
Abstract
Background
Sleep problems are common in adolescence and often related to psychopathology and impaired functioning. However, most studies have used summative scores, and little is known about how adolescents with disrupted sleep perceive their specific symptoms and dysfunctions. This study explored differences in levels of psychiatric symptoms and functional ability between Swedish adolescents with and without self-reported disturbed sleep in a school-based sample.
Methods
Swedish adolescents (n = 618, mean age 15.7+/-1.9yrs) answered the PROMIS pediatric measures for fatigue, anxiety, depression, pain interference, anger, physical activity and peer and family relationships. Logistic regression analyses were performed to assess differences between respondents with and without disturbed sleep.
Results
Disturbed sleep was associated with higher levels of symptoms of fatigue, anxiety, depression, anger and pain interference, as well as lower functional abilities in terms of physical activity and peer- and family relationships. Adolescents reporting disturbed sleep generally displayed a pattern of impaired executive functioning, internal emotional distress and school- and sleep related worry and dysfunction, as compared to physical disability, aggressive behavior, stress and generalized worry.
Conclusions
The present study adds to the understanding of how disturbed sleep and specific psychiatric symptoms and functional ability are interrelated, which may also have clinical implications.
Keywords
Introduction
Disordered sleep, especially insomnia, is common in adolescence (Dohnt et al., 2012). An individual with insomnia displays difficulties in falling asleep, in staying asleep as long as desired, and/or suffers from early awakenings for at least three nights per week over at least 3 months, with associated clinically significant functional impairment (American Psychiatric Association, 2013). Diagnostic and statistical manual of mental disorders (fifth ed.). Washington). Adolescent insomnia has a mean age of onset of 11 years with difficulties initiating sleep as the most common symptom (Johnson et al., 2006). 10 % of adolescents in the general population meet criteria for insomnia and one third of them report “at least some” insomnia symptoms (Dohnt et al., 2012). Sleep loss can affect mood states in this age group, with symptoms of depression and anger –in addition to fatigue– being higher after disturbed sleep (Short & Louca, 2015). When resulting in sleepiness, disordered sleep in adolescents also negatively affects executive functioning (Anderson et al., 2009) and contributes to increased irritability, inattention, and lack of motivation (Carskadon, 2011). In addition, experimental sleep restriction results not only in self-reported negative affective functioning but also in negative affective behavior in social peer contexts (McMakin et al., 2016), altogether suggesting that disturbed sleep may cast shadows not only on emotional functioning but also on academic performance and functioning.
The transition from childhood to adolescence seems to present an increased risk of developing both sleeping problems and comorbid psychiatric symptomatology (McMakin & Alfano, 2015). In fact, more than half of adolescents with insomnia fulfill criteria for another comorbid psychiatric disorder (Johnson et al., 2006) most commonly Major Depressive Disorder (MDD) or anxiety disorders (Johnson et al., 2000). Sixty-six percent of adolescents with insomnia also presented depressive symptoms (Amaral et al., 2017) in one study focusing on sleep and MDD. As many as 90% of children with anxiety disorders in late childhood/early adolescence also report symptoms of disordered sleep (Chase & Pincus, 2011). In addition to psychiatric problems, disordered sleep often occurs together with pain in both adults (Kundermann et al., 2004) and adolescents (Kanstrup et al., 2014), and experimental sleep deprivation has been shown to contribute to increased pain sensitivity (Haack et al., 2009; Kundermann et al., 2004). In adolescents with chronic pain, 60% suffer from insomnia and the link between pain, depression and functional disability was mediated by insomnia (Kanstrup et al., 2014). Thus, insomnia is common in adolescents and is connected with other problems that are likely to both contribute to sleep problems and to be negative consequences of disordered sleep. Furthermore, for adolescents with disordered sleep and co-morbid anxiety disorders and/or depression a priority in targeting disordered sleep may decrease symptoms of the comorbid states (Aslund et al., 2018; Meltzer & Mindell, 2014) (Åslund et al., 2020) as well as fatigue and anger (Van Dyk et al., 2017).
Self-reported symptomatology is generally restricted to the use of inventories and their summative scores, indicating a general degree of symptoms or absence or presence of a specific disorder. Not much is thus known about specific self-reported symptoms or functional disabilities that distinguish adolescents with disordered sleep from those without sleep problems. The aim of the present study was therefore to explore and elucidate in greater detail the variety of self-reported symptoms and functional abilities between adolescents with and without self-reported disturbed in a sample of Swedish adolescents, and to identify what specific symptoms and functional abilities may differentiate these groups.
