
Abstract
Background
Comorbidities among mental disorders can have long-term impacts on children’s development and mental health. There is little robust data about the prevalence of comorbidities in preschool-aged children. The aim was to identify the prevalence of comorbidities among mental disorders in a cohort of 3–4-year-old children in Australia.
Methods
Women were recruited to the Australian Mercy Pregnancy Emotional Wellbeing Study at <20 weeks’ gestation. Mental disorders were assessed among their children at 3- to 4-years old using the Preschool Age Psychiatric Assessment (PAPA). Prevalence of comorbidities is reported.
Results
Almost half (48%) of the children (n = 545) met criteria for mental disorders captured by the PAPA; 43% had anxiety disorders. Of children with at least one diagnosis, 44% had another mental disorder; this represents 21% of the whole sample. Depressive disorders occurred only alongside other disorders, both anxiety disorders and externalising disorders. At least one anxiety disorder was present in more than half of children with specific externalising disorders.
Conclusions
Comorbidity of mental disorders among preschool-aged children is relatively common. Preschool children presenting with mental health symptoms may benefit from assessment protocols which consider multiple mental health disorders, and integrated services to address these.
Plain Language Summary
Mental disorders in young children can have a long-term impact on their health and development, especially if children experience more than one mental disorder at the same time. This is known as “comorbidity”. We aimed to investigate the prevalence and nature of comorbidities among a cohort of preschool-aged children in Australia, in order to inform better mental health assessment of and treatment for children in this age range. The sample consisted of 3- and 4-year-old children (n=545) of women from a longitudinal pregnancy cohort study in Australia. They were assessed for mental disorders using the Preschool Age Psychiatric Assessment (PAPA), administered via a telephone interview with their mothers. More than one in five children (21%) in our sample had two or more diagnoses of mental disorders according to the PAPA. Among children with at least one PAPA mental disorder, 44% had at least one additional mental disorder. At least one anxiety disorder was present in more than half of children with attention deficit/hyperactivity disorder (ADHD), conduct disorder, oppositional defiant disorder (ODD) and depression. Thus, comorbidities did not always fit within externalising or internalising dimensions. Clinicians assessing mental health in preschool-aged children should assess for multiple disorders across both externalising and internalising dimensions. Integrated mental health services are required to address comorbidities in these early years.
Introduction
Mental disorders among preschool-aged children can have negative effects on their development and mental health across the lifespan (Angold & Egger, 2007). Early identification of and intervention for mental disorders prior to the commencement of formal education is recommended to prevent poor educational, occupational and health (physical and mental) outcomes (Center on the Developing Child, 2010; Weitzman and Wegner, 2015).
In research and even clinical settings the presence of symptoms of poor mental health among preschool-aged children is commonly assessed by parent completion of a dimensional measure (Achenbach & Edelbrock, 1981; Whalen et al., 2017); scores are typically compared with population norms, to indicate whether these symptoms are within a ‘clinical range’ indexing the likely presence of internalising (problems within the self) and externalising (conflict with the external environment) disorders (Achenbach & Edelbrock, 1981; Whalen et al., 2017). In contrast, few studies report on the prevalence of mental disorders in preschool children using structured diagnostic interviews with parents, which overcome the possible bias of parental proxy reporting via rigorous structured questions which yield diagnoses consistent with the Diagnostic and Statistical Manual of Mental Disorders, DSM-5 (American Psychiatric Association, 2013).
The prevalence of mental disorders among children has been reported in systematic reviews; however these either include broad age ranges from age 4 to 18 (Barican et al., 2022) or focus on specific populations such as children attending primary care (Charach et al., 2020). A relatively recent systematic review and meta-analysis included more than 18,000 children 1 to 7 years old (Vasileva et al., 2021); this review included only studies in which children’s mental disorders were assessed using structured interviews with parents. The overall pooled prevalence of any mental disorder among children aged 1 to 7 years old was estimated at 20.1% (95% CI [15.7, 25.4]) (Vasileva et al., 2021). Among the ten included studies, only three reported on mental disorders among preschool-aged children in settings that can be considered representative of the overall population: children attending required vaccination appointments in Iraq (n = 829, age 12–48 months, mean 30 months) (Al-Jawadi & Abdul-Rhman, 2007), children attending required community health check appointments in Norway (n = 2,475, 46–63 months, mean 53 months) (Wichstrøm et al., 2012), and children recruited through commercial mailing lists in the USA (n = 541, 36–50 months, mean 43.2 months) (Bufferd et al., 2011). Of these, only two (Bufferd et al., 2011; Wichstrøm et al., 2012) utilised the Preschool Age Psychiatric Assessment (PAPA) (Egger et al., 1999) for diagnosis of mental disorders; the third study reporting on mental disorders among preschool-aged children in community settings reported using interviews based on a standardised questionnaire including diagnostic criteria taken from the DSM-IV (Al-Jawadi & Abdul-Rhman, 2007). Based on the PAPA, Bufferd et al. (2011) reported a substantially higher overall prevalence of mental disorders (27%) than Wichstrøm et al. (2012) (6%).
