health disorder, by comparing it to a validated diagnostic or symptom severity measure of a DSM/ICD mental health disorder or a control group (this criterion was added after preregistration to ensure studies using VRE in assessment were included)
Search strategy
Five databases, PsycInfo, PubMed, Embase, Scopus, and Web of Science, were searched from the beginning of records to 7th June 2021 (updated 5th July 2023). The search strategies were refined by a research librarian. Keyword searches in these databases consisted of a combination of target population terms and VRE terms. Population search terms included child* OR kids OR adolescen* OR teen* OR young OR youth OR juvenile OR minor OR pediatric OR paediatric. VR search terms included virtual reality OR virtual realit* OR virtual environment* OR VR. See supplementary materials for search strategies. Search results were exported into EndNote X9. A manual search of reference lists of all included papers was also conducted.
Study selection
Figure 1 summarises the study selection process. After duplicates were removed, 8,448 studies were screened based on title and abstract with 50 articles screened by an independent second reviewer. There was 90% agreement, with disagreements resolved through discussion. After 8,331 studies were excluded, the remaining 117 studies were screened through full-text reading. Ten percent of studies were screened by the second reviewer with 100% inter-rater agreement. Manual searches of the reference lists of all included studies identified no further studies. Thirteen studies met eligibility criteria and were included in this review. PRISMA-ScR flowchart of study selection process.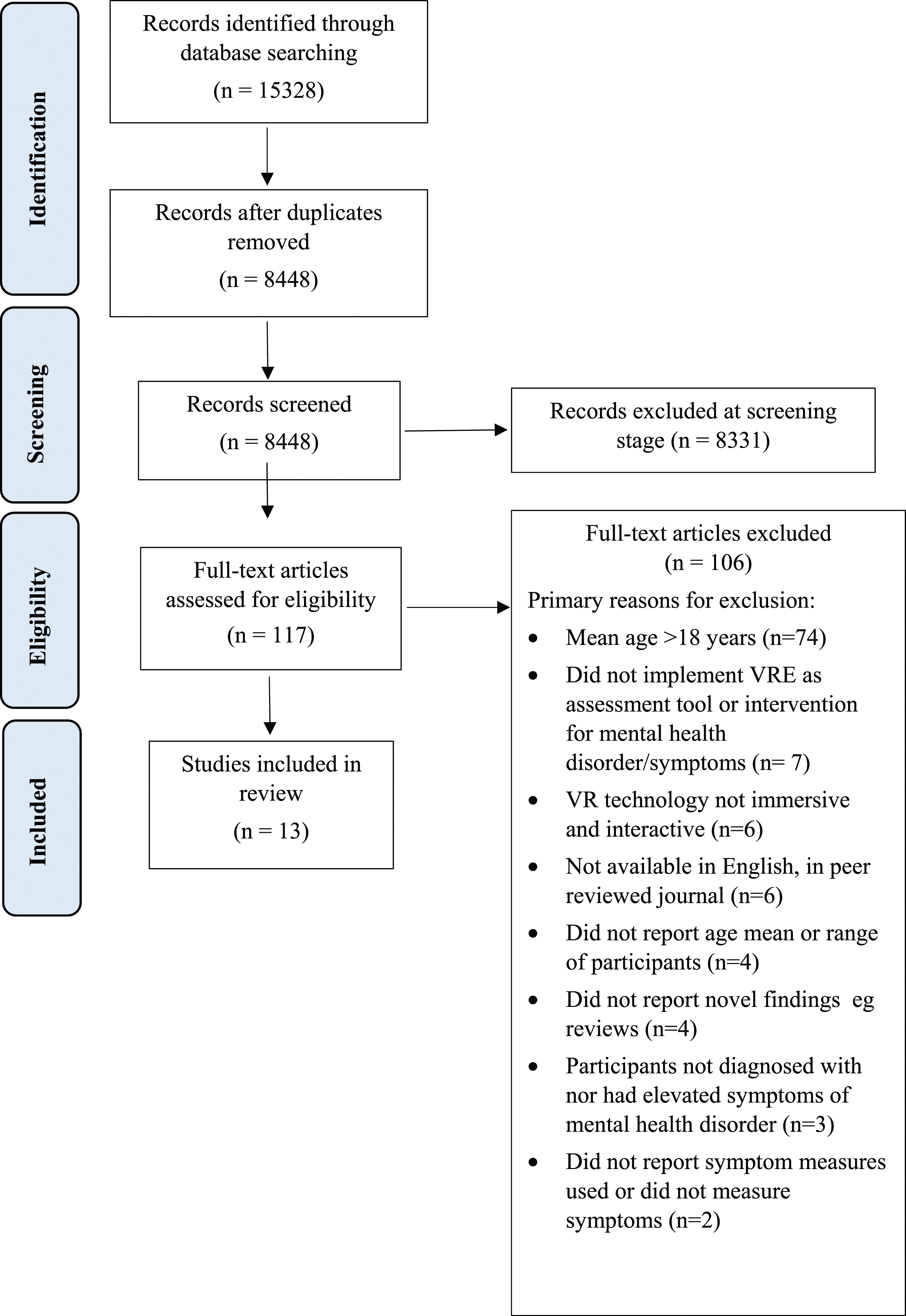
Data extraction and synthesis
Extracted data included study design, aim, procedure, outcome measures, and key findings, as well as VRE technology used, and participant demographics. A narrative synthesis was conducted.
Results
Study characteristics
Study characteristics and demographics.
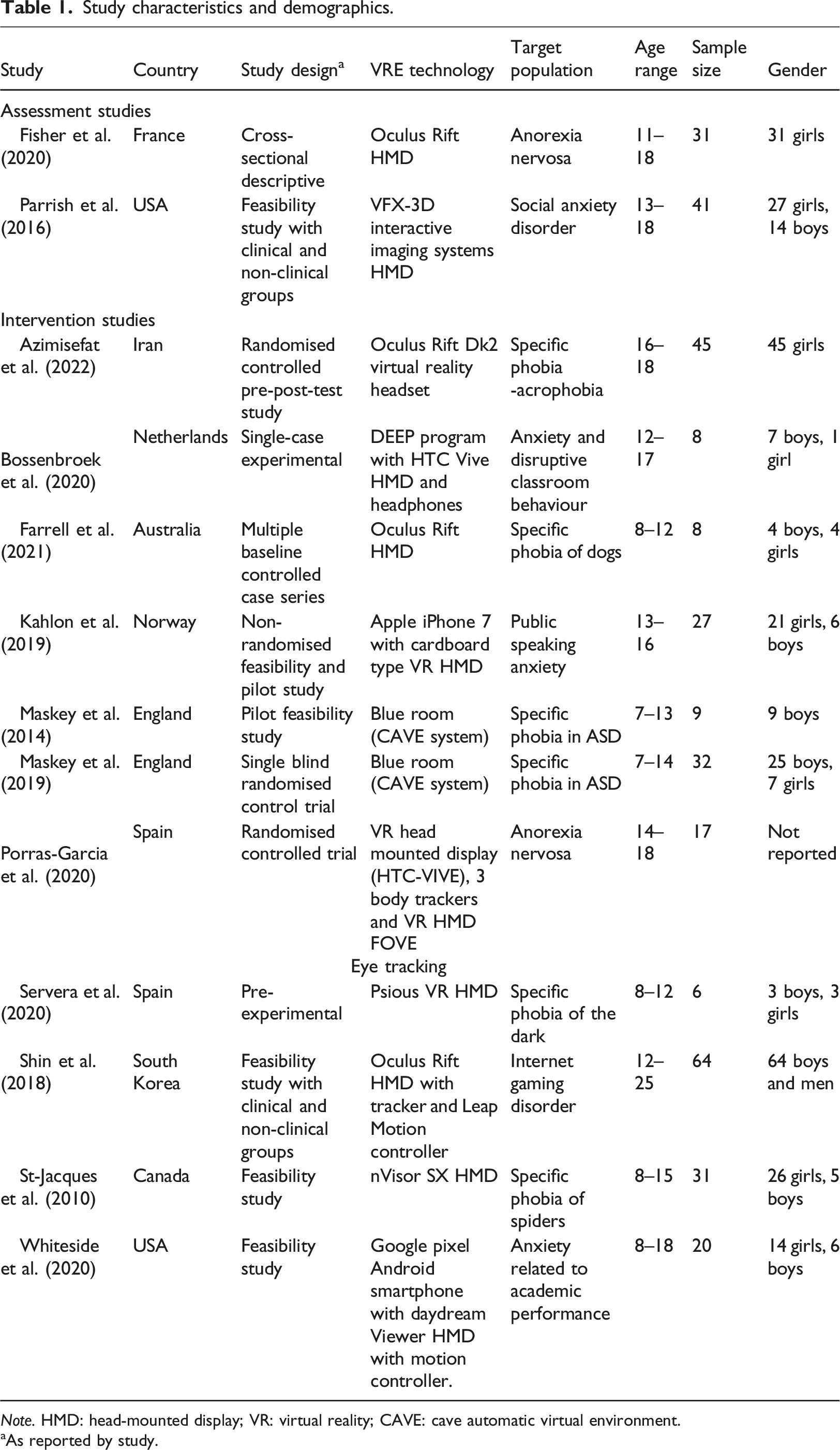
Note. HMD: head-mounted display; VR: virtual reality; CAVE: cave automatic virtual environment.