Methods
Data collection and procedure
Data was collected from four schools of different socioeconomic standards in a medium-sized town and its surroundings in the northern part of Sweden during school year 2018–2019. The purpose of that project was to develop new instruments for screening and treating mental illness among young patients. Ethical approval was given by the Regional Ethical Review Board in Umeå, Sweden (number 2018/59-31). Verbal and written information was given to students by their teachers and written consent was obtained from those who chose to participate. From students <15 years, informed consent was obtained by the parents/guardians. Participants received a code to access the web survey during school hours, with assistance from a teacher and research assistant if required. Due to all questions having to be answered to finish the survey, no missing data was created. Participants were provided with a snack while filling out the survey and received a cinema gift card upon completion.
The study population was a convenience sample with students aged 12-20. A total of 897 students were asked to participate in the study and 618 (69%) agreed to do so.
Outcome measures
Disturbed sleep
Respondents were defined as having “disturbed sleep” if they responded “often” or “always” (as opposed to “never” or “sometimes”) to at least one of two sleep-related items from the larger data collection (described in 2.1): “I have trouble sleeping” (from the Revised Children’s Anxiety and Depression Scale (Chorpita et al., 2000)) or “I sleep poorly” (from Beck Youth Inventory II (Beck, 2001)) while non-disturbed sleepers responded “never” or sometimes” to these items. A dichotomous variable called “Disturbed sleep” was created.
Symptoms and functions
All respondents completed the Patient Reported Outcomes Measurement Information System (PROMIS) pediatric measures of fatigue (Lai et al., 2013; Quinn et al., 2014), anxiety (Quinn et al., 2014), depressive symptoms (Quinn et al., 2014), pain interference (Quinn et al., 2014; Varni et al., 2014), anger (Quinn et al., 2014), physical activity (Tucker et al., 2014), peer relationships (Dewalt et al., 2013) and family relationships (Bevans et al., 2017). PROMIS were developed using qualitative and item response theory methods to measure physical, mental and social health (Cella et al., 2010). PROMIS pediatric measures documents self-reported symptoms and functioning over the previous 7 days with a 5-option response with higher scores indicating more of the measured symptom or function. PROMIS measures are constructed to allow items to be analyzed separately, permitting a more flexible data collection. Swedish translations of the PROMIS pediatric measures have been established (Chaplin et al., in manuscript). Definition of the PROMIS measure domains are found at www.healthmeasures.net. For detailed information on the measures used in the data collection (version, number of items), see Supplementary Table 1.
Statistical analyses
All statistical analyses were performed using Stata, version 16.0. To characterize the sample and the subgroups of respondents with and without disturbed sleep, independent sample t-tests were used on demographic variables. Due to the dependent variable “Disturbed sleep” being dichotomous, logistic regressions were performed to analyze differences in levels of symptoms and functions between the two groups. Analyzes were performed on summative PROMIS-scores, as well as on individual item-scores, with p< 0.05 considered statistically significant. All effect sizes were calculated as standardized Cohen’s d’s (Cohen, 1992) with 95% confidence intervals (95% CIs). Effect sizes were considered “small” if d = 0.0–0.4, “moderate” if d = 0.4–0.7 and “large” d ≥ 0.7 (Cohen, 1988; Matthey, 1998). As the study had an explorative approach, all results were analyzed and no limitations for possible Type-I errors were made.
Results
Sample characteristics
Disturbed sleep
Demographic data of all respondents and subgroups of respondents reporting “disturbed sleep” or “non-disturbed sleep”.