Vasileva et al. (2021) estimated that comorbidity, namely the presence of more than one disorder, occurred in 6.4% (95% CI [1.3, 54.0]) of children 1 to 7 years old; approximately a third of children with one diagnosis of a disorder met criteria for at least one other disorder (Vasileva et al., 2021). The authors reported considerable heterogeneity among the included studies (Vasileva et al., 2021). In the above-mentioned US study (Bufferd et al., 2011), 9% of children had two or more diagnoses; 34% of those with one diagnosis met criteria for multiple diagnostic categories (Bufferd et al., 2011). In the Norwegian study (Wichstrøm et al., 2012), overall prevalence of comorbidities was not reported. However, the odds of attention-deficit/hyperactivity disorder (ADHD), oppositional defiant disorder (ODD), conduct disorder, anxiety disorder and depression were significantly higher among those diagnosed with other disorders, compared to those without (Wichstrøm et al., 2012).
In summary, there is substantial heterogeneity among studies reporting on prevalence of mental disorders among children, with regard to the age range of children assessed, measurement of mental disorders, study location and design, and populations targeted (Barican et al., 2022; Charach et al., 2020; Vasileva et al., 2021). The overall prevalences of mental disorders and comorbidities among preschool-aged children are difficult to identify from the current literature; only two studies have assessed mental disorders in community samples by diagnostic interviews such as the PAPA (Bufferd et al., 2011; Wichstrøm et al., 2012); these two studies, conducted in Norway and the US, were published more than a decade ago. The aim of this study was to describe childhood mental disorders and comorbidities among a cohort of 3- to 4-year-old children in Australia, using the PAPA.
Methods
Study Design
Data from the Mercy Pregnancy Emotional Wellbeing Study cohort are used for this study. Further details about this study can be found in the cohort profile paper (Galbally et al., 2017). Women completed Wave 1 data collection at recruitment at up to 20 weeks’ gestation; they were subsequently followed up at up to 28 weeks’ gestation (Wave 2); subsequent data about both the mothers and their children were collected at six months postpartum (Wave 4), 12 months postpartum (Wave 5) and when their children were 3 to 4 years old (Wave 6). At birth, information was captured from hospital records but not from women themselves (Wave 3). Data from Wave 6 (child age 3–4 years) are included in this paper. Sample characteristics are drawn from Wave 1 (<20 weeks’ gestation) and Wave 3 (birth) data.
Recruitment
As described (Galbally et al., 2017), recruitment took place at metropolitan maternity hospitals in Melbourne, Victoria and Perth, Western Australia, as well as regional and rural hospitals in Western Australia. This was a selected cohort design, in which women formally diagnosed with current depression using the Structured Clinical Interview for DSM-IV (SCID-IV) (Carter et al., 2010) were deliberately over-recruited, as well as a group of non-depressed pregnant women.
Women were eligible to participate if they were less than 20 weeks’ gestation and proficient in English. Exclusion criteria were psychotic or substance abuse disorders, child protection involvement, intellectual disability, serious physical illness or psychiatric illness requiring current acute inpatient admission.
Measures
Child mental disorder: The primary outcome was a diagnostic classification of one or more mental disorder among 3–4-year-old children according to DSM-5 criteria (American Psychiatric Association, 2013), and assessed by the Preschool Age Psychiatric Assessment (PAPA) (Egger et al., 1999). The PAPA is a semi-structured research diagnostic instrument that measures psychiatric symptoms and disorders according to the DSM-5, for pre-school age children, aged 2-5. The e-measures electronic version of the PAPA was administered through interviews with mothers of 3-4 years old within MPEWS. The research team undertook training with the authorised trainers of this instrument from Duke University, Developmental Epidemiology (Egger & Angold, 2006), which included coding practice and checking coding with trainers. Following the initial training, subsequent interview administrators underwent a month of training with experienced interviewers who had been trained in the original training with PAPA developers. To facilitate inter-rater reliability, the novice interviewers also completed the coding of at least three interviews after training whilst under supervision with experienced interviewers before completing coding on their own. To ensure quality control, protocol fidelity and consistency for the duration of the data collection, regular supervision with experienced trainers was offered fortnightly to administrators, in which coding queries were discussed with other novice and experienced interviewers.
In the PAPA, compulsory questions are asked about whether symptoms have been present or absent in the past 3 months. If an item is endorsed, the parent is asked follow-up questions, such as onset, frequency, duration and severity of symptoms, and impairment, and to give examples of the behaviour. These behavioural examples provide critical information which guide the interviewer to formally code the PAPA in e-measures. Subsequently an algorithm is applied to determine diagnosis based on coded data. The PAPA has been validated as a reliable standardized measure of DSM-4 psychiatric symptoms and disorders in pre-schoolers (Egger et al., 2006). Its test-retest reliability is comparable to widely used and well-established measures for older children and adults (Egger et al., 2006).
For the purposes of this study, we include the following DSM-5 diagnoses measured using the PAPA: anxiety disorders (separation anxiety, social anxiety, specific phobia, agoraphobia, panic attacks and generalised anxiety disorder (GAD)); post-traumatic stress disorder (PTSD); depressive disorders (including major depression, dysthymia, and/or other specified depressive disorders); attention-deficit/hyperactivity disorder (ADHD), conduct disorder and oppositional defiant disorder (ODD).
As women with a current depressive episode within the past two years were over-represented in this study, we report on the number and proportion of women who met these criteria, as assessed using Modules A and D of the SCID-IV-TR, Clinician Version (First et al., 1997).