aAs reported by study.
Synthesis of results
Assessment studies
Two studies investigating the use of VREs to assess symptoms of mental health disorders were identified (see Table 1). Fisher et al. (2020) assessed the effectiveness of a VR-based scale for adolescents with anorexia nervosa to rate their body image perception and desired body, by comparing it to conventional paper-based figure rating scales. The outcomes of this descriptive cross-sectional study showed that body image disorders symptoms reported on the VR-based scale were comparable to symptoms reported on the paper-based figure rating scales. Also using VRE for assessment, Parrish et al. (2016) reported the feasibility of VREs differentiating between adolescents with and without social anxiety disorder, and whether exposure to VRE social environments (a party, giving a presentation) was more anxiety producing than exposure to VRE neutral environments (art gallery). Adolescents with social anxiety disorder reported significantly higher Subjective Units of Distress (SUDS) than the control group when exposed to the VRE social environments, and both groups found the VRE social environments significantly more distressing than the VRE neutral environment.
Intervention studies
Summary of the primary aims, procedure, outcome measures, and key findings of studies.
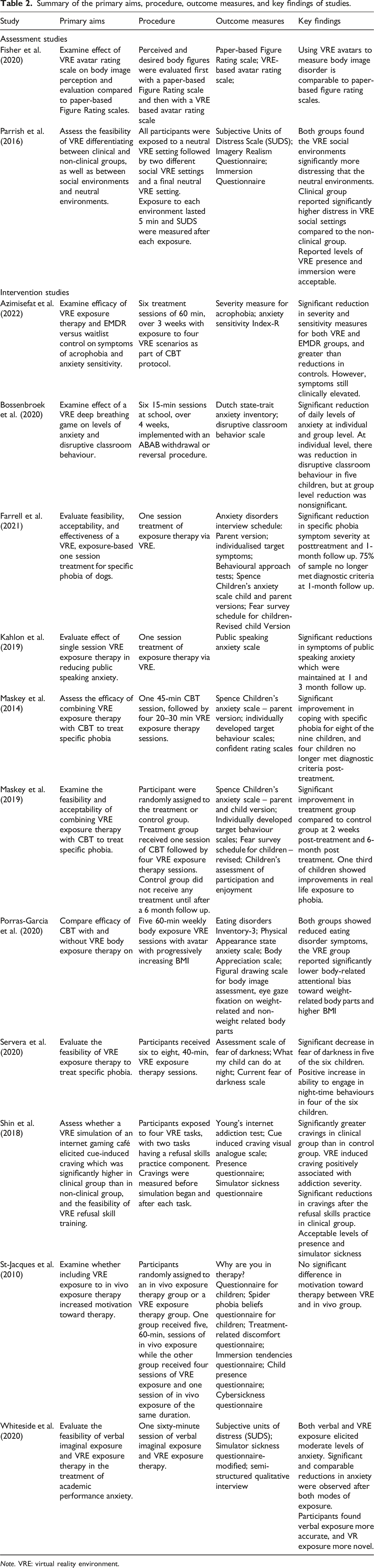
Note. VRE: virtual reality environment.