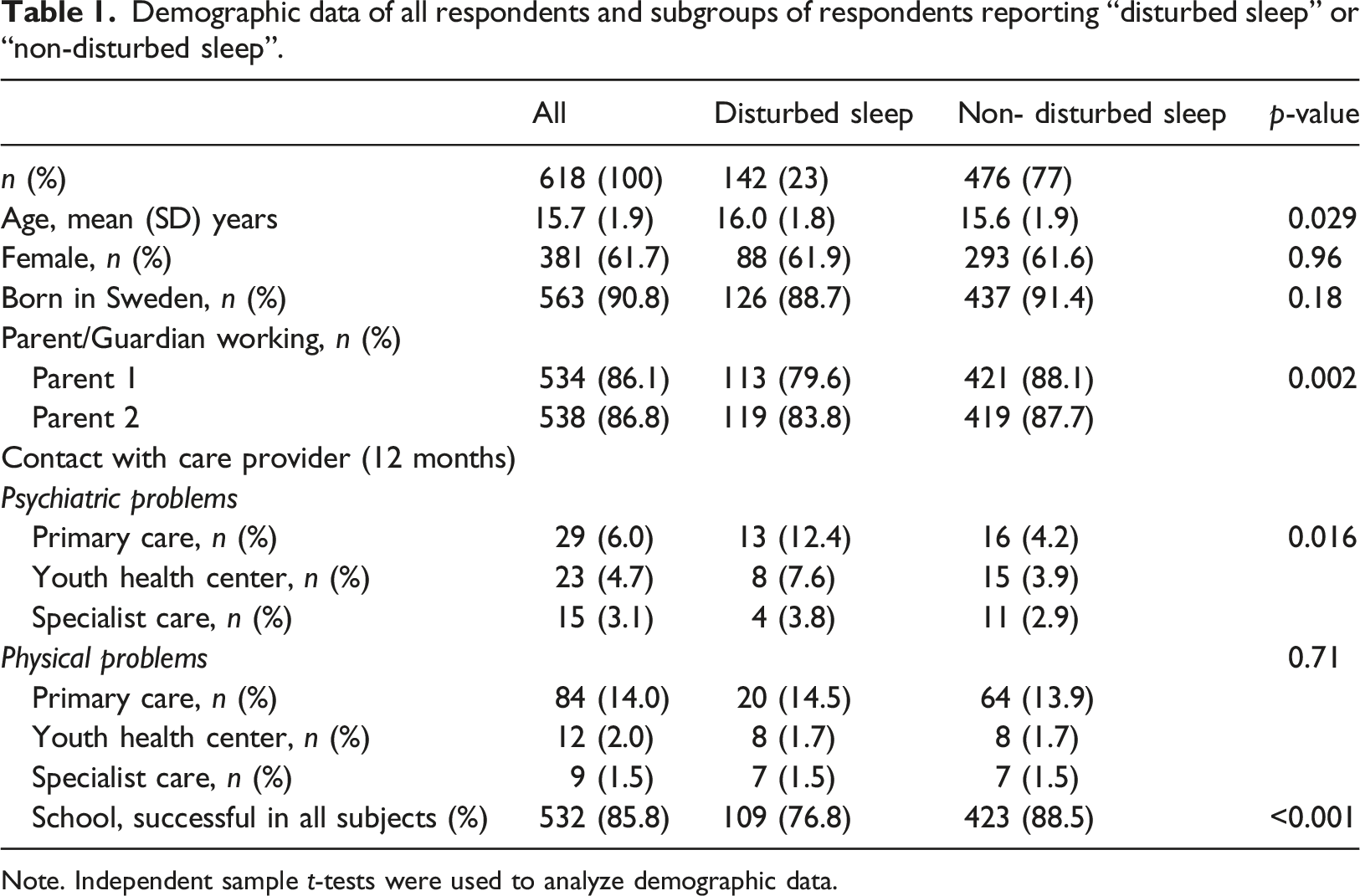
Note. Independent sample t-tests were used to analyze demographic data.
Demographics
Table 1 also presents demographic data for the total sample and for the two respective subgroups (disturbed sleep; non-disturbed sleep) separately. A majority of respondents were female, born in Sweden and with both parents/guardians working. A minority of respondents reported having been in contact with a primary care unit, a youth health center or a specialist care unit for psychiatric and/or physical problems during the last 12 months.
Differences in levels of symptoms and functions between poor and good sleepers
Results of the differences between the groups (disturbed sleep; non-disturbed sleep) on summative scores for all measure domains.