Statistical Methods
This is a descriptive study, presenting data on prevalence and patterns of mental disorders and comorbidities in our sample of 3–4-year-old children. Data were analysed using IBM SPSS Statistics version 29.
To evaluate attrition bias, data on sociodemographic characteristics and depression status at <20 weeks’ gestation were compared between women who completed the PAPA (at child age 3–4 years) with women who did not. For binary variables such as depression status, Χ2 tests were used, applying the continuity correction. For maternal age, which was not normally distributed, a Mann-Whitney U test was applied.
We report the proportion of children who met DSM-5 criteria for each disorder, and for two or more disorders, according to the PAPA. As a sensitivity analysis we compare the prevalence of two or more mental disorders among children of women who had a current depressive episode at < 20 weeks, and children of women who did not.
Patterns of comorbid mental disorders were first explored by examining the proportion of children diagnosed with each mental disorder, and then their comorbidity patterns with another disorder. For example, we report the proportion of children with a diagnosis of ADHD who also had an additional diagnosis of each other disorder. We demonstrate the degree of comorbidity using a heatmap, generated within Excel using an algorithm to group the data into 6 colour categories; green shades represent lower proportions while red shades indicate higher proportions.
Secondly, we report the odds ratios (OR) and confidence intervals associated with having a specific mental disorder, for each other disorder. Owing to multiple comparisons (approximately 70) and the associated risk of Type I errors, we apply a Bonferroni correction and report only odds ratios with statistical significance <0.001. The only other PAPA-based studies to calculate odds ratios for combinations of mental disorders among preschool children (Bufferd et al., 2011; Wichstrøm et al., 2012) report substantial odds ratios of 5 and above. To detect a more modest odds ratio (OR) of about 2.0 with 80-90% power at a 5% significance level, one requires approximately 16 cases and 16 controls (Lemeshow et al., 1988). Thus, we did not calculate odds ratios within any groups for which exposure (in this case the other mental disorder) did not occur in at least 16 cases.
Ethics
The study has been approved by the Mercy Health Research Ethics Committee (Victoria, R08/22, 3 July 2012) and the South Metropolitan Health Service Human Research Ethics Committee (Western Australia, 2016-192, 11 October 2016). Each woman provided written consent to participate at each wave of data collection. If PAPA interview participants became distressed, the interview was suspended or paused, and the interviewer provided options to abort or reschedule the interview. Information on available supports for women was provided on the Participant Information and Consent form at each wave of data collection, and interviewers discussed these with women as appropriate. Women were also offered a telephone call with a psychiatrist from the research team if they would like to discuss support options. Interviewers offered all women a letter to their child’s general practitioner, psychologist, paediatrician or psychiatrist summarising the results of the research interview. If women indicated they would like this to occur, we obtained written consent from them along with the practitioner’s mailing address.
Results
Sample Sociodemographic Characteristics for Women Who did Versus did Not Complete the PAPA at Wave 6
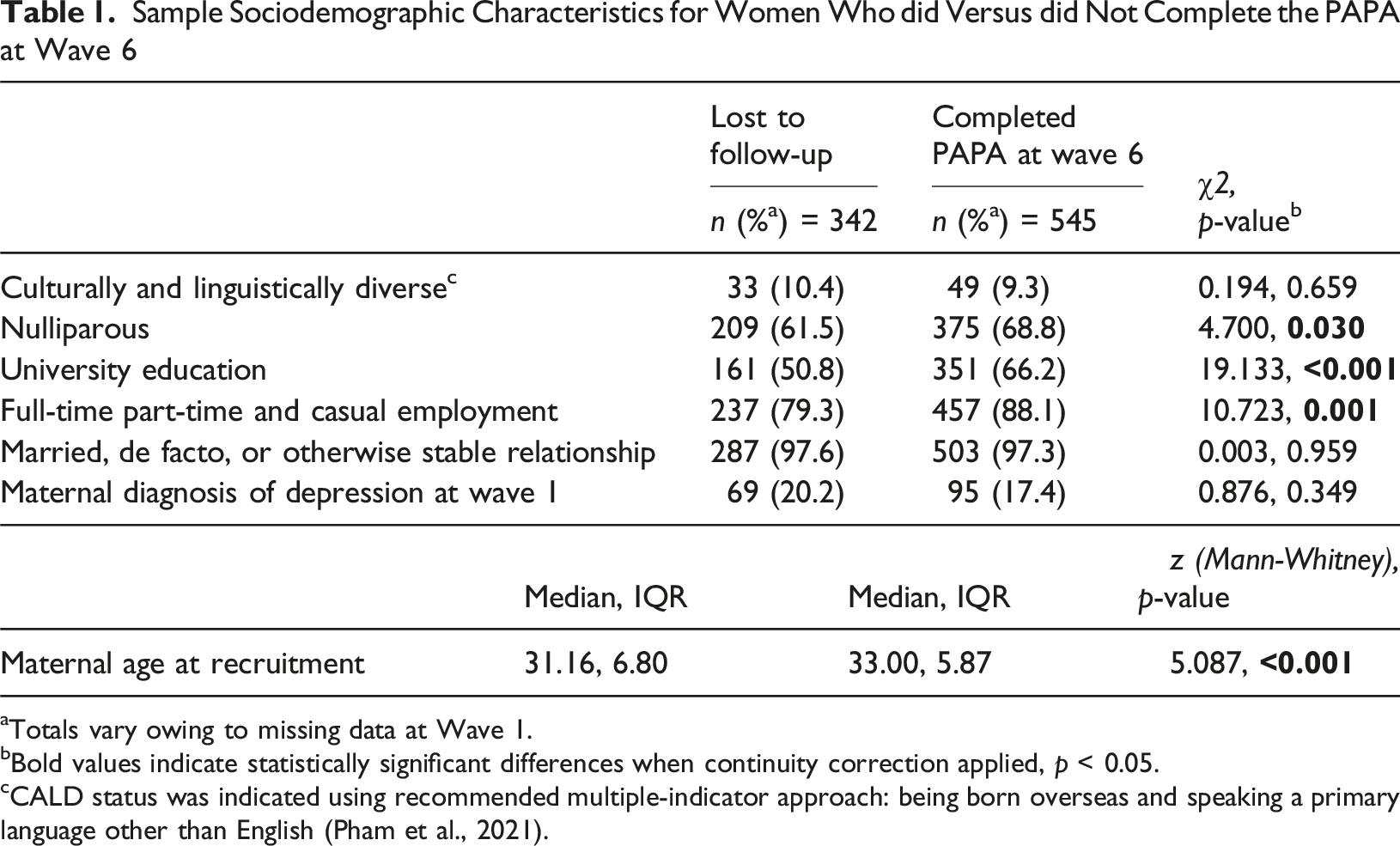
aTotals vary owing to missing data at Wave 1.