Discussion
The aim of this systematic scoping review was to evaluate how VREs have been implemented in the assessment and treatment of child and adolescent mental health conditions. This review included 13 studies, 11 examined use of VREs in treatment, and two examined use of VREs in assessment. Research is still mostly testing feasibility and piloting interventions with small numbers of participants. Most studies focused on examining the use of VREs as an exposure therapy tool, which findings suggest is a feasible mode of assessing and treating anxiety-related disorders and one study using VRE exposure reported to be effective with adolescents with anorexia nervosa (Porras-Garcia et al., 2020). Furthermore, this review found emerging support for VRE deep breathing training for anxiety (Bossenbroek et al., 2020), VRE assisted treatment of internet gaming disorder (Shin et al., 2018) and VRE assessment of body image evaluation in anorexia nervosa (Fisher et al., 2020). Several studies were piloting the use of VREs with next steps being RCTs. Therefore, while this review included more studies using VREs than Halldorsson et al. (2021), with findings indicating promise for the use of VREs in both assessment and treatment, and for conditions more broadly than just anxiety disorders, our recommendations regarding the need for RCTs and larger samples are similar.
Beyond the limited number of studies, there are several limitations in the current literature. This review defined VREs as a computer-generated simulation of a three-dimensional environment, which is immersive and responsive to an individual’s movements, and is experienced through HMDs and CAVE systems. However, a significant number of studies use the term VR or VRE to refer to technology that does not meet this definition. In the current review, six studies were excluded at full text screening due to the technology utilised (and described as VR/VRE) not being immersive and interactive (Dewis et al., 2001; Falconer et al., 2019; Gutiérrez Maldonado et al., 2009; Langer et al., 2016; Wong Sarver et al., 2014; Woodruff et al., 2007), with various more such studies identified in earlier stages of screening. The technology these studies refer to as VR included desktop computer displays and wall projected displays. It should also be noted that the literature also uses the term “virtual environments” to refer to virtual reality technology. It is important for future research to maintain a definition of VREs as the technology used in HMDs and some CAVE systems and separate the concept of VRE from non-immersive and interactive technology. Such differentiation would allow the field to clearly understand what is meant by VREs and facilitate synthesis of evidence. It is also important for future studies to provide clear details of the VRE hardware and software that is used, so that the VRE technology can be easily identified and comparisons to other hardware and software can be made.
Further limitations arise from the designs of the studies with only three RCTs included in this review. It is common for studies in an emerging field to be feasibility or case series studies. The primary issue with these studies is that without a randomised control group, it cannot be determined whether changes are due to the experimental intervention or due to other factors such as the natural progression of a disorder or spontaneous recovery (McNair & Lewis, 2012). As such, the most that could be said about the studies in this review is that they show promise and now should be tested using RCTs that compare VRE interventions with existing treatments. Such studies should also aim to clarify the advantages and disadvantages of VRE assisted assessments and interventions compared to traditional approaches, in particular examining motivation, engagement, and retention-aspects proposed to show an advantage for VREs, as well as efficacy.
Another limitation of the study designs were the small sample sizes, which meant they were underpowered. Although some studies had somewhat larger samples, they contained non-clinical control groups (Parrish et al., 2016; Shin et al., 2018). Furthermore, many of the studies only assessed participants at a single point in time. For intervention studies, the length of interventions varied in terms of the duration of each session and the number of total sessions. Outcomes of some intervention studies were also limited due to not conducting posttreatment follow-ups (Bossenbroek et al., 2020; Servera et al., 2020; Shin et al., 2018; Whiteside et al., 2020), which provide evidence regarding whether outcomes are maintained.
It is evident that research on the use of VRE assessments and interventions with children has mainly focused on anxiety-related disorders. While this is also reflected in the adult literature, research on VRE assessments and interventions for adults has also evaluated its application in eating disorders, psychotic disorders, depressive disorders, PTSD, and substance use disorders (Cieślik et al., 2020; Maples-Keller et al., 2017). As such, it is recommended that future research evaluate whether VRE assessments and interventions are feasible with children with a broader range of mental health problems. We only included studies where children met criteria for a mental health disorder, and so excluded studies of children with elevated levels of problem behaviours. These children may well have met criteria for a disorder and as these are children likely to be seen in child mental health services this is a limitation of our review.