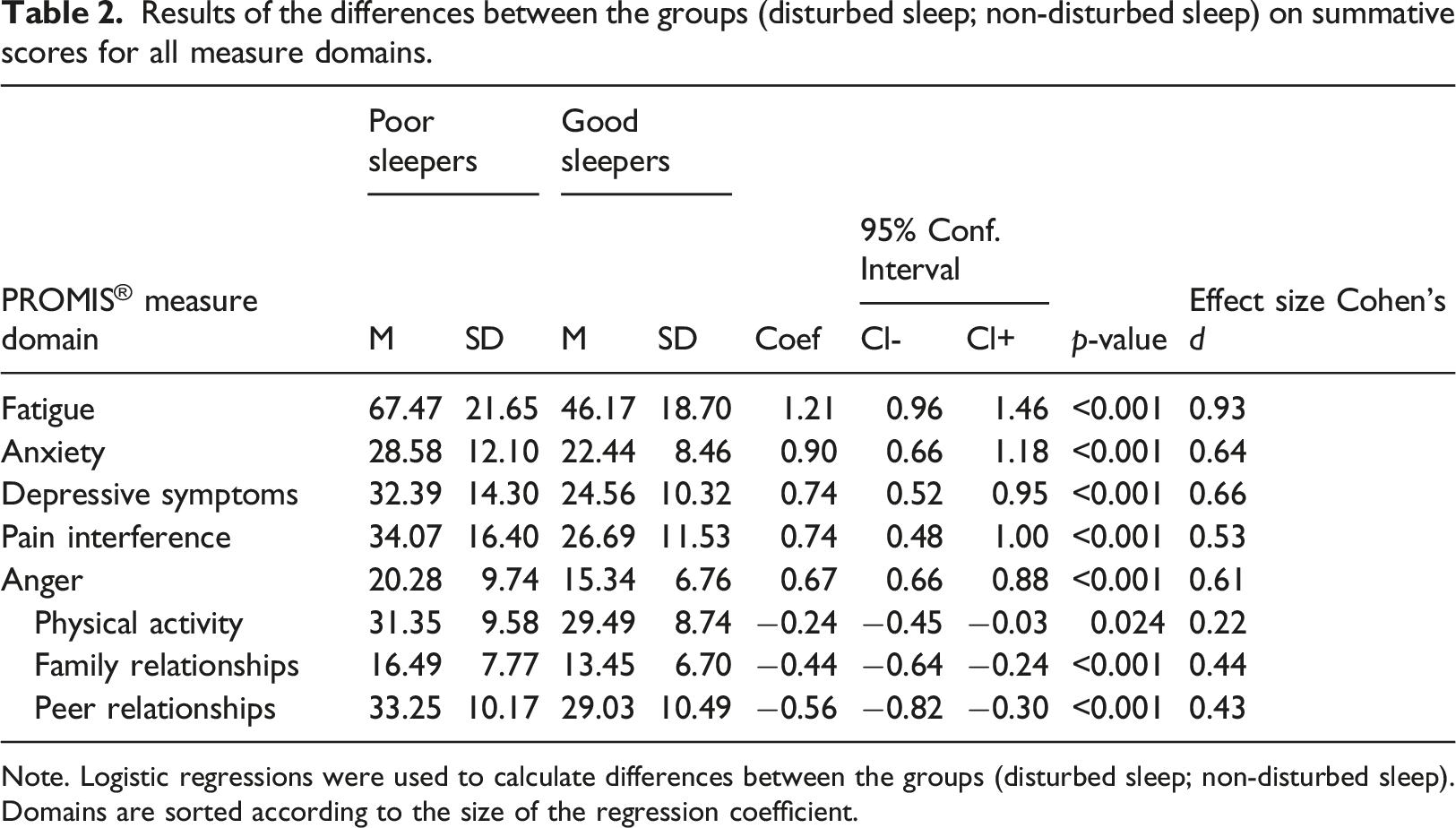
Note. Logistic regressions were used to calculate differences between the groups (disturbed sleep; non-disturbed sleep). Domains are sorted according to the size of the regression coefficient.
Differences in specific symptoms and functions between respondents with disturbed sleep and non-disturbed sleep
Differences in mean item score, as displayed by the regression coefficient, between respondents in the two groups (disturbed sleep; non-disturbed sleep) for all n = 116 items.