bBold values indicate statistically significant differences when continuity correction applied, p < 0.05.
cCALD status was indicated using recommended multiple-indicator approach: being born overseas and speaking a primary language other than English (Pham et al., 2021).
Mental Disorders at 3-4 years (n (%))
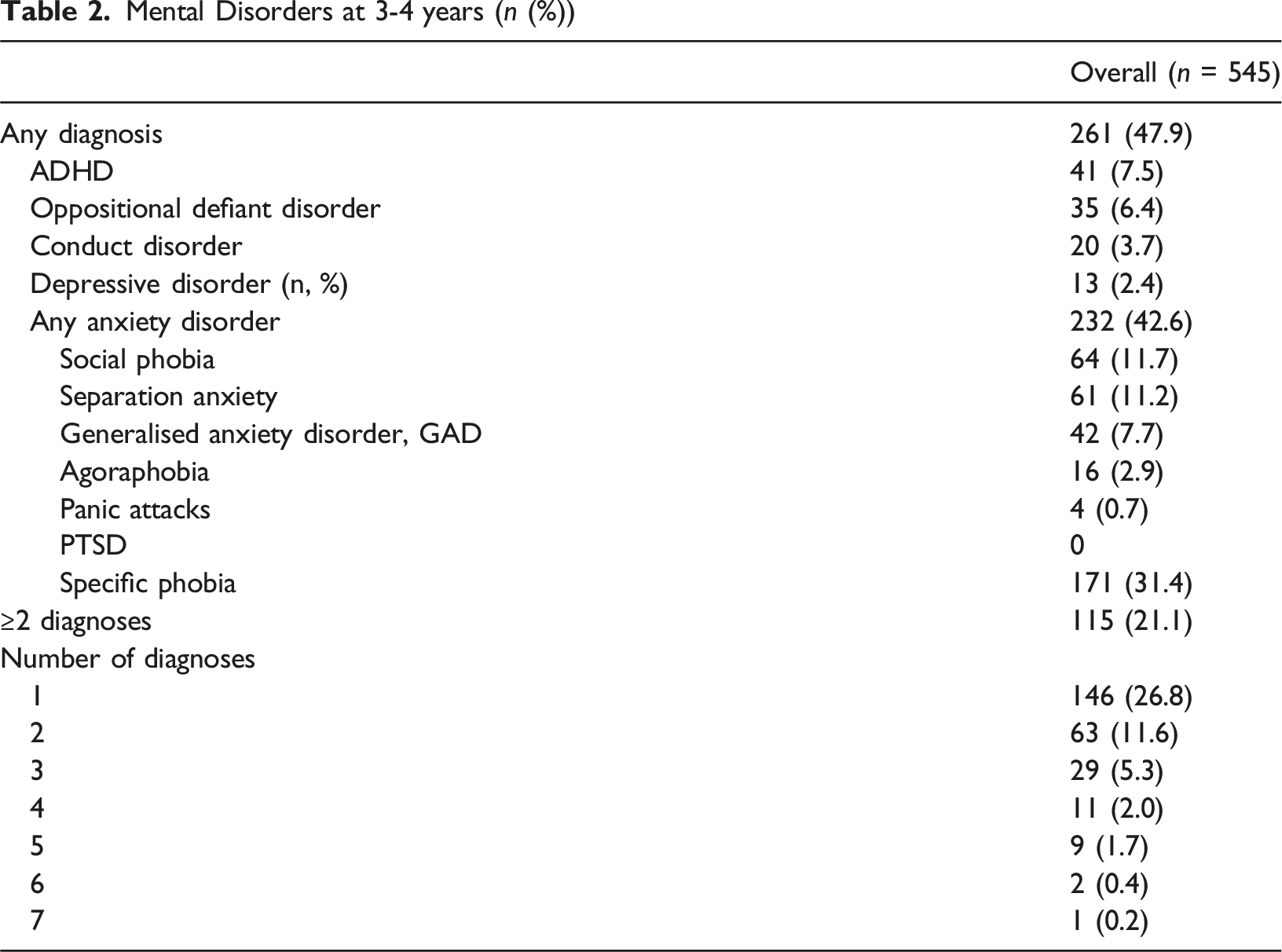
About half of all children (47.9%) had at least one diagnosis. Of those with at least one diagnosis, 115 (44.1%) had two or more mental disorder diagnoses; this represents 21.1% of the whole sample (Table 2). There was a significant difference between the proportion of children with two or more diagnoses among mothers with and without a diagnosis of depression at Wave 1 (30.5% versus 19.1%, p = 0.019), but not after removal of specific phobias (17.9% versus 11.6%, p = 0.129).