Several studies did not clearly describe who implemented the VRE assessment or intervention, and the clinician training that was involved for delivering them, a key issue for implementation of these approaches. Another issue to be considered ahead of introducing these approaches to clinical practice is that the age range of participants were large, including different developmental age groups (Shin et al., 2018; St-Jacques et al., 2010; Whiteside et al., 2020). These studies applied the same VRE intervention approach to children as young as 8-years-old and as old as 15 and 18, with no indication of changing their approach due to a participant’s age. This may not reflect good clinical practice, as the approaches clinicians use with children across different developmental periods vary significantly (Weems et al., 2020). Including such large age ranges can be justified if a study aims to investigate the differences between developmental age groups, however the current studies did not indicate this as an aim of their investigations. The only study that reported different responses from participants based on age was Whiteside et al. (2020), who reported qualitative findings that younger children expressed preference for therapists that used VRE exposure therapy rather than verbal exposure techniques. These gaps in the literature raise the following questions: are outcomes and levels of acceptability and engagement different across age groups? How do VRE assessments and treatments protocols need to be modified for different age groups? Future investigations should aim to answer such questions. Further, no study has assessed whether VRE assessments or interventions can be implemented with young children below the age of 7.
Children may experience VREs as being more real than adults (Sharar et al., 2007). If children and adolescents do find it more difficult to separate reality from virtual reality, they may find virtual environments just as confronting or frightening as real-life situations. This suggests that further work is needed to establish whether children across developmental age groups experience the realism of VREs differently and how that would affect implementation or outcomes of VRE assessments and interventions.
Across the studies included in this review there was a range of VRE hardware and software used. There were only two studies that used the same VRE hardware and software, which was the CAVE system implemented by Maskey et al. (2014, 2019). Whether the use of different VRE technology significantly impacts the interpretability of the results is unknown, and future research should seek to identify factors of VRE hardware and software that could impact outcomes. This has also been identified as an issue in the adult literature implementing VRE assessments and interventions (Cieślik et al., 2020). Even so, this variability impacts the replicability of these studies, especially regarding the software used across studies. Some software used in the studies was independently developed and is not readily available for others to access, and even in cases where the software is publicly available, the VRE were modified by the research team. Furthermore, few papers provided detailed descriptions of what the VRE stimuli looked like and the functions that participants could perform within the VRE. Another challenge in this area is the rapid advancement of VRE technology, which may mean that the technology used in studies quickly become replaced with more advanced technology, as is the case with the VRE HMDs used in Parrish et al. (2016) and St-Jacques et al. (2010)’s studies. An answer to this issue might be for papers to provide detailed information on the hardware and software technology used, as well as detailed descriptions of the VRE stimuli presented to participants. Of note, the significant advantages of HMDs over CAVE systems, such as more accurate near field representation and the ability to use headsets with adjustment for the IPD of individual children suggest that future development of VREs are likely to be HMDs rather than CAVE systems.
Conclusion
The potential benefits of implementing VRE assessments and treatments of psychological disorders into clinical practice has raised the interest of many in the mental health field. Much of the child literature has focused on assessing the applicability of VREs in neurodevelopmental disorders and paediatric procedural anxiety. This systematic scoping review investigated how VRE assessments and interventions had been applied to other mental health disorders. The current literature shows promise for the use of VRE assessments and interventions of childhood mental health problems, particularly as an exposure therapy tool for anxiety-related disorders. There is emerging support for VRE deep breathing training for anxiety, VRE assisted treatment of internet gaming disorder and anorexia nervosa, and VRE assessment of body image evaluation in anorexia nervosa. However, most work to date is feasibility studies. High-quality research is still needed to understand whether VREs are a viable and effective mode of assessing and treating mental health disorders in children and adolescents, and how it compares to existing evidence-based approaches, given its promise to improve both engagement and outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.