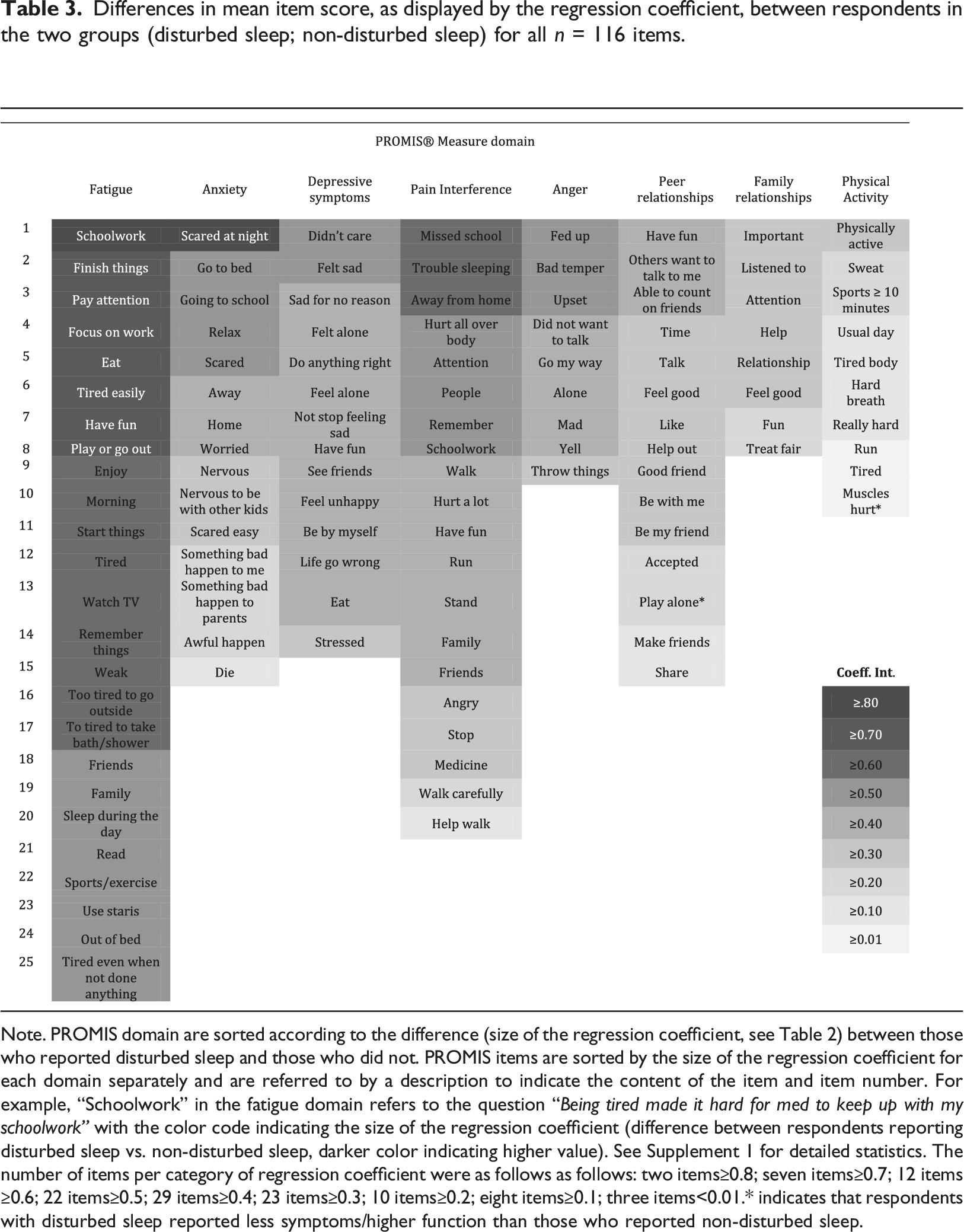
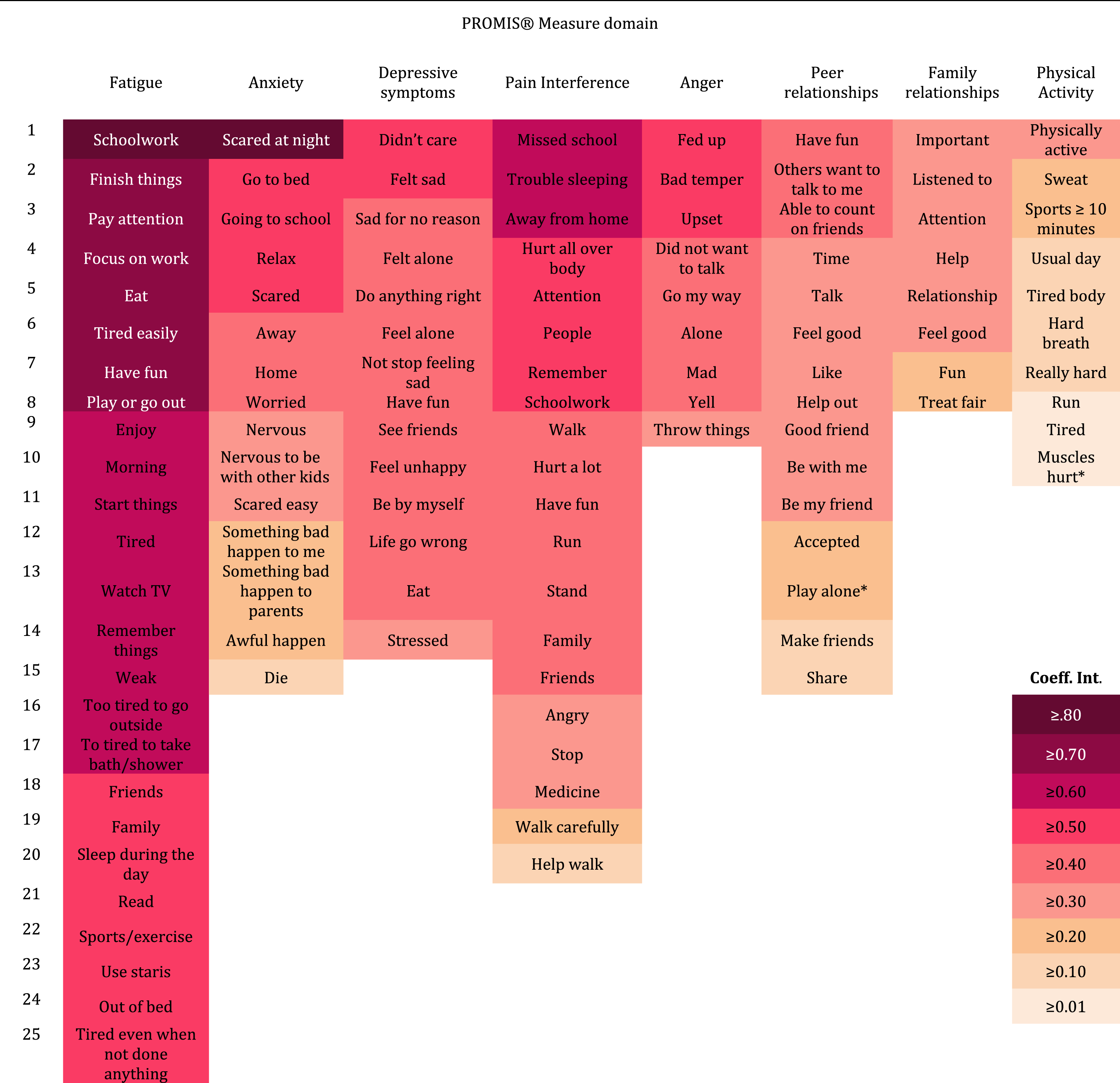
Note. PROMIS domain are sorted according to the difference (size of the regression coefficient, see Table 2) between those who reported disturbed sleep and those who did not. PROMIS items are sorted by the size of the regression coefficient for each domain separately and are referred to by a description to indicate the content of the item and item number. For example, “Schoolwork” in the fatigue domain refers to the question “Being tired made it hard for med to keep up with my schoolwork” with the color code indicating the size of the regression coefficient (difference between respondents reporting disturbed sleep vs. non-disturbed sleep, darker color indicating higher value). See Supplement 1 for detailed statistics. The number of items per category of regression coefficient were as follows as follows: two items≥0.8; seven items≥0.7; 12 items ≥0.6; 22 items≥0.5; 29 items≥0.4; 23 items≥0.3; 10 items≥0.2; eight items≥0.1; three items<0.01.* indicates that respondents with disturbed sleep reported less symptoms/higher function than those who reported non-disturbed sleep.
Full item-questions for the items with the largest and smallest regression coefficient (differences between respondents reporting disturbed sleep vs. non-disturbed sleep).