Prevalence of Specific Comorbidities
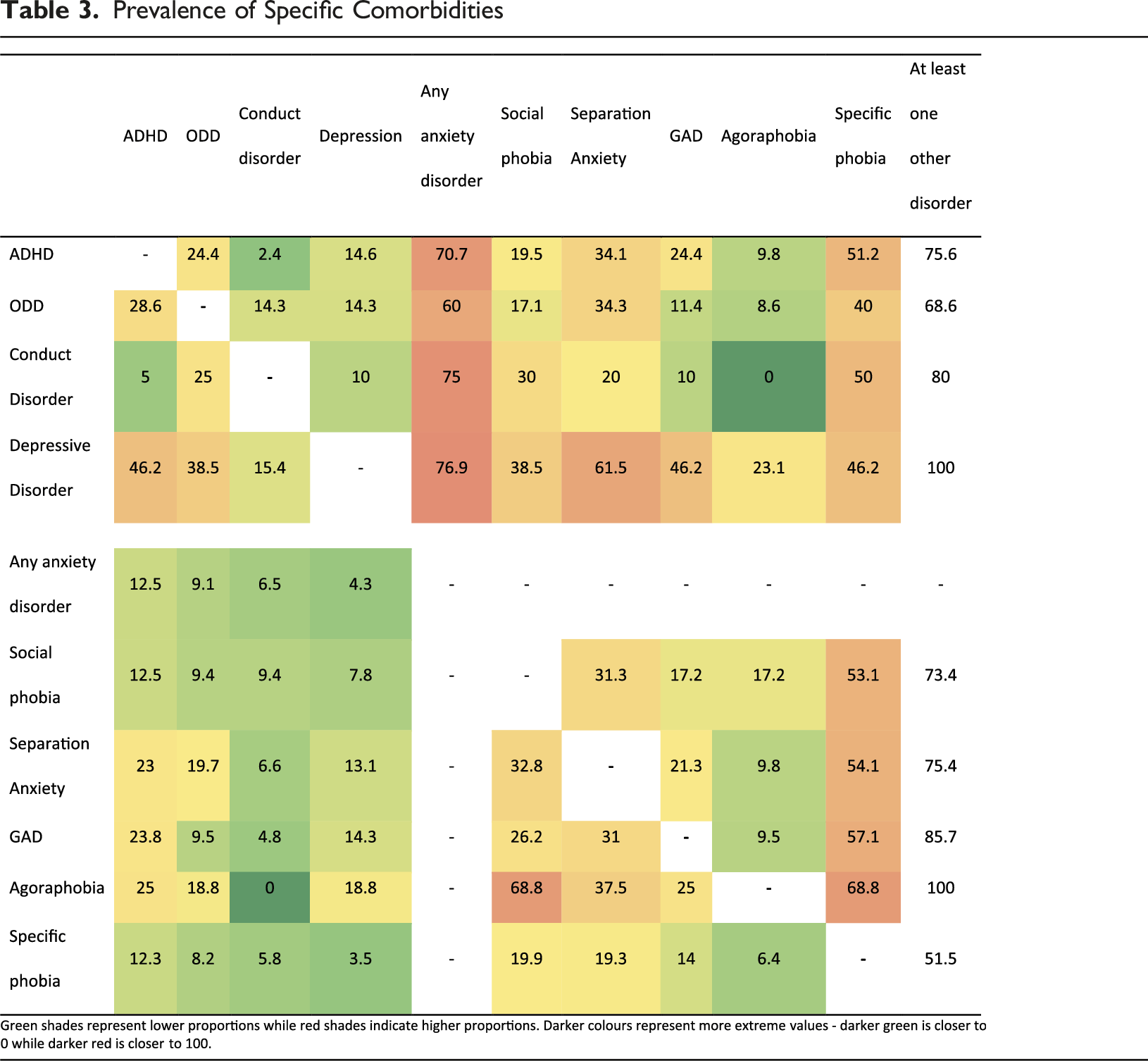
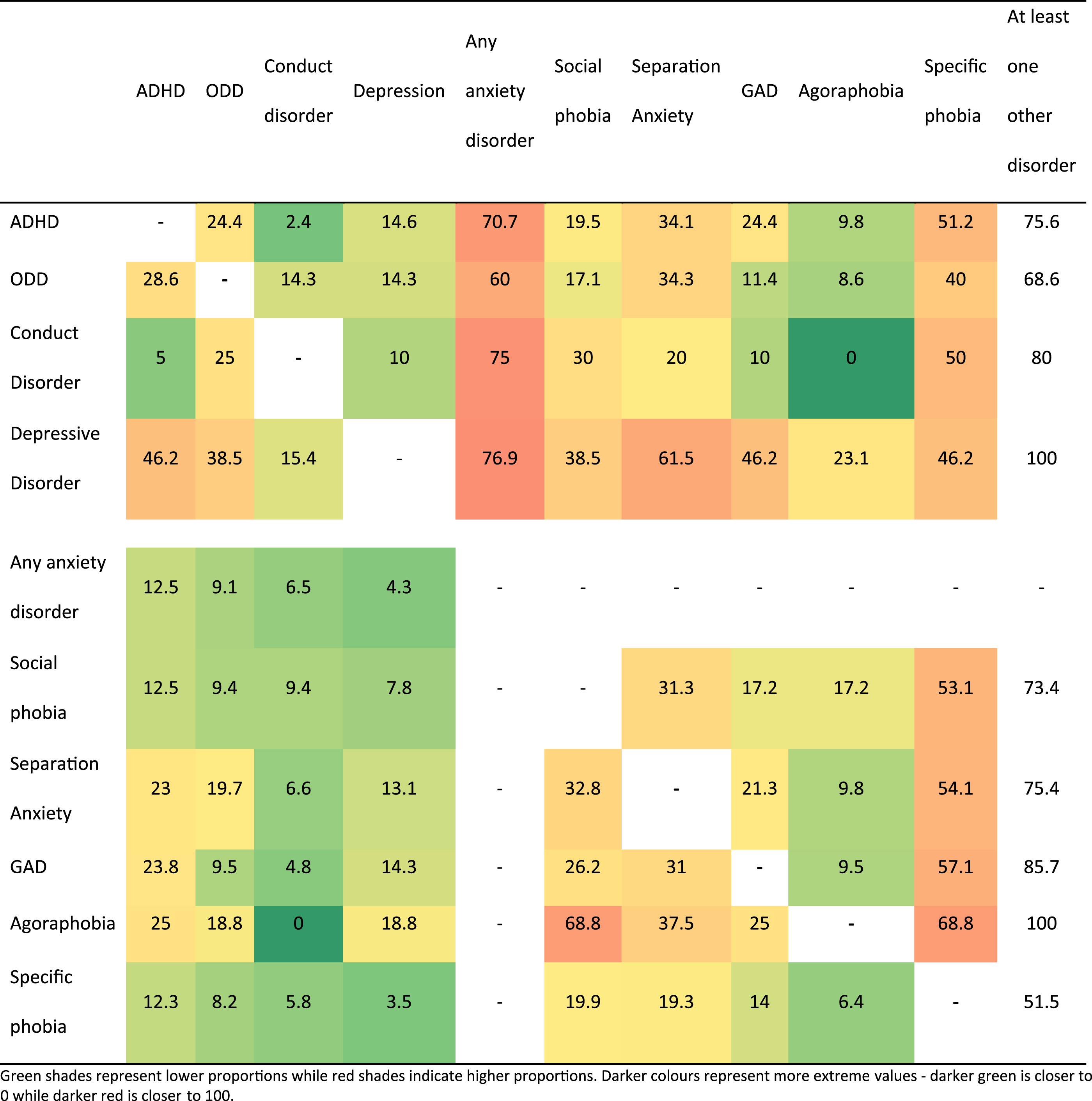
Among children with ADHD, ODD, conduct disorder and depressive disorder, between 60% and 77% of each group of children also had at least one anxiety disorder. At least half of the children with ADHD (51.2%) and those with conduct disorder (50.0%) also had specific phobias. Within the anxiety disorders, more than half of the children with social phobia (53.1%), separation anxiety (54.1%), GAD (57.1%) and agoraphobia (68.8%) also had specific phobias.
Odds Ratios (95% Confidence Intervals) of Each Other Diagnosis Given Each Diagnosis, Where p < 0.001 (Excluding Depressive Disorders and Panic Attacks)
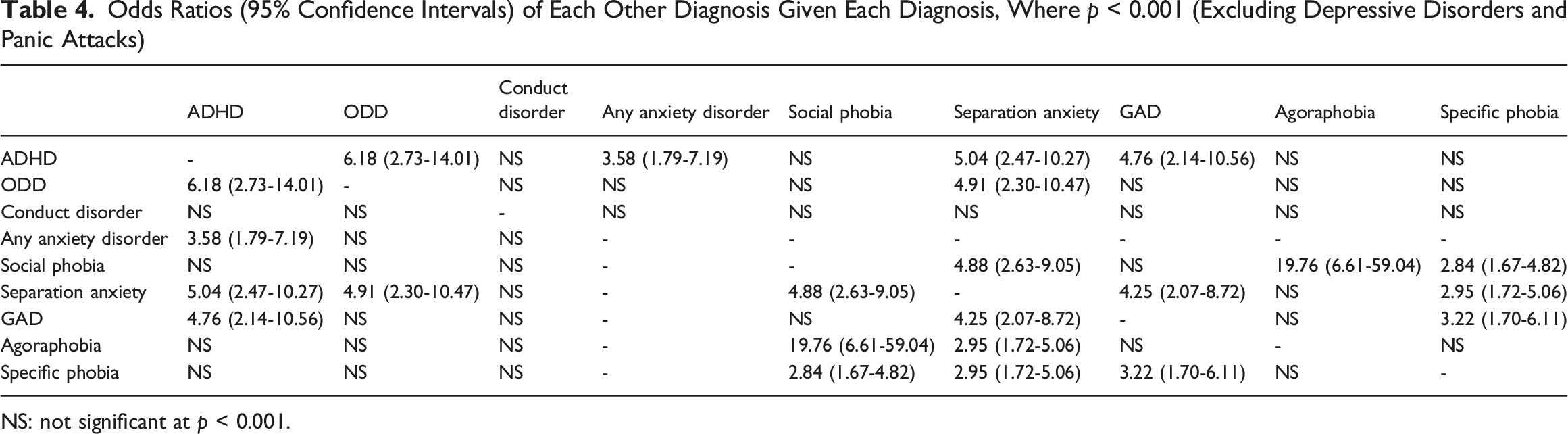
NS: not significant at p < 0.001.