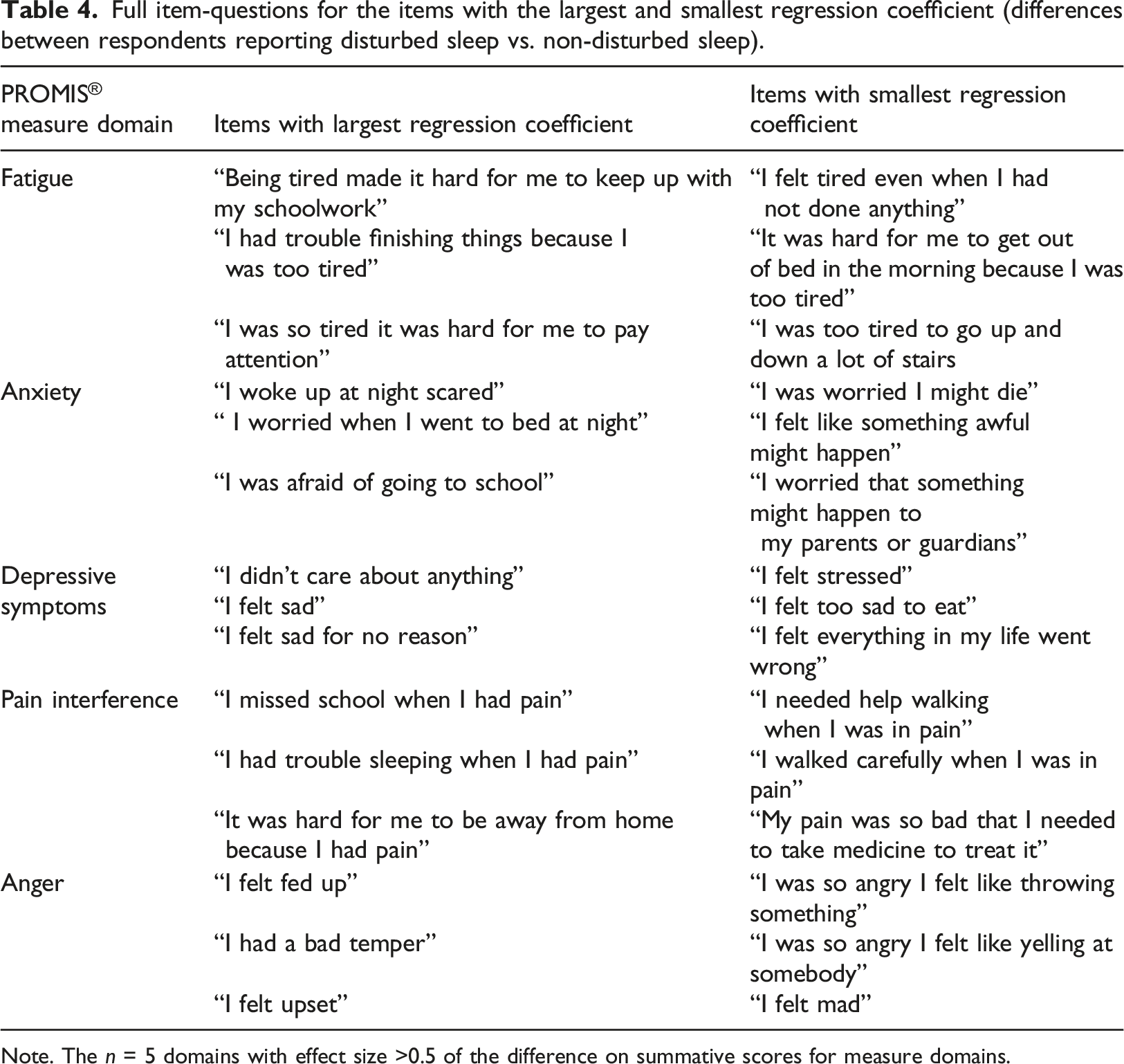
Note. The n = 5 domains with effect size >0.5 of the difference on summative scores for measure domains.
Discussion
This study examined differences in levels of symptoms and functional domains between adolescents with self-reported disturbed sleep and non-disturbed sleep in a school-based Swedish cohort. A more detailed examination of differences in specific symptomatology and functional abilities between these groups was also performed. When comparing summative scores for the two groups, the differences were significant for all measures, with the respondents with disturbed sleep being worse off. This group thus reported higher symptom levels overall, with fatigue, anxiety, depression, anger and pain interference differing the most as compared to those reporting non-disturbed sleep. Effect sizes were moderate to large. For the functional domains (physical activity, peer- and family relationships), respondents with disturbed sleep reported lower functioning, but these domains differed relatively less between the groups (with small to medium effect sizes). These findings are consistent with previous observations in adolescents in which sleep disturbances have notably been associated with depression and anxiety (Short & Louca, 2015; Van Dyk et al., 2017).
Regarding specific psychiatric symptoms and functional abilities, the respondents with disordered sleep reported higher scores for all items in the symptom domains and lower scores in the function domains (with two exceptions out of all 116 items). For the 20% items with the largest regression coefficient, all items originated from a symptom-domain rather than a functional domain. Three quarters of the items originated from the fatigue scale. The last observation is not surprising considering the close relation between sleep and recovery (Lo et al., 2016), even though it should be noted that motivational factors (which are also related to sleep (Axelsson et al., 2020)) are also highly related to fatigue, for example to muster energy in order to perform an activity. The rest of these items originated from the domains of pain interference, anxiety and anger. This suggests that sleep disturbances are more strongly associated with these symptoms, as compared to depressive symptoms or physical/social function. For the 20% items with the smallest regression coefficient, 70% of items were related to functional domains, and more specifically to physical activity, suggesting that these functions are not specifically impaired due to disturbed sleep.