Consistent with the fact that that all children with depressive disorder and all those with agoraphobia had other mental disorders, these disorders were associated with much higher odds of several other mental disorders.
Discussion
The aim of this study was to describe mental disorders and comorbidities among a cohort of 3- to 4-year-old children, using the PAPA interview. We found that almost half (48%) of the children in this study met criteria for at least one PAPA diagnosis, and 21% had two or more diagnoses. Of those with one diagnosis, 44% had two or more diagnoses.
To our knowledge, this is the first study in Australia to report on mental disorders and comorbidities among preschool-aged children, using the PAPA. This is also the first study to use the PAPA among a non-clinical sample in this age group in more than a decade, at a time when a substantial increase in the prevalence of mental health problems among children and adolescents is being labelled a ‘youth mental health crisis’ (McGorry et al., 2025). The prevalence of disorders among preschool-aged children in our study (48%) is substantially higher than previously reported in two international studies which used the PAPA more than a decade ago. In Norway, the prevalence was reported to be 6% (2012) while in the USA it was 27% (2011). The children in our study were a similar age to those in the USA study (mean age for both studies 43 months), which is younger than the mean age for the study in Norway (mean 53 months). The high prevalence of mental disorders in our sample could be ascribed to the much larger proportion (31%) with specific phobias in our study compared to the prevalence of specific phobias in the USA study (9%) (2011) and the Norwegian study (1%) (2012), both of which also assessed mental disorders using the PAPA. Without specific phobias the overall prevalence in our findings would have been reduced to 32%. Specific phobias are the most prevalent anxiety disorder among children and adolescents and as such, can often inflate overall prevalence estimates (Rapee et al., 2023). Fear responses to scenarios such as the dark, storms, dentists and doctors may be considered normal in pre-schoolers at low frequencies (Egger et al., 2006); these may be relatively transient compared to other disorders.
The overall prevalence of comorbidity (meeting criteria for two or more diagnoses according to the PAPA) in our sample was 21%. Another PAPA-based study among a non-clinical sample reported the prevalence of comorbidity at 9% (Bufferd et al., 2011). In our study, depressive disorders and agoraphobia occurred only with other disorders, not on their own. The highest association was observed between social phobia and agoraphobia. Although specific anxiety disorders commonly occurred with other anxiety disorders this was not exclusively the case.
In this study, we found no significant difference in prevalence of comorbidities among children of women with depression early in pregnancy and those without, when we excluded specific phobias. This is surprising given the association between antenatal maternal distress and adverse socioemotional outcomes among children (Rogers et al., 2020); however, the authors of this review and meta-analysis suggest that the use of self-report measures to assess maternal mental health and child outcomes limits the interpretation of the findings. More research is needed to investigate associations between antenatal depression and comorbidities among preschool-aged child mental disorders, with both maternal and depression and child disorders assessed with diagnostic interviews rather than self-report measures.
Strengths and Limitations
This study adds to a small group of studies (Bufferd et al., 2011; Wichstrøm et al., 2012) reporting prevalence of mental disorders and comorbidities among preschool-aged children, using the PAPA structured interviews with parents (Egger et al., 2006, 2019).
We acknowledge several limitations. The PAPA, while widely used and demonstrating high test-retest reliability among preschool children, was adapted from the parent version of the Child and Adolescent Psychiatric Assessment (CAPA) (Angold et al., 1995); other assessments are available that were developed specifically for this age group (In-Albon et al., 2020). Ours was a selected cohort study, not recruited for the purpose of reporting prevalence and hence without the specific methodological requirements for a prevalence study. Mothers with depression diagnosed early in pregnancy are over-represented due to the recruitment strategy and therefore this is not a community sample where generalisable prevalence data can be ascertained. Overreporting of children’s psychiatric symptoms has been reported among depressed mothers (Müller et al., 2011, 2014). We did not assess maternal depression with structured interviews at child age 3–4. Although we took steps to improve statistical power (excluding small groups from odds ratio calculations) and corrected for multiple comparisons, we advise readers to interpret Table 4 with caution owing to some very wide confidence intervals. Given the deliberate over-sampling of women with depression in our longitudinal cohort, the relatively high level of tertiary education, and the fact that only 62% of women recruited during pregnancy completed the PAPA when their children were 3–4 years old, we recommend that this finding be confirmed with a large, more representative sample, controlling for relevant pregnancy and early childhood environmental factors.
Further limitations may include that we administered the PAPA via telephone interview and not face to face as originally recommended by the authors of the PAPA (Egger & Angold, 2004). Information bias leading to false positives may arise from telephone interviewing. Although other studies report telephone interviews for the PAPA (Bufferd et al., 2011; Danzig et al., 2013; Hattangadi et al., 2024), reliability for telephone-based administration is lacking. Owing to limited resources, we were unable to implement double coding of the PAPA interviews beyond the initial training period of novice interviewers; inter-rater reliability can therefore not be reported Our study was a cross-sectional assessment of the children; future research to report on the trajectory and stability of disorders and comorbidities is recommended. It is not known how impairment associated with multiple diagnoses compares with that associated with single diagnoses; a nuanced assessment of impairment for both groups of children could address this in future research. In addition, we collected data only from mothers; it would be preferable to have multiple sources of data and future studies should collect data from fathers or other informants, to reduce informant bias (Bufferd et al., 2011).
The PAPA is a reliable diagnostic instrument for the preschool population. The high prevalence ascertained in our study may arise due to the robustness of this instrument compared with other studies which utilised parent-reported rating scales. However, the high prevalence may also be the result of over-pathologisation of normative responses, such as fear, which is a normative developmental phenomenon among preschool-aged children. As mentioned, the PAPA was adapted from the CAPA; diagnostic criteria for older children have therefore been applied to a younger age group. In addition, we have noted methodological limitations including non-representative sampling, informant bias and information bias arising from telephone interviewing. Our findings should therefore be treated as preliminary and with caution, awaiting replication by other studies in Australia or similar settings that utilise research-based semi-structured diagnostic interviews such as the PAPA. Longitudinal studies would illuminate homo- and heterotypic trajectories in children in non-clinical samples; among a clinical sample of children from preschool to primary school age, heterotypic development was relatively common, especially in the presence of maternal mental disorders (Jobs et al., 2019).
Alternatively, rather than the result of measurement or cohort effects, the high prevalence could be attributable to the preschool developmental window – a developmental vulnerability window which needs to be managed with care. As such, a “preschool-limited vulnerability” contrasting with “life-course-persistent variants” can be hypothesized as analogous to the “adolescence-limited” subtype of antisocial behaviours reported by Moffitt (1993). As noted above, the features of specific phobias, which appear to be particularly prevalent during the preschool period, could be conflated with normal developmental fears, or represent features of a normal developmental phase that will resolve with maturation. Longitudinal follow-up studies can track the developmental trajectories and differentiate whether “preschool-limited” and “life-course-persistent” subtypes exist.
Implications
Preliminary findings from out study, to be interpreted with caution, suggest that among preschool-aged children assessed with the PAPA, almost half yielded at least one diagnosis of a mental disorder. If problems are identified early, adjustments can be made before and once formal education begins, potentially preventing educational impacts from chronicity of mental disorders in later childhood and adulthood (Lyons-Ruth et al., 2017; Weisz et al., 2017). If mental health problems are left undetected, relationships with caregivers and peers may worsen over time and become more resistant to change (Bricker et al., 2004).
The relatively common occurrence of comorbidities (21% of children in our sample, 44% of those with a diagnosis according to the PAPA) suggests that children presenting with any mental disorder should be comprehensively assessed using a multi-methods assessment framework for a broad range of mental disorders. In addition, comorbidities may not be limited to “internalising” and “externalising” categories. When comorbid mental disorders are identified, coordinated child mental health services and treatments need to be accessible for a child and their family (Fisher, 2022). Comorbidity complicates treatment of children (Weisz et al., 2017); treatments that focus on single disorders may not be appropriate and may need to be replaced by treatments that consider multiple disorders (Barlow & Carl, 2012); the evidence for efficacy of such treatments is still limited and mostly among older children (Weisz et al., 2017).
Our findings also raise the possibility whether there exists a “preschool-limited” variant of psychopathology. Such variants can explain the high prevalence, analogous to the steep increase in anti-social behaviours in the adolescence window (Moffitt, 1993). Future studies with longitudinal design can explore this hypothesis; and if confirmed, examine the predictors of “preschool-limited” and “life-course-persistent” subtypes.
Our study suggests that clinicians and researchers should be aware of the relatively high prevalence of mental disorders and various comorbidities among these. Prior to the commencement of formal education, there is a window of opportunity to identify and manage disorders and lay the foundation for more optimal mental health and relationships.
Footnotes
Acknowledgments
The authors are extremely grateful to the participants for their ongoing participation in the study. We would also like to thank the MPEWS team of research coordinators and data collectors, without whom this work would not have been possible.
Ethical Considerations
The study has been approved by the Mercy Health Research Ethics Committee (Victoria, R08/22, 3 July 2012) and the South Metropolitan Health Service Human Research Ethics Committee (Western Australia, 2016-192, 11 October 2016).
Consent to Participate
Each woman provided written consent to participate at each wave of data collection.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported through the 2012 National Priority Founding Round of Beyondblue in a three-year research grant (ID 519240) and a 2015 National Health and Medical Research Council (NHMRC) project grant for 5 years (APP1106823). For Western Australian data, we would like to also acknowledge the support of the Spinnaker Foundation, Telethon Perth Children’s Foundation and WA Country Health Service in supporting this study. The funders had no involvement in the study design; the collection, analysis and interpretation of data; writing of the report; and the decision to submit the article for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.