The items with largest and smallest regression coefficients were further examined for the five most relevant measure domains (with d>0.5 of the summative score difference between respondents reporting disturbed vs. non-disturbed sleep). For fatigue, the groups differed most regarding executive functioning (e.g., attention, finishing tasks) and least in impaired physical function (e.g., get out of bed, taking the stairs). This is in line with previous reports on disturbed sleep, attention and working memory in adolescence (Lo et al., 2016). For depression, poor sleepers showed more internal emotional distress (e.g., feeling of sadness) while the least difference regarded general stress and loss of feeling of control. Even though a relation between sleep problems and stress has been documented in adolescence (Astill et al., 2013; Mesquita & Reimão, 2010), the results of the present study suggest that poor sleep could be less related to stress than more internal depressive symptoms.
Importantly, regarding anxiety symptoms, worrying at bedtime and feeling scared when in school were more related to disordered sleep as compared to generalized anxiety. This may imply that insomnia-specific rumination, which is known to be related to hyperarousal and insomnia in adults (Palagini et al., 2017), is applicable for adolescents too. These results support the notion that insomnia treatment targeting anxiety-driven rumination at bedtime can improve both the anxiety and the disordered sleeping patterns in adolescence (Åslund et al., 2020). Comorbidity between disordered sleep and anxiety in general could benefit from more detailed examination in future studies, both when examining the prevalence of these disorders, and with regard to sleep intervention outcomes. Respondents with disordered sleep scored higher on self-reported anger and tended to internalize anger (e.g., feeling upset or fed up) to a greater extent compared to those with normal sleep., while more overt aggressive behaviors (e.g., feeling like yelling/throwing) differed less between the groups. These results suggest a relationship between disordered sleep and “quiet” anger, rather than aggressive behavior, much like the results for the depressive symptoms domain.
For pain interference, the groups differed most with regard to school attendance and sleep quality, as opposed to physical exercise and medication. This suggests that although both groups might use medication to treat their pain to an almost equal extent, adolescents reporting disturbed sleep have a reduced school attendance due to pain when compared to their peers who do not report disturbed sleep. These results are consonant with insomnia being a mediator of the relationship between pain and functional disability in adolescents (Kanstrup et al., 2014).
There are several strengths and limitations of the present study. The observational and cross-sectional design precludes any conclusions regarding causality in the observed relationships between disturbed sleep on the one hand and symptomatology and functional ability on the other. In future studies, it would be beneficial to use repeated measures over time in order to achieve a more solid understanding of how changes in sleep problems might aggravate symptoms of psychopathology and impact overall function, and vice versa. It should be noted that respondents were not geographically stratified and did not fully match the Swedish pediatric population (e.g., the gender ratio), making the generalizability of the results uncertain. However, the sample is large and heterogeneous regarding socio-economic status due to the data being collected in several schools. Due to the explorative approach of the study, no restrictions were applied to data concerning Type-I error, increasing the risk of false positive findings and future studies are necessary to validate the current findings.
Conclusion
The present study supports the observation that disturbed sleep is associated with higher levels of symptoms of fatigue, depression, anxiety, anger and pain interference, as well as lower physical activity and peer- and family relationships in adolescents. It indicates that disturbed sleep is more related to executive functioning, internal emotional distress and school- and sleep related worry and dysfunction compared to physical disability, aggressive behavior, stress and generalized worry. Long-term follow-up studies as well as assessment of interventions targeting sleep problems in adolescents to analyze mediating and moderating factors and to better understand the direction of causality are warranted. These research findings contribute to our understanding of how sleep and specific psychiatric symptoms and functional abilities are interrelated, which may have implications for the future development of improved treatment for insomnia as well as for anxiety disorders and depression in adolescents. Targeting specific components of comorbid psychiatric disorders, such as anxiety-driven rumination about sleep and internalized anger and depression, could enhance treatment effects following psychological treatments of insomnia in adolescents.
Supplemental Material
Supplemental Material - Disturbed sleep and patterns of psychiatric symptoms and function in a school-based sample of adolescents
Supplemental Material for Disturbed sleep and patterns of psychiatric symptoms and function in a school-based sample of adolescents by Lie Åslund, Anna Andreasson, Mats Lekander, Eva Henje, Inga Dennhag Child Psychology and Psychiatry
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Svenska Sällskapet för Medicinsk Forskning (S253341) and Forskningsrådet om Hälsa, Arbetsliv och Välfärd (350-2012-303).
Supplemental Material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.